ARTICLE
Descriptive Epidemiological Features of Bronchiolitis
in a Population-Based Cohort
Mieke Koehoorn, PhDa,b, Catherine J. Karr, MD, PhDc,d, Paul A. Demers, PhDa,b, Cornel Lencar, MFa, Lillian Tamburic, BSce, Michael Brauer, ScDa
aSchool of Environmental Health,bSchool of Population and Public Health, andeCentre for Health Services and Policy Research, University of British Columbia,
Vancouver, Canada; Departments ofcPediatrics anddEnvironmental and Occupational Health Sciences, University of Washington, Seattle, Washington
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
In clinical populations bronchiolitis is associated with socio-demographic, clinical and environmental factors.
What This Study Adds
To our knowledge, this is the first population-based study of bronchiolitis risk in Canada and one of few in the world. Cases included outpatient visits and hospitalizations.
ABSTRACT
OBJECTIVE.The goal was to investigate the epidemiological features of incident bron-chiolitis by using a population-based infant cohort.
METHODS.Outpatient and inpatient health records were used to identify incident bronchiolitis cases among 93 058 singleton infants born in the Georgia Air Basin between 1999 and 2002. Additional health-related databases were linked to provide data on sociodemographic variables, maternal characteristics, and birth outcome measures.
RESULTS.From 1999 to 2002, bronchiolitis accounted for 12 474 incident health care encounters (inpatient or outpatient contacts) during the first year of life (134.2 cases per 1000 person-years). A total of 1588 hospitalized bronchiolitis cases were iden-tified (17.1 cases per 1000 person-years). Adjusted Cox proportional-hazard analyses for both case definitions indicated an increased risk of incident bronchiolitis in the first year of life (follow-up period: 2–12 months) for boys, infants of First Nations status, infants with older siblings, and infants living in neighborhoods with smaller proportions of maternal postsecondary education. The risk also was elevated for infants born to young mothers (⬍20 years of age) or mothers who did not initiate breastfeeding in the hospital. Infants with low (1500 –2400 g) or very low (⬍1500 g) birth weight and those with congenital anomalies also had increased risk. Maternal smoking during pregnancy increased the risk of hospitalized bronchiolitis.
CONCLUSIONS.This population-based study of the epidemiological features of bronchiolitis provides evidence for inter-vening with high-risk infants and their families. Clinical and public health interventions are recommended for the modifiable risk factors of maternal breastfeeding and smoking and for modification of vulnerable environments where possible (eg, limiting exposure to other young children), during high-risk periods such as the first few months of life or the winter season.Pediatrics2008;122:1196–1203
B
RONCHIOLITIS IS ANinfection of the lower respiratory tract that usually affects infants in the first year of life.1Themost common cause of bronchiolitis is respiratory syncytial virus (RSV) (⬃90% of cases in North America).2
However, a number of other respiratory viruses (such as influenza, parainfluenza, rhinovirus, human metapneumovirus, and bocavirus) also can cause bronchiolitis. Bronchiolitis is the leading cause of morbidity among infants⬍1 year of age in North America and Europe,1,3–6and hospital admission rates have been increasing over the past 2 decades.1
Given the frequency and burden of illness, there are very few population-based, epidemiological studies of risk factors associated with bronchiolitis. A Medline search identified 1811 articles focused on “bronchiolitis” or “bron-chiolitis, viral,” of which 468 were focused on “infant” or “child.” Of those, 72 were on “risk factors” or “epidemi-ology” of bronchiolitis. A review of the abstracts for those 72 articles identified 21 that provided epidemiological evidence of risk factors for the primary onset of bronchiolitis, as opposed to articles on clinical outcomes among children with bronchiolitis,7diagnostic or clinical practice guidelines,8bronchiolitis as a risk factor for other outcomes
such as asthma,9review articles,10or editorials.11
Of the 21 articles on the epidemiological features of bronchiolitis, 11 were cross-sectional clinical studies (eg, hospitalized sample),12–22 9 were case-control or case-crossover studies,23–31 and only 1 was a population-based
study.32One additional clinical study was identified from study references.33The majority of the studies investigated
hospitalization or mortality outcomes for bronchiolitis, with 2 exceptions; 1 study included outpatient visits as part
www.pediatrics.org/cgi/doi/10.1542/ peds.2007-2231
doi:10.1542/peds.2007-2231
Key Words
bronchiolitis, epidemiological features, cohort studies, population-based studies, Cox proportional-hazards models Abbreviation
RSV—respiratory syncytial virus Accepted for publication Mar 3, 2008
Address correspondence to Mieke Koehoorn, PhD, Department of Health Care and Epidemiology, University of British Columbia, 5804 Fairview Ave, Vancouver, British Columbia, Canada V6T 1Z3. E-mail: mieke. [email protected]
of a combined outcome,19 and the population-based
study32investigated RSV-positive test results via
outpa-tient physician visits. The populations for the clinical studies ranged from 89 hospitalized infants20 to 8265
hospitalized infants16 with the exception of a national
study of emergency department visits, with almost 2 million hospitalization outcomes over 10 years.22 The
case-control studies ranged from 34 pairs30 to 18 595
case subjects with 10 matched control subjects.27
The population-based, 1-year, follow-up study of 1179 healthy infants identified male gender and ⬍1 month of or no breastfeeding as risk factors for RSV infection in multivariate models adjusted for sociodemo-graphic factors.32 It also found a protective interaction
effect for breastfeeding among mothers with a lower education level. Studies of clinical populations indicate that native or aboriginal infants (eg, First Nations or Inuit)13,17have higher rates of hospital admissions related
to bronchiolitis, although this may be attributable to unmeasured socioeconomic factors rather than genetic factors. Bronchiolitis (and RSV) is also more common in male infants,13,32 infants of low birth weight or
gesta-tional age,14,15,17,18,23,25,30,33 and infants born to young
mothers.18,19 It is associated with no breastfeeding or
early weaning,23,25,29,32living in crowded conditions or in
the presence of older siblings14,18,30,32,33or attending day
care,14exposure to secondhand smoke or tobacco during
pregnancy,18,19,23,33 and social disadvantage.16,26,32
Case-control studies identified environmental exposures asso-ciated with the risk of bronchiolitis, including exposure to wood-burning in the home24and air quality measures
(2.5-m particulate matter levels).27
The purpose of this study was to conduct a large, population-based, epidemiological study of a compre-hensive set of concurrent risk factors for bronchiolitis, including both hospitalizations and outpatient visits to physicians. Although bronchiolitis is common, there are limited population-based studies on the epidemiological features of this condition, and little is known about what causes infants to be susceptible to infection in the gen-eral population.
METHODS
Overview
This was a retrospective cohort study of infants born between 1999 and 2002 in the geographic area defined as the Georgia Air Basin, British Columbia (N ⫽
119 345). The analysis excluded multiple births and births of⬍25 weeks of gestation (n⫽2606). A total of 14 488 births were excluded because of missing data on maternal age or First Nations status and 9193 births because of incomplete residential history (because this cohort was the basis for a study investigating residential air pollution exposures and risk of bronchiolitis), for a final study population of 93 058 births.
Data Sources
Health data are available from the British Columbia Linked Health Database for research purposes, through an approved process34governed by a data access
agree-ment between the researchers and the data stewards. Medical services and hospitalization data were provided and governed by the Ministry of Health, Government of British Columbia, and vital statistics data by the British Columbia Vital Statistics Agency. These data were merged, through an additional data access agreement, with records in the provincial perinatal database, gov-erned by the British Columbia Reproductive Care Pro-gram. The research database was constructed by merging vital statistics birth records (for cohort enumeration ac-cording to residential postal codes) with outpatient med-ical services billing records and inpatient hospital dis-charge records, for identification of cases for the period of 1999 –2003 (allowing a minimum of a 1-year fol-low-up period for all births). Birth and health records were merged with the provincial perinatal database for maternal characteristics (maternal age, infant age, breastfeeding initiation, smoking during pregnancy, and parity) and birth outcome measures (gestational age, preterm complications, and low birth weight complica-tions). First Nations status was available from hospital discharge records for all births, with socioeconomic in-dicators for education and household income from Sta-tistics Canada census data. The research database was provided to the research team with all personal fiers removed and replaced by anonymous study identi-fiers. The identifiers were unique to each infant and enabled identification of the same infants across data sources. The research protocol was approved by the Uni-versity of British Columbia Behavioral Research Ethics Committee.
Outcomes
Infants were monitored from the second to 12th month after birth, and cases were identified from the first health care encounter with an International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis code35of 466 (acute bronchitis and bronchiolitis) in the
outpatient medical charts (general practitioner or spe-cialist visit) or a principal diagnosis code of 466.1 (acute bronchiolitis) in the hospital discharge records. Only the first encounter (either outpatient visit or hospitalization) for each infant was counted as the case. The outpatient medical services records allow for 1 diagnosis code, coded to the first 3 digits only of the International Clas-sification of Diseases, Ninth Revision, Clinical Modifica-tion coding system, which necessitated the broader in-clusion criteria for this data set. A second case definition was limited to hospitalizations only, with the more-specific diagnosis code of 466.1. Only the first hospital-ization was counted as the case. These data do not in-clude emergency department visits unless they resulted in a hospital admission. The databases are considered comprehensive for outpatient and inpatient encounters, given a universal, publicly funded, health care system.
Risk Factors
years), maternal education (in quartiles), household in-come (in quintiles), urban versus rural residence, mater-nal smoking during pregnancy, breastfeeding initiation in the hospital, First Nations status, parity (yes or no, as a proxy measure for older siblings), birth weight (nor-mal: 2500 – 4000 g; low: 1500 –2500 g; very low:⬍1500 g; high:⬎4000 g), gestational age (25–28 weeks, 29 –32 weeks, 33–35 weeks, orⱖ36 weeks), preterm complica-tions (yes or no), and low birth weight complicacomplica-tions (yes or no). Urban residence, based on census data, is defined as living in an area with⬎400 people per km2.36
Education and household income variables, also based on census data, represent the distribution of median household incomes (in quintiles) and the proportion of the population with postsecondary education (in quar-tiles) according to neighborhood (ie, census subdivi-sions). These census variables were assigned to infants on the basis of their mother’s postal code of residence within a neighborhood.
Analysis
Follow-up monitoring was from the second to 12th month of life; the first month of life was excluded because bronchiolitis infection is not common among infants in the first month18 and exclusion reduces
misclassification of other acute respiratory infections. The Cox proportional-hazard model37 was used to
in-vestigate the association between risk factors and an infant’s first clinical encounter related to bronchiolitis. Factors associated with bronchiolitis at the bivariate level (95% confidence interval for the hazard rate ratio) were entered into the final multivariate model. Models were constructed for both case definitions of bronchiolitis, for comparison purposes.
RESULTS
The study cohort included 93 058 singleton births in the Georgia Air Basin between 1999 and 2002 with com-plete data. The cohort was 48.6% female, 1.2% of First Nations status, and 45.9% firstborn. Eighty-two percent of infants had a normal birth weight (2500 – 4000 g), and 89.0% were born at term (gestational age of ⬎38 weeks). Less than 10% of infants had complications related to either preterm status (7.1%) or low birth
weight (6.7%). Less than 1% of the study cohort had congenital anomalies. Maternal smoking during preg-nancy was recorded for 9% of the birth cohort, and lack of breastfeeding initiation at the hospital was recorded for 7.5% of the cohort. The majority (57.3%) of infants were born to mothers ⱖ29 years of age. The excluded population had similar proportions of female infants (48.5%) and mothers in the lowest education quartile (25.9% vs 24.0%) and household income quintile (21.9% vs 21.6%) but a larger proportion of infants of First Nations status (2.9%).
A total of 12 474 incident bronchiolitis cases (134.1 cases per 1000 person-years) were identified from out-patient and inout-patient encounters among cohort infants during the first year of life (second to 12th month). A total of 1588 bronchiolitis cases were identified from hospitalizations only (17.1 cases per 1000 person-years). The rates of bronchiolitis were higher in the excluded population (146.1 and 23.1 cases per 1000 person-years, respectively).
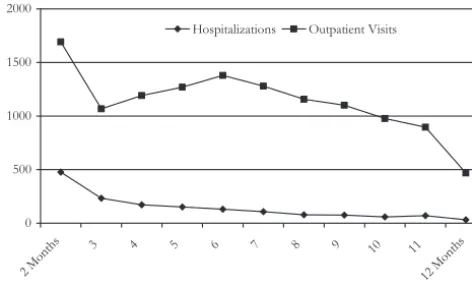
An analysis of bronchiolitis cases according to calen-dar month of diagnosis (Fig 1) and age of diagnosis (Fig 2) indicated that incident cases occurred more fre-quently during the winter months (December through March) and in the first months of life. The same trends were observed for bronchiolitis defined on the basis of outpatient visits as noted for hospitalizations.
The distributions of risk factors between infants with and without bronchiolitis, by outpatient and inpatient case definitions, are shown in Table 1. Because of quantitative correlations or conceptual overlap between the measures of maternal education and household income (Spearman’s ⫽0.43), gestational age and birth weight (Spearman’s ⫽0.30), congenital anomalies and preterm complications (Spearman’s⫽0.32), and low birth weight complications and preterm complications (Spearman’s ⫽ 0.97), only maternal education, birth weight, and congenital anoma-lies were entered in the final multivariate models.
In the final regression models adjusted for covariates (Table 2), the risk of incident bronchiolitis in the first year of life remained elevated for male infants, infants of First Nations status, infants with older siblings, and in-fants living in neighborhoods with smaller proportions of maternal postsecondary education (lowest quartile,
0 500 1000 1500 2000
Jan Feb Mar Apr May June Jul Aug Sep Oct Nov Dec Hospitalizations Outpatient Visits
FIGURE 1
Frequency of bronchiolitis cases according to month of diagnosis.
0 500 1000 1500 2000
2 Mont
hs 3 4 5 6 7 8 9 10 11
12Mo nths
Hospitalizations Outpatient Visits
FIGURE 2
TABLE 1 Bivariate Results for Bronchiolitis Among Infants in the Georgia Air Basin Region in 1999 –2002
Variable Outpatient or Inpatient Bronchiolitis Case Definition Inpatient Bronchiolitis Case Definition
n(%) Unadjusted Hazard Rate Ratio (95% Confidence Interval)
n(%) Unadjusted Hazard Rate Ratio (95% Confidence Interval) Bronchiolitis No Bronchiolitis Bronchiolitis No Bronchiolitis
Gender
Female 5150 (41.3) 40 028 (49.7) 1.00 628 (39.5) 44 550 (48.7) 1.00
Male 7324 (58.7) 40 524 (50.3) 1.37 (1.32–1.42) 960 (60.5) 46 888 (51.3) 1.46 (1.32–1.62) Maternal age
20–29 y 4580 (36.7) 26 343 (32.7) 1.00 586 (36.9) 30 337 (33.2) 1.00
⬎29 y 7524 (60.3) 52 335 (65.0) 0.84 (0.81–0.87) 935 (58.9) 58 924 (64.4) 0.82 (0.74–0.91)
⬍20 y 370 (3.0) 1874 (2.3) 1.12 (1.01–1.25) 67 (4.2) 2177 (2.4) 1.58 (1.23–2.04) Maternal educationa
High 2531 (20.3) 21 051 (26.1) 1.00 300 (18.9) 23 282 (25.5) 1.00
Medium high 3056 (24.5) 20 716 (25.7) 1.21 (1.15–1.28) 377 (23.7) 23 395 (25.6) 1.25 (1.08–1.46) Medium low 3286 (26.3) 20 092 (24.9) 1.34 (1.27–1.41) 415 (26.1) 22 963 (25.1) 1.41 (1.22–1.64) Low 3601 (28.9) 18 693 (23.2) 1.56 (1.48–1.64) 496 (31.2) 21 798 (23.8) 1.78 (1.55–2.06) Maternal smoking during pregnancy
No 11 217 (89.9) 73 432 (91.2) 1.00 1351 (85.1) 83 298 (91.1) 1.00
Yes 1257 (10.1) 7120 (8.8) 1.14 (1.08–1.21) 237 (14.9) 8140 (8.9) 1.78 (1.55–2.04) Breastfeeding initiation at hospital
Yes 11 267 (90.3) 74 788 (92.8) 1.00 1383 (87.1) 84 672 (92.6) 1.00
No 1207 (9.7) 5764 (7.2) 1.36 (1.28–1.44) 205 (12.9) 6766 (7.4) 1.86 (1.61–2.16) First Nations status
No 12 210 (97.9) 79 738 (99.0) 1.00 1516 (95.5) 90 432 (98.9) 1.00
Yes 264 (2.1) 814 (1.0) 1.98 (1.76–2.24) 72 (4.5) 1006 (1.1) 4.23 (3.34–5.35) Parity (siblings)
No 4560 (36.6) 38 162 (47.4) 1.00 474 (29.9) 42 248 (46.2) 1.00
Yes 7914 (63.4) 42 390 (52.6) 1.52 (1.47–1.58) 1114 (70.1) 49 190 (53.8) 2.04 (1.83–2.04) Birth weight
2500–4000 g 10 222 (81.9) 66 380 (82.4) 1.00 1239 (78.0) 75 363 (82.4) 1.00
ⱖ4000 g 1666 (13.4) 11 371 (14.1) 0.95 (0.90–1.01) 185 (11.7) 12 852 (14.1) 0.88 (0.75–1.02) 1500–2500 g 489 (3.9) 2492 (3.1) 1.25 (1.14–1.37) 122 (7.7) 2859 (3.1) 2.56 (2.12–3.08)
⬍1500 g 97 (0.8) 309 (0.4) 1.88 (1.54–2.29) 42 (2.6) 364 (0.4) 6.56 (4.82–8.92) Congenital anomalies
No 12 355 (99.0) 79 932 (99.2) 1.00 1560 (98.2) 90 727 (99.2) 1.00
Yes 119 (1.0) 620 (0.8) 1.22 (1.02–1.46) 28 (1.8) 711 (0.8) 2.26 (1.56–3.29)
Household incomeb
High 1635 (13.1) 13 272 (16.5) 1.00 207 (13.0) 14 700 (16.1) 1.00
Medium high 2246 (18.0) 15 485 (19.2) 1.17 (1.09–1.24) 295 (18.6) 17 436 (19.1) 1.20 (1.01–1.44) Medium 2643 (21.2) 16 945 (21.0) 1.25 (1.17–1.33) 320 (20.2) 19 268 (21.1) 1.19 (1.00–1.41) Medium low 2930 (23.5) 17 490 (21.7) 1.33 (1.26–1.42) 378 (23.8) 20 042 (21.8) 1.35 (1.14–1.60) Low 3020 (24.2) 17 360 (21.6) 1.38 (1.30–1.47) 388 (24.4) 19 992 (21.9) 1.39 (1.17–1.64) Residencec
Urban 11 148 (89.3) 71 061 (88.2) 1.00 1374 (86.5) 80 805 (88.4) 1.00
Small town 120 (1.0) 841 (1.0) 0.91 (0.76–1.09) 21 (1.3) 940 (1.0) 1.30 (0.84–1.99) Rural fringe 955 (7.7) 7040 (8.7) 0.87 (0.82–0.93) 155 (9.8) 7839 (8.6) 1.15 (0.98–1.36) Rural 261 (2.1) 1632 (2.0) 1.02 (0.90–1.15) 38 (2.4) 1854 (2.0) 1.20 (0.87–1.66) Gestational aged
⬎35 wk 11 949 (95.8) 78 369 (97.3) 1.00 1432 (90.2) 88 886 (97.2) 1.00
33–35 wk 346 (2.8) 1603 (2.0) 1.37 (1.23–1.53) 87 (5.5) 1862 (2.0) 2.85 (2.30–3.54) 29–32 wk 121 (1.0) 436 (0.5) 1.70 (1.42–2.04) 44 (2.8) 513 (0.6) 5.08 (3.77–6.86) 25–28 wk 58 (0.5) 144 (0.2) 2.33 (1.80–3.01) 25 (1.6) 177 (0.2) 8.04 (5.42–11.9) Preterm complications
No 11 457 (91.8) 74 995 (93.1) 1.00 1378 (86.8) 85 074 (93.0) 1.00
Yes 1017 (8.2) 5557 (6.9) 1.18 (1.11–1.26) 210 (13.2) 6364 (7.0) 2.02 (1.75–2.34) Low birth weight complications
No 11 504 (92.2) 75 273 (93.4) 1.00 1386 (87.3) 85 391 (93.4) 1.00
Yes 970 (7.8) 5279 (6.6) 1.19 (1.12–1.27) 202 (12.7) 6047 (6.6) 2.04 (1.76–2.37)
Analyses were performed with Cox’s proportional-hazards model.
aHigh was defined as⬎44% of neighborhood residents with postsecondary education, medium high as 36% to 44%, medium low as 28% to 36%, and low as⬍28%; infants were assigned to categories on the basis of mothers’ postal codes of residence.
bThe distribution of median household incomes within a neighborhood according to quintile was determined; infants were assigned to categories on the basis of mothers’ postal codes of residence. cCategories were based on Census population density data, with urban defined as an area with⬎400 people per km2.
compared with highest quartile). The risk was also ele-vated for infants born to young mothers (⬍20 years versus 20 –29 years of age) and mothers who did not initiate breastfeeding in the hospital. Infants with a low (1500 –2400 g) or very low (⬍1500 g) birth weight and those born with a congenital anomaly also had an in-creased risk of bronchiolitis. The hazard rate ratios for all of the preceding risk factors were higher in the model of hospitalized bronchiolitis cases, compared with the com-bined inpatient and hospitalized definition, with an ap-proximately twofold increased risk observed for infants with older siblings and a congenital anomaly, a threefold increased risk associated with First Nations status, and a sixfold increased risk associated with very low birth weight (⬍1500 g, compared with 2500 – 4000 g). An elevated risk of bronchiolitis associated with maternal smoking during pregnancy remained significantly ele-vated in the model for hospitalized bronchiolitis only
(hazard rate ratio: 1.49; 95% confidence interval: 1.27– 1.72).
DISCUSSION
This is the first study to evaluate the epidemiological features of bronchiolitis in Canada by using a popula-tion-based cohort, a comprehensive set of risk factors through linkage of several longitudinal and retrospective databases, and the inclusion of outpatient visits in the case definition. Our data suggested that 13.4% of single-ton infants born in the Georgia Air Basin had incident bronchiolitis requiring a clinical encounter within the first year of life and 1.7% of cases were serious enough to warrant hospitalization. This rate is lower than previ-ously reported rates of acute hospitalized bronchiolitis for Canadian infants5,38 and for infants in other
coun-tries,16,22although the lowest rates were reported in the
province of British Columbia (2.5%).38 The previous
studies were not limited to first encounters for calcula-tion of hospitalizacalcula-tion rates, and others studies tended to use a broader definition of hospitalized bronchiolitis.22
The prevalence of hospitalized bronchiolitis in this study is closer to bronchiolitis rates in other studies that used a confirmed RSV lower respiratory tract infection out-come.32,38 However, 2.3% of our excluded population
met the hospitalized case definition, an estimate closer to previous reports for British Columbia,38which may
in-dicate a conservative bias in the current findings. Com-parable population-based studies are limited, but one using physician visits as the first point of contact32
indi-cated a comparable overall bronchiolitis rate of 10.4% in a study of 1179 infants.
Our study used administrative health records to cap-ture outpatient visits and hospitalizations for bronchioli-tis, as well as administrative databases for infant and maternal characteristics. An assessment of the validity and reliability39of key variables captured in the perinatal
database (relative to patient charts) indicated good sen-sitivity and specificity for maternal smoking status (79% and 98%, respectively) and breastfeeding initiation (95% and 73%, respectively). In addition, the breast-feeding initiation rate of 92.5% in the current study parallels the population estimates for breastfeeding (of any duration) reported by women in the Canadian Com-munity Health Survey for the province of British Colum-bia (93.1%) and the city of Vancouver (90.4%),40 the
most densely populated area of the study region. The survey data also indicated that the majority (81.8%) of women in Vancouver who breastfeed do so for ⱖ6 months.
The validity and reliability of coding for bronchiolitis have not been established for these data sources, but the consistency of findings between the more-specific hos-pitalized bronchiolitis definition and the bronchiolitis definition that included outpatient visits supports the validity of using outpatient records to capture cases. In addition, bronchiolitis cases followed recognized season-al6and temporal41patterns for infection for both
outpa-tient and inpaoutpa-tient case definitions. Higher risk estimates for all significant variables for hospitalized bronchiolitis may indicate greater specificity for more-severe
inpa-TABLE 2 Multivariate Results for Bronchiolitis Among Infants in the Georgia Air Basin in 1999 –2002
Variable Adjusted Hazard Rate Ratio (95% Confidence Interval) Outpatient or
Inpatient Case Definition
Inpatient Case Definition
Gender
Female 1.00 1.00
Male 1.38 (1.33–1.43) 1.49 (1.34–1.64) Maternal age
20–29 y 1.00 1.00
⬎29 y 0.81 (0.78–0.84) 0.78 (0.70–0.87)
⬍20 y 1.23 (1.10–1.37) 1.65 (1.27–2.15) Maternal educationa
High 1.00 1.00
Medium high 1.16 (1.10–1.22) 1.20 (1.03–1.40) Medium low 1.24 (1.18–1.31) 1.23 (1.05–1.42)
Low 1.39 (1.32–1.46) 1.44 (1.24–1.66)
Maternal smoking during pregnancy
No 1.00 1.00
Yes 1.03 (0.97–1.09) 1.47 (1.27–1.69)
Breastfeeding initiation at hospital
Yes 1.00 1.00
No 1.19 (1.12–1.26) 1.33 (1.14–1.54)
First Nations status
No 1.00 1.00
Yes 1.65 (1.46–1.86) 2.94 (2.31–3.75)
Parity (older siblings)
No 1.00 1.00
Yes 1.58 (1.53–1.65) 2.24 (2.01–2.51)
Birth weight
2500–4000 g (normal) 1.00 1.00
ⱖ4000 g (high) 0.89 (0.84–0.93) 0.80 (0.68–0.93) 1500–2500 g (low) 1.29 (1.18–1.42) 2.64 (2.19–3.18)
⬍1500 g (very low) 1.84 (1.50–2.25) 6.19 (4.53–8.48) Congenital anomalies
No 1.00 1.00
Yes 1.18 (0.98–1.41) 2.16 (1.49–3.14)
Analyses were performed with Cox’s proportional-hazards model.
tient cases and some misclassification of respiratory ill-ness by using the outpatient administrative data records. However, we conclude from our results that outpatient visits provide a reasonable measure of bronchiolitis in the general population and that estimates based on only clinical populations and hospitalized cases may underes-timate the incidence and burden of disease in the general population (13.4%, compared with 1.7%, in the current study), even with a degree of misclassification with the 3-digit diagnostic code of 466 in the present study.
We did not have confirmation of RSV infection among bronchiolitis cases. Therefore, our case definition represents the multitude of viral causes. We were inter-ested in the outcome of bronchiolitis in general, as a public health burden, and not risk factors for a specific etiologic agent.
Our data confirm previous findings, based on smaller clinical populations, that the risk of bronchiolitis is sea-sonal and is associated with male gender, younger ma-ternal age, lower mama-ternal socioeconomic status, low birth weight, parity (as a surrogate measure for older siblings in the home), no breastfeeding initiation at the hospital, and First Nations status. Maternal smoking dur-ing pregnancy and congenital anomalies also were asso-ciated with increased risk of bronchiolitis, but only for cases severe enough to result in hospitalization.
An increased risk of bronchiolitis for First Nations infants is consistent with previous findings of higher hospitalization rates for bronchiolitis among Native American and Alaskan infants13,16 and among Inuit
in-fants.17 It is not clear, on the basis of previous studies,
whether this increased risk is attributable to cultural differences (ie, differences in breastfeeding patterns), re-duced access to health care in remote areas,42 or
envi-ronmental exposures such as indoor air pollution (wood smoke).24However, an independent effect for First
Na-tions status was found in the current study after adjust-ment for breastfeeding and socioeconomic factors, in an area with a universal health care system. The observed increased risk may still be attributable to residual con-founding or unmeasured covariates, including respira-tory system or immune system susceptibility. Infants with compromised physiological features,43as indicated
by the presence of congenital anomalies, had an in-creased risk of hospitalized bronchiolitis in the current study.
It is important to note that our study variable identi-fied only individuals with First Nations status (registered with the Canadian government for services and benefits) and underrepresented individuals who identified them-selves as native or aboriginal persons. According to 2001 statistics, 1.9% of the population in the greater Vancou-ver region is aboriginal (including North American In-dian, Me´tis, and Inuit persons), compared with 1.2% with First Nations status for those⬍1 year of age in the study cohort, and the proportion of aboriginal persons ⬍4 years of age is probably greater, given a younger age distribution than in the overall population.44Indeed, we
observed a larger proportion of infants of First Nations status (and a higher rate of bronchiolitis) in the excluded
population, which indicates that hazard rate ratios may be underestimated in the current study.
We observed an elevated risk for younger gestational age in the bivariate regression analyses and for the cor-related variable of birth weight in the multivariate anal-yses. Younger infants, including premature infants, are thought to be susceptible to viral infections as a result of missing the transplacental transfer of antibodies.45–47Our
finding of a protective effect for mothers who reported breastfeeding initiation is consistent with the importance of the transfer of maternal antibodies to infants for re-ducing the risk of infection.45,48Lower birth weight and
young gestational age also may indicate a relatively im-mature immune or respiratory system, increasing sus-ceptibility to infection.4,33
Maternal characteristics of younger age and lower so-cioeconomic status were identified previously but may be explained by reduced access to health care services,42 or
lower rates of breastfeeding and smoking status49among
disadvantaged mothers. The current study identified an independent effect of younger maternal age after adjust-ment for breastfeeding initiation and an independent effect of socioeconomic status (education level) after adjustment for smoking status during pregnancy, among a cohort of mothers and infants with universal access to health care services. Although the independent effect of maternal age may be attributable to other, unmeasured, socioeconomic factors, it also may suggest a biological mechanism related to maternal nutrition, health status, or stress that alters the development of the respiratory system of the fetus. The independent effect of socioeconomic status may be a sur-rogate measure for important environmental exposures for infant respiratory outcomes27worthy of further
investiga-tion, including both outdoor (eg, living near major high-ways, with increased exposure to poor air quality) and indoor (eg, wood smoke) air quality exposures. Measures of socioeconomic status (education level) were aggregate, neighborhood-level variables based on Census data and residence. This may result in some misclassification but is considered to be nondifferential in the current study and probably an issue of a 1-category difference, rather than misclassification from the lowest quartile to the highest quartile.
The finding that exposure to maternal smoking was associated with the risk of hospitalized bronchiolitis is in agreement with previous studies33and specifically
find-ings for more-severe infections.18,50Maternal and
pater-nal environmental tobacco smoke has been linked to reduced lung function and increased airway responsive-ness, which may predispose infants to more-severe in-fections.51Although it is likely that a large proportion of
mothers who smoke during pregnancy continue to do so after birth, we had only a measure of maternal smoking during pregnancy. Although this is a potential limita-tion, our finding is consistent with a previous study linking maternal smoking during pregnancy with severe bronchiolitis outcomes (death)18 and provides evidence
that smoking during pregnancy is itself associated with bronchiolitis.
first year of life. Higher birth order is likely associated with having older siblings and/or sharing a room with siblings, which increases the likelihood of viral infection transmission. These specific factors were identified pre-viously as risks for bronchiolitis and other respiratory tract infections6,33and have some public health relevance
for reducing risks associated with crowding during peak periods, especially in public facilities such as day care centers.
One of the main strengths of our study is the large sample that is representative of the population of British Columbia. Unlike most other studies, we investigated the epidemiological features of bronchiolitis by using a population-based sample and a wide range of variables concurrently. The comprehensive risk profile provides direction for recommendations to reduce the incidence and burden of bronchiolitis in the general population. From a public health perspective, interventions are war-ranted to increase breastfeeding initiation and to reduce maternal smoking (especially for reducing the numbers of more-severe, hospitalized cases). Clinicians can sup-port parents to alter these modifiable risk factors, espe-cially for high-risk infants (such as those born with low birth weight or born to young mothers) and during periods of higher risk (such as the first few months after birth and the winter season). In addition, public health practitioners and clinicians need to be aware of the entire environment of the infant and to advise families on making changes that might reduce the risk or severity (hospitalization) of bronchiolitis, such as limiting expo-sure to other young children or outdoor/indoor air pol-lution for at-risk infants during high-risk periods.
ACKNOWLEDGMENTS
Dr Koehoorn was supported in part by the Michael Smith Foundation for Health Research Scholar Award. The research was supported in part by Health Canada via an agreement with the British Columbia Centre for Dis-ease Control to the Border Air Quality Study, and by the Center for Health and Environment Research (CHER) at the University of British Columbia. CHER is funded by the Michael Smith Foundation for Health Research.
The linked research database was provided by the Centre for Health Services and Policy Research, Univer-sity of British Columbia via the British Columbia Linked Health Database. Medical services and hospitalization data were provided by the Ministry of Health, Govern-ment of British Columbia; Vital Statistics data by the British Columbia Vital Statistics Agency; and perinatal data by the British Columbia Reproductive Care Pro-gram.
REFERENCES
1. Shay DK, Holman RC, Newman RD, Liu LL, Stout JW, Ander-son LJ. Bronchiolitis-associated hospitalizations among US children, 1980 –1996.JAMA.1999;282(15):1440 –1446 2. Hall CB. Respiratory syncytial virus and parainfluenza virus.
N Engl J Med.2001;344(25):1917–1928
3. Collins CL, Pollard AJ. Respiratory syncytial virus infections in children and adults.J Infect.2002;45(1):10 –17
4. Welliver RC. Review of epidemiology and clinical risk factors
for severe respiratory syncytial virus (RSV) infection.J Pediatr.
2003;143(5 suppl):S112–S117
5. Langley JM, LeBlanc JC, Smith B, Wang EE. Increasing inci-dence of hospitalization for bronchiolitis among Canadian chil-dren, 1980 –2000.J Infect Dis.2003;188(11):1764 –1767 6. Law BJ, Carbonell-Estrany X, Simoes EA. An update on
respi-ratory syncytial virus epidemiology: a developed country per-spective.Respir Med.2002;96(suppl B):S1–S7
7. Kemper AR, Kennedy EJ, Dechert RE, Saint S. Hospital read-mission for bronchiolitis. Clin Pediatr (Phila). 2005;44(6): 509 –513
8. American Academy of Pediatrics, Subcommittee on Diagnosis and Management of Bronchiolitis. Diagnosis and management of bronchiolitis.Pediatrics.2006;118(4):1774 –1793
9. Piippo-Savolainen E, Remes S, Kannisto S, Korhonen K, Kor-ppi M. Asthma and lung function 20 years after wheezing in infancy: results from a prospective follow-up study.Arch Pediatr Adolesc Med.2004;158(11):1070 –1076
10. Jartti T, Ma¨kela¨ MJ, Vanto T, Ruuskanen O. The link between bronchiolitis and asthma.Infect Dis Clin North Am.2005;19(3): 667– 689
11. Pinquier D, Fauroux B. Acute bronchiolitis in infants [in French].Arch Pediatr.2005;12(spec no. 3):1
12. Dharmage SC, Rajapaksa LC, Fernando DN. Risk factors of acute lower respiratory tract infections in children under five years of age.Southeast Asian J Trop Med Public Health. 1996; 27(1):107–110
13. Lowther SA, Shay DK, Holman RC, Clarke MJ, Kaufman SF, Anderson LJ. Bronchiolitis-associated hospitalizations among American Indian and Alaska Native children.Pediatr Infect Dis J.
2000;19(1):11–17
14. Flores P, Rebelo-de-Andrade H, Goncalves P, et al. Bronchioli-tis caused by respiratory syncytial virus in an area of Portugal: epidemiology, clinical features, and risk factors. Eur J Clin Microbiol Infect Dis.2004;23(1):39 – 45
15. Grimaldi M, Cornet B, Milou C, Gouyon JB. Prospective re-gional study of an epidemic of respiratory syncytial virus (RSV) bronchiolitis.Arch Pediatr.2002;9(6):572–580
16. Jansson L, Nilsson P, Olsson M. Socioeconomic environmental factors and hospitalization for acute bronchiolitis during in-fancy.Acta Paediatr.2002;91(3):335–338
17. Banerji A. High rates of hospitalization for bronchiolitis in Inuit children on Baffin Island.Int J Circumpolar Health.2001;60(3): 375–379
18. Holman RC, Shay DK, Curns AT, Lingappa JR, Anderson LJ. Risk factors for bronchiolitis-associated deaths among infants in the United States.Pediatr Infect Dis J.2003;22(6):483– 490 19. Zamorano A, Marquez S, Aranguiz JL, Bedregal P, Sanchez I.
Association of acute bronchiolitis with climate factors and en-vironmental contamination. Rev Med Chil. 2003;131(10): 1117–1122
20. D’Elia C, Siqueira MM, Portes SA, Sant’Anna CC. Respiratory syncytial virus-associated lower respiratory tract infections in hospitalized infants.Rev Soc Bras Med Trop.2005;38(1):7–10 21. Tsolia MN, Kafetzis D, Danelatou K, et al. Epidemiology of
respiratory syncytial virus bronchiolitis in hospitalized infants in Greece.Eur J Epidemiol.2003;18(1):55– 61
22. Mansbach JM, Emond JA, Camargo CA Jr. Bronchiolitis in US emergency departments 1992 to 2000: epidemiology and prac-tice variation.Pediatr Emerg Care.2005;21(4):242–247 23. Al-Shehri MA, Sadeq A, Quli K. Bronchiolitis in Abha,
south-west Saudi Arabia: viral etiology and predictors for hospital admission.West Afr J Med.2005;24(4):299 –304
25. Ruiz-Charles MG, Castillo-Rendo´n R, Bermu´dez-Felizardo F. Risk factors associated with bronchiolitis in children under 2 years of age [in Spanish].Rev Invest Clin.2002;54(2):125–132 26. Spencer N, Logan S, Scholey S, Gentle S. Deprivation and
bronchiolitis.Arch Dis Child.1996;74(1):50 –52
27. Karr C, Lumley T, Schreuder A, et al. Effects of subchronic and chronic exposure to ambient air pollutants on infant bronchi-olitis.Am J Epidemiol.2007;165(5):553–560
28. Karr C, Lumley T, Shepherd K, et al. A case-crossover study of wintertime ambient air pollution and infant bronchiolitis. En-viron Health Perspect.2006;114(2):277–281
29. Pisacane A, Graziano L, Zona G, et al. Breast feeding and acute lower respiratory infection.Acta Paediatr.1994;83(7):714 –718 30. Simoes EA, King SJ, Lehr MV, Groothuis JR. Preterm twins and triplets: a high-risk group for severe respiratory syncytial virus infection.Am J Dis Child.1993;147(3):303–306 31. McConnochie KM, Roghmann KJ. Parental smoking, presence
of older siblings, and family history of asthma increase risk of bronchiolitis.Am J Dis Child.1986;140(8):806 – 812
32. Holberg CJ, Wright AL, Martinez FD, Ray CG, Taussig LM, Lebowitz MD. Risk factors for respiratory syncytial virus-associated lower respiratory illnesses in the first year of life.
Am J Epidemiol.1991;133(11):1135–1151
33. Lanari M, Giovannini M, Giuffre L, et al. Prevalence of respi-ratory syncytial virus infection in Italian infants hospitalized for acute lower respiratory tract infections, and association between respiratory syncytial virus infection risk factors and disease severity.Pediatr Pulmonol.2002;33(6):458 – 465 34. Chamberlayne R, Green B, Barer ML, Hertzman C, Lawrence
WJ, Sheps SB. Creating a population-based linked health database: a new resource for health services research.Can J Public Health.1998;89(4):270 –273
35. Practice Management Information.International Classification of Diseases, Ninth Revision: Clinical Modification. 6th ed. Los Angeles, CA: Practice Management Information; 2003
36. du Plessis V, Beshiri R, Bollman RD, Clemenson H. Definitions of “Rural.” Ottawa, Canada: Statistics Canada, Agricultural Division; 2002. Agriculture and Rural Working Paper Series Working Paper 61
37. Cox DR. Regression models and life tables.J R Stat Soc Ser B Stat Methodol.1972;34(2):187–220
38. Canadian Institute for Health Information; Canadian Lung Association; Health Canada; Statistics Canada.Respiratory Dis-ease in Canada. Ottawa, Canada: Health Canada; 2001 39. McIntyre E, Brauer M, Demers PA, Lencar C, Ostry A.
Assess-ment of the Validity and Reliability of Selected Maternal Risk Factor Data Obtained From the British Columbia Perinatal Database. Ot-tawa, Canada: Health Canada; 2007
40. Statistics Canada. Canadian Community Health Survey cycle 3.1 public use microdata. Available at: http://data.library.ubc. ca. Accessed December 13, 2007
41. Simoes EA. Respiratory syncytial virus infection.Lancet.1999; 354(9181):847– 852
42. Smyth RL, Openshaw PJM. Bronchiolitis. Lancet. 2006; 368(9532):312–322
43. Arnold SR, Wang EE, Law BJ, et al. Variable morbidity of respiratory syncytial virus infection in patients with underlying lung disease: a review of the PICNIC RSV database.Pediatr Infect Dis J.1999;18(10):866 – 869
44. British Columbia Statistics.British Columbia Statistical Profile of Aboriginal Peoples, 2001, With Emphasis on Labour Market and Post Secondary Education Issues.Victoria, British Columbia: Govern-ment of British Columbia; 2001. Available from www.bcstats. gov.bc.ca/data/cen01/abor/tot㛭abo.pdf. Accessed July 23, 2007 45. Ogilvie MM, Vathenen AS, Radford M, Codd J, Key S. Mater-nal antibody and respiratory syncytial virus infection in in-fancy.J Med Virol.1981;7(4):263–271
46. Wong DT, Ogra PL. Neonatal respiratory syncytial virus infection: role of transplacentally and breast milk-acquired antibodies.J Virol.1986;57(3):1203–1206
47. Hall CB, Kopelman CB, Douglas JRG, Geiman JM, Meagher MP. Neonatal respiratory syncytial virus infection. N Engl J Med.1979;300(8):393–396
48. Roine I, Fernandez JA, Vasquez A, Caneo M. Breastfeeding reduces immune activation in primary respiratory syncytial virus infection.Eur Cytokine Netw.2005;16(3):206 –210 49. Li R, Ogden C, Ballew C, Gillespie C, Grummer-Strawn L.
Prevalence of exclusive breastfeeding among US infants: the Third National Health and Nutrition Examination Survey (phase II, 1991–1994). Am J Public Health. 2002;92(7): 1107–1110
50. Wright AL, Holberg C, Martinez FD, Taussig LM. Relationship of parental smoking to wheezing and nonwheezing lower re-spiratory tract illnesses in infancy. J Pediatr. 1991;118(2): 207–214
51. Adler A, Ngo L, Tosta P, Tager IB. Association of tobacco smoke exposure and respiratory syncitial virus infection with airways reactivity in early childhood. Pediatr Pulmonol. 2001;32(6): 418 – 427
DOI: 10.1542/peds.2007-2231
2008;122;1196
Pediatrics
and Michael Brauer
Mieke Koehoorn, Catherine J. Karr, Paul A. Demers, Cornel Lencar, Lillian Tamburic
Cohort
Descriptive Epidemiological Features of Bronchiolitis in a Population-Based
Services
Updated Information &
http://pediatrics.aappublications.org/content/122/6/1196
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/122/6/1196#BIBL
This article cites 45 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/bronchiolitis_sub
Bronchiolitis
http://www.aappublications.org/cgi/collection/epidemiology_sub
Epidemiology
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-2231
2008;122;1196
Pediatrics
and Michael Brauer
Mieke Koehoorn, Catherine J. Karr, Paul A. Demers, Cornel Lencar, Lillian Tamburic
Cohort
Descriptive Epidemiological Features of Bronchiolitis in a Population-Based
http://pediatrics.aappublications.org/content/122/6/1196
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.