RELATIONSHIPS BETWEEN ACCOUNTABLE CARE ORGANIZATIONS AND SKILLED NURSING FACILITIES: WHAT ARE THE CRITICAL PROCESS ELEMENTS?
Lisa Shock
A dissertation submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Public Health in the Department of Health Policy and Management in the
Gillings School of Global Public Health.
Chapel Hill 2019
Approved by: Sandra Greene Dale Green
Susan Helm-Murtagh Kristen Reiter
© 2019 Lisa Shock
ABSTRACT
Lisa Shock: Relationships Between Accountable Care Organizations and Skilled Nursing Facilities: What Are the Critical Process Elements?
(Under the direction of Sandra Greene)
Accountable care organizations (ACOs) have an incentivized Centers for Medicare and Medicaid Services (CMS) contractual agreement to ensure that attributed Medicare patients receive cost-efficient, high-quality care. It is hypothesized that relationships between ACOs and skilled nursing facilities (SNFs) may correlate with positive patient outcomes for cost and quality. Contractual elements are defined as specific processes and procedures measured by outcome metrics. Readmissions, length of stay (LOS), and episodic cost of care are potential outcome markers to assess SNF care delivery quality.
This study aimed to define critical relationship provisions between ACOs and SNFs that influence patient health outcomes. A value-based ACO and CMS contract, which defines
A systematic literature review explored relationships between ACOs and SNFs, examined elements and provisions of contracted relationships, and identified potential correlations to cost of care, SNF care quality, and health outcomes. The current literature demonstrates limited positive outcomes, defined as reduced readmission rates and post-acute savings per beneficiary, when care is delivered at a SNF with an ACO relationship.
A mixed-methods approach utilized qualitative and quantitative data collected from ACO health systems nationwide in two stages: (1) analysis of qualitative data collected through key informant interviews with leaders from ACOs, health systems, and community SNFs within each community intended to reveal important provisions to include in a ACO/SNF relationship; and (2) quantitative data analysis performed using existing SNF utilization reports to evaluate elicited themes around people, data, and education as evidenced by ACO network processes and
ACKNOWLEDGMENTS
I would like to acknowledge the following individuals: my husband for his tireless
TABLE OF CONTENTS
LIST OF TABLES ... ix
LIST OF FIGURES ... x
LIST OF ABBREVIATIONS ... xi
CHAPTER 1: BACKGROUND ... 1
Conceptual Framework ... 6
Definitions ... 9
Research Questions and Hypothesis ... 10
CHAPTER 2: LITERATURE REVIEW ... 11
Methods ... 11
Results ... 13
Readmissions ... 15
Cost ... 17
ACO/SNF Contracting and Cost ... 17
Discussion ... 18
Readmissions ... 19
Contracting ... 21
Cost ... 23
Geographic Area ... 23
CHAPTER 3: METHODOLOGY ... 26
Aims ... 26
Methodology for the Phase 1 Qualitative Analysis ... 29
Delimitations ... 37
Data Management Plan ... 37
Data Analysis Plan ... 38
Second Coder Interrater Reliability ... 41
Methodology for the Phase 2 Quantitative Study ... 42
Data Sources ... 46
Data Analysis Plan ... 47
Study Limitations ... 49
CHAPTER 4: RESULTS ... 51
Results of the Phase 1 Qualitative Study ... 51
In-Depth Qualitative Analysis: Key Findings ... 54
Theme 1: Importance of Data ... 54
Theme 2: Emphasis on People ... 56
Theme 3: Importance of Education ... 58
Results of the Phase 2 Quantitative Analysis ... 64
CHAPTER 5: DISCUSSION ... 74
CHAPTER 6: PLAN FOR CHANGE ... 79
APPENDIX A: ABSTRACTION TABLE ... 91
APPENDIX B: LITERATURE REVIEW QUALITY TABLE ... 93
APPENDIX C: KEY INFORMANT INTERVIEW GUIDES ... 95
APPENDIX E: DATA DICTIONARY FOR POST-ACUTE COST
LIST OF TABLES
TABLE 1: Definitions of terms used ... 9
TABLE 2: Research aims and proposed methods ... 27
TABLE 3: ACO selection and summary descriptors ... 30
TABLE 4: CMS ACO program descriptors... 31
TABLE 5: Independent and dependent variables ... 47
TABLE 6: Example correlation of ACO patient outcomes to SNF processes ... 49
TABLE 7: Completed key informant interview categories and roles by ACO ... 52
TABLE 8: Total ED utilization by ACO: ED visits/100 days from the top 15 SNFs ... 72
TABLE 9: Comparison of case mix index and total cost for SNF admissions by ACO ... 72
LIST OF FIGURES
FIGURE 1A: Conceptual model ... 7
FIGURE 1B: ACO/SNF quality framework ... 7
FIGURE 2: PRISMA flow diagram ... 14
FIGURE 3: Mixed-methods approach ... 29
FIGURE 4: Approach to data analysis for the phase 1 qualitative research ... 39
FIGURE 5: Prevalent themes elicited from the qualitative study ... 42
FIGURE 6: Framework for ACO/SNF relationship development ... 43
FIGURE 7: ACO B SNF Cost and Utilization Report ... 66
FIGURE 8: ACO C SNF Cost and Utilization Report ... 67
FIGURE 9: ACO D SNF Cost and Utilization Report ... 68
FIGURE 10: ACO F SNF Cost and Utilization Report ... 69
FIGURE 11: LOS comparison for non-preferred versus preferred SNFs ... 70
FIGURE 12: Thirty-day readmission rate comparison for non-preferred versus preferred skilled nursing facilities ... 71
FIGURE 13: Variation in SNF utilization metrics ... 73
FIGURE 14: Example SNF collaborative scorecard results ... 83
LIST OF ABBREVIATIONS
ACO accountable care organization
CFIR Consolidated Framework for Implementation Research
CMI case mix index
CMS Centers for Medicare and Medicaid Services
EBP evidence-based practice
ED Emergency Department
IRB institutional review board
LOS length of stay
MDS minimum data set
MSSP Medicare Shared Savings Program
CHAPTER 1: BACKGROUND
The need to control excess health care spending in the United States has led to new, innovative payment models under the Centers for Medicare and Medicaid Services (CMS). With the passage of the Affordable Care Act, one such model is the accountable care organization (ACO). ACOs are defined as health care entities that demonstrate efforts to reduce fee-for-service Medicare spending through care and cost improvement efforts (Pham, Cohen, & Conway, 2014). The ACO may be composed of any combination of hospitals, health systems, and independent physician associations under an ACO governance structure delivering coordinated care. Driven by a focus on value-based care, ACOs have proliferated nationwide (Fisher & Shortell, 2010).
ACOs promote collaboration around cost and quality between physicians, hospitals, and other clinicians, along with community health care organizations. Through the development of processes designed to improve quality and slow spending growth for a defined population of Medicare beneficiaries, new relationships and collaborations result in new models of care delivery and collaboration (Fisher & Shortell, 2010).
In order to be successful, hospitals and physicians participating in shared savings programs via ACOs will need to establish meaningful partnerships with all types of providers, including post-acute care providers. Post-acute care, including long-term hospital care,
in the utilization of post-acute care and inpatient services (Newhouse & Garber, 2013).
Partnerships with SNFs are particularly critical, since they account for about half of Medicare’s post-acute care spending (Mechanic, 2014).
SNFs are defined as residential settings for people who have compromised their activities of daily living and require 24-hour clinical care. While the term “nursing home” is often used loosely, not all nursing homes are SNFs. To qualify as a SNF, the facility must meet federal criteria for Medicaid and Medicare reimbursement for nursing care, including the following: the supervision of the care of every patient by a physician, the employment full-time of at least one registered nurse, the maintenance of records concerning the care and condition of every patient, the availability of nursing care 24 hours a day, the presence of facilities for storing and
dispensing drugs, the implementation of a utilization review plan, and overall financial planning including an annual operating budget and a 3-year capital expenditures program (Centers for Medicare and Medicaid Services, 2018c; Merriam Webster, 2017). As many SNFs are community based or corporate owned, even today there is often no pre-existing relationship between a physician organization or hospital system and a SNF. As ACOs have become more prevalent nationwide as a vehicle for coordination of clinical care, there is an increased effort to create preferred networks of post-acute providers between ACOs and their geographic
community in an effort to save money and improve quality through better management of post-acute care, ensuring that patients are treated in the most cost-effective, clinically appropriate setting (Mechanic, 2014).
clinicians working within hospitals and SNFs to influence care for ACO-attributed patients” (p. 518).
Defining quality within the SNF setting is challenging due to many nuances that may ultimately influence outcomes. The development of processes and procedures that lead to specific changes in health care delivery is hypothesized to influence outcomes such as length of stay (LOS) and readmission rates. Operationalizing “quality” from standard definitions can be problematic, as the definitions are extremely general and subjective and resulting measures are unable to fully realize the quality concept (Castle, Zinn, Brannon, & Mor, 1996). Due to this inability to adequately realize and define “quality” in nursing homes, quality indicators are prevalent rather than quality measures. This helps denote a less precise association between the “indicator” and actual quality (i.e., they are surrogate measures) (Castle & Ferguson, 2010).
Donabedian (1988) proposed that quality could be measured in terms of structures (S), processes (P), and outcomes (O) (Castle & Ferguson, 2010). Structural (organizational) measures are the organizational characteristics associated with the provision of care. Process measures are characteristics of things done to and for the resident. Outcome measures are the desired states one would (or would not) like to achieve for the resident (Castle & Ferguson, 2010). ACOs can influence quality of care delivery by implementing specific processes and procedures within the ACO/SNF relationships created within their geography. Within these operational partnerships, a network of SNFs that are preferred partners with the ACO develops through this increased collaboration.
Aside from geographic location, ACOs focus on three basic characteristics when
(Mechanic, 2014). As ACOs work to improve quality and optimize spending, innovation in post-acute care is accelerating and extending into the SNF community (Mechanic, 2014). Contractual participation in MSSP ACOs has been associated with reductions in post-acute spending without reducing quality, primarily through clinician efforts within hospitals and SNFs to influence care for ACO patients (McWilliams et al., 2017).
Process implementation within the ACO relationship has led to reduced SNF spending and has been shown to increase ACO savings rates (Muhlestein et al., 2018). Implementation of specific processes to facilitate coordination of care between hospital and post-acute care settings presents a viable opportunity for ACOs to improve cost performance. The dollars spent per Medicare beneficiary vary greatly among referral regions and there is controversy about the causes of this variation, its effects on quality and outcomes, and what, if anything, should be done about it (Newhouse & Garber, 2013).
ACOs must report quality data to CMS at the end of each performance year. CMS
measures every ACO’s quality performance using standard methods across four quality domains: patient/caregiver experience, care coordination/patient safety, preventive health, and at-risk populations (Centers for Medicare and Medicaid Services, 2018a). All ACOs report their performance on SNF cost control to the CMS through the ACO-35 Skilled Nursing Facility 30-Day All-Cause Readmission Measure (Centers for Medicare and Medicaid Services, 2016) in addition to reporting performance on a number of other metrics.
geographic area. The ACO has an existing contractual incentive with CMS to ensure that these attributed Medicare patients receive cost-efficient, high-quality care (Centers for Medicare and Medicaid Services, 2017b). Instituting a contractual relationship for patient management
between the ACO and a SNF allows for potential improvement in care coordination between the hospital and the chosen SNF discharge setting.
When ACOs are creating preferred partnership networks with community SNFs, leakage outside of the network is a significant concern. As choice of SNF upon discharge is ultimately left to the patient and family, it is increasingly challenging for the ACO to develop relationships with all possible SNFs that their attributed beneficiaries may possibly use. This challenge contributes to the difficulty of ensuring that attributed patients are treated in a high-quality, cost-effective SNF.
Readmissions are one marker for low quality of care delivery within the SNF. A study by Wang et al. (2016) reported that increasing nursing home performance is associated with
decreases in community-level risk-standardized readmission rates. One potential pathway for increased SNF performance could match assessment of SNF quality and SNF resources to ensure adequate handling of patient clinical needs upon hospital discharge. Potentially, there would be bidirectional communication of quality and resource capability from the SNF to hospital for every ACO-attributed Medicare patient and, as a result, each patient would be appropriately matched on hospital discharge to a SNF capable of addressing his or her condition with high-quality care and adequate resource delivery.
included in the ACO network or not, would define collaboration of care, data exchange, and measurement of quality in the post-acute setting. These relationships, initiated by the ACO as the owner of the responsibility for the attributed patient, may have financial benefits to both parties and are designed to ensure coordinated care that results in lower costs.
Currently, it is unknown what specific elements are critical to include within a
relationship between an ACO and a SNF that will result in improved cost, quality, and health outcomes. Examples of possible contractual relationship processes that might influence quality of SNF care would include ACO case management to assess appropriate LOS recommendations and timeliness of communications between the discharging hospital and the ACO. Additional research is needed to understand what contractual processes and provisions are positively associated with reductions in cost, readmissions, and LOS. This research will focus on the relationships between SNFs and ACOs, examine processes used by the ACO to coordinate care within the SNF, and compare outcomes between beneficiaries admitted to SNFs with established ACO relationships to those outcomes for beneficiaries admitted to SNFs outside the preferred ACO post-acute network.
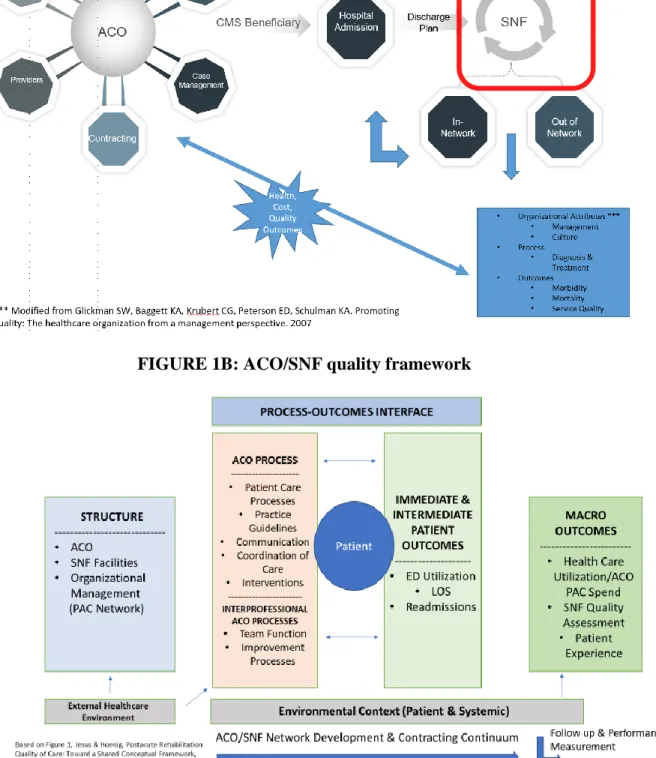
Conceptual Framework
FIGURE 1A: Conceptual model
FIGURE 1B: ACO/SNF quality framework
Ultimately, the choice of SNF upon discharge is up to the patient and/or the patient’s family. The organizational structure of the SNF in terms of physical environment, management of executive leadership, culture, and information management will all influence the patient experience and will likely influence patient outcomes. The red box noted in Figure 1A is where the second conceptual model around SNF quality is inserted as noted in Figure 1B.
This addition to the model addresses key factors influencing the ACO network structure as well as the process design and outcomes inside the SNF that will influence patient outcomes including LOS and readmission rates. The anticipated barriers and facilitators related to ACO/SNF contract implementation are housed within the process and outcomes interface, which is directly influenced by the ACO/SNF network structure. This adaptation of a post-acute rehabilitation conceptual framework provided the theoretical support for the conceptual model and drove the design of the qualitative research questions within the first portion of this research study (Jesus & Hoenig, 2015).
The inclusion or exclusion of the SNF to which the beneficiary is admitted in the ACO network would be dependent on the ACO/SNF relationships within a given geographic area. After SNF admission, a comparison may be made between SNFs, to assess readmission rates, cost, and quality between the in- and out-of-network SNFs and then assess influence on patient outcomes. Ultimately, a clearer understanding of the organizational attributes and facility
processes may provide additional information beyond published SNF quality rankings to allow a more informed consent for the patient at the initial decision point for SNF admission.
context to include actions taken by patients or their families. Within the Donabedian (1988)
model, the measurement of process is nearly equivalent to the measurement of quality of care
because process contains all acts of healthcare delivery. This research study sought to understand
the critical processes and procedures that, when implemented within a SNF and coordinated by
the ACO, influence patient variables of LOS and readmission rates.
Definitions
Definitions of terms used in this work are provided in Table 1. Here, the patient population is specifically defined as Medicare ACO beneficiaries admitted to a SNF. The existence of a contractual relationship will be compared to no relationship or usual activity. The health outcomes measured will be specifically LOS within the SNF and readmission rate from SNF back to the hospital.
TABLE 1: Definitions of terms used
Term Definition
Accountable care organization (ACO)
Health care organizations that demonstrate efforts to reduce fee-for-service Medicare spending through care improvement
(Pham et al., 2014) Skilled nursing
facility (SNF)
A residential setting of care for people who have compromised their activities of daily living and require 24-hour clinical care. SNFs are also referred to as nursing homes
Contractual relationship
A legal contract between an ACO and a SNF that defines
collaboration, data exchange, and measurement of quality in post-acute care. These contracts may have financial benefits to both parties and may include specific operational service requirements
Health outcomes Limited specifically to definitions of length of stay (LOS; the number of days a patient stays in a SNF for a clinical episode of care),
readmissions (defined as a bounce-back admission from SNF to hospital), and Emergency Department (ED) utilization
SNF quality of care Defined as the quality of health care delivery and services provided as measured by publicly available data and health outcomes in the “place” (SNF), which may influence frequency of bounce backs and rates of ED utilization and readmission
Research Questions and Hypothesis
Do ACO-attributed Medicare beneficiaries discharged to SNFs that have a defined relationship with an ACO have better outcomes than ACO-attributed Medicare beneficiaries discharged to non-contracted SNFs? This mixed-methods study sought to define what specific contract provisions between the ACO and the SNF lead to better outcomes and to identify the process mechanisms by which specific contract relationship provisions lead to better outcomes (e.g., process changes).
CHAPTER 2: LITERATURE REVIEW
Methods
A review of the literature was conducted to address the following research question: Do health outcomes for patients in SNFs that have contractual relationships with ACOs differ from health outcomes for attributed patients admitted to SNFs with no contractual relationship with ACOs? Articles included in this review were obtained from systematic searches of the following databases: PubMed, ProQuest Health Management, SCOPUS, and Web of Science. The
following search terms were used to address the definitions above: (“skilled nursing care” OR “skilled nursing facility” OR “nursing home” OR “nursing facilities” OR “long-term care”) AND (“accountable care organization” OR “ACO” OR “pay for value”) AND “contract” OR
“reimbursement” OR “cost” OR “relationship” OR “incentive” OR “Medicare”.
Snowballing and citation mining using the key words above helped to build the overall body of literature for this review. Inclusion criteria included full-text articles in English and articles specifically discussing ACOs and post-acute care networks with mention of SNF care. Descriptive and analytical studies were accepted, as were studies containing qualitative or quantitative data. Studies that included the Medicare population as SNF patients and addressed quality of care in that setting were included. Additional studies discussing bounce-back
readmissions from SNF to hospital were also included. Articles defining characteristics contributing to LOS in the SNF setting were similarly reviewed.
outcomes of readmission rates from SNF to hospital, cost, or LOS; and those broadly discussing quality metrics without specific mention of skilled nursing or long-term care. Additional
exclusions were applied when looking at the SNF as a setting. Studies discussing residents at facilities labeled as rest homes or extended care facilities were excluded, as those settings may not house patients with the same level of clinical acuity and care needs seen in a SNF.
Search results were captured, duplicates were removed, and inclusion and exclusion criteria were applied. Initially, article titles were reviewed to identify studies that provide insight into the research question regarding the association between ACOs and SNFs. Abstracts were then reviewed to assess studies based on inclusion criteria. Additional search terms were factored into the search strategy to define inclusion criteria and included the following: “length of stay” OR “readmissions” OR “quality” OR “patient admission” OR “patient transfer”.
For studies meeting the inclusion criteria, full-text articles were obtained and read. A data abstraction form was created in Excel and catalogued the author, journal name, study design, and study population (Appendix A). As many of the final included articles were health policy
Results
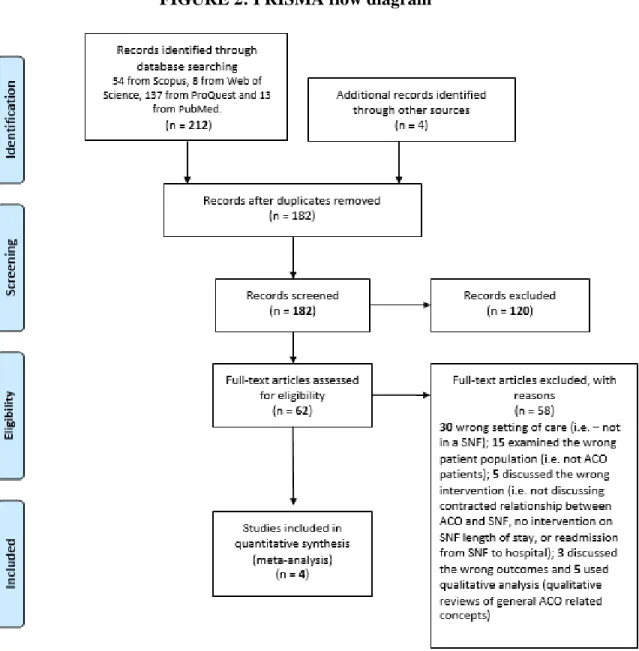
Results of the literature review are illustrated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram in Figure 2. The literature search yielded 212 references, including 54 from Scopus, 8 from Web of Science, 137 from ProQuest, and 13 from PubMed. Four additional references were identified through bibliographic references and recommended articles from Mendeley. After duplicates were identified and
FIGURE 2: PRISMA flow diagram
there were few. The literature remains sparse when examining the connection between ACOs and SNFs as it correlates to patient readmission rates or LOS in the SNF. This literature review defined the research to date and there is a surplus of commentary within the gray literature on population health and ACOs in general. Given the author’s role at a national population health company and work with ACOs nationwide, the author reads these updates daily. For the final dissertation, an additional literature review was conducted to add any critical or materially relevant articles.
Of the remaining articles, four presented quantitative data analyses on one or more outcomes. Five additional articles were excluded because they were qualitative reviews of general ACO-related concepts and did not address the appropriate inclusion outcomes.
The remaining four quantitative studies could be grouped into two studies that primarily examined readmissions alone as a quality outcome (Maly et al., 2012; Winblad, Mor, McHugh, & Rahman, 2017) and two studies that examined specific but incompletely defined process elements between ACOs and SNFs (Lage, Rusinak, Carr, Grabowski, & Ackerly, 2015; McWilliams et al., 2017). The themes of outcome analysis, cost, and contracting elements are further reported within these results.
Readmissions
Maly et al. (2012) reviewed available CMS ratings data and performed claims data analysis to examine readmission rates, whereas Winblad et al. (2017) performed a comparative analysis between ACO-affiliated hospitals and non-affiliated hospitals in reducing readmissions.
readiness for collaboration with the Lehigh Valley Health Network Organization. One of their specific variables of quality was measurement of the 30-day readmission percentage from SNF to hospital. They showed a decrease in readmissions for those patients admitted to SNFs within their preferred network. The authors found that by analyzing indicators of quality, they could create a scorecard that allowed the physician organization to prioritize relationships and referrals into community SNFs from the Lehigh Valley hospital system. Maly et al. (2012) hypothesized that using a tool to define strong collaboration between hospital and SNF will ultimately improve quality of patient care and reduce costs.
rate than non-ACO hospitals and they reduced hospitalizations within 30 days by more than 3 percentage points (Winblad et al., 2017).
Cost
Cost as a separate analysis was not undertaken in either the Winblad et al. (2017) or (Maly et al., 2012) studies. This was a noted limitation of these articles. Effect on cost reduction was implied in the readmissions analysis by Maly et al. (2012); however, more detail from additional claims analysis would be needed to reaffirm this conclusion.
ACO/SNF Contracting and Cost
The two remaining articles in this review more comprehensively addressed the theme of contracting between ACOs and SNFs and specifically discussed which individual relationship elements emerged as clinically significant, therefore influencing patient outcomes. Lage et al. (2015) showed a process for selecting SNF partners for an ACO collaborative network. They created a scorecard that awarded points based on quality criteria such as CMS five-star ratings, days of available clinical coverage within the facility, and readmission rates. They were one of the only groups to risk adjust the population admitted to a given SNF. Lage et al. (2015) used the OnPoint-30 Readmission Measure from the third quarter of 2013 to “calculate an expected readmission rate for each SNF using variables from the minimum data set (MDS) to adjust for illness severity. This measure is made available through the American Health Care Association and has been submitted and endorsed in 2016 by the National Quality Forum” (p. 805).
(Lage et al., 2015). Some of the ACOs included in this study cohort implemented some or all of these elements; however, these specific processes were not addressed as study inclusions.
When Lage et al. (2015) examined readmissions as an outcome, they noted that “… the average expected readmissions rate was 19.4%. For selected SNFs, this rate was slightly lower (18.4%), and for the ‘met minimum criteria; not selected’ SNFs, the rate was 20.4%” (p. 806).
McWilliams et al. (2017) looked more specifically at the cost component of the
ACO/SNF relationship. The primary endpoint of the study by McWilliams et al. (2017) was to evaluate changes in post-acute care spending and use of post-acute care associated with provider participation as ACOs in the MSSP and show the pathways by which these changes occurred (p. 518). The authors examined beneficiary spending longitudinally over time, comparing those served by ACOs to beneficiaries served by local non-ACO health care professionals (control group). They also examined costs before and after entry into the MSSP. McWilliams et al. (2017) reported that across 114 ACOs in 2012, participation in Medicare Shared Savings was associated with an overall reduction in post-acute spending driven by reductions in acute
inpatient stays and LOS in the SNF. McWilliams et al. (2017) further emphasized that reductions in LOS were largely attributed to within the hospital or within the SNF changes in care that were applied specifically to ACO patients. Cost estimates were similar for ACOs with and without financial ties to hospitals and their data showed that participation in the MSSP was not associated with significant changes in 30-day readmissions, use of highly rated SNFs, or mortality (McWilliams et al., 2017).
Discussion
was performed on readmission rates and clear inclusion and exclusion criteria were noted within each final study. The cost analyses of McWilliams et al. (2017) were thorough and this was the only study to approximate a per-beneficiary savings because of an ACO network contract. A significant limitation to overall quality was that each individual study touched on one or more variable components around four main themes: readmissions, contracting, cost, and geographic area. While LOS was initially proposed as a cost outcome, this variable was only tangentially discussed in the final review, and there were no definitive correlations reported when examining LOS within an ACO/SNF relationship.
Readmissions
Post-acute care in rural communities often includes care provided in swing beds. The term “swing bed” describes the level of care hospitalized patients receive once they are no longer in need of acute care. According to the Minnesota Department of Health (2007),
A national swing-bed program was first authorized in the 1980 Omnibus Budget Reconciliation Act (Public Law 96-499) allowing Medicare and Medical
Assistance reimbursement of swing-bed care in rural hospitals with fewer than 100 beds. Swing-bed admissions are limited to patients who require some level of skilled nursing care and are currently in a hospital acute care bed. Patients cannot be admitted to a swing bed from either the community or a skilled nursing facility unless they have spent three days in an acute care hospital bed for related service needs within the past 30 days. Swing bed days are generally limited to 40 days per patient under state law. (p. 4)
Within the ACOs included in this study, there was no significant proportion of rural hospitals meeting these criteria; therefore, the presence of swing beds was not included in the final analysis. An additional question was asked regarding the presence or absence of swing beds in each SNF key informant interview to verify this as well.
Patient demographics, including younger age in the commercial population, may change the outcomes of readmission rate as well as the salient components of the ACO/SNF contractual relationship. Commercial patients in risk arrangements may have fewer chronic diseases and more acute traumatic episodes, therefore limiting the ability to influence post-acute care costs or outcomes.
added patients from the community hospitals and physician networks. SNFs have a high attrition rate with many admitted for short-term rehabilitation as well as a high mortality rate due to the medical complexity of the elderly patients that they serve. Systemically addressing hospital/SNF relationships from a perspective of referral patterns has not been fully vetted in the literature. Many SNFs will assert that their facility readmission rates are less than optimal because they see sicker patients. Risk adjustment in the post-acute care setting is newly developing and is a gap in much of the literature and outcomes analysis.
Lage et al. (2015) were the only authors to use a risk-adjusted scoring measure to provide a case mix within the SNFs they analyzed. OnPoint-30 calculates an expected readmission rate for each SNF using variables from their MDS to adjust for illness severity. The MDS is part of the U.S. federally mandated process for clinical assessment of all residents in Medicare- or
Medicaid-certified SNFs. This data set collects information on each resident’s functional
capabilities and helps the care team to identify clinical problems (Centers for Medicare and
Medicaid Services, 2015). Aside from risk adjustment, the authors also used a scoring system in an attempt to define ACO/SNF partnership quality beyond publicly reported metrics (Lage et al., 2015).
Contracting
episode. They also did not mention the contractual process elements required to improve
outcomes for admitted patients to SNFs (Lage et al., 2015). Maly et al. (2012) scored and ranked discharges from hospital to SNF but focused primarily on high-volume SNFs rather than LOS or overall episode cost within the SNF.
McWilliams et al. (2017) examined claims data to investigate post-acute spending, but they defined their contracts as contracts between ACO organizations and the CMS Shared Savings ACO Program. Their focal relationship and did not focus directly on the contractual connection between ACO and SNF. Winblad et al. (2017) had a similar distinction, focusing only on the relationship between ACO-affiliated hospitals and SNFs. Their study also lacked meaningful information illustrating the specifically contracted process elements implemented between the ACO and SNF.
Within the final analysis for this dissertation, it must be acknowledged that the
hospital/SNF relationship may be a significant influence on the ACO/SNF relationship. Given the availability of data on all attributed beneficiaries within a given ACO, there may be situations in which the hospital or the SNF are one or both out of the ACO network. This will be a
Cost
Data discussing actual post-acute spending between ACO-affiliated facilities were
limited within this review. The only study to fully measure cost and show statistically significant reductions in SNF spending for ACO-affiliated entities was by McWilliams et al. (2017).
Specific cost metrics within the ACO and SNF relationships that positively influenced patient outcomes were not well defined across any articles reviewed.
McWilliams et al. (2017) were the most thorough in their analysis, showing that participation in a MSSP was associated with an overall reduction in post-acute spending (differential change in 2014 for ACOs versus control group) of −$106 per beneficiary. They addressed their cost analysis by showing that changes in post-acute care spending and use of post-acute care services were associated with provider participation in ACOs in the MSSP. No other study reviewed or performed a similar cost analysis.
Geographic Area
Summary
Future research is needed to fully understand the contractual process elements needed to ensure positive outcomes when patients are admitted to a SNF. The presence of an ACO
relationship between ACO and SNF is hypothesized to create a system of monitoring and addition of resources to ensure a higher quality of care. However, this connection has not been adequately proven within the literature.
Limitations in this review process included a restricted number of articles that showed defined contractual relationships between the entities of ACO and SNF. Many articles were excluded because they did not meet the criteria of setting of care (i.e., not in a SNF), they examined other patient populations (i.e., not ACO patients), they discussed other interventions (i.e., not a contracted relationship between ACO and SNF, no intervention on SNF LOS, or readmission from SNF to hospital), or they discussed other outcomes (i.e., did not examine SNF costs, LOS, or readmission rates).
This review does successfully demonstrate that there are initial positive correlations between ACO-affiliated hospitals and SNF to hospital readmission rates. This review also shows positive results of effective SNF network creation in an ACO collaborative network (Lage et al., 2015) and in one specific geographic area in Lehigh Valley (Maly et al., 2012). Additional research is needed to show that the contractual processes deemed important to include a facility in an ACO relationship are indeed positively associated with improvement in patient outcomes of readmissions and LOS.
individual patient health outcomes to patient choice of a SNF with guided context from the hospital discharge planners and then showing an added association with decreased health care cost is challenging due to multiple variables, confounders, and system issues. This research analysis has an existing hypothesis that if a SNF contracts with an ACO, there will be improvement in overall cost and quality of care for admitted patients.
Local ACOs must work with SNFs and community agencies within their geographic area to ensure that providers and patients are both informed and educated such that attributed ACO patients receive the appropriate level of health care service for their clinical needs. Feedback tied to clinical and financial outcomes supports the mission of the ACO to improve overall health while controlling costs and essentially solidifies the relationship between the ACO and the SNF.
CHAPTER 3: METHODOLOGY
The primary, overarching research question of this study is to define the critical
processes, led by ACOs, that facilitate SNF relationships and influence patient health outcomes. The rationale from the conceptual framework presented earlier is that the presence of a value-based contract between the ACO and CMS, which defines accountability for a specific population and includes metrics examining cost and quality, will lead the ACO to develop relational processes and procedures with community SNFs which result in meaningful improvements in patient health outcomes at the SNF, including LOS, ED utilization, and hospital readmission rates. It is therefore hypothesized that the presence of a relationship between an ACO and a SNF will result in a preferred ACO network of SNFs and within that network, specific operational process and procedural changes will result in reduced LOS, improved readmission rates between hospital and SNF, and decreased ED utilization.
Aims
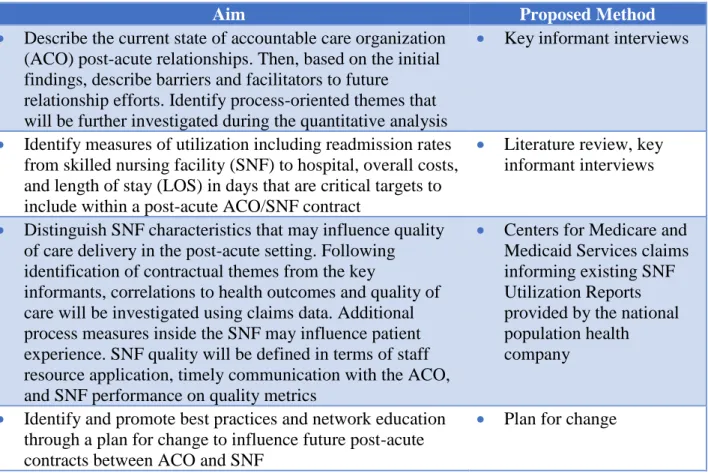
TABLE 2: Research aims and proposed methods
Aim Proposed Method
• Describe the current state of accountable care organization (ACO) post-acute relationships. Then, based on the initial findings, describe barriers and facilitators to future
relationship efforts. Identify process-oriented themes that will be further investigated during the quantitative analysis
• Key informant interviews
• Identify measures of utilization including readmission rates from skilled nursing facility (SNF) to hospital, overall costs, and length of stay (LOS) in days that are critical targets to include within a post-acute ACO/SNF contract
• Literature review, key informant interviews
• Distinguish SNF characteristics that may influence quality of care delivery in the post-acute setting. Following identification of contractual themes from the key
informants, correlations to health outcomes and quality of care will be investigated using claims data. Additional process measures inside the SNF may influence patient experience. SNF quality will be defined in terms of staff resource application, timely communication with the ACO, and SNF performance on quality metrics
• Centers for Medicare and Medicaid Services claims informing existing SNF Utilization Reports provided by the national population health company
• Identify and promote best practices and network education through a plan for change to influence future post-acute contracts between ACO and SNF
• Plan for change
This analysis utilizes both qualitative and quantitative data collected from ACO health systems nationwide in two stages. The first stage comprised analysis of qualitative data collected by the researcher through key informant interviews with ACO, health system, and SNF
The author works for a national population health company that partners with health systems as they enter into ACO contracts with CMS. The Chief Legal Counsel as well as the Chief Compliance Officer were supportive of this work and agreed to support this work in subsequent publications. Institutional review board (IRB) approval included a guarantee of anonymity at every health system; therefore, all data were blinded, and each health system identity was protected. As a clinical leader, the author has relationships with multiple health systems nationwide and is directly involved in the execution and operational design of their individual clinical programs. The author’s association with the national population health company allows access to reports that analyze CMS claims data for each health system, in addition to other data inputs, including admission/discharge/transfer feeds from the ACO-affiliated hospitals, electronic health record data from physician practices, laboratory and imaging data to examine utilization patterns, and data on social determinants including demographics.
While this research is of scholarly interest to the author’s national population health company, it is not part of the author’s ongoing role or responsibilities, nor is it a requirement of the author’s work. This national population health company has agreed to support this effort with resources. Informed consent was obtained from each key informant and each ACO. Assistance from an analyst employed by the national population health company was obtained to query the ACO data and review reports on specific variables related to SNF cost and quality. These variables were defined and chosen based on the themes that emerged from the initial qualitative key informant interviews.
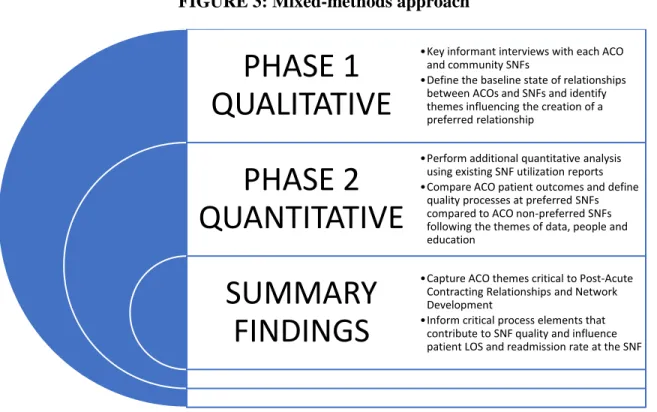
characterization of the social, historical, and political impacts of the findings. An exploratory sequential mixed-methods design (Creswell, 2014) was planned to begin with a qualitative research phase and explore the views of ACO leaders, health system leaders, and community SNF leaders. Inquiry and feedback from these key informant interviews then defined the components of the analysis in the quantitative phase that would be most clearly correlated with patient health outcomes.
FIGURE 3: Mixed-methods approach
Methodology for the Phase 1 Qualitative Analysis
ACOs were selected based on their relationship with the national population health company of the author and the presence of a contractual ACO relationship with CMS
participating in either the Track 1, Track 3, or Next Generation ACO programs. The purpose of conducting these interviews was to determine the important components that define relationships between ACOs and SNFs, examine how ACOs are developing preferred SNF networks, and
PHASE 1
QUALITATIVE
PHASE 2
QUANTITATIVE
SUMMARY
FINDINGS
•Key informant interviews with each ACO and community SNFs
•Define the baseline state of relationships between ACOs and SNFs and identify themes influencing the creation of a preferred relationship
•Perform additional quantitative analysis using existing SNF utilization reports •Compare ACO patient outcomes and define
quality processes at preferred SNFs compared to ACO non-preferred SNFs following the themes of data, people and education
•Capture ACO themes critical to Post-Acute Contracting Relationships and Network Development
identify specific outcome measures of utilization within successful post-acute ACO/SNF contracts. For the qualitative analysis, key informants were identified from six ACO health systems. This number was chosen initially because it was deemed reasonable and manageable. The key informants were initially defined as having an ACO partner relationship with the national population health company. Of the 15 initial partnerships currently in place with the author’s employer, six health systems were chosen based on maturity, geography, and size. Maturity was defined as initial entry into value-based care/population health or more than 1 year of experience in a population health/value-based contract. Geography was defined as urban or rural based on general geography and span of network. Size was defined by number of
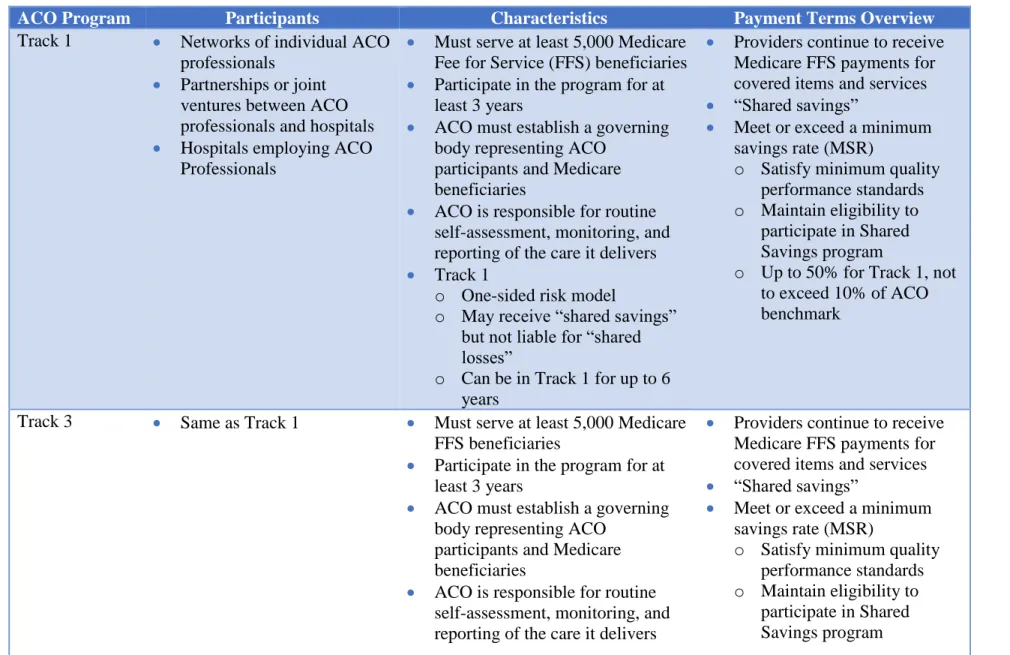
beneficiaries, and all of the health systems had at least 15,000 attributed Medicare fee-for-service lives. A listing of the ACOs chosen and their respective features, including type of CMS ACO contract, is shown in Table 3. Program types are compared and contrasted in Table 4.
TABLE 3: ACO selection and summary descriptors
ACO Size (No. of Covered Beneficiaries)
Location (Rural or Urban)
Maturity (No. of Years as an ACO in Value-Based Care and CMS Program)
A 18,000 Rural 1 as Next Generation ACO
B 20,000 Rural 3 as Next Generation ACO
C 21,000 Urban 3 as Track 3 ACO
D 20,000 Urban 5 as Track 1 ACO
E 18,000 Urban 1 as Next Generation ACO
31
TABLE 4: CMS ACO program descriptors
ACO Program Participants Characteristics Payment Terms Overview
Track 1 • Networks of individual ACO professionals
• Partnerships or joint ventures between ACO professionals and hospitals
• Hospitals employing ACO Professionals
• Must serve at least 5,000 Medicare Fee for Service (FFS) beneficiaries
• Participate in the program for at least 3 years
• ACO must establish a governing body representing ACO
participants and Medicare beneficiaries
• ACO is responsible for routine self-assessment, monitoring, and reporting of the care it delivers
• Track 1
o One-sided risk model
o May receive “shared savings” but not liable for “shared losses”
o Can be in Track 1 for up to 6 years
• Providers continue to receive Medicare FFS payments for covered items and services
• “Shared savings”
• Meet or exceed a minimum savings rate (MSR)
o Satisfy minimum quality performance standards
o Maintain eligibility to participate in Shared Savings program
o Up to 50% for Track 1, not to exceed 10% of ACO benchmark
Track 3 • Same as Track 1 • Must serve at least 5,000 Medicare FFS beneficiaries
• Participate in the program for at least 3 years
• ACO must establish a governing body representing ACO
participants and Medicare beneficiaries
• ACO is responsible for routine self-assessment, monitoring, and reporting of the care it delivers
• Providers continue to receive Medicare FFS payments for covered items and services
• “Shared savings”
• Meet or exceed a minimum savings rate (MSR)
o Satisfy minimum quality performance standards
32
• Tracks 2 and 3
o Two-sided risk model
o May receive “shared savings” AND liable for “shared losses”
o Up to 70% for Track 3, not to exceed 20% of ACO benchmark
• Liable for “shared losses” (Tracks 2 and 3):
o ACO meets or exceeds a minimum loss rate (MLR) it must repay a portion of the losses it generates
o Capped at 15% for Track 3 Next Generation • Same as Tracks 1 and 3
• Preferred Providers (not Next Gen providers/ suppliers)
o Providers/suppliers who may offer benefit enhancements to Next Gen beneficiaries and participate in Advanced Payment Models (APMs); services furnished will count toward each beneficiary calculation in ACO score
• Must serve at least 10,000 beneficiaries (7,500 if a RHC)
• Prospective Benchmarks
• Two Risk Arrangements:
o Arrangement A—shared savings and losses of up to 80%
o Arrangement B—shared savings and losses of up to 100%
• First dollar shared savings for spending below the benchmark and accountable for first dollar shared losses for spending above the benchmark
• Benefit Enhancement Tools
o Greater access to post-discharge home visits and telehealth and SNF services
o Opportunities for beneficiaries to receive rewards for receiving care from ACO and affiliated providers
• Prospective Benchmarks
• Four Payment Options:
o Normal FFS
o Normal FFS + per beneficiary per month (PBPM) recouped against shared savings or in addition to losses
o Population-based payments,
providers/suppliers have FFS claims reduced and ACO receives a monthly payment equal to the FFS reduction percentage
o Capitation, ACO receives monthly Per Beneficiary Per Month (PBPM)
capitation payments and is responsible for paying claims for ACO providers
33
o Process that allows
beneficiaries to confirm their care relationship with ACO providers
o Greater collaboration between CMS and ACOs in relation to their care
Key informants for each ACO were chosen by segregation into three role types: population health administrators/ACO leaders who were employees of the national population health company and responsible for implementation of post-acute network efforts, health system leaders/collaborators, and SNF community leaders within the ACO geography who receive ACO-attributed patients as admissions. General relationship barriers and facilitators and best practice relationship process recommendations were solicited from all three groups. For each chosen health system, a minimum of one member from each category was interviewed.
Informants were contacted initially by e-mail to request their participation. A brief description of the study was shared using a standardized script. When participants agreed to be interviewed, an appointment was scheduled either in person or via conference call at a time convenient to the participant. The face-to-face meetings were held in a private room, and all sessions were recorded after the principal investigator reviewed the study parameters and requested the participant’s permission and the participant gave informed consent.
Interview questions included inquiries across several categories, as follows: risks and benefits of post-acute relationship development; network development strategies, including barriers and facilitators and specific relational questions discussing ACO/SNF process elements as well as financial incentives; and needed physician and provider education as well as patient and family education. To address the research question, key informant opinions were solicited to define what specific processes and procedures were most critical to successful ACO/SNF
relationships.
informant opinions on the definition of quality care inside the SNF. Example probes could elicit additional descriptors around processes of nurse case management, utilization review within the SNF, data exchange, and timeliness of communication between hospital and SNF or ACO and SNF. The key informant interview guide is provided in Appendix C. Prior to use, the
questionnaire was pre-tested with two separate ACO leaders in two separate ACOs.
The principal investigator obtained consent from the key informant at the time of the face-to-face interview or conference call. The consent form was reviewed orally by the principal investigator and each participant was invited to ask detailed questions about the study. Study participants were interviewed in English. All study procedures were described in detail, with special emphasis on confidentiality, such that the participant was fully informed of his or her requirements while participating in the study. During this consent process, participants were reminded they were free to choose to take part in the research study or refuse.
Those who consented to participate in the study were interviewed for approximately 30 minutes. Questions were prioritized to keep the total interview time to 30 minutes or less. During the consent process, all participants were informed that the information they provided through these interviews was anonymous (i.e., not shared with anyone outside of the research team) and voluntary (i.e., they were not obligated to answer any question). Interviewees were told that they were free to take breaks and/or terminate the interview at any time.
Identification numbers, rather than names, were used on research materials to identify participants. Hard copies of interview guides and collateral materials were stored separately in a locked cabinet in the principal investigator’s office. All interview data and transcripts were stored in password-protected files on a computer at the principal investigator’s office. Once the interview data were analyzed and the study was completed, all transcripts were destroyed to ensure that no responses would be linked to an individual. All interview results are presented in aggregate and the names of the individual participants are kept confidential. Descriptors of key informants are included by role (population health administrator/ACO leadership, health system leader, or SNF regulator); to maintain anonymity of the respondent, individual participant names are not included.
Following each interview, all notes or phone recordings were transcribed using a purchased and encrypted application on the investigator’s phone. Completed transcripts were reviewed in detail and verified against the digital recording. Transcript-based content analysis of interviews was coded using NVivo 12 Plus qualitative analysis software, in which transcripts and field notes were carefully read and systematically coded to identify emerging themes. The
content analysis utilized an inductive approach, which revealed themes and identified patterns through a multi-phase coding process. The documents were coded, and a code book was created from relevant themes related to the research questions under investigation, based on the
collective knowledge, perceptions, and experiences of the researchers and informants.
reviewed to identify themes. The identified themes informed the variables to include within the quantitative claims analysis and contributed to the plan for change in order to influence the development of future policy and ACO/SNF relationship recommendations. The research process was reviewed and closely monitored by the dissertation chair and the committee members.
Delimitations
Purposeful selection was used to identify both ACO sites and key informants to assist with answering the research questions (Creswell, 2014). The qualitative study included only ACOs that were in a contractual arrangement with the investigator’s national population health employer and SNF leadership from facilities that received ACO patients. Other ACOs were excluded from this study because the primary focus of this dissertation is on the relationship between ACOs and SNFs and the author had access to the supporting clinical data and claims files for those affiliated ACOs. The selection of key informants was facilitated by company staff known to have working knowledge regarding ACO/SNF network strategies.
Data Management Plan
The qualitative portion of this study required the collection and storage of confidential data in several formats (e.g., transcription files, Word documents, transcribed documents, data analysis software files, e-mail communications, etc.). The location of the data files was password protected and only the researcher had access to all of the study files. The key informant interviews were recorded using a purchased application called ACR Pro on the investigator’s cell phone. The application is password protected and uses cloud technology to transport audio files to the partner transcription service, Otter. The investigator obtained a password-protected account with Otter; the audio records were digitally and securely shared and subsequently transcribed through this
password-protected folder upon completion and also uploaded into the password-password-protected version of NVivo 12 Plus, which was purchased and downloaded only to the investigator’s secured computer. The investigator followed the IRB security procedures recommended with IRB approval and the computer was additionally protected with the appropriate antivirus software.
Data Analysis Plan
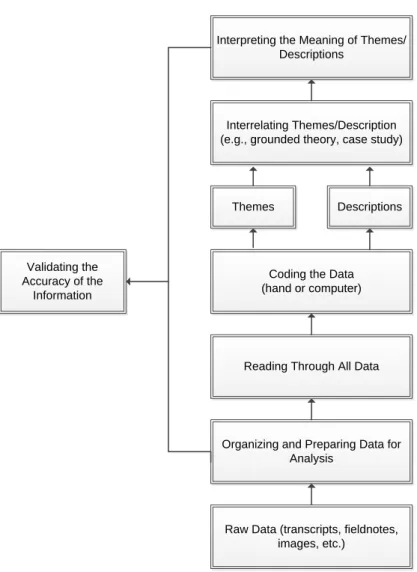
The conceptual model listed in Figure 1B was used to guide the qualitative data analysis procedures. This model contains key factors comprising the ACO/SNF network structure as well as process design and outcomes that will influence anticipated barriers and facilitators related to ACO/SNF relationship development. This post-acute rehabilitation conceptual framework provided the theoretical support for the conceptual model and drove the design of the research questions within the first portion of this qualitative research study (Jesus & Hoenig, 2015). This conceptual model guided the development of a data codebook for the key informant interviews with special emphasis placed on structure, process, and outcomes, with quality as an overarching theme.
FIGURE 4: Approach to data analysis for the phase 1 qualitative research
Interpreting the Meaning of Themes/ Descriptions
Interrelating Themes/Description (e.g., grounded theory, case study)
Themes Descriptions
Coding the Data (hand or computer)
Reading Through All Data
Organizing and Preparing Data for Analysis
Raw Data (transcripts, fieldnotes, images, etc.)
Validating the Accuracy of the
Information
Source: Reprinted from Research Design: Qualitative, Quantitative, and Mixed Methods
Approaches (4th ed., p. 197), by J. W. Creswell, 2014, Thousand Oaks, CA: SAGE Publications, Inc.
As each transcript was reviewed, themes and patterns were compared and contrasted according to the quality framework in Figure 1B. Initially, commonalities between the sites were examined in order to identify missing information and to discuss what shared processes were revealed against the qualitative conceptual model. This iterative process modification of the interview probes after one round of pre-testing with two separate and individual key informants helped to further understand findings that were not part of the initial questionnaire.
The key informant interviews sought to identify SNF characteristics that influence quality and may therefore influence patient outcomes. System complexity is a confounder, influencing SNF choice. For example, during the first initial interviews, key informants mentioned education about SNF quality as a criterion for partnership. This estimation of SNF quality was initially defined by the key informants to be evidenced by star ratings and public CMS data, but some key informant interviews also cited the importance of SNF clinical care capabilities (i.e., could the SNF admit a patient on a wound vac or who needed intravenous infusions as a decision-making determinant for hospital/SNF transitions?). While not tied directly to the relationships between ACOs and SNFs, this finding spoke to the complexity of the hospital discharge process resulting in admission of the patient to the SNF, and more specific questions were then asked to delineate opinions on education directed at the referring physician and hospital team, patients and families, or both for subsequent interviews.
deeper analysis of themes across ACO/SNF networks and enabled comparison by different factors, such as organization size, geographic location, and maturity of efforts into value-based care.
Results from the qualitative study informed the quantitative study analysis approach. The most frequently cited ACO processes influencing quality of care delivery within the SNF were derived to define the critical best practices influencing the primary outcomes of SNF LOS and readmission rate.
Second Coder Interrater Reliability
To ensure that there was a high correlation of interrater reliability, a second coder was engaged to code a significant proportion of the qualitative key informant interviews (McHugh, 2012). Second coding was performed in two groups: midway through the interview collection period and at the end of data collection. A total of eight transcripts were reviewed and second coded, totaling 10 key informants of the total of 47 participants. Of the 47 total interviews performed, the second coder addressed 8 total interviews and 10 of the key informant interview inputs to help alleviate any concern around the group interview experience encountered for participants from ACO E. In total, 21% of all intake data were second coded.
Methodology for the Phase 2 Quantitative Study
Themes obtained from key informant interviews in Phase 1 of the research study informed the quantitative portion of the research and included the following: data sharing with SNFs either individually or collectively, presence of an ACO clinical team member in the SNF to facilitate care transitions and execution of care, and patient/family/referring provider education at the time of SNF admission. As stated in the research hypothesis, an ACO/CMS contract leads to ACO/SNF relationship processes which lead to higher SNF quality which leads to better patient outcomes. For the purposes of this report, these relationship processes will be further distilled in nomenclature to the broader categories of data sharing, people, and education. All of the ACOs included in this study had confirmed policies and procedures that were implemented in their preferred SNF relationships. The presence of these ACO processes was confirmed and housed within the overarching theme of quality of SNF care delivery as shown in Figure 5.
FIGURE 5: Prevalent themes elicited from the qualitative study
SNF
QUALITY
Data
People
In order to define specific and successful ACO behaviors and determine how the
presence or absence of these processes influenced outcome metrics (LOS, readmission rates), the above themes were further distilled into binary yes/no questions to establish the presence or absence of best practices for quantitative analysis. The definition of preferred partners within this study is defined as the presence of a collaborative relationship between ACO and SNF. This relationship includes processes and procedures related to exchange of data, placement of staffing resources such as a Registered Nurse or Community Health Worker within the SNF to perform care coordination activities, and education for patients, families, and providers on the capability and services of the SNF at the time of transition (admission).
This framework, illustrated in Figure 6, is designed to address best practices for
ACO/SNF relationships and define specific and binary system processes that may influence the outcome variables of SNF LOS, readmission rate, and measurement of ED utilization from SNFs.
FIGURE 6: Framework for ACO/SNF relationship development
SNF
Quali
ty
Data
Collaborative Data Sharing (Y/N)If YES - Dependent Variable Analysis
People
Team based ACO care INSIDE SNF (Y/N)If YES - Dependent Variable Analysis
Education
Presence of an educational process/curriculum for transition from hospital to
SNF (Y/N)
Data sharing was repeatedly mentioned as important in the key informant interviews. Each ACO in the study cohort had some level of data sharing between ACO and SNF. In order to define those SNFs where data were exchanged with the ACO, a binary yes/no question was asked to confirm that the ACO was facilitating collaborative meetings and sharing data on cost and quality with the SNFs in their respective community.
People, defined as an ACO-affiliated case manager, registered nurse, or another health care delivery provider such as an ACO physician, nurse practitioner, or physician assistant was cited as a successful influencer on quality of care within the SNF and a defining variable for the resulting LOS for the patient. In order to define those SNFs where people were used to facilitate care, a binary yes/no question was asked to confirm that the ACO was facilitating team-based care inside the SNFs within their respective community.
Education was repeatedly emphasized from the key informants for both the hospital and transition team referring the patient to the SNF as well as patients and families as they chose the next setting of care. ACOs that created a defined curriculum for education at the points of
transition within the hospital and physician networks and that also had policies and procedures to educate patients and families toward SNFs with ACO relationships. In order to define those SNFs where education was part of the process of selection during patient transition, a binary yes/no question was asked to confirm that the ACO was following an educational process and sharing data on cost and quality for the SNFs in their respective community to assist with informed decision making for SNF selection.
were verified using the binary questions defining ACO processes with SNFs. Then, using a utilization report that examined the top 15 SNFs for each ACO, a quantitative analysis was performed on the dependent variables of readmission rate from SNF to hospital, LOS within the SNF, and ED utilization. These initial binary questions established a minimum baseline; some ACOs may be doing more or have additional processes in place, but the activities in Figure 6 were chosen as a minimum best practice for each ACO/SNF relationship as these behaviors were repeatedly mentioned by the key informants.
The unit of analysis is the SNF within each selected ACO. The themes of people, data, and education all contribute to the implementation and execution of quality care delivery inside the SNF and the presence or absence of specific ACO processes is thought to influence the outcomes of LOS, readmission rate, and ED utilization.
An example of a framework designed to address the quality of care within the SNF and the relationship to specific ACO processes and outcomes is illustrated in Figure 1B. The ACO entity will or will not perform specific processes that, if present or absent, will result in effects on patient health outcomes including ED utilization, LOS, or readmission back to the
discharging hospital. The presence of these activities around data, people, and education defines a preferred facility where the ACO has a relationship with the SNF and performs the binary processes. The non-preferred SNFs do not have the preferred relationship with the ACO and therefore do not experience the data exchange, staff resourcing, or education at the transition of care which may lead to their facility selection for patient admission.
additional variable contributing to SNF quality. While this study does not include patient-level analyses of satisfaction with individual SNFs, future directions for research considering patient-reported outcomes are recommended.
Data Sources
The national population health company where the investigator is employed has a data warehouse that stores CMS claims data as well as health system data such as patient charts within the electronic health record, laboratory data, imaging data, and patient demographics. This company also has a proprietary population health platform that can report workflow generated data identifying the presence or absence of specific clinical processes such as case management by a registered nurse or a referral to a social worker. Data sources included health systems identified as having an ACO contract with CMS and those that had an operating partner relationship with this national population health company.
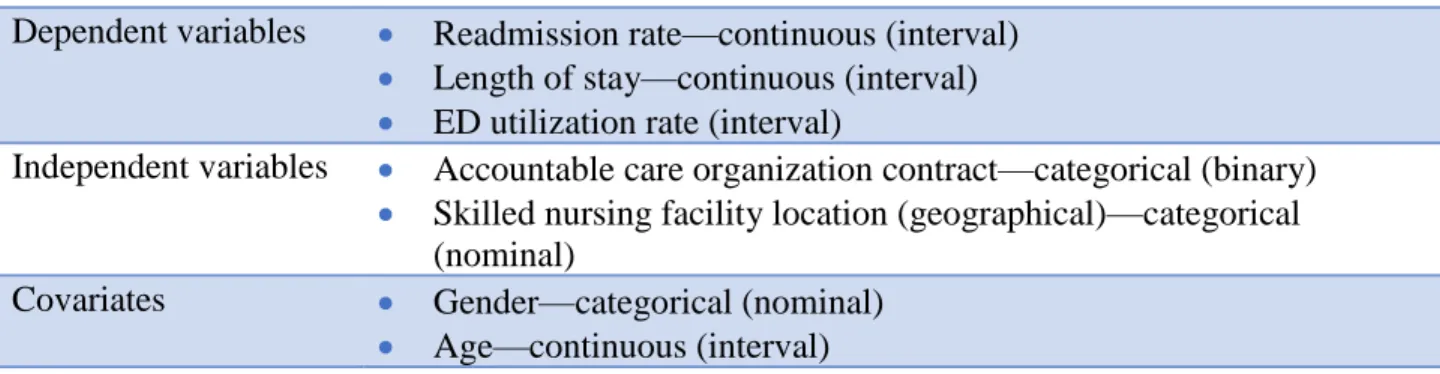
Initially proposed independent and dependent variables are defined in Table 5. The number of variables was intentionally kept small to address the descriptive correlation to themes by outcome as illustrated above.
TABLE 5: Independent and dependent variables
Dependent variables • Readmission rate—continuous (interval)
• Length of stay—continuous (interval)
• ED utilization rate (interval)
Independent variables • Accountable care organization contract—categorical (binary)
• Skilled nursing facility location (geographical)—categorical (nominal)
Covariates • Gender—categorical (nominal)
• Age—continuous (interval)
An analyst employed with the national company provided the cost and use reports as well as the summary results for the top 15 SNFs where ACO-attributed patients were admitted from January 2018 to September 2018 and reflected claims paid through December 2018. These SNFs were sorted by total cost to the ACO and query verification was made with the local ACO leadership team to obtain answers to the binary process questions around data, people, and education. SNFs that had affirmative answers in all three categories were classified as preferred for each ACO network and compared to those facilities that did not have those relational
processes and procedures present between ACO and SNF. The yes/no answers helped to address the research question, whether LOS, readmission rate, and ED utilization were different for patients admitted to preferred versus non-preferred SNFs. The author was blinded to all SNF patient names as well as identifiers for the parent ACO.
Data Analysis Plan