Bosn J Basic Med Sci 2014; 14 (2): 70-74Abstract
Surgical revascularization of the heart (CABG - coronary artery bypass grafting) is one way of treating coronary heart disease. Bleeding is one of the serious and frequent complications of heart surgery and can result in increased mortality and morbidity. Hemostasis disorder may be secondary consequences of surgical bleeding, preoperative anticoagulant therapy, and the use of cardiopulmonary bypass. Tests used for routine evaluation of the coagulation system are activated partial thromboplastin time (APTT) and international normalized ratio (INR). Th e study encountered patients who were hospitalized at the Clinic for Cardiovascular Diseases, University Clinical Center Tuzla. Patients underwent elective coronary artery bypass heart surgery either with cardiopulmonary bypass (on-pump CABG) or without it (off -pump CABG). Th e aim of this study was to compare the changes in coagulation tests (APTT, INR) in patients who were operated on-pump and pa-tients operated off -pump. Our study showed that the values of APTT and INR tend to increase immediately after surgery. Twenty-four hours after surgery these values are declining and they are approaching the preoperative values in all observed patients (p <.). Comparing APTT between the groups we found that postoperative APTT levels are signifi cantly higher in the group of patients who underwent surgery with cardiopulmonary bypass (p <.). Changes in coagulation tests after surgical revascularization of the heart are more pronounced in patients who were operated with on-pump technique compared to patients operated off -pump technique.
© Association of Basic Medical Sciences of FB&H. All rights reserved
KEY WORDS: CABG, on-pump, off -pump, APTT, INR
international normalised ratio after on-pump and
off -pump surgical revascularization of the heart
Lejla Selimović Čeke1*, Semir Imamović2, Farid Ljuca3, Zoran Jerkić1, Goran Imamović4,
Munevera Hadžimešić2, Aida Pojskić2, Jasmina Kovčić1
1Clinic for Cardiovascular Diseases, University Clinical Center Tuzla, Trnovac bb, 75000 Tuzla, Bosnia and Herzegovina. 2Clinic of
Anaesthesiology and Reanimatology, University Clinical Centre Tuzla, Trnovac bb, 75000 Tuzla, Bosnia and Herzegovina. 3Department
of Physiology, Faculty of Medicine, University of Tuzla, Univerzitetska 1, 75000 Tuzla, Bosnia and Herzegovina. 4Fresenius Medical Care
GmbH, Vrazova 22, 71000 Sarajevo, Bosnia and Herzegovina.
INTRODUCTION
Surgical revascularization of the heart (CABG coronary artery bypass grafting) is one way of treating coronary heart disease. CABG improves blood fl ow to the heart. Healthy artery or vein is used to bypass the occluded coronary artery. It creates a new path for blood fl ow to the heart muscle. Th e operation is performed with the use of cardiopulmonary bypass (CPB) called on-pump technique or without the use of CPB called off -pump technique. Opinions are still divided on which is
the better way. On-pump CABG procedure is performed while the heart is stopped. Th e blood supply must be provid-ed to the rest of the body when the heart is stoppprovid-ed. Th ere-fore, surgeons use the CPB as an artifi cial circulation system that does the work of the heart and the lungs. On-pump CABG today is a safe procedure that has a small risk of death and/or complications. Th e average risk of this procedure for a low-risk patient is to . Th e patient’s other health-threat-ening conditions increase these risks. Some of the important complications that can occur with this technique are stroke, kidney or liver failure, decrease in higher mental function, and bleeding. Th ese complications have been ascribed to the use of the pump and the need to manipulate both the heart and the large arteries to place the patient on CPB. Off -pump CABG is considered as the new method of performing CABG. Th e complications of on-pump CABG, spurred the develop-ment of this technique. Th is procedure is performed with the heart beating and without the use of the CPB. Grafts are * Corresponding author: Lejla Selimović Čeke,
Clinic for Cardiovascular Diseases, University Clinical Center Tuzla, Trnovac bb, 75000 Tuzla, Bosnia and Herzegovina Phone: +387 35 303 254
Fax: +387 35 265 411
e-mail: [email protected]
Bosn J Basic Med Sci 2014; 14 (2): 71-74
attached to the heart while it is constantly moving and fi lled with blood. Special devices can mechanically stabilize the rel-evant part of the heart so that the suturing can be performed on a relatively immobile platform. Th e risk of death and/or complications from off -pump CABG is also about to in a low-risk patient. Th e choice of procedure should depend on the comfort level of the surgeon performing the procedure on a particular patient because these two procedures seem equally eff ective []. Postoperative bleeding is common after heart surgery. Nearly of patients had increased postoper-ative bleeding, and required reoperation because of exces-sive bleeding []. Bleeding is one of the serious and frequent complications of heart surgery and can result in increased mortality and morbidity []. It can be caused by surgical error, disorder of hemostasis, or a combination of both. Hemostasis disorder may be secondary consequences of surgical bleed-ing, preoperative anticoagulant therapy and use of cardiopul-monary bypass. Hemostatic system consists of a coagulation system, endothelial cells, regulatory proteins, platelets and fi brinolysis []. Th ese elements work together to prevent the loss of blood from damaged blood vessels without occlud-ing the entire vessel. In some situations, this activation can spread to the entire body causing coagulation and throm-botic complication. Cardiac surgery, especially with the use of CPB leads to such a scenario []. CPB is, however, associated with massive activation of the infl ammatory and coagulation systems because of conversion to laminar fl ow, blood con-tact with the artifi cial bypass surface, cold cardiac ischemia and hypothermia. Th e causes of coagulopathy after CPB are reduced platelet function or count, excessive fi brinolysis, re-duced circulating levels of coagulation factors, hypothermia []. Development of cardiac immobilization techniques al-lows complete revascularization on the beating heart (off-pump). Th is strategy avoids infl ammation and hemostatic problems caused by CPB and reduce the pro-infl ammatory stimulus to sternotomy and the revascularization procedure itself. Tests used for routine evaluation of the coagulation sys-tem are activated partial thromboplastin time (APTT) and international normalized ratio (INR). APTT is used to screen for abnormalities of the internal factor coagulation pathway (reduction or defect factors VIII, IX, XI and XII), as well as the common path (fi brinogen, factors II, V, X). It is also used for monitoring heparin therapy. Normal values are - s. INR allows standardization of the results of the prothrombin test (PT) in diff erent laboratories. Normal values are from – . PT test is used to evaluate the activity of coagulation factors involved in an external way of coagulation (factor II, V, VII, X), assessment of synthetic liver function, control dose of oral anticoagulant therapy with coumarins. It mea-sures the time in seconds it takes to form fi brin. Th e activated clotting time (ACT) is the most commonly used functional
test to measure heparin anticoagulation during cardiac sur-gery. Th is test is based on the ability of whole blood to form a visible fibrin monomer within a glass tube. Studies that compared coagulation in on-pump versus off -pump CABG were done before [, ]. Th ese studies proved that coagula-tion is more disrupted after on-pump operacoagula-tion. Tests used in these studies are not routinely used. Th at's why our study is based on routinely used coagulation tests (APTT, INR). Th e aim of this study was to compare changes in APTT and
INR in patients operated by on-pump and off-pump tech-nique. In accordance with previous studies we hypothesis that postoperative levels of APTT and INR will be above ref-erent limit in both groups of patients. We expect that APTT and INR will be significalty higher in the on-pump group.
MATERIALS AND METHODS
Patients
The study was prospective in character and referred to the monitoring of changes in coagulation tests after surgi-cal revascularization of the heart. Th e sample included consecutive patients who were hospitalized at the Clinic for Cardiovascular Diseases University Clinical Center Tu-zla diagnosed with coronary artery disease. Patients under-went elective coronary artery bypass heart surgery. Writ-ten consent was obtained from all the patients included in the study. The study has been approved by the Local Ethic Committee. Investigations were carried out in accor-dance with the Declaration of Helsinki as revised in .
Procedures
protec-
Bosn J Basic Med Sci 2014; 14 (2): 72-74 tion was achieved with cold (°C) potassium cardioplegia. Inthe off -pump group, CABG was performed on the beating normothermic heart with local cardiac wall immobilization. Before the anastomosis was started, unfractionated heparin was administered ( IU/kg.b.w), followed by additional -IU of heparin to maintain ACT > s. Th e hepa-rin was reversed by the administration of protamin. We used a different target ACT for both procedures, because there were diff erent indications for the use of anticoagula-tion. Whereas in the on-pump group heparin was mainly used to prevent clotting in the CPB system, in the off -pump group it was needed to prevent clotting in the harvested in-ternal mammary arteries and in the native coronary system during grafting. Th e postoperative ACT after protamine in-fusion was the same in both groups (<). Hypothesizing that off -pump would not infl uence hemostasis, we decided to study the effects after the operation. Protamine sulfate binds to negatively charged unfractionated heparin. Th e re-sultant protamine-heparin complex is rapidly cleared by the reticuloendothelial system. Protamine is routinely adminis-tered postoperatively to reverse the high concentrations of heparin required for patients undergoing cardiac surgery. In group after completion of CPB, the heparin was reversed by administration of mg protamin/ IU of heparin. In group , patients received .-. mg protamine/ IU hepa-rin. If the ACT remained elevated following the initial dose of protamine, an additional dose of -mg protamine was given to decrease ACT <s. For ACT measurement we used Medtronic ACT II coagulation analyzer. Assessment of coagulation status of patients was done using coagulation tests: activated partial thromboplastin time (APTT) and in-ternational normalized ratio (INR). INR is the inin-ternational normalized value for prothrombin time (PT). For both tests we used automatical coagulation analyzer Siemens Sysmex CA-th System. The blood sample for analysis was ob-tained from the peripheral vein in a tube with anticoagulant sodium citrate and in the ratio of :, one part anticoagu-lant and nine parts of blood. As a reagent for the PT test is used Th romborel S, and for APTT Pathtromtin SL. Blood samples were collected preoperatively, at admission in inten-sive care unit (ICU) and the day after surgery. Time elapsed from sampling to analysis was not greater than one hour.
Statistical analysis
Statistical analysis was performed by using the Med-Calc for Windows version ... (MedMed-Calc Soft-ware, Mariakerke, Belgium) statistical package. The values were expressed as mean ± SEM. Two groups of con-tinuous variables with normal distribution of data were compared using ANOVA for repeated measures after their categorization. The level of significance was p <..
RESULTS
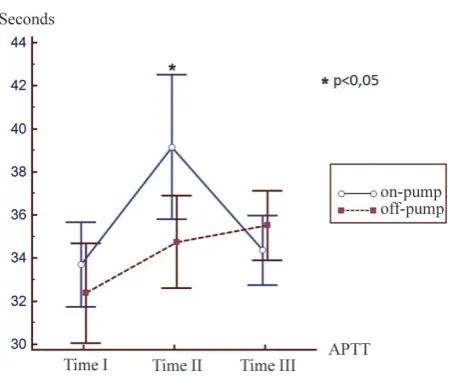
We randomly assigned patients who were scheduled for elective fi rst-time CABG to undergo the procedure either with cardiopulmonary bypass (on-pump CABG) or with-out it (off-pump CABG). In the on-pump group, () were female and () male, and the mean age was . ± . years. In the off -pump group, (.) individuals were female and (.) were male, with a mean age of . ± . years. Th ere were no signifi cant diff erences in the age or sex ratio between groups (Table ). In our study we compared the values of APTT and INR in patients oper-ated with the use of CPB (on-pump) and patients operoper-ated off-pump. Tests were performed before surgery (Time I), after admission in the ICU (Time II) and the day after sur-gery (Time III). Mean APTT levels were found to be signif-icantly higher in Time II compared to Time I and Time III in on-pump group. A signifi cant diff erence was not found between Time I and Time III in the on-pump group (Table ). In the off -pump group mean APTT levels were found to be significantly higher in Time I compared to Time III. A significant difference was not found between Time I and Time II in the off -pump group (Table ). Comparing APTT
On-pump Off -pump p
N 30 30
Age 59.47 ± 7.31 57.03 ± 7.56 1.0
Gender n % n %
Male 21 70.0 20 66.7 0.78
Female 9 30.0 10 33.3 0.78
TABLE 1. Demographic characteristics of patients
Variable Time I Time II Time III
APTT (N=30) 33.70±0.96* 39.16±1.63** 34.36±1.37 INR (N=30 1.07±0.019*** 1.43±0.04**** 1.19±0.022 TABLE 2. Changes in APTT and INR in the on-pump group
Values are expressed as mean ± SEM. APTT activated partial thrombo-plastin time; INR International Normalization Ratio; Time I – preoperative; Time II –after admission in intensive care unit; Time III –24 hours after the operation; * p <0.05 Compared to Time II; ** p <0.05 Compared to Time III; *** p <0.05 Compared to Time II and Time III; ****p <0.05 Compared to Time III.
Variable Time I Time II Time III
APTT (N=30) 32.38±1.13* 34.75±1.05 35.51±0.79 INR (N=30) 1.13±0.02** 1.31±0.064*** 1.18±0.016 TABLE 3. Changes in APTT and INR in the off -pump group
Bosn J Basic Med Sci 2014; 14 (2): 73-74
between the groups we found mean APTT levels in Time II to be signifi cantly higher in the on-pump group (Figure ). Mean INR levels were found to be significantly higher in Time II compared to Time I and Time III in the on-pump group (Table ). Mean INR levels were found to be signifi -cantly higher in Time II compared to Time I in the off -pump group. In the off -pump group mean INR levels were found to be significantly higher in Time III compared to Time I (Table ). Comparing INR between the on-pump and off-pump group, signifi cant diff erence was not found (Figure ).
DISCUSSION
APTT and INR are used as a routine tests to check patient´s coagulation system. APTT is most commonly used for monitoring anticoagulation therapy with heparin. Various studies have measured APTT following cardiac surgery and have found it to be commonly elevated [-]. Some stud-ies have shown a positive correlation between APTT and postoperative hemorrhage following cardiac surgery [-]. Our study showed prolonged APTT and INR after the surgery despite neutralization of heparin with protamine. Our fi ndings are in accordance with other studies that have shown massive activation of hemostasis during and early after cardiac surgery performed with the use of CPB [,]. APTT was more elevated in patients who underwent surgery with the use of CPB. After the operation, when patients were received in the ICU, APTT values were higher than nor-mal in the majority of patients operated with the on-pump technique. APTT was slightly higher in patients operated with the off -pump technique, but signifi cant diff erence was not found. Twenty-four hours after surgery APTT values in
both groups of patients decreased to preoperative values. In the on-pump group, statistically signifi cant diff erence was not found between preoperative values and values hours after the operation. In the off pump group we found signifi -cant diff erence between those two measurements. Th is can be explained by “heparin rebound” phenomenon. ”Hepa-rin rebound” phenomenon usually occurs - hours after neutralization of heparin with protamine []. This phe-nomenon is often attributed to reappearance of circulating heparin. Th eories accounting for “heparin rebound” include late release of heparin sequestered in tissues, delayed return of heparin to the circulation from the extracellular space via lymphatics, clearance of an unrecognized endogenous heparin antagonist, and more rapid clearance of protamine in relation to heparin [,]. Ravi Taneja and colleagues showed that in the majority of patients APTT was increased postoperatively but according to their research it is not due to “heparin rebound” phenomenon []. Th ey speculate that elevated APTT may have been related, at least in part, to an excessive protamine dose in an attempt to reverse heparin. Higher APTT values after heart surgery can be explained by hemodilution and reduction of coagulation factors by in patients operated with CPB, whereas in patients operated with the off-pump technique due to increased consump-tion intraoperatively and postoperatively []. According to some studies large doses of protamine can increase APTT values []. Agnese Ozolina in her study also found that after heart surgery APTT was increased, but increased APTT was not correlated with increased postoperative bleeding []. INR values showed the least change in both groups of pa-tients. After surgery in patients operated with cardiopulmo-nary bypass INR was slightly elevated. Th is is consistent with FIGURE 1. Comparison of APTT changes between on-pump and
off -pump group
Time I – preoperative APTT; Time II – APTT after admission in in-tensive care unit; Time III – APTT 24 hours after the operation; * p <0.05 – Time II on-pump compared to Time II off -pump.
FIGURE 2. Comparison of INR changes between on-pump and off -pump group
Bosn J Basic Med Sci 2014; 14 (2): 74-74 previous studies []. In patients operated by the off - pumptechnique the average value of INR after operation was nor-mal. Pawan K et al showed that preoperative INR greater than aff ects postoperative bleeding []. In our study, all patients had preoperative INR less than . Comparing INR between the groups, statistically signifi cant diff erence was not found.
CONCLUSION
This study has shown that surgical revascularization of the heart leads to prolonged coagulation tests (APTT and INR) above the reference value. These tests are used to routinely check internal, external and common co-agulation pathway. APTT and INR after the operation are above referent limit in both groups of patients. This indicates that there is a disorder of coagulation in terms of hypocoagulability. APTT values are significantly more elevated in patients operated with the use of CPB, indicat-ing that hypocoagulability is more pronounced in these patients. Hypocoagulability increases the risk for massive postoperative bleeding and the need for blood transfusion.
DECLARATION OF INTEREST
Th e authors declared no confl icts of interest.
REFERENCES
[] Shekar PS. On-pump and off -pump coronary artery bypass grafting. Circulation ; ():e-e.
[] Karkouti K, Wijeysundera DN, Yau TM, Beattie WS, Abdelnaem E, McCluskey SA. et al. Th e independent association of massive blood loss with mortality in cardiac surgery. Transfusion ; : -.
[] Paparella D, Brister SJ, Buchanan MR. Coagulation disorders of cardiopulmonary bypass: a review. Intensive Care Med. ; ():-.
[] Guyton AC, Hall JE. Textbook of Medical Physiology, th ed. Else-vier Saunders, .
[] Sniecinski RM, Chandler WL. Activation of the hemostatic system during cardiopulmonary bypass. Anesth Analg. ;():- .
[] Casati V, Gerli C, Franco A, Della Valle P, Benussi S, Alfi eri O, et al. Activation of coagulation and fibrinolysis during coronary surgery: on-pump versus off-pump techniques. Anesthesiology ;:–.
[] Lo B, Fijnheer R, Castigliego D, Borst C, Kalkman CJ, Nierich AP. Activation of hemostasis after coronary artery bypass grafting with or without cardiopulmonary bypass. Anesth Analg ;;-.
[] Ramsey G, Arvan DA, Stewart S, Blumberg N. Do preoperative laboratory tests predict blood transfusion needs in cardiac opera-tions? J Th orac Cardiovasc Surg ; : –.
[] Nuttall GA, Oliver WC, Beynen FM, Santrach PJ, Strickland RA,Murray MJ.Determination of normal versus abnormal activat-ed partial thromboplastin time and prothrombin time after cardio-pulmonary bypass. J Cardiothorac Vasc Anesth ; : –. [] Nuttall GA, Oliver WC, Ereth MH, Santrach PJ. Coagulation tests
predict bleeding after cardiopulmonary bypass. J Cardiothorac Vasc Anesth ; : –.
[] Blome M, Isgro F, Kiessling AH, Skuras J, Haubelt H, Hellstern P. et al. Relationship between factor XIII activity, fi brinogen, haemosta-sis screening tests and postoperative bleeding in cardiopulmonary bypass surgery. Th romb Haemost ; : –.
[] Despotis GJ, Filos KS, Zoys TN, Hogue CW Jr, Spitznagel E, Lap-pas DG. Factors associated with excessive postoperative blood loss and hemostatic transfusion requirements: a multivariate analysis in cardiac surgical patients. Anesth Analg ; :–.
[] Milas B, Jobes D, Gorman R. Management of bleeding and coagu-lopathy after heart surgery. Semin Th orac Cardiovasc Surg ; :.
[] Frick PG, Brogli H. Th e mechanism of heparin rebound after ex-tracorporeal circulation for open cardiac surgery. Surgery ; ():-.
[] Gravlee GP, Arora S, Lavender SW, Mills SA, Hudspeth AS, Cordell AR. et al. Predictive value of blood clotting tests in cardiac surgical patients. Ann Th orac Surg ; : –.
[] Subramaniam P, Skillington P, Tatoulis J. Heparinrebound in the early postoperative phase following cardiopulmonary bypass. Aust N Z J Surg. ; (): –.
[] Taneja R, Marwaha G, Sinha P, Quantz M, Stitt L, Gao R. et al. Ele-vated actiEle-vated partial thromboplastin time does not correlate with heparin rebound following cardiac surgery. Can J Anaesth. ; ():-.
[] Chandler WL. Eff ects of hemodilution, blood loss, and consump-tion on hemostatic factor levels during cardiopulmonary bypass. J Cardiothorac Vasc Anesth. ; (): –.
[] Inagaki M, Goto K, Katayama H, Benson KT, Goto H, Arakawa K. Activated partial thromboplastin time-protamine dose relation in the presence and absence of heparin. J Cardiothorac Anesth, ; (): –.
[] Ozolina A, Strike E, Sondore A, Vanags I. Coagulation tests and their association with postoperative blood loss after cardiac sur-gery with cardiopulmonary bypass. Acta Medica Lituanica. ; (); –.
[] Tettey M, Aniteye E, Sereboe L, Edwin F, Kotei D, Tamatey M. et al. Predictors of post operative bleeding and blood transfusion in cardiac surgery. Ghana Med J. ; (): -.