Cost-effectiveness Analysis of a Mobile Phone SMS Text-based
Smoking Cessation Intervention
Jabali Wells, MD, MSc, University of Chicago Booth School of Business; Chicago, IL, USA Ananth Srinath, MSc, Sri Shankara Cancer Hospital and Research Centre; Banglore, India
Caroline Free, MBChB, MRCGP, DRCOG, PhD, London School of Hygiene and Tropical Medicine, Department of Nutrition and Public Health Intervention Research; London, UK
Gareth Forde, MD, PhD, Michigan State University, Department of Obstetrics and Gynecology, Grand Rapids, Michigan Colin Forde, PhD, University of South Florida; Tampa, Florida
Introduction
A
dverse health effects from tobacco consumption have been extensively investigated in the last half century. However, despite this, smoking still remains one of the most widely studied public health issues. It has been esti-mated that in excess of one billion people consume cigarettes globally,1 with 10% of all deaths worldwide beingsmoking-related.2 Within the United Kingdom (UK), greater than
20% of the adult population use tobacco products, with half of those who smoke at least one pack of cigarettes per day being at risk of death from tobacco-related diseases.3 In fact,
consumption of cigarettes and other tobacco products is the primary risk factor in 7 of the 10 leading causes of mortality in England and Wales.4
While the overall prevalence of tobacco consumption in the UK has been declining in recent years,3 young adults and
those from lower socioeconomic groups continue to have the highest rates of smoking.5,6 In fact, the majority of regular
smokers in the UK admit to commencing their habit prior to the age of 20 years.7 Consequently, most cessation campaigns
and public policy initiatives related to tobacco consumption target younger smokers. Even though the speed and degree of morbidity and mortality reduction that results from smok-ing cessation is debated,8 research indicates that smoking
cessation among younger adults produces greater accrued public health and economic benefits than smoking cessation among older adults.9
Even so, there is no defined protocol for a long-term smoking cessation intervention in the UK. The National In-stitute for Clinical Excellence (NICE) does, however, provide guidelines for several short-term cessation treatments to be taken in the weeks following a pre-determined quit date.10
These pharmacologic therapies (including buproprion, nico-tine replacement therapy, and varenicline) have been shown to be effective in randomized trials. Nevertheless, the high rate of medication non-adherence among younger individu-als limits their effectiveness in clinical practice.11 Conversely,
NICE also recommends non-pharmacologic counseling in-terventions that may confer sustainable cessation as a result of behavioral modification, with therapies ranging from self-help books and literature, to high-frequency individual and group counseling sessions. Despite the reported effectiveness
Corresponding Author: Jabali Wells, MD, MSc University of Chicago Booth School of Business Chicago, IL, USA
Email: [email protected]
Abstract
Objective: To examine the cost-effectiveness of a mobile phone SMS text-based smoking cessation intervention of young adult smokers in the United Kingdom.
Design: A Markov model was constructed to exam-ine data from British and international literature. The SMS text-based intervention is compared with a NHS behavioral modification smoking cessation program.
Setting: Community setting in the United Kingdom. Participants: 200 people, average age of 37, in the London metropolitan area.
Main Outcome Measures: Cost per life years gained.
Results: The SMS text-based smoking intervention is more advantageous from the health care payer and societal viewpoints. Sensitivity analyses illustrate robust results. The incremental cost-effectiveness ratio (ICER) is£1.86 per life year gained, far be-low the NICE willingness to pay cost-effectiveness threshold of £20,000.
of intensive group and individual counseling-based cessation programs,12 younger smokers are frequently reluctant to
en-gage in these interventions due to lack of interest and fear of peer ridicule and non-acceptance.14 Ultimately, gains in
pub-lic health initiatives such as smoking cessation intervention programs have been impeded by a lack of a comprehensive mechanism for evaluating such programs. Complex interven-tions that incorporate policy considerainterven-tions, environmental factors, and individual patient-centered components should be assessed with measurements suited to their settings, goals, and purpose.14
SMS text-based smoking cessation interventions using mo-bile devices represent a new and innovative mode of facili-tating behavioral modification. Much like counseling-based schemes, an SMS text intervention is a motivational tool that promotes adherence to cessation goals with the use of positive reinforcement to modify unwanted responses to stimuli that facilitate smoking behavior.15 Also, SMS texting interventions
have the additional benefit of being an inexpensive mode of delivering interactive personalized messages at any given time, to almost anyone with a mobile device. Even more, the number of mobile phones in the UK now exceeds the num-ber of people in the country, with 70% of mobile phone users being 40 years of age or below.16 Thus, SMS text-based
smok-ing interventions possess tremendous potential to decrease smoking behavior and tobacco-related illness. Research that analyzes the effectiveness of text-based cessation programs is growing, with several recent studies in the US and New Zea-land demonstrating statistically significant short-term increas-es in abstinence.17 Free et al.18 examined the effectiveness of
an SMS text-based smoking cessation intervention in the UK and demonstrated significant increases in smoking cessation rates in the short-term. Utilizing the data from the Free et al.18
Txt2Stop randomized clinical pilot trial, this study aims to as-sess the cost-effectiveness of a texting intervention.
Methods
Design
Using Microsoft Excel, a Markov model was constructed to assess the cost and effectiveness of a SMS-text based smoking cessation intervention to a combined individual and group counseling-based smoking cessation program that adheres to NICE guidelines (Figure 1). Markov models are useful in representing a changing health state over time, when there is a known probability of shifting from one health state to the next. Markov cycles were 1-month in duration, with an ini-tial half-cycle correction. Due to the fact that there is a time value of money, direct and indirect costs associated with the TxT2Stop intervention were discounted to determine their present value. Thus, a discount rate of 3.5 percent was used according to the recommendations of a NICE-commissioned panel for economic evaluation of smoking cessation treat-ments.19
First, a cohort of 200 smokers, with an average age of 37 years, and located in the London metropolitan area was eval-uated. All participants commenced within a health state that was characterized by a desire to quit smoking, and were given
£50 at the conclusion of the study. Participants were random-ly allocated into the Text2Stop intervention or the NHS be-havioral modification program after determining a quit date. Smoking cessation was evaluated via participant self-reports at one-month following quit date, and by salivary cotinine test at six-months following quit date.
At one-month following the quit date, there is a given probability of progressing into either a state of cessation or relapse. Of those who have abstained after one-month, there are concomitant probabilities of moving into a terminal state of cessation, or state of relapse at six-months. At both one-month and six-one-months following quit date, cohorts who have relapsed incur respective probabilities of moving into a termi-nal state of cessation-after-relapse, or a state of relapse-after-relapse. Finally, for those in the relapse-after-relapse state, there is a given probability of progressing to a terminal state of cessation-following-relapse, or a terminal state of contin-ued smoking. Inevitably, these states are representative of the recurring, relapsing nature of smoking behavior that is de-fined by chronic nicotine dependence.20
Figure 1.
Probability Data
The transitional probabilities in the Markov model have been obtained from several data sources, including published literature and the public domain (Table 1). Probabilities for the Txt2Stop intervention were taken from the results of the
Free et al.18 randomized controlled pilot study. Because the age
are most likely to utilize mobile devices,16 age-adjustment of
the smoking cessation probabilities in the Txt2Stop treat-ment was unnecessary. Alternatively, smoking cessation prob-abilities for the NHS counseling-based intervention could not be ascertained from published trials (Table 2). Rather, these probabilities were acquired from articles referenced in litera-ture reviews, case studies, and population studies.21,22 In
ad-dition, probabilities related to behavioral modification inter-ventions that were unavailable in the UK public domain were obtained in US public health databases.23 Although tobacco
consumption in the UK is higher than that of the US, age, gender and socioeconomic distributions of individuals who smoke are quite similar in these two countries.2 As a result,
the use of US-based probabilities were assumed to be viable, equivalent substitutes in lieu of unattainable UK-based data.
Table 1. Txt2Stop Intervention*
Health State Probability
$FTTBUJPOBUXFFLTBGUFSRVJUEBUF 3FMBQTFBUXFFLTBGUFSRVJUEBUF $FTTBUJPOBUNPOUITBGUFSRVJUEBUF 3FMBQTFBUNPOUITBGUFSRVJUEBUF
%BUBGSPN'SFFFUBM TUVEZ
1BSUJDJQBOUTXIPEJEOPUGPMMPXVQXFSFUSFBUFEBTDPOUJOVJOHTNPLFSTXIPSF-lapsed
Markov* Node Health State Probability
Relapse-after-relapse $FTTBUJPOBGUFSSFMBQTF
.BSLPWDZDMFNPOUI
*OJUJBMIBMGDZDMFDPSSFDUJPO*ODSFNFOUBMmOBM 1BSSPUUFUBM
Table 2. Counseling-based Intervention
Health State Probability
$FTTBUJPOBUXFFLTBGUFSRVJUEBUF 3FMBQTFBUXFFLTBGUFSRVJUEBUF $FTTBUJPOBUNPOUITBGUFSRVJUEBUF 3FMBQTFBUNPOUITBGUFSRVJUEBUF
64%FQBSUNFOUPG1VCMJD)FBMUI4FSWJDFT -BODBTUFSBOE4UFBE
Markov* Node Health State Probability
Relapse-after-relapse $FTTBUJPOBGUFSSFMBQTF
.BSLPWDZDMFNPOUI
*OJUJBMIBMGDZDMFDPSSFDUJPO*ODSFNFOUBMmOBM 1BSSPUUFUBM
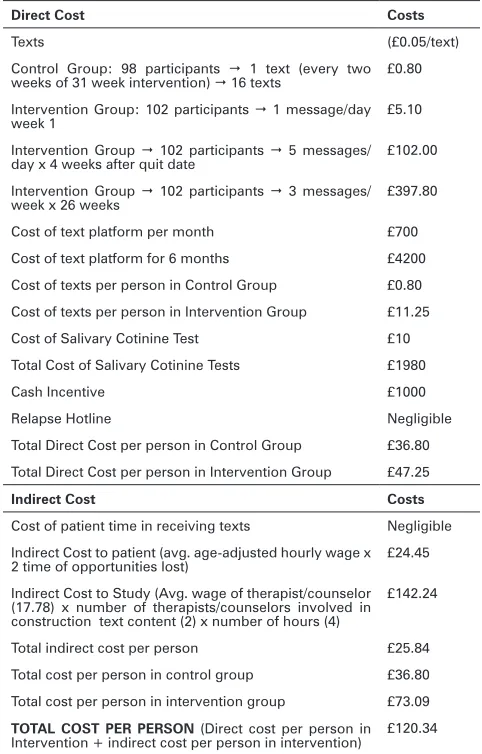
Cost Data
Direct costs associated with the Txt2Stop intervention were obtained from the lead investigator of the study. The capital costs of the study are illustrated in Table 3, and includ-ed the monthly platform maintenance of the text program, as well as the total costs of texts sent to participants. Other direct costs consisted of the salivary cotinine tests, and cash incentives given to participants whose cotinine test confirmed self-reports of smoking cessation. Although a relapse support
hotline that was made available to participants could be in-cluded as a direct cost, the lead investigator noted this expen-diture as being negligible. Conversely, indirect costs to the study, such as those related to the remuneration of therapists and counselors who constructed text message content, were obtained from the calculation of various labor statistics that were obtained in the public domain.24 Furthermore, indirect
costs to participants were determined from public records of wage surveys that were used to estimate time and value of forgone opportunity costs to participate in the Txt2Stop in-tervention.25
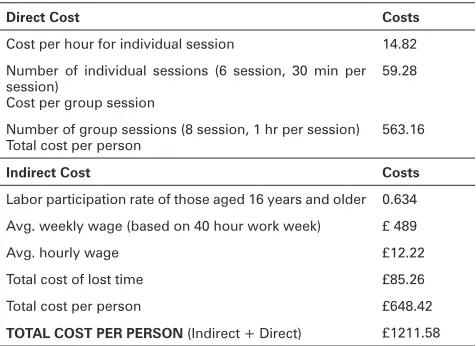
Capital costs associated with the NHS counseling-based smoking cessation intervention were readily accessible in the public domain (Table 4). These costs, which are commensu-rate with the wages of the counselors delivering the interven-tion, were detailed in national guidelines that provide a cost-ing template for program implementation.26 Equally, indirect
costs of the counseling-based program had to be obtained from labor statistics in the public domain.25 In the end,
aver-age aver-age-adjusted hourly waver-ages of participants were used to estimate the opportunity cost of hours forgone to be involved in the intervention.
Table 3. Txt2Stop Intervention
Direct Cost Costs
Texts bUFYU
$POUSPM (SPVQ QBSUJDJQBOUT 1 text (every two weeks of 31 week intervention) UFYUT b *OUFSWFOUJPO(SPVQQBSUJDJQBOUT NFTTBHFEBZ
week 1 b
Intervention Group QBSUJDJQBOUT NFTTBHFT
EBZYXFFLTBGUFSRVJUEBUF b
Intervention Group QBSUJDJQBOUT NFTTBHFT
XFFLYXFFLT b
Cost of text platform per month b $PTUPGUFYUQMBUGPSNGPSNPOUIT b Cost of texts per person in Control Group b Cost of texts per person in Intervention Group £11.25 Cost of Salivary Cotinine Test b Total Cost of Salivary Cotinine Tests b
Cash Incentive b
Relapse Hotline Negligible
Total Direct Cost per person in Control Group b Total Direct Cost per person in Intervention Group b
Indirect Cost Costs
Cost of patient time in receiving texts Negligible Indirect Cost to patient (avg. age-adjusted hourly wage x
2 time of opportunities lost) b *OEJSFDU$PTUUP4UVEZ "WHXBHFPGUIFSBQJTUDPVOTFMPS Y OVNCFS PG UIFSBQJTUTDPVOTFMPST JOWPMWFE JO DPOTUSVDUJPOUFYUDPOUFOU YOVNCFSPGIPVST
b
Total indirect cost per person b Total cost per person in control group b Total cost per person in intervention group b
Table 4. Counseling-based Intervention
Direct Cost Costs
Cost per hour for individual session
/VNCFS PG JOEJWJEVBM TFTTJPOT TFTTJPO NJO QFS
session)
Cost per group session
Number of group sessions (8 session, 1 hr per session)
Total cost per person
Indirect Cost Costs
-BCPSQBSUJDJQBUJPOSBUFPGUIPTFBHFEZFBSTBOEPMEFS "WHXFFLMZXBHF CBTFEPOIPVSXPSLXFFL £
Avg. hourly wage £12.22
Total cost of lost time £
Total cost per person b
TOTAL COST PER PERSON (Indirect + Direct) £1211.58
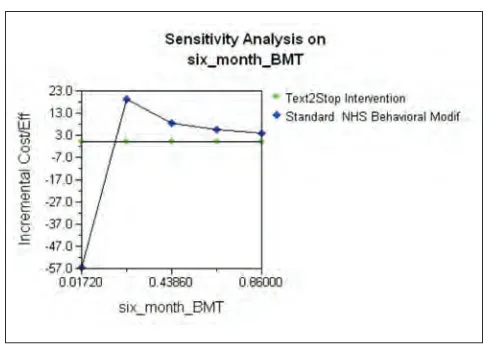
Effectiveness Data
An array of one-way sensitivity analyses was utilized on eight variables to demonstrate the strength of model on the cost-effectiveness of treatments (Table 5). Additionally, one-way sensitivity analyses were all run using one the variables set at an extreme value within the range of sensitivity. Not to mention, all analyses were completed using a willing to pay benchmark of £20,000 per QALY gained.27
Table 5. Sensitivity Analysis
Base Lower
Threshold UpperThreshold
Cessation after relapse
XFFLDFTTBUJPOXDPVOTFMJOHJO
-tervention
XFFL DFTTBUJPO X5YU4UPQ JO
-tervention 1.275
NPOUI DFTTBUJPO XDPVOTFMJOH
intervention
NPOUIDFTTBUJPOX5YU4UPQ
Discount rate
Time horizon
Txt2Stop costs
Counseling intervention costs
Counseling intervention _LYG
Txt2Stop_LYG
$POmEFODF*OUFSWBMPSUPUJNFTCBTF 8JMMJOHOFTTUPQBZUISFTIPMEbQFS2"-:HBJOFE
Results
The analysis reveals that both the SMS text-based smoking cessation intervention and the NHS behavioral modification smoking cessation scheme lie below the NICE willingness to pay cost-effectiveness threshold of £20,000. Nonetheless, the SMS text-based smoking intervention is less expensive with an estimated cost of £120.34 per person, compared with a projected £1211.58 per person cost for the NHS behavioral modification smoking cessation program. Conversely, expect-ed life-years gainexpect-ed are greater for an individual who partici-pates in the NHS intervention (1300), as opposed to a smoker who quits as a result of utilizing the SMS text-based program
(708). Thus, the NHS intervention is more effective, but the SMS text-based intervention is less costly. Still, when evaluat-ing both cost and effectiveness data, the SMS text-based ap-proach is more cost-effective because each additional GBP spent using this intervention will yield better value for money when compared to the NHS program.
A tornado diagram was constructed to compare the rela-tive importance of the different variables (Figure 11). The sensitive variables were modeled as uncertain values, while the other variables were maintained at stable baseline numbers to examine the net monetary benefit (vertical line). The NICE willingness to pay cost-effectiveness threshold of <20,000 is not violated. The results of the other sensitivity analyses are illustrated in Figures 2-10.
Figure 2.
Figure 3.
Figure 5.
Figure 6.
Figure 7.
Figure 8.
Figure 9.
Figure 11.
Discussion
Research has only begun to transition from investigating the clinical feasibility of mHealth interventions through ran-domized control trials to studies analyzing their economic im-pact. Our work is one of the first cost-effectiveness analyses of a mobile health intervention. Moreover, we have shown that a SMS text-based smoking cessation program is relatively inexpensive and effective in yielding short-term smoking ces-sation rates. However, for the duration of this investigation, we assumed that long-run average direct and indirect costs remain constant as output is increased. In reality, capital expenditures for novel technologies can have a significant impact on direct and indirect costs in the long-run. Being that this study illustrates SMS text-based smoking cessation interventions increase self-reported quitting in the short-term, transaction costs (including opportunity costs) have the propensity to create a barrier to the adoption of mobile health interventions. Nevertheless, recent evidence demon-strates that text-based smoking cessation programs achieve biochemically verified continuous abstinence at 6 months after quit date.28 These findings suggest that SMS text-based
interventions should be considered for inclusion in smoking cessation programs, as investments in these novel technolo-gies may achieve economies of scale.
Future investigations of SMS text-based smoking cessation interventions will also require improving the limitations of our research. First, the sample size of our study was quite small. Subsequent projects will need a larger sample to con-fer statistical power and increased internal validity. Essential-ly, the primary challenge to maintaining a large sample size is the loss of participants in follow-up. It is for this reason that participants were given a financial incentive to follow-up and submit a confirmatory salivary cotinine test. Hence, future studies will require the use of innovative methods to keep participants engaged, and to ensure follow-up and collection of data. Not to mention, increased participant follow-up is also necessary for any studies that may attempt to illustrate long-term advantages (i.e. six months or greater) of SMS text-based programs. In the end, the utilization of mobile health technologies in the delivery of healthcare appears to be ro-bust. The ubiquity of mobile devices, the ease of their use,
and the low costs of mobile-based interventions are advanta-geous for widespread adaptation.
References
1. World Bank (1999). Curbing the Epidemic: Governments and the Eco-nomic of Tobacco Control. The International Bank for Reconstruction and Development, World Bank, Washington D.C.
2. World Health Organization (2002). The World Health Report. Reducing Risks, Promoting Health Life. World Health Organization, Geneva. 3. National Health Service (2008). Statistics on Smoking: England, 2008.
In-formation Centre of the National Health Service (ICNHS).
4. Griffiths C., Rooney C., Brock A. (2005). Leading causes of death in Eng-land and Wales-how should we group causes? Health Statistics Quarterly 1: 6-17.
5. Simpson C., Hippisley-Cox J., Sheikh A. (2010). Trends in the epidemiol-ogy of smoking in the United Kingdom. British Journal of General Practice 60(572): e121-e127.
6. National Cancer Research Institute (2008). Beyond Smoking Kills: Protect-ing Children, ReducProtect-ing Inequalities. Action on SmokProtect-ing and Health. Lon-don, United Kingdom.
7. Goddard E. (2008). General household survey 2006: smoking and drinking among adults. UK Office for National Statistics.
8. Critchley J., Capewell S. (2003). Mortality Risk Reduction Associated with Smoking Cessation in Patients with Coronary Heart Disease. Journal of the American Medical Association 290(1): 86-97.
9. Bolin K., Borgman B., Gip C., Wilson K. (2011). Current and future avoid-able cost of smoking-Estimates for Sweden 2007. Health Policy 103(1): 83-91.
10. U.K. National Institute for Health and Clinical Excellence. Smoking ces-sation services (PH10). http://www.nice.org.uk/PH010 (last accessed 4/29/12).
11. Taddeo D., Egedy M., Frappier J.Y. (2008). Adherence to treatment in ado-lescents. Pediatric Child Health 13(1): 19-24.
12. Lancaster T., Stead L., Silagy C., Sowden A. (2000). Effectiveness of inter-ventions to help people stop smoking: findings from the Cochrane Library. British Medical Journal 321: 355-8.
13. Rigotti N., Lee J., Wechsler H. (2000). U.S. college students’ use of tobacco products: results of a national survey. Journal of the American Medical As-sociation 284: 699-705.
14. Glasgow R., Vogt T., Thomas M., Boles S. (1999). Evaluating the Public Health Impact of Health Promotion Interventions: The RE-AIM Frame-work. American Journal of Public Health 89(9): 1322.
15. Bauer S., Percevic R., Okon E., Meerman R., Kordy H. (2003). Use of text messaging in the after-care of patients with bulemia nervosa. European Eat-ing Disorders Review 11(3): 279-90.
16. Mobile Data Association (2009). MDA Q4 2009 UK Mobile Trends Report. 17. Fjeldsoe B., Marshall A., Miller Y. (2009). Behavior Change Interventions
Delivered by Mobile Telephone Short-Message Service. American Journal of Preventive Medicine 36(2): 165-73.
18. Free C., Whittaker R., Knight R., Abramsky T., Rogers A., Roberts I.G. (2009). Txt2Stop: a pilot randomized controlled trial of mobile phone-based smoking cessation support. Tobacco Control 18: 88-91.
19. York Health Economics Consortium (2007). NICE Cost Effectiveness of Interventions for Smoking Cessation. http://www.nice.org.uk/nicemedia/ live/11925/41100/41100.pdf (last accessed 4/29/12)
20. Agboola S., Coleman T., McNeill A. (2009). Relapse prevention in the UK Stop Smoking Service: a qualitative study of health professionals’ views and beliefs. BioMed Central Health Services Research 9:67.
21. Lancaster T. and Stead L. (2002). Individual behavioral counseling for smoking cessation. Cochrane Database of Systematic Reviews 3:CD001292. 22. Parrott S., Godfrey C., Raw M. (1998). Guidance for Commissioners on the
Cost-Effectiveness of Smoking Cessation Interventions. Thorax 53:S2-37. 23. U.S. Department of Public Health Service (2008). Clinical Practice
Guide-lines, Treating Tobacco Use and Dependence: 2008 Update. U.S. Depart-ment of Health and Human Services, Washington, DC.
24. UK Office for National Statistics (2010). Statistical Bulletin: Labor market statistics.
25. UK Office for National Statistics (2009). Annual Survey of Hourly Earnings. 26. National Institute for Health and Clinical Excellence (2008). Smoking cessation service costing template for implementing NICE guidelines. Na-tional Health Service. United Kingdom.
27. Appleby J., Devlin N., Parkin D. (2007). NICE’s cost effectiveness threshold. British Medical Journal 335: 338-9.