Gaps in the Implementation of Shared
Decision-making: Illustrative Cases
Elliott Mark Weiss, MD, MSME,a,bJonna D. Clark, MD,a,bCarrie L. Heike, MD, MS,bAbby R. Rosenberg, MD, MA, MS,a,b Seema K. Shah, JD,cBenjamin S. Wilfond, MD,a,bDouglas J. Opel, MD, MPHa,b
abstract
Shared decision-making (SDM) has emerged as the preferred decision-making model in the clinician-patient relationship. Through collaboration, SDM helps to facilitate evidence-based medical decisions that are closely aligned with patient or surrogate preferences, values, and goals. How to implement SDM in clinical pediatric practice, however, remains elusive, in part because SDM in pediatrics is complicated by the involvement of parents as a special class of surrogate decision-maker. A provisional framework for the process of SDM in pediatrics was recently proposed by Opel to help facilitate its implementation. To identify aspects of the framework that require refinement, we applied it across a diverse range of clinical cases from multiple pediatric specialties. In doing so, several questions surfaced that deserve further scrutiny: (1) For which medical decisions is consideration of SDM required? (2) What is considered medically reasonable when there is variability in standard practice? (3) Can an option that is not consistent with standard practice still be medically reasonable? (4) How should public health implications be factored into SDM? (5) How should variability in preference sensitivity be approached? (6) How should the developing autonomy of adolescents be integrated into SDM?; and (7) How should SDM address parental decisional burden for emotionally charged decisions? We conduct a brief analysis of each question raised to illustrate key areas for future research.
Shared decision-making (SDM) is a process in which clinicians and patients“share information…take steps to build a consensus about the preferred treatment; and [reach an agreement] on the treatment to implement.”1It has emerged as the preferred decision-making model for the clinician-patient relationship.2,3The paramount goal of SDM is to facilitate sound medical decisions that are aligned with patient or surrogate preferences, values, and goals. Although there is consensus for SDM as
a concept, there is not consensus regarding how to practice it: When should it be used? How should it manifest? What needs to be shared?4,5 Our goal in this article is not to resolve
these questions but rather to illustrate how they appear in clinical decision-making to stimulate future research in SDM in pediatrics.
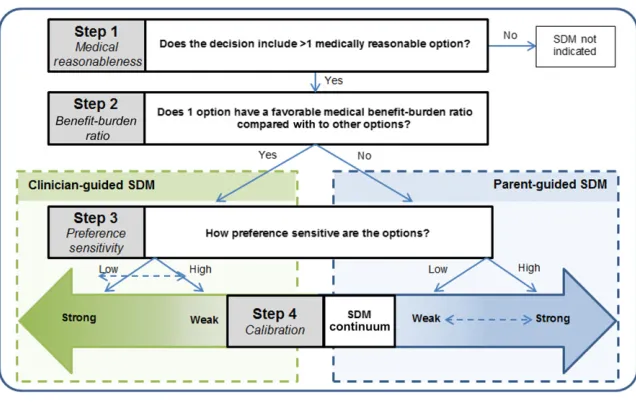
Opel4recently proposed a 4-step framework for SDM in pediatrics (Fig 1). The framework is intended to help clinicians determine if SDM is indicated, and if so, determine the process needed to implement it with parents (or the child’s legal decision-maker) in pediatrics (Table 1). Step 1 addresses medical reasonableness. This prompts the clinician to consider whether the decision includes.1 medically reasonable option (defined as an option that is consistent with standard practice); if not, SDM is not indicated. Step 2 addresses benefi
t-aTreuman Katz Center for Pediatric Bioethics, Seattle Children’s Research Institute, Seattle Children’s Hospital, Seattle, Washington;bDepartment of Pediatrics, School of Medicine, University of Washington, Seattle, Washington; andcDepartment of Pediatrics, Feinberg School of Medicine, Northwestern University, Chicago, Illinois
Dr Weiss conceptualized and designed the project, drafted the initial manuscript, and reviewed and revised the manuscript; Dr Opel conceptualized and designed the project, contributed intellectual content to the manuscript, and critically reviewed the manuscript; Drs Heike, Clark, Rosenberg, and Wilfond and Ms Shah contributed intellectual content to the manuscript and critically reviewed the manuscript; and all authors approved thefinal manuscript as submitted and agree to be accountable for all aspects of the work.
DOI:https://doi.org/10.1542/peds.2018-3055 Accepted for publication Dec 13, 2018
Address correspondence to Elliott Mark Weiss, MD, MSME, Division of Neonatology, Department of Pediatrics, School of Medicine, University of Washington, 4800 Sand Point Way NE, Mailstop FA.2.113 Neonatology, Seattle, WA 98105. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2019 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
FUNDING:No external funding.
POTENTIAL CONFLICT OF INTEREST:The authors have indicated they have no potential conflicts of interest to disclose.
burden ratio. This prompts the clinician to consider whether 1 option has a favorable benefit-burden assessment compared with other options: if so, clinician-guided SDM is indicated, and if not, parent-guided SDM is indicated. Step 2 is intended to support clinician obligations to promote the medical interests of their patients.6Step 3 addresses
preference sensitivity. This prompts the clinician to assess how strongly a decision’s trade-offs (eg, in risks, benefits, and outcomes) might be influenced by the parent’s particular principles, values, and goals. If a decision is highly preference sensitive (eg, denoted by the“high” arrows leading from step 3 in Fig 1), then clinicians are guided toward an SDM approach with greater parental involvement (eg, a strong version of parent-guided SDM or a weak version of clinician-guided SDM). If a decision is not preference sensitive (denoted by the“low”arrows leading from step 3 in Fig 1), then clinicians are guided toward an SDM approach in which less parental involvement may be appropriate (eg, a strong version of clinician-guided SDM or a weak version of parent-guided SDM). Step 4 is calibration. This prompts clinicians to calibrate these SDM approaches (eg, change the approach from strong to weak clinician-guided SDM) on the basis of other decisional
characteristics, such as the urgency of the decision, whether the
intervention is longitudinal (versus a single event), and whether the intervention is clinician- or parent-implemented.7–12
This framework was intended as provisional, with the expectation that further revisions would be needed. To identify aspects of the provisional framework that require refinement, we applied it across a diverse range of clinical cases from multiple pediatric specialties. The following cases are derived from a composite of real patient cases, with the intention that each case illustrates particular
core decisional elements. These cases therefore represent real decision-making scenarios. Names and other identifying information in these cases, however, arefictional. With each case, we identify a question regarding an aspect of the framework that requires additional scrutiny. We conduct a brief analysis of each question raised to illustrate key areas for future research.
FOR WHICH MEDICAL DECISIONS IS CONSIDERATION OF SDM REQUIRED? Oscar, a 3-week-old extremely premature infant in the NICU, has developed nonspecific feeding intolerance and abdominal distention. He is hemodynamically stable and has otherwise benign examination results. Although necrotizing enterocolitis is the most concerning diagnosis on his differential, this appears unlikely because of Oscar’s well appearance. The treating neonatologist decides to stop feeds pending results from laboratory studies and a 2-view abdominal radiograph to assess for pneumatosis or free air. He calls Oscar’s mother, informs her of her son’s changing clinical status, the medical team’s concerns, and the pending diagnostic radiographs. The neonatologist does
not include in this discussion with the parents his decision to get a 2-view (rather than 1-view) radiograph. Is that appropriate?
Given Oscar’s clinical change and concern for development of necrotizing enterocolitis, radiologic evaluation is indicated. The need for this evaluation is appropriately discussed with the family. However, the decision to get a 2-view radiograph is made by the neonatologist exclusively; the parents are not involved or made aware of the neonatalogist’s rationale. Indeed, several options may have been available: a 1-view radiograph is modestly less sensitive but half the radiation, abdominal ultrasound is highly sensitive (by a trained operator) and free of ionizing radiation but is time intensive and expensive, abdominal computed tomography is sensitive and specific but comes with greater expense and radiation.
According to the framework, SDM need not be used in decisions without
.1 medically reasonable option. Rather, alternative decision-making approaches can be used, such as clinician-controlled decision-making. This is 1 explanation for why the neonatologist did not involve the family in the decision to obtain a 2-view radiograph.
FIGURE 1
An alternative explanation, however, is that this is a technical decision that ought to simply qualify as something that requires input into the
framework. In this sense, this case prompts consideration of which clinical activities (eg, monitoring, therapy, or intervention) cross the threshold into a decision that should be shared with the parents. Many interventions routinely include parental decision involvement, such as administering chemotherapy, performing lumbar punctures, and inserting central lines. Yet clinicians participate in many activities without engaging in shared deliberation with parents, such as the frequency with which vital signs are obtained. Pushed to the extreme, SDM may become unwieldy or even absurd. Some decisions are technical, but how this determination is made, and by whom, remains unresolved.
There is minimal guidance for clinicians to determine which decisions should be fed into the framework algorithm. There are likely some medical decisions that clinicians do not need to assess for whether SDM is an appropriate approach, but which types of decisions these are needs description. Doing so will help clarify and justify when the
framework does or does not apply.
WHAT IS CONSIDERED MEDICALLY REASONABLE WHEN THERE IS VARIABILITY IN STANDARD PRACTICE? Patrick is a 2-year-old previously healthy boy admitted to the ICU after a submersion injury. He disappears at a family reunion for 15 minutes and
is found nonresponsive and facedown submerged in a creek. Bystander cardiopulmonary resuscitation is initiated, and when emergency medical services arrive, he requires an additional 15 minutes of cardiopulmonary resuscitation to regain spontaneous circulation. His pH on arrival to the hospital is 6.8. He has no purposeful movements but has sluggishly reactive pupils with intact cough and gag reflexes. Despite maximal support with mechanical ventilation for severe acute respiratory distress syndrome, his pulmonary disease and hypoxemia continue to worsen.
The intensivist wonders whether extracorporeal life support (ECLS) should be considered. At her previous institution, patients with submersion injury were considered ineligible for ECLS because of the poor neurologic prognosis. However, at her current center, such patients are not absolutely excluded from ECLS candidacy given the possibility of neurologic recovery.
Although data illustrate that half of all drowning victims supported with ECLS survive, the morbidities of survivors remain unknown.13,14This absence of morbidity data has resulted in variability in the use of ECLS for submersion injuries across pediatric centers: some centers offer it, whereas others do not. When uncertainty in outcome results in variability in whether a particular treatment is offered, is that enough for that option to be deemed medically reasonable and for SDM to be used?15
The medical-reasonableness step of the framework anchors what is medically reasonable on what is standard practice. If there is a lack of consensus on what constitutes standard practice, as is suggested in this case, there is likely a range of what is medically reasonable. Therefore, application of the
framework to this case would appear to result in the conclusion that use of ECLS is a medically reasonable option, and the decision of whether to use ECLS should involve SDM with the parents.
However, there are facets to this case that may support a non-SDM
approach. ECLS is a scarce resource: there are a limited number of ECLS circuits at a limited number of centers. Therefore, explicit medical criteria for ECLS use are essential to ensure availability for those most likely to benefit. These criteria may be outlined in institutional policy and constrain the ability to employ SDM. It appears, then, that there may be features of a decision that, although there is.1 medically reasonable option, override the use of SDM. There is a need to identify and describe which decisional features, when present, constrain the use of SDM despite there being.1 medically reasonable option.
CAN AN OPTION THAT IS NOT CONSISTENT WITH STANDARD PRACTICE STILL BE MEDICALLY REASONABLE?
Sarah, a 10-day old infant with cleft palate, presents to the craniofacial team. She has had difficulty
TABLE 1Identified Gaps by Using Opel’s 4-Step Framework for SDM in Pediatrics
Location in Framework Gap Domains
Before step 1 For which decisions is consideration of SDM required? Decisional factors Step 1 What is considered medically reasonable when there is variability in standard practice? Decisional factors Step 1 Can an option that is not consistent with standard practice still be medically reasonable? Decisional factors Step 2 How should public health implications be factored into SDM? External factors
Step 3 How should variability in preference sensitivity be approached? Parent and/or patient factors Step 3 How should the developing autonomy of adolescents be integrated into SDM? Parent and/or patient factors Step 3 How should SDM address parental decisional burden for emotionally charged decisions? Decisional factors
breastfeeding and demonstrates poor weight gain and linear growth. Sarah exhibits excellent feeding skills with a cleft bottle and takes a full feed during the clinic visit. The feeding therapist recommends that Sarah transition to cleft bottle–only feeds to maximize growth.
The parents, however, wish to continue exclusive breastfeeding. The feeding therapist feels that a time-limited trial of exclusive breastfeeding with prompt follow-up is probably safe but is extremely unlikely to be successful. When conferring with her colleagues, all agree that Sarah needs to transition to cleft bottle–only feeds. The feeding therapist is uncomfortable with the parents’choice to continue exclusive breastfeeding.
The data are mixed on acceptable growth patterns and the definition of failure to thrive in 10-day-old infants,16 but cleft palate can result in inadequate oral intake because of ineffective breastfeeding from an inability to create suction.17,18There is some evidence supporting cleft bottle–only feeds, but far stronger in this case is the medical team’s experience. This case reveals another difficulty in the medical-reasonableness step of the framework: what level of evidence is needed to consider an option medically reasonable?
Standard practice, which is integral in the framework for defining what is medically reasonable, is ideally based on high-quality, reproducible
scientific evidence. However, this level of evidence is not always available. This is acknowledged in the framework by allowing for a lower threshold of evidence to determine what is standard practice, such as experiential evidence and
professional norms. In Sarah’s case, transitioning to cleft bottle–only feeds could be argued to be standard practice on the basis of the collective clinical expertise of the feeding therapist and her colleagues. There also is a long-standing professional
norm to institute cleft-bottle feeds for such patients. Yet, it could similarly be argued that because limited empirical data are available for the use of cleft-bottle feeds, other options may be considered medically
reasonable for time-limited trial.
Because only decisions with.1 medically reasonable option warrant SDM, it is critical to have a clear conception of what is medically reasonable. Linking what is medically reasonable to standard practice is a start because it eliminates the need to consider options solely on the basis of opinion polls and personal beliefs. However, it is less clear whether determinations of what is medically reasonable should vary depending on the informing quality of evidence. A treatment option that is considered standard practice but is based on low-quality evidence, such as professional norms or experience, would seem to require a different
medical-reasonableness assessment than a treatment option that is informed by several randomized controlled trials. There may be room in the former scenario, for instance, to entertain other options outside of standard practice as being medically reasonable given the existence of only low-quality evidence. There is a need to better describe how the quality of evidence available for a specific option might modify the range of what might be considered medically reasonable.
HOW SHOULD PUBLIC HEALTH IMPLICATIONS BE FACTORED INTO SDM?
Vivian, a 7-year-old girl, presents to her pediatric nurse practitioner (NP) with 5 days of blood in her stool. Her mother said this began after Vivian ate food at a neighborhood block party and that a neighbor recently developed bloody diarrhea requiring hospitalization. Her mother describes Vivian’s stool as solid, not liquid, but with moderate amounts of bright red blood. Vivian is afebrile and well hydrated, and her vital signs are
within normal range. On her examination, the NP notes mild abdominal tenderness and a small analfissure. She is worried about a foodborne pathogen, such as Shiga toxin–producing Escherichia coli. However, Vivian’s examination results are reassuring, and the analfissure may explain the bloody stool.
The NP concludes that there are 2 medically reasonable options: close observation or sending a stool culture. She initially concludes that neither option has a more favorable medical benefit-burden ratio. After consulting with her practice colleagues, however, they point out that if Vivian does have Shiga toxin–producing E coli, diagnosing it early may help identify an outbreak, locate potential sources of ongoing transmission, and prevent further transmission from such sources, resulting in a public health benefit.
This case reveals a difficulty clinicians can face with the benefit-burden step of the framework: how to weigh individual interests against those of public health. Although the clinicians’ duty to protect public health is generally subordinate to their duties to the individual patient, it may not be clear when public health interests take priority. In Vivian’s case, there are public health benefits to obtaining a stool culture, and there also may be some direct benefit to Vivian, such as increased vigilance for complications (including hemolytic-uremic
clinician-directed or parent-directed SDM) depends on the answer.
Broader questions are germane here, too. When should clinicians burden patients with an intervention that has public health benefit but little benefit to the individual patient? Are there certain elements of such situations that make prioritizing public health benefit more justifiable? Certain interventions may be justified without use of SDM if the potential public health benefits outweigh the individual burdens, particularly in emergencies. However, caution in assessing the balance of public health benefit over the burden to the individual is important and necessary. In assessing medical benefits and burdens, clinicians lack guidance in how to consider public health interests against those of their patients, thereby potentially affecting the SDM approach used.
HOW SHOULD VARIABILITY IN PREFERENCE SENSITIVITY BE APPROACHED?
Jonah, a 6-year-old boy with cystic fibrosis (CF), presents with his parents to a new pulmonologist at the interdisciplinary CF clinic. Jonah was diagnosed with CF at 4 weeks of age after newborn screening and was started on enzyme supplementation and fat-soluble vitamins for
pancreatic insufficiency. This resulted in adequate growth. Starting at 3 years of age, he had 3 pulmonary exacerbations annually requiring hospitalization. His parents are concerned about the number of his exacerbations and whether other treatment options are available.
His parents also explain that they are strictly vegan. Both parents work full-time for an animal-rights
organization. They will be traveling internationally to an animal-rights conference and ask about travel precautions related to Jonah’s illness.
In addition to providing them with the contact information for the local CF
center during their travel, the
pulmonologist recommends a series of interventions that will help clear Jonah’s airway and reduce the
frequency of exacerbations. One is daily treatment with dornasea. The clinician wonders whether he should disclose that this medication originates from animals given Jonah’s parents’
involvement in animal rights. However, he decides not to, in part, because Jonah already is taking standard pancreatic enzyme replacement, which also originates from animals.
The treatment decision in this case involves several medically reasonable options. Although the consequences of malnutrition in CF are both severe and avoidable in most patients, the consequence of not using dornasea on pulmonary health is more ambiguous.19It is 1 of several interventions that can attenuate the decline in pulmonary function, and the absence of using it does not clearly result in accelerated lung-function decline. As such, per the framework, use of SDM and explicit elicitation and incorporation of parent preferences would be appropriate.
This case, however, reveals the challenges of determining which preferences to elicit and incorporate because some decisions may be preference sensitive for particular individuals even if they are not preference sensitive for most individuals. For instance, for most people, the use of pancreatic enzymes to treat CF is not a preference-sensitive decision. Even among those with preferences regarding pork products (because pancreatic enzymes are a porcine product), many orthodox Jewish and Muslim religious leaders have supported their use because there are no effective alternatives, and the therapies are clearly beneficial and potentially lifesaving.20Yet,
a preference about porcine products may be important to these parents.
Dornaseais a recombinant protein derived from Chinese hamster ovary
cell lines. Given Jonah’s parents’ vegan status, it is conceivable that they might have personal concerns about the use of any animal products. As such, one might argue that it is indeed an obligation to elicit the parents’preferences regarding this aspect of dornaseabecause it is known that they are animal-rights activists. Alternatively, one might argue that an obligation to explore parental preferences in this way is too broad and virtually limitless: for instance, would this not mean that clinicians should elicit parental preferences regarding the ingredients of each medication prescribed?
It may be that there are greater obligations, in general, to inquire about specific preferences that might be relevant to particular parents or members of specific religious groups. A second consideration here relates to the consequences of forgoing these interventions. Because not treating with dornaseaappears to be a medically reasonable option, eliciting the parents’preferences regarding the animal origins of dornaseamight be more important. Clinicians lack guidance on which parental preferences should be specifically elicited with SDM.
HOW SHOULD THE DEVELOPING AUTONOMY OF ADOLESCENTS BE INTEGRATED INTO SDM?
Michiko, a 14-year-old girl, presents to her family medicine physician for health supervision. Her history is notable for being sexually active with multiple male and female partners in the past year without barrier protection. She was seen last week for an acute visit and was tested for sexually transmitted infections; results of all tests were negative. The physician recommends a new contraceptive method.
them involved. The physican is aware of state guidelines suggesting that Michiko is able to provide consent for
contraception if she decides it is medically indicated (ie, no parental consent is required). However, this state also allows for parental notification by a physician. The physician has treated Michiko’s older sister (the physician knows the family well) and feels that Michiko would benefit from the long-term support from her parents, although they will likely be initially upset. Because the law permits Michiko to unilaterally accept contraception but also allows the physician to unilaterally involve her parents, she is uncertain how best to proceed.
In this case, some of the complexities of SDM particular to the adolescent patient are considered. Although it is not a question of whether to respect an adolescent’s emerging autonomy in SDM, it is unclear how to do so. In this case, prescribing contraception appears to be the only medically reasonable option (although there are many medically reasonable contraception options). Abstinence is not realistic for Michiko and not providing another contraceptive method would be contrary to standard practice. Therefore, per the framework, a non-SDM approach may be appropriate.
Yet, another interpretation of this case might be that contraception is a highly preference-sensitive decision, subject to values and beliefs. This would suggest, however, that the decision to prescribe contraception should be patient-guided, with the clinician deferring to patient preference. This approach is within the domain of SDM.
Furthermore, if SDM is appropriate, the clinician must decide whether it is more appropriate to practice SDM with Michiko alone or with her parents. Unless Michiko fears that her parents could cause her harm, it may be reasonable to involve her parents. Adolescents have greater plasticity and learning ability than adults but
are more susceptible to peer pressure and tend to disregard long-term consequences.21,22Michiko may therefore benefit from parental involvement. Alternatively, there may be real harm from involving her parents without her agreement, including loss of trust in her physician, which could result in her avoiding future medical care.
The framework for implementing SDM in pediatrics was developed to guide decision-making involving nonadolescent patients. However, there is a need to adapt it to include adolescents and their parents. Clinicians lack guidance on how to integrate adolescents into SDM.
HOW SHOULD SDM ADDRESS PARENTAL DECISIONAL BURDEN FOR EMOTIONALLY CHARGED DECISIONS?
Alex, a 6-year-old boy with metastatic alveolar rhabdomyosarcoma,
presents to his pediatric oncologist. There are no curative treatment options. The oncologist identifies 3 medically reasonable options: palliative chemotherapy, phase I clinical trials, and palliative care without chemotherapy. None has a clearly favorable benefit-burden ratio, and each is highly preference sensitive.
The oncologist knows Alex’s family well. Alex’s parents are highly distressed. When Alex received chemotherapy, they struggled when offered multiple options: his father noted that they felt immense burden around these choices but also felt guilty if they did not participate in decision-making. Because of this, the oncologist decides to shoulder more of the decisional burden by using her knowledge of the parents’values and employing physician-guided SDM.
This case exemplifies the concern that highly charged emotional states may jeopardize parents’ability to make determinations consistent with their values and preferences, an ability preferred, if not required, for SDM.23
In this case, parent-guided SDM would be indicated given multiple medically reasonable and highly preference-sensitive options, none of which has a clearly favorable benefi t-burden ratio.24–26However, some parents tasked with participating in SDM are highly distressed. Intense negative emotions, such as anxiety, sadness, or anger, directly impact decision-making processes. For example, after receiving serious or difficult news, surrogate decision-makers cannot fully recall their options and neglect their usual deliberation of each potential decision.27–29
Thus, it can be problematic to expect parents to fully evaluate and
articulate their preferences when intense emotions are unavoidable. One solution is to give additional time for deliberation; effectively
communicating difficult news requires time to digest it.24,25 However, time may be inadequate: parental distress may not diminish sufficiently to allow for improved SDM. A second option is to instead use a physician-guided model of SDM: the clinician solicits values and then directs decision-making.25However, this may result in low parental involvement of a highly preference-sensitive decision. Clinicians lack guidance on how to calibrate along the SDM continuum when decisional burden and emotions are elevated.
CONCLUSIONS
Opel’s4provisional framework for SDM in pediatrics has the potential to provide guidance for clinicians on how to implement SDM in different pediatric disciplines. However, there are areas within the framework in need of additional specification. These 7 example cases bring up at least 3 important domains for future research into pediatric SDM:
charged decisions; external factors, including public health concerns and interventions with limited
availability; and parent or patient factors, including the developing autonomy of adolescents and variability in preferences. Each of these should be targets of future empirical and conceptual research to further facilitate the practice of SDM in pediatrics.
ACKNOWLEDGMENTS
We thank Heather Spielvogle and Kim Sawyer for their review of the article and the research group at the Treuman Katz Center for Pediatric Bioethics for their contribution to an earlier form.
ABBREVIATIONS CF: cysticfibrosis
ECLS: extracorporeal life support NP: nurse practitioner
SDM: shared decision-making
REFERENCES
1. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango).Soc Sci Med. 1997;44(5):681–692
2. Kon AA. The shared decision-making continuum.JAMA. 2010;304(8):903–904
3. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA. 1992;267(16):2221–2226
4. Opel DJ. A push for progress with shared decision-making in pediatrics. Pediatrics. 2017;139(2):e20162526
5. Rosenbaum L. The paternalism preference–choosing unshared decision making.N Engl J Med. 2015; 373(7):589–592
6. Beauchamp TL, Childress JF.Principles of Biomedical Ethics. 5th ed. New York, NY: Oxford University Press; 2001
7. Montori VM, Gafni A, Charles C. A shared treatment decision-making approach between patients with chronic conditions and their clinicians:
the case of diabetes.Health Expect. 2006;9(1):25–36
8. Weiss EM, Barg FK, Cook N, Black E, Joffe S. Parental decision-making preferences in neonatal intensive care. J Pediatr. 2016;179:36–41.e3
9. Müller-Engelmann M, Keller H, Donner-Banzhoff N, Krones T. Shared decision making in medicine: the influence of situational treatment factors.Patient Educ Couns. 2011;82(2):240–246
10. Kaplan RM. Shared medical decision making. A new tool for preventive medicine.Am J Prev Med. 2004;26(1): 81–83
11. Keirns CC, Goold SD. Patient-centered care and preference-sensitive decision making.JAMA. 2009;302(16):1805–1806
12. Weiss EM, Xie D, Cook N, Coughlin K, Joffe S. Characteristics associated with preferences for parent-centered decision making in neonatal intensive care.JAMA Pediatr. 2018;172(5):461–468
13. Burke CR, Chan T, Brogan TV, et al. Extracorporeal life support for victims of drowning.Resuscitation. 2016;104: 19–23
14. Champigneulle B, Bellenfant-Zegdi F, Follin A, et al. Extracorporeal life support (ECLS) for refractory cardiac arrest after drowning: an 11-year experience.Resuscitation. 2015;88: 126–131
15. Kim KI, Lee WY, Kim HS, Jeong JH, Ko HH. Extracorporeal membrane oxygenation in near-drowning patients with cardiac or pulmonary failure.Scand J Trauma Resusc Emerg Med. 2014;22:77
16. Paul IM, Schaefer EW, Miller JR, et al. Weight change nomograms for thefirst month after birth.Pediatrics. 2016; 138(6):e20162625
17. Kaye A, Thaete K, Snell A, Chesser C, Goldak C, Huff H. Initial nutritional assessment of infants with cleft lip and/or palate: interventions and return to birth weight.Cleft Palate Craniofac J. 2017;54(2):127–136
18. Parameters for evaluation and treatment of patients with cleft lip/ palate or other craniofacial differences. Cleft Palate Craniofac J. 2018;55(1): 137–156
19. Massie J, Morgan A, Gillam L. When is too little care, too much harm in cystic
fibrosis? Psychological and ethical approaches to the problem.J Cyst Fibros. 2017;16(2):299–303
20. Imrie CW, Connett G, Hall RI, Charnley RM. Review article: enzyme
supplementation in cysticfibrosis, chronic pancreatitis, pancreatic and periampullary cancer.Aliment Pharmacol Ther. 2010;32(suppl 1):1–25
21. McCormick EM, Telzer EH. Adaptive adolescentflexibility:
neurodevelopment of decision-making and learning in a risky context.J Cogn Neurosci. 2017;29(3):413–423
22. Gardner M, Steinberg L. Peer influence on risk taking, risk preference, and risky decision making in adolescence and adulthood: an experimental study. Dev Psychol. 2005;41(4):625–635
23. Rosenberg AR, Dussel V, Kang T, et al. Psychological distress in parents of children with advanced cancer.JAMA Pediatr. 2013;167(6):537–543
24. Back AL, Arnold RM.“Yes it’s sad, but what should I do?”Moving from empathy to action in discussing goals of care.J Palliat Med. 2014;17(2): 141–144
25. Gramling R, Sanders M, Ladwig S, Norton SA, Epstein R, Alexander SC. Goal communication in palliative care decision-making consultations.J Pain Symptom Manage. 2015;50(5):701–706
26. Gramling R, Norton SA, Ladwig S, et al. Direct observation of prognosis communication in palliative care: a descriptive study.J Pain Symptom Manage. 2013;45(2):202–212
27. Power TE, Swartzman LC, Robinson JW. Cognitive-emotional decision making (CEDM): a framework of patient medical decision making.Patient Educ Couns. 2011;83(2):163–169
28. Jansen J, van Weert JC, de Groot J, van Dulmen S, Heeren TJ, Bensing JM. Emotional and informational patient cues: the impact of nurses’responses on recall.Patient Educ Couns. 2010; 79(2):218–224
DOI: 10.1542/peds.2018-3055 originally published online February 5, 2019;
2019;143;
Pediatrics
Shah, Benjamin S. Wilfond and Douglas J. Opel
Elliott Mark Weiss, Jonna D. Clark, Carrie L. Heike, Abby R. Rosenberg, Seema K.
Gaps in the Implementation of Shared Decision-making: Illustrative Cases
Services
Updated Information &
http://pediatrics.aappublications.org/content/143/3/e20183055 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/143/3/e20183055#BIBL This article cites 28 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/ethics:bioethics_sub Ethics/Bioethics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2018-3055 originally published online February 5, 2019;
2019;143;
Pediatrics
Shah, Benjamin S. Wilfond and Douglas J. Opel
Elliott Mark Weiss, Jonna D. Clark, Carrie L. Heike, Abby R. Rosenberg, Seema K.
Gaps in the Implementation of Shared Decision-making: Illustrative Cases
http://pediatrics.aappublications.org/content/143/3/e20183055
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.