Kangaroo Care:
Creating a Video Teaching Tool for Parents and Neonatal Nurses
Melissa Robinson
A Project presented to the faculty of The University of North Carolina at Chapel Hill
in fulfillment of the requirements for Undergraduate Honors
Date Completed: March 28, 2014
Honors Advisor Approval: ___________________________ Rhonda Lanning, RN MSN CNM IBCLC
Abstract
Kangaroo Care (KC) is the process of holding an infant skin-to-skin, a timeless technique with scientific benefits revealed in the 1970’s (Johnson, 2013). With a thorough literature review, many benefits of KC were discovered for infants, parents, and nurses. Many professional health care organizations support the implementation of KC early in the infant’s life, as neonates are better regulated by their mothers as compared to hospital incubators (Mori, Khanna, Pledge & Nakayama, 2010). A survey of nurses (n=70) was conducted at the Newborn Critical Care Center (NCCC) at UNC Hospitals to identify a possible need for increased KC education, evaluate the nurses’ perceptions of KC, and establish a preference for a teaching tool. The majority of those surveyed (64%) agreed a video would be the most effective medium to educate both parents and nurses on KC. In addition, research has shown that videos serve as an effective tool to educate patients in a cost-effective manner (Shah, Swanson, Nobay, Peterson, Caprio & Karuza, 2012). A DVD explaining the benefits of KC was created, and the proper transfer technique for KC was demonstrated. This teaching tool is intended to be used in the NCCC to educate parents and nurses on the benefits of KC for infants, and to increase implementation of KC.
Introduction
Kangaroo Care (KC), a term describing the process of a parent holding an infant skin-to-skin, was developed in 1979 in Bogota, Columbia, when hospitals experienced a shortage of infant incubators (Whitelaw & Sleath, 1985). Dr. Edgar Rey, who piloted KC in Bogota,
understood that a mother’s warm body could regulate her infant’s temperature and also facilitate breastfeeding (Thukral, Chawla, Agarwal, Deorari & Paul, 2008). Since Dr. Rey’s initial work with KC, many benefits for the infant, mother, father, and hospital staff have been identified. The term KC comes from the method of caregiving that kangaroos provide. The kangaroo mother serves as an incubator to keep her joey warm until it can manage extrauterine life (Funk, Tilney, Mitchell & Walker, 2012).
About 15 million babies are born prematurely each year, which equates to more than 1 in 10 babies worldwide (Blencowe et al., 2012). Prematurity is the leading cause of newborn death, and after pneumonia, is the second leading cause of all child deaths, so these babies need extra care, including KC (Lawn, Cousens & Zupan, 2005). More than 80% of premature babies die from lack of simple care such as temperature regulation and feeding support (Lawn, Mwansa-Kambafwile, Horta, Barros & Cousens, 2010). KC can provide these essential life-saving measures, and could save an estimated 450,000 babies each year if KC is implemented (Lawn et al., 2010). For years, professional health care organizations such as the American Academy of Pediatrics (AAP), the Association of Women’s Health, Obstetric and Neonatal Nurses
(AWHONN), and the National Association of Neonatal Nurses (NANN) have recommended KC because of the innumerable health benefits for both infants and families (Ludington-Hoe & Morgan, 2013).
From a previous externship in a Neonatal Intensive Care Unit (NICU), I experienced the inconsistencies of initiating KC and performing the KC transfer. After observing the hesitancy I noted in some nurses and parents, I wanted to create a teaching tool that explains to parents and nurses how beneficial KC is compared to any risks involved with transferring the baby. Many infants in the NICU are attached to multiple lines, tubes, and drains, so moving them poses a risk for the equipment to dislodge from the infant. Some nurses may fear the detachment of the equipment because they provide life saving medication and oxygenation, and it can be difficult to reattach or reinsert the lines. In addition, premature babies are very small and fragile, so parents fear that picking the infant up will cause the baby harm.
My hope is that creating this tool will ease the concerns for many nurses and parents who are hesitant to move their baby, and to initiate KC with greater consistency. I believe this video will encourage neonatal nurses to advocate for family bonding and developmentally appropriate care.
A survey of nurses from the Newborn Critical Care Center (NCCC) at UNC Hospitals identified a need for an educational tool about KC. In response to the nurses’ opinions gathered from the survey and research evidence from scholarly articles, a video teaching tool was
produced. This educational video was created for nurses and parents and it describes the benefits of KC for the infant, parents, and staff, as well as the correct transfer procedure for KC based on the NCCC’s policy. The intent of this video is to educate parents on KC and the benefits it provides, and also to review the KC transfer policy for any nurses or parents who are uncertain about initiating KC.
Review of Literature
According to the Nils Bergman, full time KC researcher and promoter, KC is defined as holding a diapered baby, in the prone, upright position, on the mother or father’s naked chest with a blanket draped over the baby’s back (Bergman & Bergman, 2013). KC, also referred to as Kangaroo Mother Care or Skin-to-Skin Care, can be done with preterm, high risk, and healthy newborns (Nursing Policy Committee, 2013). It is recommended that infants be held for at least an hour, because that is the optimal time for the infant to naturally find the breast (Caruana, 2008).
Benefits of KC for Neonates
KC has many evidence-based benefits for premature babies, those born before 38 weeks gestation. Low birth weight (LBW) is a significant problem among premature infants, affecting about 20 million babies each year (Samra, Taweel & Cadwell, 2013). A study conducted by Samra, Taweel, and Cadwell (2013) compared a group of infants’ post-birth weight gain using KC and a control group. The infants held skin-to-skin had a significantly higher daily weight gain and regained their birth weight sooner than the control group. In addition, a review of several randomized control trials found that KC is associated with a 51% reduction in neonatal mortality for LBW babies if started in the first week, compared to incubator care (Lawn, Mwansa-Kambafwile, Horta, Barros & Cousens, 2010).
Pain management is a central issue to promote development in neonates, because uncontrolled pain can lead to lower pain thresholds later in infancy and during adolescent
development (Kashaninia, Sajedi, Rahgozar & Noghabi, 2008). Nonpharmacologic methods, like KC, are appropriate to alleviate procedural pain because of their short-term effectiveness,
(Kashaninia et al., 2008). In a study conducted by Kashaninia, Sajedi, Rahgozar, and Noghabi (2008), babies held in KC for 10 minutes cried significantly less than the babies left in their incubators. Only 6% of the KC babies were scored as having severe pain using the Neonatal Infant Pain Scale, compared to 60% of the incubator babies (Kashaninia et al., 2008). KC also reduces physiologic instability during painful procedures and stimulates faster recovery from pain (Ludington-Hoe & Morgan, 2013). During KC, the mother and infant together reduce their cortisol-based stress level during painful procedures, and KC has been shown to eradicate the brain’s pain memory and pathways that lead to long-term adverse effects of pain (Meek & Huertas, 2012; Castral et al., 2012). Other interventions to control pain such as sucrose
(TootSweet 24% sucrose solution) have been identified as pain-control techniques, but compared to other ways, KC does a better job of relieving when used as single intervention to decrease pain (Meek & Huertas, 2012).
Hypoglycemia, or low blood sugar, can be a significant problem in infants with diabetic mothers, or even premature infants who metabolize energy stored as glucose to maintain body heat (Morgan & Ludington-Hoe, 2013). Studies report a decreased incidence of hypoglycemia during KC when compared to incubator care (Morgan & Ludington-Hoe, 2013). Because of these findings, KC is recommended as a treatment to prevent or reverse hypoglycemia without requiring food intake (Munson, Saatkamp & West, 2011).
Sepsis is another difficult problem to treat and prevent in premature infants because of the immature immune system. For a variety of reasons, KC has been found to reduce the risk and number of hospital-acquired infections in preterm infants (Morgan & Ludington-Hoe, 2013). KC enhances skin hydration so the infant’s skin, the body’s first line of defense, is better protected from infections (Abouelfettoh, Ludington-Hoe, Burant & Visscher, 2011). In addition, an infant
can pass antigens to the mother during KC, and the mother can then pass antibodies back to the infant, which can fight the antigens even 2 to 3 days later (Ludington-Hoe, 2011). As a result of such findings, the Canadian Pediatric Society endorses KC as a method to reduce the number of infections in premature infants (Jefferies, 2012).
KC contributes to neurodevelopment in premature infants because it accelerates brain development and infants who were given KC also have better mental function throughout their lives (Morgan & Ludington-Hoe, 2013). It is thought that brain development occurs with KC because cerebral oxygenation increases, sleep cycles are improved, and the infants receive multisensory stimulation in a pleasing manner (Morgan & Ludington-Hoe, 2013).
Human breast milk provides many benefits for newborns compared to human milk substitutes. These benefits include: reduced risk of infection, increased neurodevelopment, and protection from Type II diabetes (Ahmed & Sands, 2010). The American Academy of Pediatrics recommends KC as a method to increase breastfeeding success, specifically stating that healthy newborns should remain skin-to-skin with their mother until after the first breastfeeding (Bagby & Bowen, 2012). A KC program originating at the University of Louisville Hospital found that breastfeeding initiation rates increased from 51% in July 2010 to 74% in July 2011 during the time of KC initiation (Bagby & Bowen, 2012). The percentage of mothers and infants
documented as participating in KC in the mother–baby unit also increased from 35% to 51% (Bagby & Bowen, 2012). In another study, the t-test showed that very preterm babies that received human milk had experienced more time in KC per day compared to the babies that did not breastfeed or drink their mother’s milk (Flacking, Ewald & Wallin, 2011). Holding an infant to a mother’s chest increases her milk letdown and ability to express milk, as evidenced in a study by Lau, Hurst, Smith, and Schanler (2007). The study showed that a mother’s maintenance
of milk expression correlated positively with infant birthweight and KC holding (Lau, Hurst, Smith & Schanler, 2007). KC not only increases the likelihood of infant breastfeeding, but also the mother’s ability to express milk.
Regulation of temperature is a significant benefit of KC, as evidenced in a meta-analysis by Mori, Khanna, Pledge, and Nakayama (2010). 22 studies showed during KC, an infant’s temperature can increase by 0.22°C, and 12 studies showed the temperature after KC can increase by 0.14°C (Mori, Khanna, Pledge & Nakayama, 2010). Temperature regulation is important for many reasons, as noted by Turnbull and Petty (2013):
Risk of hypothermia is higher in premature babies because of the child’s ineffective positioning ability, greater body water content, decreased subcutaneous and brown fat, immature skin, reduced ability to peripherally vasoconstrict and poorly developed metabolic mechanisms. (p. 18)
A study by Ludington-Hoe et al. (2006), found that mothers’ breasts were able to change
temperature according to their infants’ temperature when holding twins. For example, a mother’s left breast decreased in temperature when twin A’s temperature increased, while the mother’s right breast increased in temperature when twin B’s temperature decreased (Ludington-Hoe et al., 2006).
Several studies have explored the effect of KC on twins and triplets. Jarvis and Burnett (2009) reported that a set of triplets moved closer to each other, “hugged” one another, and had synchronized sleep time after being held by their mother. The study described above by
Ludington-Hoe et al. (2006) also shows that twins can be held in KC and the mother’s breasts can individually regulate their temperature. According to Jarvis and Burnet (2009), multiple-gestation neonates can use KC as a developmentally supportive method, but the authors report
more research is needed before shared KC can be commonplace in the NICU because of the potential for infection spreading between siblings.
Kangaroo Care is also beneficial in dire situations such as when unstable infants are born outside of the hospital. Preterm infants born outside the hospital have double the mortality compared with infants born in a hospital (Funk, Tilney, Mitchell & Walker, 2012). Using KC during transportation to a hospital has been noted as an acceptable way to transport an infant. This means of transport involves smoother movements and improved infant containment
compared with a conventional isolette, and this mode of transport aids mother/infant bonding and regulates the infant’s temperature (Funk, Tilney, Mitchell & Walker, 2012). The Transport Risk Index of Physiologic Stability (TRIPS) scale identifies temperature, BP, respiratory status and response to harmful stimuli as the main predictors of illness severity upon admission to the NICU. KC addresses all of these predictors, making KC transport a better transportation method than an incubator (Ludington-Hoe & Morgan, 2013). Currently, Louisville, Kentucky is the only city where emergency medical services providers are being educated on the benefits of KC transport (Ludington-Hoe & Morgan, 2013).
Benefits of KC for Mothers
Mothers with ill or preterm infants are at a higher risk for postpartum depression, which includes symptoms such as fear, despair, sadness, and anxiety (Bigelow, Power, MacLellan-Peters, Alex & McDonald, 2012). Postpartum depression can also have an effect on the mother’s infant. These children are at risk for cognitive, social, and emotional developmental difficulties (Bigelow et al., 2012). One study conducted by Bigelow et al. (2012), found that mothers who provided KC for approximately 6 hours a day reported fewer symptoms of depression using the Edinburgh and the CES-D scales than mothers in the control group. The mother’s salivary
cortisol levels were also measured, and the study reported that mothers in the KC group had a greater reduction in salivary cortisol than the control group. This indicates that mothers’ physiological stress during the infants’ first month of life was decreased in the KC group compared to the control group (Bigelow et al., 2012).
In addition to a risk of postpartum depression, mothers with children in the NICU have expressed feelings of separation, exclusion, and helplessness (Kearvell & Grant, 2010). Multiple studies have shown that mothers who provide KC have enhanced mother-infant attachment and had the opportunity to get to know one another in a great way (Kearvell & Grant, 2010). This sense of attachment during KC also increased maternal confidence (Kearvell & Grant, 2010). In another study, infants who engaged in early KC demonstrated higher maternal-child interaction scores after 1 year of age, compared with those who did not engage in early skin-to-skin contact (Haxton, Doering, Gringras & Kelly, 2012).
When the infant lies on the mother’s stomach during KC, oxytocin is released in the mother’s brain, decreasing maternal pain perception and discomfort (Lindgren et al., 2012). This interaction between mother and child can be especially healing for mothers after a cesarean section or painful vaginal birth. In addition, both short and long-term stress was found to decrease in mother’s who participated in KC (Flacking, Thomson, Ekenberg, Lowegren & Wallin, 2013).
Benefits of KC for Fathers
Despite the common phrase ‘Kangaroo Mother Care,’ KC can be provided by fathers as well. Separation from the infant, a lack of control, and a struggle to gain control are common feelings expressed among fathers with infants in the NICU (Blomqvist, Rubertsson, Kylberg, Joreskog & Nyqvist, 2012). Much like mothers, when fathers are active in their infant’s care,
their attachment and confidence increase (Blomqvist et al., 2012). KC and touching the infant makes fathers feel like an important participant in the infant’s care, and it helps them realize the infant is real and their own (Fegran, Helseth & Fagermoen, 2008). The study by Fegran, Helseth, and Fagermoen (2008) found that after fathers performed KC, they felt they were caring for the infant in a natural way and father–infant attachment increased. Another study found that both parents should be directly involved in KC, which supports fathers’ participation in KC as equal to mothers’ (Tessier et al., 2009).
KC does not just apply to the traditional mother-father dyad. Same-sex couples, in addition to other caregivers such as aunts, uncles, and grandparents, are eligible to perform KC. Research regarding the benefits of KC for these caregivers has not yet been conducted, so further studies using these caregivers are needed.
Benefits of KC for Staff
While KC directly impacts infants and parents, KC can also positively affect NICU staff and the hospital system. The study by Lima, Quintero-Romero, and Cattaneo (2000) reports that KC reduces hospital stay and nursing load, which ultimately reduces hospital expenses. Staff members recognize that KC is beneficial in reducing parent stress and increasing parent comfort, so educating and encouraging parents to perform KC may indirectly decrease nurses’ stress (Cooper et al., 2007).
Cooper (2013) explained that KC increases parent satisfaction, so the families that are satisfied with care are more likely to contribute to a pleasant work environment for staff. Time and workload for staff also decrease as infants stabilize during KC, and the parent-staff
Development of a Teaching Tool:
With the cost of DVD production becoming more affordable, video education is becoming a viable educational approach compared to the standard written material education. Videos are an effective tool for patients who have auditory or visual learning styles and they may aid patients who have low functional health literacy to understand the content that is being shared (Hill et al., 2009).
A study that created an educational video on fecal occult blood tests for colorectal cancer patients found that actual demonstration of the test was needed to provide more detailed
instruction (Katz et al., 2009). The patients also recommended that the video include a physician, because their authoritative voice has shown to be a significant motivator for patients to complete the fecal occult blood tests (Katz et al., 2009).
In addition to satisfaction and information retention with video education, another study showed that videos can lead to behavior change. The study by Lovarini and Bawden (2010) found participants were strongly motivated to prevent themselves from falling and had greater confidence in their abilities after watching a video, compared to participants who used written materials for education.
The University of Rochester developed video podcasts for continuing medical education to be used by emergency medical services personnel. The researchers found that video podcasts offer the flexibility to be played on demand, repeated if necessary, and they offer consistency in content and teaching ability (Shah, Swanson, Nobay, Peterson, Caprio & Karuza, 2012). The participants enjoyed the convenient access to the videos, and recommended using videos as the media for future educational opportunities (Shah et al., 2012).
Malcolm Knowles recognized that adults learn distinctly from children, and focused on the principle of andragogy, which says adults should be in control of their own learning (Mitchell & Courtney, 2005). Knowles’ Adult Learning Theory describes six key elements that lead to optimal learning in adults: “a need to know; a responsibility for one’s own learning; the role of experience as a resource in one’s learning; a readiness or applicability of the information to one’s life situation; motivation to learn; and problem-centered learning with real-life problems,”
(Mitchell & Courtney, 2005). These elements were considered when creating the video teaching tool because other interventions that incorporated these features were found to positively affect learning outcomes (Mitchell & Courtney, 2005).
To address the first element of the Adult Learning Theory, the benefits of KC were presented in the video to explain why KC should be initiated. The video encouraged parents to visit websites for additional resources, which gives adults a responsibility for their own learning. The assumption could not be made that adults have prior experience being in a NICU
environment, so drawing on their past experiences was not addressed. The information in the teaching tool was made applicable to the adult’s situation because it described the types of babies that are suitable to be held, and how to perform KC. The benefits of KC for mothers and fathers that were described in the video should have provided internal motivation for the parents to want to initiate KC. If the parents were not internally motivated, the kangaroo stuffed-animal was presented in the video as a present to parents who performed KC for the first time. The final element of Knowles’ theory was addressed because real-life problems of premature infants were described, as well as how KC can address and alleviate the problems that neonates may
As this literature review suggests, videos are a convenient and effective way to educate patients. The viewing of videos can be flexible, and production is cost-effective.
Methods
Rates of implementation of KC at the NCCC at UNC Hospitals was reported as low by nursing staff leaders in the NCCC. In order to assess learning needs, an online survey was conducted in the NCCC from December 26, 2013 to January 15, 2014. Candy and chocolates, as requested by the nurses, were provided as an incentive for completing the survey. The survey questions were reviewed by a UNC Qualtrics specialist, in addition to Rhonda Lanning, the academic advisor for this project, and Julie Calacday, RN at the NCCC and leader of the NCCC Developmental Care Committee. The proposal submitted to the UNC Institutional Review Board was determined to be exempt as defined under federal regulations [45 CFR 46.102 (d or f) and 21 CFR 56.102(c)(e)(l)]. UNC Qualtrics software was used to implement the survey, and a private link was emailed to the NCCC nursing staff (approximately 100 nurses). Each nurse could only complete the survey once. 70 nurses completed the online survey. Each survey question was optional, so the number of responses fluctuated for each question. The questions asked about the nurses’ opinions on what they believed to be important about KC, and what their perceptions about the importance of certain KC topics were for parents. Many questions involved ranking statements using a Likert scale. After most questions, a blank text box was provided for nurses to provide additional feedback or information that was not gathered from answering the question. The nurses were also asked about their personal comfort level with KC, and their opinions on any KC training received since working at the NCCC. Finally, the nurses were asked their preference of different media for learning the KC transfer policy, in addition to what type of media they thought would be helpful for parents to learn the KC transfer policy. The KC transfer
policy describes how to properly transfer an infant from the incubator or warmer bed to the provider of KC. The KC transfer procedure can be done with the KC provider either sitting or standing. A copy of the survey questions is included in Appendix A.
The NCCC KC policy was examined to ensure accuracy of information presented in the video. After examining the results of the survey, several topics were chosen to be included in the video. The topics selected for inclusion in the teaching video were:
• Description and history of KC
• Benefits of KC for the infant, mother, father, and staff
• Barriers to implementing KC and recommendations of how to overcome barriers • Supplies needed to implement KC
• Recommendations for parents to promote comfort during KC • Demonstration of a KC sitting transfer
• Demonstration of a KC standing transfer • List of additional resources for parents
Diane Hudson-Barr, NCCC Clinical Nurse Specialist, and Dr. Karen Wood, Medical Director of the NCCC, were interviewed for the video. Knowles’ Adult Learning Theory and six core elements of education also guided the production of the video to appeal to the learning style of adults. Katie Bruce, a media production student from the University of North Carolina at Chapel Hill, assisted in recording the interviews and transfer procedure, and producing the video.
After the video was reviewed by Rhonda Lanning and Julie Calacday, copies of the video were produced on DVDs and given to the NCCC to be used by nurses and parents in need of KC education. A copy of the video is presented in Appendix B.
Results
A total of 70 NCCC nurses completed the optional online survey; 74 nurses agreed to take the survey (Question 1), but four surveys were eliminated because none of the following questions (Question 2-19) were answered. The results were synthesized using the UNC Qualtrics software.
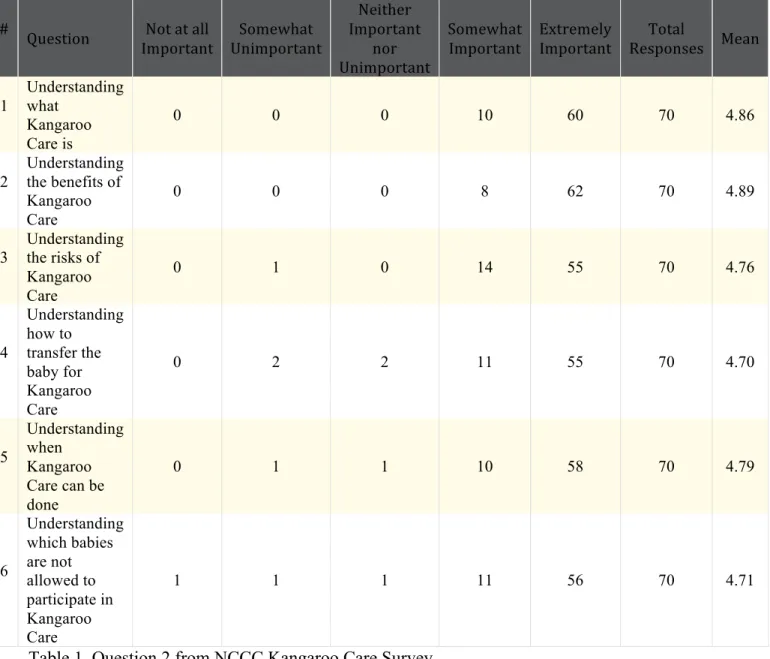
Table 1 shows the results of Question 2, which asked nurses to “Please rank the following statements according to what you perceive to be important or not important for parents
# Question Not at all Important Somewhat Unimportant Neither Important nor Unimportant Somewhat Important Extremely Important Total Responses Mean 1 Understanding what Kangaroo Care is 0 0 0 10 60 70 4.86 2 Understanding the benefits of Kangaroo Care 0 0 0 8 62 70 4.89
3 Understanding the risks of Kangaroo Care 0 1 0 14 55 70 4.76 4 Understanding how to transfer the baby for Kangaroo Care 0 2 2 11 55 70 4.70 5 Understanding when Kangaroo Care can be done 0 1 1 10 58 70 4.79 6 Understanding which babies are not allowed to participate in Kangaroo Care 1 1 1 11 56 70 4.71
Table 1. Question 2 from NCCC Kangaroo Care Survey
78.6% of nurses thought parents would benefit from understanding the risks of KC, whereas 88.6% of nurses thought parents would benefit from understanding the benefits of KC. Overall, a high percentage of nurses thought each topic would benefit parents. Question 3 allowed nurses to write what else they perceived to be important for parents to understand or learn regarding KC. Nine out of twenty responses addressed the fact that parents should know KC is expected to be done for an hour or more for each session, and two nurses wrote that the clothing worn by parents should be smoke and perfume free. One unique response included a
comment that read, “Encourage [parents] to tell nurses they want to do KC, even if it has not yet been offered. Empowerment!” and another comment that read, “Perhaps a short video
highlighting the pros and cons of kangaroo care before the initial kangaroo session [would be] helpful!”
Questions 6-10 referred to the nurses’ experience based on the past two weeks of work in the NCCC. A majority of the nurses worked 6 shifts in the past two weeks from the date of taking the survey, but only 28 of 70 nurses performed KC during those 6 shifts. When asked of those patients, how many were not allowed to participate in KC, only seven nurses had patients that did not meet criteria for participation. Approximately 36 other nurses had patients that were eligible to participate in KC, but did not. 22 of 70 nurses (31.4%) also reported educating parents on KC and 12 of 70 (17%) assisted other nurses with the KC transfer procedure.
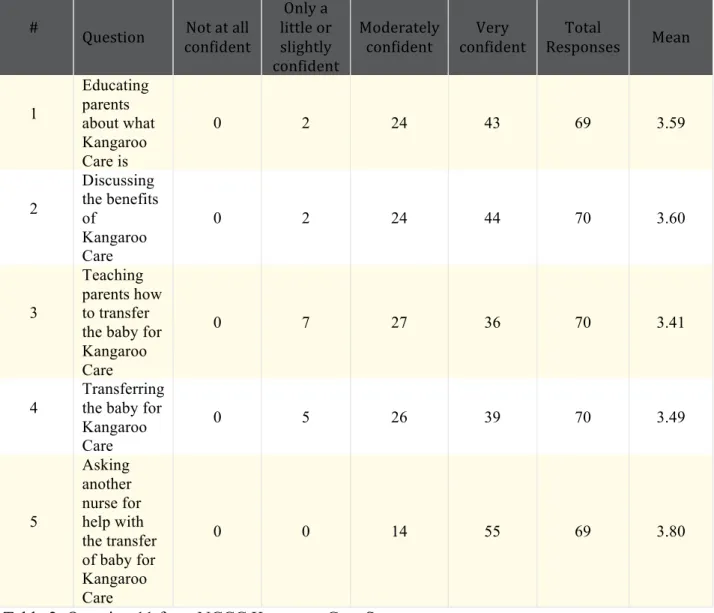
Question 11, shown in Table 2, asked the nurse to rate his/her confidence in his/her ability to perform five tasks.
# Question Not at all confident Only a little or slightly confident Moderately confident Very confident Total Responses Mean 1 Educating parents about what Kangaroo Care is 0 2 24 43 69 3.59 2 Discussing the benefits of Kangaroo Care 0 2 24 44 70 3.60 3 Teaching parents how to transfer the baby for Kangaroo Care
0 7 27 36 70 3.41
4
Transferring the baby for Kangaroo Care 0 5 26 39 70 3.49 5 Asking another nurse for help with the transfer of baby for Kangaroo Care 0 0 14 55 69 3.80
Table 2. Question 11 from NCCC Kangaroo Care Survey
While the majority of nurses were “very confident” in their ability to perform each task, it should be noted that seven nurses felt “only a little or slightly confident” teaching parents how to perform the KC transfer. In addition, this task had the lowest percentage of “very confident” responses (51.4%). The second lowest percentage of “very confident” responses and the second highest percentage of “only a little or slightly confident” responses was recorded for the
“transferring a baby for KC” task.
Question 13 asked nurses “How satisfied are you with the Kangaroo Care training you have received while working in the NCCC?” The results are shown in Table 3.
# Answer Response % 1 Very Dissatisfied 7 10% 2 Somewhat Dissatisfied 13 19% 3 Neither Satisfied nor Dissatisfied 9 13% 4 Somewhat Satisfied 27 39% 5 Very Satisfied 13 19% Total 69 100%
Table 3. Question 13 from NCCC Kangaroo Care Survey
19% of those surveyed reported being only “very satisfied” with the KC training they have received, and notably, 19% reported being “somewhat dissatisfied”.
Question 14 allowed nurses to explain how they felt about the KC transfer. One nurse wrote, “I have never had training,” and another nurse asked to have additional training. A common theme among responses was concerns for intubated babies, because tube dislodgment or extubation is a risk during the transfer process. Another common response was a need for consistency with teaching the transfer process.
Question 15 asked, “How do you think other nurses on your unit feel about transferring a baby for Kangaroo Care? Please feel free to elaborate.” 5 out of 40 nurses commented that newer and inexperienced nurses appear more hesitant to initiate KC, and 7 out of 40 comments
mentioned concern for endotracheal tube and IV dislodgment.
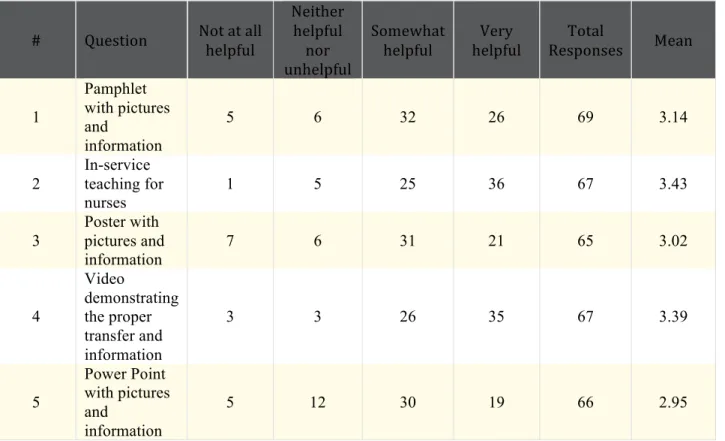
Question 16 asked nurses, “How helpful would the following be for you to learn or review how to properly transfer a baby for Kangaroo Care?” As shown in Table 4, 52.2% of nurses agreed that a KC video would be “very helpful” to learn or review the KC transfer. 53.7% of nurses thought an in-service session about KC would be “very helpful”. Question 17 allowed nurses to additionally comment on anything else that would be helpful for them to learn the KC transfer, and two of nine nurses wrote that “ a video with information on the risks and benefits of
kangaroo care, when it is and is not appropriate, [and the] importance of doing kangaroo care,” would be helpful.
# Question Not at all helpful
Neither helpful
nor unhelpful
Somewhat
helpful helpful Very Responses Total Mean
1 Pamphlet with pictures and information 5 6 32 26 69 3.14 2 In-service teaching for nurses 1 5 25 36 67 3.43 3 Poster with pictures and information 7 6 31 21 65 3.02 4 Video demonstrating the proper transfer and information 3 3 26 35 67 3.39 5 Power Point with pictures and information 5 12 30 19 66 2.95
Table 4. Question 16 from NCCC Kangaroo Care Survey
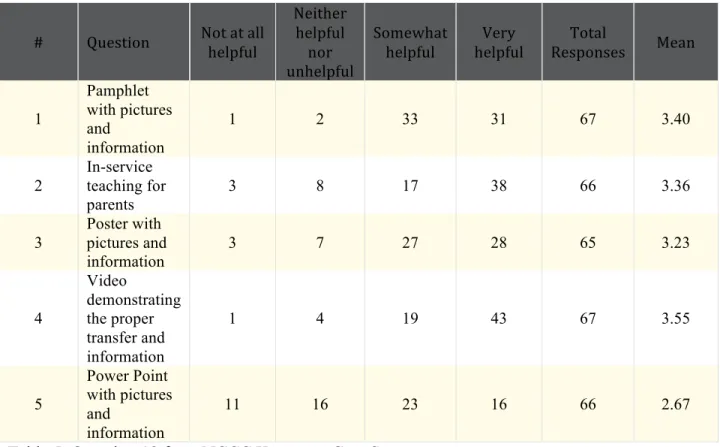
Similar to Question 16, Question 18 asked nurses “How helpful do you think the
following would be for parents to learn or review how to properly transfer a baby for Kangaroo Care?” According to Table 5, 64.2 % of nurses reported that a video would be “very helpful” for parents to learn the KC transfer, and only one nurse out of 67 thought the video would be “not at all helpful”.
# Question Not at all helpful Neither helpful nor unhelpful Somewhat helpful Very helpful Total Responses Mean 1 Pamphlet with pictures and information 1 2 33 31 67 3.40 2 In-service teaching for parents 3 8 17 38 66 3.36 3 Poster with pictures and information 3 7 27 28 65 3.23 4 Video demonstrating the proper transfer and information 1 4 19 43 67 3.55 5 Power Point with pictures and information 11 16 23 16 66 2.67
Table 5. Question 18 from NCCC Kangaroo Care Survey Discussion
The findings from the online survey in the NCCC reveal that nurses believe a KC video would be an effective teaching-tool for both nurses and parents. Question 2, “Please rank the following statements according to what you perceive to be important or not important for parents when learning about Kangaroo Care,” guided the emphasis of topics to be included in the video. Because more nurses reported the KC benefits would be more helpful for parents to learn compared to KC barriers, the benefits were more heavily focused on in the video. Overall, a majority of nurses agreed each topic in Question 2 was important for parents to learn, which is why they are all addressed in the video to some degree. The nurses’ comments from Question 3, such as the need for parents to wear odorless clothing, and to KC for at least an hour, provided additional and beneficial content to be included in the video.
Question 11 asked, “How confident do you feel in your ability to do each of the
following items below?” It is worrisome that seven nurses felt “only a little or slightly confident” teaching parents the KC transfer, because educating parents on the KC transfer is a task that should be done by all nurses with great confidence. Nurses are the primary motivators for parents to initiate KC, so proper training for nurses is needed to provide excellent patient education. The same can be said for a low percentage of nurses feeling “very confident” for the task of
“transferring a baby for KC”. In addition to KC transfer education, all nurses should feel confident in the actual transfer procedure.
A total of 29% of nurses surveyed reported being “somewhat dissatisfied” and “very dissatisfied” with the KC training they have received, as shown in Question 13. While 39% reported being “somewhat satisfied,” KC education should be very satisfying to all nurses since KC is such a crucial aspect of infant care.
Because nurses expressed concern for ET tube dislodgment in Question 14 and 15, an intubated baby doll was used in the teaching video. This video will also fulfill the need for consistency with training as addressed in Question 14, and hopefully newer nurses will feel more confident initiating KC with the creation of this video, as mentioned in Question 15.
A video teaching-tool was created using the knowledge that 52.2% of nurses agreed that a KC video would be “very helpful” to learn or review the KC transfer, and that 64.2 % of nurses reported that a video would be “very helpful” for parents to learn the KC transfer. In addition, as noted in the literature review, the study by Katz et al., 2009 found that patients preferred viewing an actual demonstration so that more detailed instruction could be provided.
In order to more fully investigate and use and usefulness of this video education tool, parent and nurse evaluation should be implemented in the NCCC. It is anticipated that as more families and nurses view this video, awareness will increase among staff and other parents.
Implications for Future Practice
This video is intended to be used as a teaching tool for parents and nurses in the NCCC. When parents are new to the unit and in need of KC education, nurses can use this video to educate parents. In addition, if nurses are in need of education and review of the KC transfer process, they may view this video at the NCCC as well. After parents view the video, nurses can be available at the bedside to answer any questions that parents may still have regarding KC.
If a budget allows, numerous copies of the DVD can be stored in the NCCC so that each parent can go home with a copy. This will allow parents to refer to the DVD if they have
questions about KC once home with their child, because KC can be done even after the infant is discharged from the NICU.
Future plans include distributing this video to other hospitals to use as KC education in their neonatal units. Other plans include adding Spanish subtitles to the video so that Spanish-speaking families may receive KC video education. The video could also serve as a Learning Management System (LMS) training module for the NCCC. Submission to a pediatric nursing journal is also being considered, as the video could be shared more widely in this forum.
Limitations
There are several limitations to this educational video. The survey sample was targeted to a specific NICU, so KC experiences and preferences for a teaching tool may not be generalized to other hospital NICUs. As with many nursing procedures, changes to the KC transfer policy may occur in the future, which would lead to revisions of this teaching tool. This video only
serves English speaking families, and does not account for individuals who may be deaf and/or blind. Additionally, this video has only been reviewed by two nurses, and has not been reviewed by parents of infants in the NCCC. Further evaluation of the video by a variety of nurses and parents will be needed to determine the video’s effectiveness.
Conclusion
KC provides innumerable benefits to infants hospitalized in a NICU setting, in addition to mothers, fathers, and NICU staff. Because KC is a task that only parents can participate in, it is crucial that nurses educate parents on KC. It is important that nurses understand what the benefits of KC are and how to safely transfer a baby, so that KC implementation can be
increased. Videos are an effective way to educate patients and nurses, and the video teaching tool created was carefully designed after thorough research and review of feedback from NCCC nurses. The video’s intended use is to provide consistent education of the KC transfer procedure based on the NCCC policy, and serve as a means to educate nurses and parents on KC.
Acknowledgments
The researcher would like to acknowledge and thank her advisor, Rhonda Lanning, for her insight and guidance concerning this project; Julie Calacday, the NCCC Developmental Care Committee leader and NCCC RN, for her assistance with the survey implementation and video filming; Katie Bruce, a UNC undergraduate media productions student, for her guidance and assistance with filming and editing the video; and the NCCC for its support of her research project. This project was also supported by the Tom and Elizabeth Long Excellence Fund for Honors, administered by Honors Carolina, and by the Alpha Alpha Chapter of Sigma Theta Tau International Honor Society Research Grant.
References
Abouelfettoh, A., Ludington-Hoe, S., Burant, C., & Visscher, M. (2011). Effect of skin-to-skin contact on preterm infant skin barrier function and hospital-acquired infection. Journal of Clinical Medicine Research, 3(1), 36-46. doi: 10.4021/jocmr479w
Ahmed, A., & Sands, L. (2010). Effect of pre- and postdischarge interventions on breastfeeding outcomes and weight gain among premature infants. Journal of Obstetric, Gynecologic & Neonatal Nursing, 39(1), 53-63. doi: 10.1111/j.1552-6909.2009.01088.x
Bagby, K., & Bowen, S. (2012). Kangaroo care increases breastfeeding rates. Journal of Obstetric, Gynecologic & Neonatal Nursing, 41(1), 286-290. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?vid=4&sid=b 2af7b50-e155-4735-8f29-12d905dfff8e@sessionmgr4003&hid=4108
Bergman, N., & Bergman , J. (2013). Whose choice? Advocating birthing practices according to baby’s biological needs. The Journal of Perinatal Education, 22(1), 8-13. doi:
10.1891/1058-1243.22.1.8
Bigelow, A., Power, M., MacLellan-Peters, J., Alex, M., & McDonald, C. (2012). Effect of mother/infant skin-to-skin contact on postpartum depressive symptoms and maternal physiological stress. Journal of Obstetric, Gynecologic & Neonatal Nursing, 41(3), 369-382. doi: http://dx.doi.org.libproxy.lib.unc.edu/10.1111/j.1552-6909.2012.01350.x Blencowe, H., Cousens, S., Oestergaard, M., Chou, D., Moller, A., Narwal, R.,… Lawn, J.
(2012). National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. The Lancet, 379(9832), 2162-2172. doi: 10.1016/S0140-6736(12)60820-4
Blomqvist, Y., Rubertsson, C., Kylberg, E., Joreskog, K., & Nyqvist, K. (2012). Kangaroo mother care helps fathers of preterm infants gain confidence in the paternal role. Journal of Advanced Nursing, 68(9), 1988-1996. doi:
http://dx.doi.org.libproxy.lib.unc.edu/10.1111/j.1365-2648.2011.05886.x
Caruana, E. (2008). Early skin-to-skin contact for mothers and their healthy newborn infants. Journal of Advanced Nursing, 62(4), 439-440. doi:
http://dx.doi.org.libproxy.lib.unc.edu/10.1111/j.1365-2648.2008.04669.x
Castral , T., Warnock, F., Ribiero, L., de Vasconcelos, M., Leite, A., & Scochi , C. (2012). Maternal factors regulating preterm infants' responses to pain and stress while in maternal kangaroo care. Latin American Journal of Nursing, 20(3), 435-443. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/22991104
Cooper, L., Gooding , J., Gallagher, J., Sternesky, L., Ledsky, R., & Berns, S. (2007). Impact of a family-centered care initiative on NICU care, staff and families. Journal of
Perinatology, 27(2), 32-37. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?sid=0b324a5 4-de1f-41f4-b6b5-3fbed6084595@sessionmgr4003&vid=11&hid=4108
Cooper, L. (Producer). (2013, Sept 11). Taking the Evidence Based Case for Kangaroo Care into the Clinical Setting [Web Video]. Retrieved from
https://www.youtube.com/watch?v=MBPROCQZd6Y
Fegran, L., Helseth, S., & Fagermoen, M. (2008). A comparison of mothers’ and fathers’ experiences of the attachment process in a neonatal intensive care unit. Journal of Clinical Nursing, 17(6), 810-816. doi: 10.1111/j.1365-2702.2007.02125.x
Flacking, R., Ewald , U., Nyqvist, K., & Starrin, B. (2006). Trustful bonds: A key to "becoming a mother" and to reciprocal breastfeeding. Stories of mothers of very preterm infants at a neonatal unit. Social Science and Medicine, 62(1), 70-80. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/15992983
Flacking, R., Ewald, U., & Wallin, L. (2011). Positive effect of kangaroo mother care on long-term breastfeeding in very prelong-term infants. Journal of Obstetric, Gynecologic & Neonatal Nursing,40(2), 190-197. doi: 10.1111/j.1552-6909.2011.01226.x
Flacking, R., Thomson, G., Ekenberg, L., Lowegren, L., & Wallin , L. (2013). Influence of NICU co-care facilities and skin-to-skin contact on maternal stress in mothers of preterm infants. Sexual & Reproductive HealthCare, 4(3), 107-112. doi:
10.1016/j.srhc.2013.06.002
Funk, D., Tilney, P., Mitchell, S., & Walker, H. (2012). Unplanned kangaroo transport of a preterm infant. Air Medical Journal, 31(6), 264-266. doi:
http://dx.doi.org/10.1016/j.amj.2012.08.006
Haxton, D., Doering, J., Gringras, L., & Kelly, L. (2012). Implementing skin to skin contact at birth using the Iowa model. Nursing for Women’s Health, 16(3), 220-230. doi:
http://dx.doi.org.libproxy.lib.unc.edu/10.1111/j.1751-486X.2012.01733.x
Hill, A., McPhail, S., Hoffmann, T., Hill, K., Oliver, D., Beer, C.,… Haines, T. (2009). A randomized trial comparing digital video disc with written delivery of falls prevention education for older patients in hospital. Journal of the American Geriatrics
Society, 57(8), 1458-1463. doi: http://dx.doi.org.libproxy.lib.unc.edu/10.1111/j.1532-5415.2009.02346.x
Jarvis, M., & Burnett, M. (2009). Developmentally supportive care for twins and higher order multiples in the NICU: A review of existing evidence. Neonatal, Paediatric & Child Health Nursing, 12(3), 2-5. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?vid=13&sid= b2af7b50-e155-4735-8f29-12d905dfff8e@sessionmgr4003&hid=4108
Jefferies, A. (2012). Kangaroo care for the preterm infant and family. Paediatrics and Child Health, 17(3), 141-146. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3287094/
Johnson, K. (2013). Maternal-infant bonding: A review of literature. International Journal of Childbirth Education, 28(3), 17-22. Retrieved from
http://eds.b.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?sid=8a30c32 0-74c9-4c14-8df0-9b9ba1a563f4@sessionmgr112&vid=1&hid=102
Kashaninia, Z., Sajedi, F., Rahgozar, M., & Noghabi, F. (2008). The effect of kangaroo care on behavioral responses to pain of an intramuscular injection in neonates. Journal for Specialists in Pediatric Nursing, 13(4), 275-280. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?sid=54297ce 0-6008-45df-b056-ed37809fef8b@sessionmgr4004&vid=1&hid=4108
Katz, M., Heaner, S., Reiter, P., Putten, J., Murray, L., McDougle, L.,… Paskett, E. (2009). Development of an educational video to improve patient knowledge and communication with their healthcare providers about colorectal cancer screening. American Journal of Health Education, 40(4), 220-228. Retrieved from
Kearvell, H., & Grant, J. (2010). Getting connected: How nurses can support mother/infant attachment in the neonatal intensive care unit. Australian Journal of Advanced Nursing, 27(3), 75-82. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?vid=14&sid= b2af7b50-e155-4735-8f29-12d905dfff8e@sessionmgr4003&hid=4108
Kianne, N., Stuart , E., Thompson , L., Evans , K., & Schneider-Klosky, M. (2008). Evaluation of the addition of video-based education for patients receiving standard
pre-chemotherapy education. European Journal of Cancer Care, 17(4), 329-339. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?sid=68cf7630 -311c-4237-a4cc-b12a3dc7a90e@sessionmgr4001&vid=4&hid=4108
Lau, C., Hurst, N., Smith, E., & Schanler, R. (2007). Ethnic/racial diversity, maternal stress, lactation and very low birthweight infants. Journal of Perinatology, 27(7), 399-408. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?sid=b2af7b50 -e155-4735-8f29-12d905dfff8e@sessionmgr4003&vid=7&hid=4108
Lawn, J., Cousens, S., & Zupan, J. (2005). 4 million neonatal deaths: When? Where? Why?. The Lancet, 365(9462), 891-900. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/15752534
Lawn, J., Mwansa-Kambafwile, J., Horta, B., Barros, F., & Cousens, S. (2010). ‘Kangaroo mother care’ to prevent neonatal deaths due to preterm birth complications. International Journal of Epidemiology, 39(1), 144-154. doi: 10.1093/ije/dyq031
Lima, G., Quintero-Romero, S., & Cattaneo, A. (2000). Feasibility, acceptability and cost of kangaroo mother care in Recife, Brazil. Annals of Tropical Paediatrics: International Child Health, 20(1), 22-26. doi: http://dx.doi.org/10.1080/02724930092020
Lindgren, L., Westling, G., Brulin, C., Lehtipalo, S., Andersson, M., & Nyberg, L. (2012). Pleasant human touch is represented in pregenual anterior cingulate
cortex. NeuroImage, 5915(4), 3427-3432. doi: 10.1016/j.neuroimage.2011.11.013 Lovarini, M., & Bawden, J. (2010). Falls prevention education delivered via digital video disc
results in greater confidence and motivation to engage in falls prevention strategies by hospitalized older people when compared with education delivered in written
format. Australian Occupational Therapy Journal, 57(5), 351-352. doi: http://dx.doi.org.libproxy.lib.unc.edu/10.1111/j.1440-1630.2010.00893.x Ludington-Hoe, S. (2011). Evidence-based review of physiologic effects of kangaroo
care. Current Women's Health Reviews, 7(3), 243-253. doi: http://dx.doi.org/10.2174/157340411796355162
Ludington-Hoe, S., Lewis, T., Morgan, K., Cong , X., Anderson, L., & Reese, S. (2006). Breast-infant temperature with twins during shared kangaroo care. Journal of Obstetric,
Gynecologic & Neonatal Nursing, 35(2), 223-231. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1890034/
Ludington-Hoe, S., & Morgan, K. (2013). Kangaroo care in the NICU, part 1: Understanding the impact of kangaroo care on neonatal vital signs. March of Dimes Foundation, Retrieved from
http://www.marchofdimes.com/nursing/modnemedia/othermedia/articles/art01_kangaroo _care_pt1_text.pdf
Meek, J., & Huertas, A. (2012). Cochrane review: Non-nutritive sucking, kangaroo care and swaddling/facilitated tucking are observed to reduce procedural pain in infants and young children. Evidence-Based Nursing, 15(3), 84-85. doi: 10.1136/ebnurs-2011-100453 Mitchell, M., & Courtney, M. (2005). Improving transfer from the intensive care unit: The development, implementation and evaluation of a brochure based on Knowles’ adult learning theory. International Journal of Nursing Practice, 11(6), 257-268. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?sid=68cf7630 -311c-4237-a4cc-b12a3dc7a90e@sessionmgr4001&vid=9&hid=4108
Morgan, K., & Ludington-Hoe, S. (2013). Kangaroo care in the NICU, part 2: Understanding the impact of kangaroo care beyond neonatal vital signs. March of Dimes Foundation, Retrieved from
http://www.marchofdimes.com/nursing/modnemedia/othermedia/articles/art02_kangaroo _care_pt2_text.pdf
Mori, R., Khanna, R., Pledge, D., & Nakayama, T. (2010). Meta-analysis of physiological effects of skin-to-skin contact for newborns and mothers. Pediatrics International, 52(2), 161-170. doi: 10.1111/j.1442-200X.2009.02909.x
Munson, M., Saatkamp, R., & West, C. (2011). Late preterm infants: Steps to success. Neonatal Network, 30(4), 267-270. doi: 10.1891/0730-0832.30.4.267
Nursing Policy Committee. (2013). Kangaroo care/skin-to-skin care. (NURS 0139). Chapel Hill, NC: UNC Hospitals.
Shah, M., Swanson, P., Nobay, F., Peterson, L., Caprio, T., & Karuza, J. (2012). A novel internet-based geriatric education program for emergency medical services
providers. Journal of the American Geriatrics Society, 60(9), 1749-1754. doi: http://dx.doi.org.libproxy.lib.unc.edu/10.1111/j.1532-5415.2012.04112.x
Tessier, R., Charpak, N., Giron, M., Cristo, M., de Calume, Z., & Ruiz-Pelaez, J. (2009).
Kangaroo mother care, home environment and father involvement in the first year of life: a randomized controlled study. Acta Paediatrica, 98(9), 1444-1450. doi: 10.1111/j.1651-2227.2009.01370.x
Thukral, A., Chawla, D., Agarwal, R., Deorari, A., & Paul, V. (2008). Kangaroo mother care an alternative to conventional care. Indian Journal of Pediatrics, 75(5), 497-503. doi: 10.1007/s12098-008-0077-7
Turnbull, V., & Petty, J. (2013). Evidence-based thermal care of low birthweight neonates. Part one. Nursing Children & Young People, 25(2), 18-22. Retrieved from
http://eds.a.ebscohost.com.libproxy.lib.unc.edu/ehost/pdfviewer/pdfviewer?sid=b2af7b50 -e155-4735-8f29-12d905dfff8e@sessionmgr4003&vid=10&hid=4108
Whitelaw, A., & Sleath, K. (1985). Myth of the marsupial mother: Home care of very low birth weight babies in Bogota, Colombia. The Lancet, 325(8439), 1206-1208. doi:
Appendix A
NCCC Kangaroo Care Survey
This survey begins with Question 2 because Question 1 served as the agreement to participate in the survey.
Q2 Please rank the following statements according to what you perceive to be important or not important for parents when learning about Kangaroo Care.
Not at all Important (1) Somewhat Unimportant (2) Neither Important nor Unimportant (3) Somewhat Important (4) Extremely Important (5) Understanding what Kangaroo Care is (1) m m m m m Understanding the benefits of Kangaroo Care (2) m m m m m Understanding the risks of Kangaroo Care (3) m m m m m Understanding how to transfer the baby for Kangaroo Care (4) m m m m m Understanding when Kangaroo Care can be done (5) m m m m m Understanding which babies are not allowed
to participate in Kangaroo
Care (6)
m m m m m
Q3 What else, if anything, do you perceive to be important for parents to understand or learn regarding Kangaroo Care? Please feel free to elaborate.
Q4 Please rank the following statements according to what you perceive to be a common or uncommon barrier for parents concerning Kangaroo Care.
Not at all common (1) Somewhat uncommon (2) Neither common nor uncommon (3) Somewhat common (4) Very common (5) Lack of knowledge about the benefits of Kangaroo Care (1) m m m m m Feeling uncomfortable in the chair while providing Kangaroo Care (2) m m m m m Feeling worried about the transfer of the baby during Kangaroo Care (3) m m m m m Feeling uncomfortable to ask nurses to begin Kangaroo Care (4) m m m m m Feeling that Kangaroo Care is unsafe for the baby (5) m m m m m Lack of knowledge about how to transfer the baby from bed
to parent during Kangaroo Care
(6)
Q5 What else, if anything, do you think gets in the way of parents implementing Kangaroo Care? Please feel free to elaborate.
Q6 In the past 2 weeks, approximately how many shifts did you work in UNC's NCCC? (Please use numbers)
Q7 In the past 2 weeks, approximately how many of your patients participated in Kangaroo Care? (Please use numbers)
Q8 In the past 2 weeks, approximately how many of your patients were not allowed to participate in Kangaroo Care based on the NCCC's policy? (Please use numbers)
Q9 In the past 2 weeks, approximately how many times did you educate parents about what Kangaroo Care is? (Please use numbers)
Q10 In the past 2 weeks, approximately how many times did you assist another nurse with his/her patient's Kangaroo Care transfer? (Please use numbers)
Q11 How confident do you feel in your ability to do each of the following items below?
Not at all
confident (1)
Only a little or slightly confident (2) Moderately confident (3) Very confident (4) Educating parents about what Kangaroo Care is (1) m m m m Discussing the benefits of Kangaroo Care (2) m m m m Teaching parents how to transfer the baby for Kangaroo
Care (3)
m m m m
Transferring the baby for Kangaroo
Care (4)
m m m m
Asking another nurse for help with
the transfer of baby for Kangaroo
Care (5)
Q12 Please read each statement to the left and answer as honestly as possible.
Strongly
Disagree (1) Disagree (2) Somewhat Neither Agree nor Disagree (3)
Somewhat
Agree (4) Agree (5) Strongly My patients feel supported by me to implement Kangaroo Care (1) m m m m m Most other patients feel supported by their nurses in the unit to implement Kangaroo Care (2) m m m m m I provide Kangaroo Care safely (3) m m m m m In general, other nurses on the unit provide Kangaroo Care safely (4) m m m m m Our unit provides Kangaroo Care an equal amount or more, compared to other hospitals (5) m m m m m
Q13 How satisfied are you with the Kangaroo Care training you have received while working in the NCCC?
m Very Dissatisfied (1) m Somewhat Dissatisfied (2)
m Neither Satisfied nor Dissatisfied (3) m Somewhat Satisfied (4)
Q14 How do you feel about the transfer of the baby from bed to parent or parent to bed for Kangaroo Care? What concerns, if any, do you have about it? Please feel free to elaborate. Q15 How do you think other nurses on your unit feel about transferring a baby for Kangaroo Care? Please feel free to elaborate.
Q16 How helpful would the following be for you to learn or review how to properly transfer a baby for Kangaroo Care?
Not at all helpful
(1) nor unhelpful (2) Neither helpful Somewhat helpful (3) Very helpful (4)
Pamphlet (1) m m m m In-service teaching for nurses (2) m m m m Poster (3) m m m m Video showing a proper transfer (4) m m m m Powerpoint with pictures and bulleted information (5) m m m m
Q17 What else, if anything, would be helpful for you to learn or review how to properly transfer a baby for Kangaroo Care? Please feel free to elaborate.
Q18 In your opinion, how helpful do you think the following would be for parents to learn or review how to properly transfer a baby for Kangaroo Care?
Not at all helpful
(1) nor unhelpful (2) Neither helpful Somewhat helpful (3) Very helpful (4)
Pamphlet (1) m m m m In-service teaching for parents (2) m m m m Poster (3) m m m m Video showing a proper transfer (4) m m m m Powerpoint with pictures and bulleted information (5) m m m m
Q19 What else, if anything, do you think would be helpful for parents to learn or review how to properly transfer a baby for Kangaroo Care? Please feel free to elaborate.
Appendix B
DVD Copies of the Kangaroo Care Video Teaching Tool will be supplied to the NCCC Links to the videos on YouTube:
Please copy and paste the links into a new webpage, or search for the title of each video on YouTube. User account is Melissa Robinson.
Kangaroo Care: An Educational Resource for Parents and Nurses https://www.youtube.com/watch?v=3MM55eEgDJ0
Kangaroo Care: Sitting Transfer
https://www.youtube.com/watch?v=r59unmwtOJI Kangaroo Care: Standing Transfer