EFFECT OF EXERCISE INTENSITY ON APPEITITE REGULATION: INFLUENCE OF SEX
AND BODY COMPOSITION
Shawn Ahuja
A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the Senior Honors Research in the Department of Exercise and Sport Science.
Chapel Hill 2019
Approved by:
© 2019
Shawn Ahuja
CHAPTER I
INTRODUCTION
The prevalence of obesity is widely known, with more than two-thirds of adults considered overweight or obese in the United States.1,2 Excess body fat is associated with a number of comorbidities including
cardiovascular disease, hypertension, type 2 diabetes mellitus, and even cancer.3 With so many
Americans at an increased, yet malleable risk for these diseases, it comes as no surprise that the cost of obesity in the United States was estimated to be $147 billion in 2008.4 The solution is to lose excess fat
mass through a sustained caloric deficit. This is potentially achieved through a reduced caloric intake via changes in dietary lifestyle and an increased caloric expenditure by exercise. However, given the
prevalence of obesity, it is clear that this approach is not easily adopted. With regards to exercise, the Centers for Disease Control has identified a lack of time and energy as the most common barriers to physical activity.5
High intensity interval training (HIIT) is gaining evidence as a powerful time-efficient and effective approach to exercise. This approach is potentially more effective than traditional sprint interval training (SIT), characterized by repeated maximal sprinting (10-30 sec), which is not as feasible and requires more time due to the recovery time between bouts. In contrast, HIIT is characterized by a series of short exercise bouts (1-3 min) completed at a very high intensity, followed by a short rest period, requiring only 10 minutes of work. This approach to exercise is feasible in a variety of populations and has also been reported to improve cardiovascular fitness and insulin sensitivity,6–8 in as few as three
weeks.6, 8 Additionally, HIIT has been shown to have higher ratings of perceived enjoyment for
load and shorter rest periods for a full body workout, requiring a total of 20 minutes. This approach to strength training is more advantageous for metabolism compared to other common techniques and is more time efficient.7
While HIIT has shown its capacity for improving cardiovascular fitness among individuals with various chronic diseases, what remains to be seen is its impact on appetite- both on an individual’s perceived desire to eat as well as their hunger hormone profile. A recent pilot study reported a transient suppression in appetite in overweight individuals following SIT, and no change in relative energy intake compared to individuals who merely rested.10 This suggests that HIIT may not cause compensatory caloric
consumption, which would negate the intended effects of exercise for overweight individuals. However, by nature of a pilot study, the sample size investigated was relatively small (n = 8.) This study also compared a less feasible exercise protocol to rest, opposed to discerning the effects of higher intensity exercise compared to traditional training. Specifically, SIT lacks feasibility for certain populations because it consists of “all out” maximal effort 30 second sprints. Studies that have compared the effect of HIIT to other modalities on appetite suppression have conflicting results; some studies show no change in appetite between modalities while others demonstrate a greater appetite suppression effect in HIIT. 11,14-16,18,20,31 To evaluate the true effect of HIIT on appetite regulation, we must evaluate HIIT in comparison to
other modes of exercise, with respect to appetite, is warranted. Furthermore, the influence of sex, or level of obesity have not been explored and warrant further investigation. Prior research suggests an increase in appetite supression in men following exercise11 and lesser hunger in individuals with greater fat mass.12
Purpose:
a. Appetite was measured from a visual analogue scale rating, the Leeds Food Preference Questionnaire, and from measures of acetylated ghrelin in plasma.
2. The secondary purpose of this study was to explore the effect of sex and level of body fat on appetite response from an acute bout of HIIT or HIRT in comparison to MICT
Research Questions:
1. Is there a difference in appetite perception between the three training modalities (HIIT, HIRT, and MICT)?
2. Is there a difference in levels of acetylated ghrelin following each of the training modalities? 3. Is there a difference in appetite between males and females following each of these training
modalities?
4. Is there a difference in appetite between individuals with varying adiposity following each of these training modalities?
Research Hypotheses:
1. Perceptions of appetite will be lower following HIIT and HIRT when compared to MICT. 2. Plasma acetylated ghrelin will be lower following HIIT and HIRT when compared to MICT.
Delimitations:
1. Participants were recreationally active (participating in physical activity 1-5 hours a week), ages 18-40 years old.
2. The study consisted of 5 visits.
3. The duration of the exercise intervention was three weeks.
4. Body composition was analyzed by dual-energy X-ray absorptiometry (DEXA).
6. Participants were excluded if they used or planned to use a supplement or prescription drug that may influence metabolic rate or appetite.
7. Participants were excluded if the health history questionnaire indicates a recent history of musculoskeletal injury, musculoskeletal disorder, metabolic disorder, or eating disorder. 8. Participants were excluded if they have lost or gained ≥ 5 kg within the last two months.
Limitations:
1. Subjects were recruited at the University of North Carolina at Chapel Hill and gyms in the surrounding areas, therefore, recruitment of participants were not be truly random.
2. Individual diets (including macronutrient distribution) and outside exercise were not controlled for.
Assumptions:
Theoretical
1. Subjects provided accurate answers to screening questions. 2. Subjects adhered to pre-visit guidelines, including fasting.
3. The one repetition maximum results were the subjects’ true max values.
4. The multiple repetition maximum tests were accurate predictions of true max values.
5. Subjects kept their dietary and training habits consistent throughout the duration of the study. 6. Subjects gave their full effort at each training visit, and effort did not differ between groups.
Statistical
1. The sample of participants that used in the study were from a population that was normally distributed.
2. The order in which the exercise modalities were completed was randomly assigned. 3. The variability in the study sample was approximately equal (homogeneity of variance
Definition of Terms:
Moderate intensity continuous training- a type of physical activity that is characterized by an absence of rest periods, with participants training at 45-55% HRR for a period of 30 minutes.
High intensity interval training- a type of physical activity that is characterized by a short bout of exercise at 90-95% HRR, followed by a short rest period, repeated 7-10 times.
High intensity resistance training- a type of resistance training that is characterized by short rest periods, with participants using a ~80% load for a moderate volume (6-8 repetitions).
One repetition maximum- the maximum amount of weight that can be lifted for one repetition, while maintaining proper form.
Repetitions to fatigue- the maximum amount of repetitions that can be completed using a given amount of weight before an individual can no longer complete a full repetition.
Resistance trained- participating in resistance training at least 3 times per week for 6 months.
Resting energy expenditure- a measurement taken to approximate the amount of kilocalories the body would use at rest during a full twenty-four hour period.
Substrate utilization- the substrate (usually carbohydrate or fat) being used by the body to produce energy; analyzed by measuring respiratory exchange ratio, which is the amount of CO2
produced divided by the amount of O2 utilized.13
Significance of Study:
CHAPTER II
LITERATURE REVIEW
Introduction
High intensity interval training (HIIT) is a time effective approach to exercise that is tolerated well in overweight and obese populations, and has reportedly improved cardiovascular fitness and insulin sensitivity in these populations.6–8 With respect to appetite, initial evidence suggests HIIT may be related
to reduce appetite compared to moderate intensity continuous training (MICT) in terms of appetite regulatory hormones and subjective reporting. However, other studies suggest that there is no difference in appetite regulation between the two modalities. Furthermore, when investigating appetite regulation, there are no current studies that simultaneously compare MICT, HIIT, and high intensity resistance training (HIRT), an exercise modality that shares the time efficiency of HIIT but confers the benefits of resistance training. Prior research has indicated that there is a difference in appetite regulation between men and women following a bout of MICT.11 With potential differences in appetite regulation between
MICT, HIIT, and HIRT, there is a further need to explore sex-based differences between each modality. Thus, the purpose of this literature review is to synthesize available evidence on HIIT and appetite regulation, explore the effect of resistance training on appetite as a predictor for HIRT’s effect, and note any sex-based differences regarding appetite regulation following exercise.
HIIT and Appetite:
A recent pilot study by Matos et al.14 that assessed subjective hunger, satiety, fullness, and prospective
food consumption in overweight and obese males participating in acute bouts of HIIT and MICT found that there was no change between the two modalities overtime in hunger, satiety, and prospective food consumption post exercise, but a transient increase in fullness immediately after HIIT.14 However, this
supported by a chronic study conducted by Martins et al.15 investigating determining the effects of HIIT
on subjective appetite, appetite-related hormones and reward value of food in sedentary obese individuals. Training modality did not show an effect on appetite when accounting for equal caloric expenditure. This group had found similar appetite responses between acute bouts of iso-caloric HIIT and MICT in a preliminary study with a smaller sample size. (n=12)16 When focusing on hunger hormones as a marker of
appetite, Metcalfe et al.17 reported no change in appetite following an acute bout of reduced exertion high
intensity interval training amongst sedentary individuals.
However, when expanding on the definition of HIIT, the literature shows almost conflicting results. When utilizing high intensity intermittent exercise (HIIE), which is characterized by a higher intensity but shorter work period when compared to HIIT, Sim et al.18 demonstrated a significant decrease in energy
intake compared to MICT amongst overweight inactive men. Specifically, when HIIE participants consumed a higher caloric standardized meal prior to pre and post intervention testing sessions, they consumed fewer calories after a 70-minute waiting period compared to when they consumed a lower caloric standardized meal. However, this effect was not seen with the MICT or control groups. Additionally, a prior study done by Sim et al.19 reported that acute bouts of HIIE were associated with
lowered ad libitum energy intake compared to MICT or no exercise. This finding was also associated with lowered activated-ghrelin levels, signifying a potential reduction in appetite despite no change in
subjective perception of appetite.19 Furthermore, a pilot study involving overweight, low-moderate
activity level individuals by Holiday et al.10 found that sprint interval training, a modality similar to HIIT
but different in that it involves “all-out effort”, showed a suppression of acylated ghrelin which was matched with a reduction in subjective appetite immediately after exercise, when compared to no exercise. Interestingly, there was no change in ad libitum caloric intake between the rest and exercise conditions, suggesting that the exercise did not result in a compensatory caloric intake. A similar study by Beaulieu et al.20 found a similar trend for SIE, but amongst physically active men and an increased level
As it stands, there appears to be uncertainty as to whether there is a difference in appetite when comparing HIIT to MICT, illustrating a need for more research on this topic.
HIRT and Appetite:
Previous data has demonstrated a decrease in both leptin and active ghrelin following resistance training twice a day for two successive days.21 While some studies suggest an association between
lowered leptin concentration and increased training volume in endurance athletes22,23, Goto et al.21
postulate that the decrease in ghrelin may be a specific response to resistance training. However, considering how ghrelin and leptin work in opposite ways to regulate appetite, and that there was no subjective measure of appetite, it is uncertain what effect acute resistance training has. When comparing resistance training to aerobic training, a study by Broom et al.24 found a similar suppression in subjective
appetite and acetylated ghrelin between acute bouts of resistance training and aerobic exercise. However, the gut peptide hormone peptide YY (PYY) was increased only in the bout of aerobic exercise, potentially suggesting greater satiety following aerobic activity.24,25 In a more practical manner, a study comparing a
bout of aerobic exercise, resistance exercise, and no exercise done found that there was no significant difference in energy intake or macronutrient preference in the post exercise meal provided to subjects despite reduced active ghrelin in the resistance training trials.26 A similar study including twelve weeks
of training found that aerobic exercise increased satiety when compared to resistance training with no significant difference between active ghrelin or PYY levels in either fasting or postprandial states.27
Extrapolating this information to HIRT, it could be hypothesized that either HIIT or MICT would confer greater appetite regulation. A study by Pessôa dos Prazeres et al.28 found that between traditional
resistance training and circuit training, a type of exercise that is similar to HIRT. However, a formal comparison between HIRT, HIIT and MICT remains to be seen.
Potential sex-based differences:
active women29 found that those who did the running exercise found both an increase in anorexigenic
peptides as well as lower relative energy intake (net energy balance when accounting for caloric expenditure and the ad libitum meal). Another study that compared the difference in hunger, energy intake, and appetite regulation between a bout of walking and rest in overweight/obese women found that those who completed the walking bout had a lower relative energy intake compared to those who
participated in rest, suggesting no acute caloric compensation following exercise.30 This suggests that
there is an anorexigenic effect following exercise that is similar to the one observed in men. When comparing the extent of this effect between the two sexes, Hagobian et al.11 found that women would start
a bout of MICT with higher levels of acetylated ghrelin and lower levels of insulin when compared to men, suggesting a stimulation of energy intake. When adding dietary energy to restore energy balance following exercise, it was found that men had a reduction in appetite while there was no effect found in women. While the authors of this study suggest that this sex difference may arise from women innately reserving body fat for reproductive success. The reproducibility of this difference in HIIT and HIRT remains to be seen. Understanding to what extent this sex difference occurs across different training modalities may help better guide exercise recommendations to women seeking to lose weight. Conclusion:
Currently, there are some studies that show there is no difference in appetite regulation between HIIT and MICT,14–16 but there are other results that suggest that HIIT derivatives may have a stronger anorexigenic
effect compared to MICT or rest.10,18,20,31 Preliminary data suggests that aerobic activity may result in
more satiety than resistance training,24,26,27 which may imply that HIIT and MICT may confer in greater
appetite regulation when compared to HIRT. However, no formal comparison has been made. Similarly, while prior research has shown greater appetite regulation in men compared to women following MICT,11
CHAPTER III
METHODOLOGY
Participants
18 subjects (9 men, 9 women) were recruited, 1 was lost due to follow-up, 1 dropped out due to an injury unrelated to the study, 1 was unable to complete the HIIT intervention, and 1 did not complete their final training. Thus, a total of 14 subjects (7 men, 7 women; mean ± SD; age= 22.8 ± 4.5 yrs; Height=172.9 ± 8.7 cm; Weight= 75.0 ± 14.6 kg; %BF: 24.6 ± 6.6%) participated in all three visits of the study and were included in the analyses.
Participants were recreationally active, participating in 1-5 hours per week of exercise.
Participants were excluded if they have a history of musculoskeletal disease, recent injury, chronic illness, underweight (BMI < 18.5 kg/m2) or severely obese. (BMI > 40 kg/m2) Additionally, if an individual
consistently consumed any supplement or prescription drug that may influence metabolic rate or appetite they were excluded. Supplementation and medical history were evaluated via a health history
questionnaire. Subjective appetite was assessed by a computerized visual analog scale (VAS) and desire to eat was assessed by a liking and wanting questionnaire. Sleep quality was be assessed by a
questionnaire.
Experimental Design:
questionnaire to confirm eligibility. If applicable, participants took a pregnancy test and upon a negative result, underwent body composition evaluation. Participants then had their body composition assessed by dual-energy X-ray absorptiometry (DEXA). Following body composition assessment, participants had their resting energy expenditure assessed by indirect calorimetry, and completed one repetition maximum (1RM) tests for both the leg press and bench press, and six rep max (6RM) tests for various accessory muscles, and were familiarized with each exercise protocol. Participants were randomized, using Random Allocation Software (Isfahan, Iran) into one of the 3 exercise bouts. Each training session had a minimum one-week washout period prior to the initiation of the next protocol. Prior to the start of training a fasted blood draw was taken to determine levels of ghrelin; participants rated their subjective appetite with a VAS, and completed a series of questionnaires to characterize food preference. Immediately following training, 30 minutes post training, and 60 minutes post training, participants again rated their subjective appetite and underwent a second blood draw at 30 minutes post training.
Preliminary Testing:
Body Composition
Participants were at least four hours fasted, and refrained from vigorous exercise for at least 24 hours prior to all baseline and exercise interventions. Due to use of the DEXA, which utilizes a very low dose of radiation, all female participants underwent a urine pregnancy test.
were completed by the same research technician for all scans. Body composition was measured as fat mass (FM), lean mass (LM), and percent body fat (%BF).
Maximal Strength Testing
Maximal strength was tested using one repetition maximums (1RM) for the bench press and leg press, and six repetition maximums (6RM) for accessory muscles. For the 1RM tests, participants did five minutes of walking on a treadmill to warm-up, followed by dynamic stretching. They were familiarized with the equipment to be used, as well as the proper technique for each lift. Participants then completed two warm-up sets at 50% (8-10 repetitions) and 80% of their 1RM (4-6 repetitions) with approximately two minutes of rest in between. After two minutes of rest, they completed one rep at an estimated 1RM value. They then completed up to three more attempts with increasing weight and two minutes of rest between attempts until they reached a point of failure.
Multiple RM tests, specifically a 6RM, were used to predict participants’ 1RM on four different accessory exercises. These exercises included an overhead shoulder press, a biceps curl, an overhead triceps extension, and an alternating stationary lunge, all using dumbbells. The research staff determined what weight participants should begin with for each exercise, based on the prior training of the individual, aiming for 3-10 successful repetitions. Participants were allowed approximately two minutes of rest between each accessory exercise. The amount of weight used (rep weight) and the number of repetitions completed until fatigue (RTF) was put in the following equation to predict participants’ 1RM32 :
Equation 1: 1RM= rep weight 0.522+0.419e−0.055∗RTF
The projected 1RM value that was calculated from this equation was then used to estimate 80% to 85% of maximum load for the HIRT bouts.
Participants had their resting heart rate (RHR) measured using a polar heart rate monitor, (Polar FT1, Polar USA, Port Washington, NY, USA), and had their age-predicted maximal heart rate (MHR) determined. Exercise target heart rates (THR) for were calculated using the Karvonen equation. [THR = ((MHR – RHR) % intensity) + MHR]33 Exercises was matched for caloric expenditure.
Resting Energy Expenditure and Respiratory Exchange Ratio
During visit 1, Resting Energy Expenditure (REE) and Respiratory Exchange Ratio (RER) data was collected. REE was collected for twenty-five minutes with the first five minutes of measurement discarded and the remaining time averaged. Participants laid down, wearing a gas mask that was connected by a tube to a metabolic cart. The metabolic cart and software (TrueOne 2400 Metabolic Measurement System, ParvoMedics, Inc., Sandy, UT, USA) measured oxygen uptake (VO2) and the
amount of carbon dioxide exhaled (VCO2) to indirectly measure REE. A Polar heart rate monitor (Polar
FT1, Polar USA, Port Washington, NY, USA) was worn during all metabolic testing. Oxygen uptake and VCO2 was measured in liters per minute (L/min). REE, expressed in kilocalories per day (kcal/day), was
be calculated using Equation 2 34 below :
Equation 2: REE=
[
(
3.9∗(
V O2)
)
+(
1.1∗(
VCO2)
)
]
∗1440minutesQuestionnaires
At each training session, participants rated their subjective appetite in terms of subjective hunger, desire to eat, and fullness using a computerized and validated version of Visual Analogue Scale (VAS)35,
immediately before, after their training, 30 min after their training, and 60 minutes after their training. Participants also measured liking and wanting of food alongside subjective appetite using a computer-based procedure called the Leeds Food Preference Questionnaire (LFPQ).36 The LFPQ provided
sensory properties of food. Participants were presented with an array of pictures of individual food items common in the diet. A database with food items either predominantly high (>50% energy) or low (<20% energy) in fat but similar familiarity, protein content, sweet or non-sweet taste and palatability were used. Thus, food choices were either high fat savory (HFSA), low fat savory (LFSA), high fat sweet (HFSW), or low fat sweet (LFSW).
Photo 1. LFPQ Food Array
Participants were also instructed to record their food intake prior to the exercise session with a 24 hour food log to control for diet.
Blood Draw
Fasted blood samples were taken prior to the start of exercise and at 30 min post exercise. Venous blood was collected into EDTA-coated tubes containing 500 KIU aprotinin (Pentapharm, Basel,
Germany) (10 mg/ml of isopropanol) were added to each milliliter of plasma immediately after centrifugation.
Exercise Intervention:
Moderate Intensity Continuous Training (MICT)
Participants reported to the lab a minimum of 4 hours fasted prior to each training session. The bout of MICT consisted of a self-selected 5-min warm-up, followed by a 20-30-min treadmill jog at 45-55% HRR. The research staff were present to record RPE and HR at the end of each minute.
High Intensity Interval Training (HIIT)
The bout of HIIT consisted of a self-selected 5-min warm-up, followed by ten rounds of a 60-s treadmill (Q65 Series 90, Quinton Instrument Co., Seattle, WA, USA) run at 85% to 95% HRR with a 60-s passive rest period, adapted from Wingfield, Smith-Ryan et al.7 The entire exercise bout was a duration of
approximately 20 min. The research staff recorded the RPE and HR at the end of each interval and ensured the participants could adhere to the bout.
High Intensity Resistance Training (HIRT)
Participants completed a 30 minute HIRT session, adapted from Paoli et al.37 Participants reported to the
lab a minimum of 4 hours fasted prior to each training session. Free weights were used to perform six different exercises. The exercises were completed in the order of: leg press and bench press (York Barbell Co., York, PA, USA), dumbbell (DB) lunges, DB shoulder press, DB biceps curls, and DB triceps extensions. Before beginning the training session, participants were allowed to warm-up as they desired for up to 10 minutes.37 Three sets were done for each exercise at a 6RM to 8RM, with 20 to 30 seconds
of rest between sets.7 The research staff spotted participants when necessary and made sure that proper
Polar heart rate monitor) and rate of perceived exertion38 were recorded after completion of each set.
HIRT bouts took approximately 30 minutes to complete.
Statistical Analyses
CHAPTER IV
RESULTS
Perceptions of Appetite
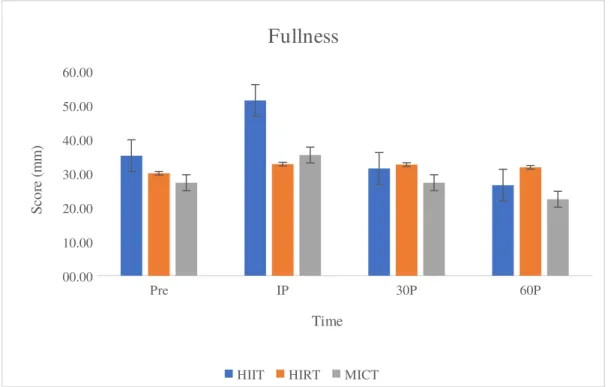
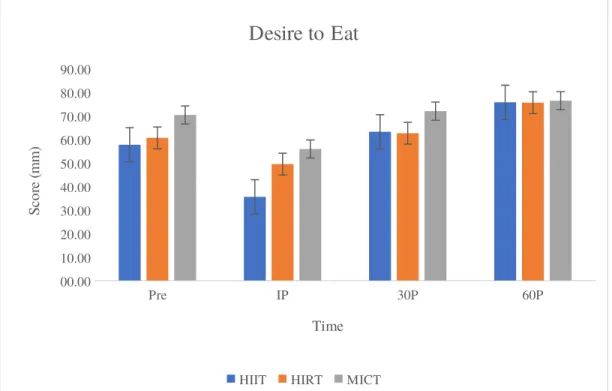
There were no significant differences in hunger, fullness, and desire to eat between interventions before, 30 minutes post exercise, and 60 minutes post exercise. There were significant differences immediately post exercise for all three outcomes. (Hunger; p=0.024, Fullness; p<0.001; Desire to eat; p=0.017). Post hoc comparisons revealed significantly lower hunger immediately post HIIT compared to
MICT(p=0.017) (Figure 1), significantly higher fullness immediately post HIIT compared to
HIRT(p=0.019) and MICT (p=0.001) (Figure 2), and significantly lower desire to eat immediately post HIIT compared to MICT(p=0.027) (Figure 3). No other group differences were found. Fullness
immediately post HIIT had a statistically significant moderate correlation with fat mass. (r=0.596; p=0.024)
Pre IP 30P 60P
0 10 20 30 40 50 60 70 80
Hunger
HIIT HIRT MICT
Time
Sc
or
e
(m
m
Figure 1. Average VAS scores for “How hungry do you feel?” by intervention and time point. * denotes
significant difference between groups (p<0.05). All figures reported as Mean SEM
Pre IP 30P 60P
00.00 10.00 20.00 30.00 40.00 50.00 60.00
Fullness
HIIT HIRT MICT
Time
Sc
or
e
(m
m
)
Pre IP 30P 60P 00.00
10.00 20.00 30.00 40.00 50.00 60.00 70.00 80.00 90.00
Desire to Eat
HIIT HIRT MICT
Time
Sc
or
e
(m
m
)
Figure 3. Average VAS scores for “How strong is your desire to eat?” by intervention and time point. *denotes significant difference between groups (p<0.05).
Food Preference
There were no significant differences in choice frequency of high fat savory foods (HFSA), low fat savory foods (LFSA), or high fat sugary foods (HFSW) between interventions at any time point. There were no significant differences in choice frequency of low-fat sugary foods (LFSW) between
p=0.023 and r=0.552; p=0.041 respectively) Additionally, choice frequency of LFSA immediately following MICT had a moderate negative correlation with LM (r=-0.544; p=0.044).
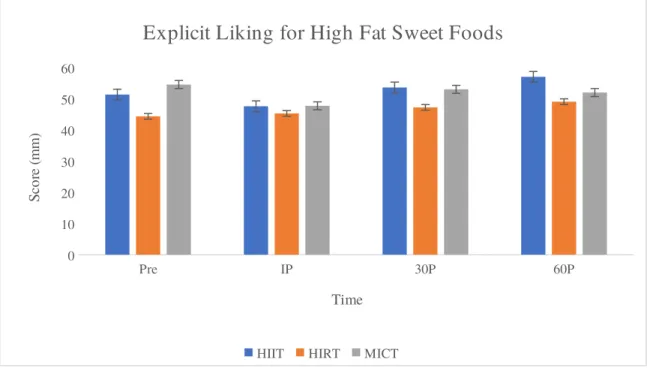
There were no significant differences in explicit liking for HFSA, LFSA, and LFSW between
interventions at each time point. There was a significant difference in explicit liking for HFSW between groups prior to exercise(p=0.039). Specifically, explicit liking for HFSW was significantly lower in HIRT compared to MICT (p=0.041), but no other group differences were found. There was also a group difference 60 minutes after exercise (p=0.005) with explicit liking for HFSW significantly greater in HIIT (57.0 mm ± 25.8) compared to HIRT at this time point (49.0 ± 26.1 mm; p=0.005) (Figure 5). No other differences were found between interventions at this time point for HFSW. There were no statistically significant correlations between demographical information and explicit liking immediately after exercise for any of the interventions.
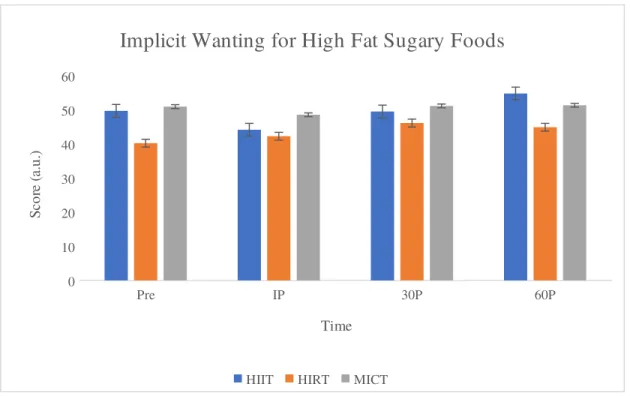
There were no significant differences in implicit wanting for LFSA between interventions at any time point. There was a significant difference in implicit wanting for HFSA between groups 30 minutes after exercise (p=0.009). Specifically, implicit wanting for HFSA was greater in MICT (58.1 ± 15.1 a.u.) compared to HIIT (51.9 ± 16.4 a.u.; p=0.010) and HIRT (51.3 ± 18.5 a.u.; p=0.039) (Figure 6). There was no difference between HIIT and HIRT at this time point, and no other group differences at any other time point. There was a significant difference in implicit wanting for HFSW prior to exercise(p=0.003). Specifically, implicit wanting for HFSW was lower in HIRT compared to HIIT(p=0.027) and
groups 30 minutes after exercise (p=0.05) with implicit wanting for LFSW in HIRT (66.0 ± 12.9 a.u.) significantly lower than MICT (74.6 ± 12.3 a.u.; p=0.002) (Figure 7). No difference was found between HIIT (69.6 ± 13.0 a.u.) and HIRT or HIIT and MICT. There were no statistically significant correlations between demographical information and implicit wanting immediately after exercise for any of the interventions.
Ghrelin
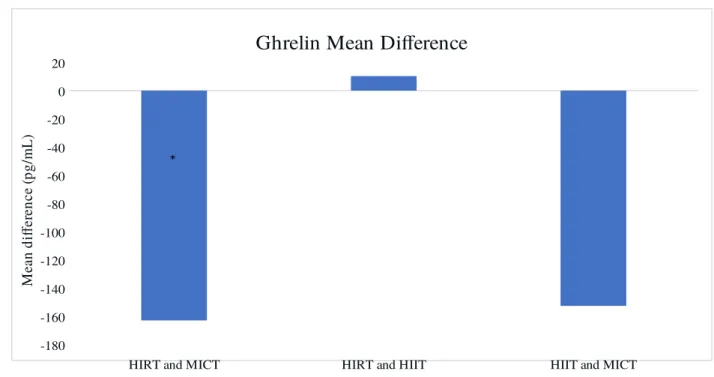
There was a significant difference between exercise modality for the change in ghrelin concentration from pre- to post-exercise (p=0.027). Post hoc analyses indicated a significantly greater decrease in ghrelin for HIRT compared to MICT [mean difference (MD) : -162.9 ± 149.2 pg/mL; p=0.004], and no difference between HIIT and HIRT (MD: 10.3 ± 278.2 pg/mL; p=1.000) or HIIT and MICT (MD: -152.6 ± 261.6 pg/mL; p=0.144) (Figure 9).
Pre IP 30P 60P
0 5 10 15 20 25 30 35 40
Choice Frequency of Low Fat Sugary Foods
HIIT HIRT MICT
Figure 4. Average choice frequency of LFSW by intervention and time point. * denotes significant difference between HIIT vs. HIRT p<0.05
Pre IP 30P 60P
0 10 20 30 40 50 60
Explicit Liking for High Fat Sweet Foods
HIIT HIRT MICT
Time Sc or e (m m )
Figure 5. Average explicit liking score for HFSW by intervention and time point. * denotes significantly lower value between groups; # denotes significantly higher value compared to HIRT p<0.05.
Pre IP 30P 60P
0 10 20 30 40 50 60 70
Implicit Wanting for High Fat Savory Foods
HIIT HIRT MICT
Figure 6. Average implicit wanting score for HFSA by intervention and time point. * denotes significantly higher value than HIIT and HIRT p<0.05.
Pre IP 30P 60P
0 10 20 30 40 50 60
Implicit Wanting for High Fat Sugary Foods
HIIT HIRT MICT
Time
Sc
or
e
(a
.u
.)
Pre IP 30P 60P 0 10 20 30 40 50 60 70 80
Implicit Wanting for Low Fat Sugary Foods
HIIT HIRT MICT
Time Sc or e (a .u .)
Figure 8. Average implicit wanting score for LFSW by intervention and time point. * denotes significantly lower value compared to all groups; p<0.05.
HIRT and MICT HIRT and HIIT HIIT and MICT -180 -160 -140 -120 -100 -80 -60 -40 -20 0
20
Ghrelin Mean Difference
M ea n di ffe re nc e (p g/ m L)
Figure 9. Ghrelin mean differences SD between exercise modalities following exercise. * denotes significant difference compared to others comparison; p<0.05.
Appetite
There were no differences between men and women.
Food Preference
There were no differences between men and women for choice frequency. Men had a strong correlation between choice frequency for HFSA and LM immediately following HIRT (r=-0.8; p=0.031) and between choice frequency for LFSW and LM immediately following MICT. (r=0.772; p=0.042). No correlations were found for women with regard to choice frequency.
Men reported significantly higher (66.7 ± 16.4) explicit liking for HFSW 60 minutes post exercise compared to women (31.1 ± 16.4; p=0.001). There were strong correlations in men between RMR and explicit liking for LFSA immediately following HIIT (r=-0.959; p<0.01). Additionally, men had strong correlations between RMR and explicit liking for HFSA (r=-0.969; p<0.01), for LFSA (r=-0.926; p=0.003), and for HFSW (r=-0.911; p=0.004) immediately following MICT. Women demonstrated no significant correlations after exercise.
CHAPTER V
DISCUSSION
compared to MICT 60 minutes after exercise. Implicit wanting for HFSA was higher in MICT compared to both HIIT and HIRT 30 minutes after exercise, suggesting a stronger preference for these foods. RMR and LM were significantly related to choice frequency of HFSW immediately after HIIT and MICT, while choice frequency for LFSA had a negative correlation with LM immediately after a bout of MICT. It is possible that individuals with higher RMR and LM may have a greater preference for high fat sugary foods following HIIT and MICT, and individuals with higher LM will have a lower preference for LFSA foods following a bout of MICT. Inconsistent with the subjective appetite measures, ghrelin was
significantly lower in HIRT following exercise compared to MICT.
High intensity interval training has previously been shown to significantly lower hunger, increase fullness, and reduce the desire to eat in obese men, when compared to MICT.14 Our results were similar
in a normal weight sample of males and females, supporting the idea that HIIT may suppress appetite after exercise more than MICT. In contrast, a previous study demonstrated that there was no significant difference in subjective appetite between HIIT and MICT in overweight and obese men.16 In addition to
previous literature demonstrating a significant effect of HIIT on appetite14,18,31, the current results also
suggest HIRT may also have a positive effect on appetite control. The present study failed to show a significant difference for ghrelin concentrations between HIIT and MICT, which is not consistent with previous literature that demonstrated a significant reduction in ghrelin immediately following intense HIIT compared to MICT.19 To date, we are aware of no study that simultaneously compares HIIT, HIRT,
and MICT with respect to appetite and food preference. The present findings demonstrated significantly lower ghrelin concentrations following HIRT when compared to MICT, and HIIT compared to HIRT, although not significant. The difference between HIRT and MICT is consistent with a prior acute training study that found a significant reduction in ghrelin immediately after a 45-minute bout of resistance training compared to a 45-minute bout of aerobic exercise and a resting control.26
subjective sensation of fullness is higher in HIIT compared to both MICT and HIRT after exercise suggests that rather than decreasing desire to eat or hunger after exercise, HIIT may simply cause individuals to lose their appetite. This is consistent with the fact that there were no differences between groups as time went on, although this could be a result of participants getting hungrier over time having undergone a four hour fast. The mechanisms for this immediate appetite suppression are unclear, but it may be related to the relatively higher intensity of the exercise when compared to MICT. Specifically, HIIT caused a greater rate of perceived exertion and HR throughout the training compared to MICT. Prior studies have shown greater increases in lactate following HIIT compared to MICT19,39 and have found that
lactate may be involved in appetite-regulatory response.39 It is possible that other relevant hormones such
as cortisol and adrenaline may play a role in this intensity dependent appetite regulation. The implications for a superior exercise modality with regard to caloric control remains unclear, but given the correlation between fat mass and fullness immediately after HIIT as well as the difference in subjective appetite, overweight and obese individuals with excess adiposity may confer greater benefits from HIIT. Additionally, HIIT may serve as a strategy to acutely control appetite.
training when compared to 45 minutes of aerobic activity.26 That is, our findings only deal with individual
preferences rather than actual food consumption. Furthermore, the greater implicit wanting for HFSA foods in MICT 30 minutes after exercise suggests a greater preference for calorically dense foods following training. HIIT or HIRT may be a better training modality for individuals who overeat high fat savory foods. For these specific individuals, HIIT may provide more benefits with its appetite suppression effect. The negative correlation between choice frequency for LFSA and lean mass immediately
following MICT suggests that individuals with greater amounts of lean mass may have a lower preference for low fat savory foods that tend to be dense in micronutrients.
The lack of difference in appetite is inconsistent with prior literature11 that demonstrated an increase in
orexigenic hormones within women following exercise. Furthermore, based upon the paradigm that women have appetite regulatory mechanisms to preserve body fat11, the greater preference for calorically
dense foods following exercise and greater existence of body composition and RMR related correlations between food preference in men seems irregular. Men with greater LM and higher RMR may have the least preference for these foods following MICT. These correlations should be applied with caution as the sample size were reduced by half.
Our hypothesis that ghrelin would be lower following HIRT compared to MICT was correct. Ghrelin levels were not significantly different between HIIT and MICT, but the change was similar to HIRT; the lack of difference in ghrelin results likely comes from the variability in the HIIT sample. The lack of direct consistency between the ghrelin results and subjective appetite results supports the importance of measuring both types of hunger responses for both physiological and clinical confirmation. The
after exercise. Application of these results should be taken with some caution as without assessment of post exercise food intake, the clinical relevance of these measures remains to be seen.
A few individuals struggled with the lack of rest with the HIRT protocol, despite finishing the entirety of the sets. One individual included within the analysis was only able to complete half of the HIIT protocol. Comparatively to other studies of this nature, we were unable to utilize a 12 hour fast and standardized meal to control for preceding appetite, and instead instructed participants to record their dietary intake. Other studies of this nature also use a more robust hormone profile, and the difference in levels of PYY and Leptin remain to be seen. Most prominently, incorporating a standardized food buffet post exercise, as with the case of the work of Sim et al.19, would have yielded a practical measure of appetite
differences on actual food choices. Additionally, future studies would benefit from measurement of relevant hormones, such as cortisol, adrenaline, and others, to more clearly identify the mechanisms contributing to the change in appetite.
REFERENCES
1. Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA. 2016. doi:10.1001/jama.2016.6458
2. Fryar CD, Carroll MD, Ogden CL. Prevalence of Overweight, Obesity, and Extreme Obesity Among Adults Aged 20 and Over: United States, 1960–1962 Through 2013–2014. 2016:6. https:// www.cdc.gov/nchs/data/hestat/obesity_adult_13_14/obesity_adult_13_14.pdf.
3. Pi-Sunyer FX. Health implications of obesity. Am J Clin Nutr. 1991. doi:10.1017/S0266462300001604
4. Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: Payer-and service-specific estimates. Health Aff. 2009. doi:10.1377/hlthaff.28.5.w822 5. Daskapan A, Tuzun EHE, Eker L, et al. Perceived barriers to physical activity in university
students. J Sport Sci Med. 2006.
on cardiometabolic risk factors in overweight/obese women. J Sports Sci. 2016. doi:10.1080/02640414.2016.1149609
7. Wingfield HL, Smith-Ryan AE, Melvin MN, et al. The acute effect of exercise modality and nutrition manipulations on post-exercise resting energy expenditure and respiratory exchange ratio in women: a randomized trial. Sport Med - Open. 2015. doi:10.1186/s40798-015-0010-3
8. Smith-Ryan AE, Melvin MN, Wingfield HL. High-intensity interval training: Modulating interval duration in overweight/obese men. Phys Sportsmed. 2015. doi:10.1080/00913847.2015.1037231 9. Westcott WL. Resistance training is medicine: Effects of strength training on health. Curr Sports
Med Rep. 2012. doi:10.1249/JSR.0b013e31825dabb8
10. Holliday A, Blannin AK. Very low volume sprint interval exercise suppresses subjective appetite, lowers acylated ghrelin, and elevates GLP-1 in overweight individuals: A pilot study. Nutrients. 2017. doi:10.3390/nu9040362
11. Hagobian TA, Sharoff CG, Stephens BR, et al. Effects of exercise on energy-regulating hormones and appetite in men and women. AJP Regul Integr Comp Physiol. 2008.
doi:10.1152/ajpregu.90671.2008
12. Caudwell P, Finlayson G, Gibbons C, et al. Resting metabolic rate is associated with hunger, self-determined meal size, and daily energy intake and may represent a marker for appetite. Am J Clin Nutr. 2013. doi:10.3945/ajcn.111.029975
13. Péronnet F, Massicotte D. Table of nonprotein respiratory quotient: an update. Can J Sport Sci. 1991.
14. Matos VAF, de Souza DC, Browne RAV, dos Santos VOA, Costa EC, Fayh APT. Acute effect of high-intensity interval exercise and moderate-intensity continuous exercise on appetite in
overweight/obese males: a pilot study. Sport Sci Health. 2017;13(2):403-410. doi:10.1007/s11332-017-0372-7
doi:10.1249/MSS.0000000000001296
16. Martins C, Stensvold D, Finlayson G, et al. Effect of moderate- and high-intensity acute exercise on appetite in obese individuals. Med Sci Sports Exerc. 2015.
doi:10.1249/MSS.0000000000000372
17. Metcalfe RS, Koumanov F, Ruffino JS, et al. Physiological and molecular responses to an acute bout of reduced-exertion high-intensity interval training (REHIT). Eur J Appl Physiol. 2015. doi:10.1007/s00421-015-3217-6
18. Sim AY, Wallman KE, Fairchild TJ, Guelfi KJ. Effects of high-intensity intermittent exercise training on appetite regulation. Med Sci Sports Exerc. 2015. doi:10.1249/MSS.0000000000000687 19. Sim AY, Wallman KE, Fairchild T, Guelfi KJ. High-intensity intermittent exercise attenuates
ad-libitum energy intake: Discovery Service for Endeavour College of Natural Health Library. Int J Obes. 2014.
20. Beaulieu K, Olver TD, Abbott KC, Lemon PWR. Energy intake over 2 days is unaffected by acute sprint interval exercise despite increased appetite and energy expenditure. Appl Physiol Nutr
Metab. 2015. doi:10.1139/apnm-2014-0229
21. Goto K, Shioda K, Uchida S. Effect of 2 days of intensive resistance training on appetite-related hormone and anabolic hormone responses. Clin Physiol Funct Imaging. 2013.
doi:10.1111/cpf.12005
22. Baylor LS, Hackney AC. Resting thyroid and leptin hormone changes in women following intense, prolonged exercise training. Eur J Appl Physiol. 2003. doi:10.1007/s00421-002-0737-7 23. Jürimäe J, Mäestu J, Jürimäe T. Leptin as a marker of training stress in highly trained male
rowers? Eur J Appl Physiol. 2003. doi:10.1007/s00421-003-0879-2
24. Broom DR, Batterham RL, King JA, Stensel DJ. Influence of resistance and aerobic exercise on hunger, circulating levels of acylated ghrelin, and peptide YY in healthy males. AJP Regul Integr
In: Journal of Physiology. ; 2009. doi:10.1113/jphysiol.2008.164269
26. Balaguera-Cortes L, Wallman KE, Fairchild TJ, Guelfi KJ. Energy intake and appetite-related hormones following acute aerobic and resistance exercise. Appl Physiol Nutr Metab. 2011. doi:10.1139/h11-121
27. Guelfi KJ, Donges CE, Duffield R. Beneficial effects of 12 weeks of aerobic compared with resistance exercise training on perceived appetite in previously sedentary overweight and obese men. Metabolism. 2013. doi:10.1016/j.metabol.2012.08.002
28. Dos Prazeres TMP, Aniceto RR, Do Rêgo Barros TA, De Lima FFM, Guerra RLF, Do Prado WL. Do different weight training methods change the appetite of young adults? Rev da Educ Fis. 2016. doi:10.4025/jphyseduc.v27i1.2711
29. Larson-Meyer DE, Palm S, Bansal A, Austin KJ, Hart AM, Alexander BM. Influence of running and walking on hormonal regulators of appetite in women. J Obes. 2012.
doi:10.1155/2012/730409
30. Unick JL, Otto AD, Goodpaster BH, Helsel DL, Pellegrini CA, Jakicic JM. Acute effect of walking on energy intake in overweight/obese women. Appetite. 2010.
doi:10.1016/j.appet.2010.07.012
31. Sim AY, Wallman KE, Fairchild TJ, Guelfi KJ. High-intensity intermittent exercise attenuates ad-libitum energy intake. Int J Obes. 2014. doi:10.1038/ijo.2013.102
32. Mayhew JL, Prinster JL, Ware JS, Zimmer DL, Arabas JR, Bemben MG. Muscular endurance repetitions to predict bench press strength in men of different training levels. J Sports Med Phys Fitness. 1995.
33. Pescatello LS, Arena R, Riebe D, Thompson PD. ACSM’s guidelines for exercise testing and prescription. 9th. Local Gov Stud. 2014. doi:10.1080/03003930500157457
34. Weir J. New methods for calculating metabolic rate with special reference to protein metabolism.
J Physiol. 1949. doi:PMCID: PMC1392602
motivation to eat in human subjects: a review of their reliability and validity with an evaluation of new hand-held computerized systems for temporal tracking of appetite ratings. Br J Nutr.
2000;84(04):405. doi:10.1017/S0007114500001719
36. Finlayson G, King N, Blundell J. The role of implicit wanting in relation to explicit liking and wanting for food: Implications for appetite control. Appetite. 2008.
doi:10.1016/j.appet.2007.06.007
37. Paoli A, Moro T, Marcolin G, et al. High-Intensity Interval Resistance Training (HIRT) influences resting energy expenditure and respiratory ratio in non-dieting individuals. J Transl Med. 2012. doi:10.1186/1479-5876-10-237
38. Borg G. Perceived exertion as an indicator of somatic stress. Scand J Rehabil Med. 1970. doi:S/N 39. Islam H, Townsend LK, McKie GL, Medeiros PJ, Gurd BJ, Hazell TJ. Potential involvement of