CONTRIBUTOR:Jonathan M. Spector, MD, MPH
Department of Health Policy and Management, Harvard School of Public Health, Boston, Massachusetts
Address correspondence to Jonathan M. Spector, MD, MPH, Harvard School of Public Health, Department of Health Policy and Management, 4th Floor, 677 Huntington Ave, Boston, MA 02115. E-mail: [email protected]
Accepted for publication Jan 25, 2012 ABBREVIATIONS
MDG—Millennium Development Goal U5MR—under-5 mortality rate UN—United Nations
doi:10.1542/peds.2011-3885
Inside Millennium Development Goal 4
This Pediatrics Perspectives column traces the origins of the promises and commitments made to decrease global under-5 mortality. The disparities that exist worldwide are extraordinarily large, although significant progress has been made since the establishment of the Millennium Development Goals (MDGs). Dr Spector traces the origins and challenges of Goal 4 (of 8) that relate specifically to this issue. Although overall survival rates are improving, outcome gaps in under-5 mortality have widened between rich and poor nations. Clearly, the MDGs must be looked at as a large package. There are specific measurements for each goal, but success in 1 area influences the outcomes in the others. Our advocacy efforts should focus on improving the lives of the world’s poorest people broadly. World leaders have commit-ted to achieving the MDGs by 2015. We all need to use our influence and personal resources to push the in-ternational community to succeed in eliminating extreme poverty and hun-ger everywhere, ultimately allowing for elimination of the growing health
disparities among the affluent and poorest nations.
—Jay E. Berkelhamer, MD
Editor, Global Health Perspectives
The Millennium Development Goals (MDGs) have been dubbed the“world’s biggest promise.”1 At the turn of the
21st century, 189 (now 192) United Nations (UN) member states agreed to support the most comprehensive poverty reduction objectives ever es-tablished (Table 1).2,3 Child mortality
is addressed through Goal 4: reduction of the global under-5 mortality rate (U5MR) by two-thirds between 1990 and 2015, equivalent to an annual drop rate of 4.3% (Table 2).4 In 1990,
the U5MR was estimated at 84 of 1000 live births, and 11.9 million largely preventable child deaths took place. If MDG 4 could be achieved, 30 million children would be saved by 2015.2
Since their launch, the MDGs have been praised and condemned.5,6This
synopsis reviews the history of MDG 4, its influence, major criticisms, and proposed ways forward after its expiration.
ORIGIN
The MDGs gained unprecedented trac-tion early on partly because their root ideas were not altogether new, but rather represented a culmination of various broad-reaching pledges made in the 1990s through a series of global summits.6For child mortality, the
ear-liest targets had been established at the World Summit for Children at the UN in 1990 (in what was, up to that time, the largest gathering of world leaders in history), followed by a reaffirmation in 1994 at the UN Inter-national Conference on Population and Development in Cairo, and put forth yet again in 1996 through the International Development Goals recommended by the Development Assistance Committee of the Organization for Economic Co-operation and Development (Table 3).1,7
The experience of the International De-velopment Goals, the MDG’s immediate precursor and blueprint, is a cau-tionary reminder of the importance of stakeholder mix in a global tar-get setting.1 Having been generated
economies and without the involve-ment of certain influential agencies such as the World Bank and Inter-national Monetary Fund, they were scarcely acknowledged in developing countries and received media attention for less than a week.1In anticipation
of the year 2000 and recognizing a “unique and symbolically compelling” opportunity, the UN General Assembly under Secretary-General Kofi Annan resolved to designate its 55th session “The Millennium Assembly.”8 The
res-olution they unanimously approved, the Millennium Declaration, included the two-thirds reduction target for under-5 mortality.9The following year,
in the Assembly’sRoad Map Towards
the Implementation of the United Nations Millennium Declaration, this target was linked with“indicators,”to guide measurement, and with a“goal,” to aid conceptual simplicity.6,10 MDG 4
was born.
INFLUENCE
Child mortality has declined markedly in all regions since 1990.11The U5MR
fell to an estimated 53 per 1000 live births in 2011, or 7.2 million total deaths, 40% of which occurred in the neonatal period.12,13 The overall
an-nualized rate of reduction since 1990 is just.2%, but the relatively greater decline from 2000–2011 (2.6%) com-pared with 1990–2000 (1.9%) reveals accelerated headway in recent years.12
In “Countdown to 2015,” a multidisci-plinary, multi-institution collaboration that tracks MDG progress, the authors report that 19 of 68 high-priority countries are on track for meeting MDG 4, 17 have cut the U5MR in half, and 47 have made significant gains.14,15
The MDGs generally are credited with helping progress by spurring a re-naissance of child-survival activities, increasing publicity, and providing a spotlight for advocacy efforts.6,16,17They
have been used by national health ministries as political leverage within their own countries and in negotiations with the international aid community.3
The results-based framework of the
MDGs galvanized donors in new ways, given that investment returns could be quantified theoretically.6
The MDGs also drew greater attention to health metrics.18Accountability for
progress brought into sharp focus the reliance on, and imperfect science of, mortality estimates traditionally generated by the UN and academic institutions.12,18,19Conflicting reports of
global and country-level MDG progress over the past decade further high-lighted problems with existing empirical data and standard methodologies.13,20
Perhaps not by coincidence, 3 major measurement initiatives were created in this time: (1) the World Health Orga-nization–led Health Metrics Network (formed in 2005), a country-owned global partnership aimed at strength-ening national health information sys-tems; (2) the Institute for Health Metrics and Evaluation (founded in 2007), an independent global health research center based at the University of Washington; and (3) the UN Commis-sion on Information and Accountability for Women’s and Children’s Health (established 2010), charged with de-signing action plans for global report-ing and accountability on women’s and children’s health.21–23
Work to achieve MDG 4 additionally brought to light the challenges of translating knowledge into practice in high-priority countries. Failure of evidence-based innovations to straight-away produce public health impact has resulted in calls for emphasis on im-plementation research.24–26
Finally, MDG 4 put neonatal survival on the map. Recognition that MDG 4 will not be met without sizable reductions in neonatal mortality led to substantial increases in advocacy, funding, and ac-tivities to support newborn health.27,28
CRITICISMS
Chief concerns with MDG 4 parallel those expressed about the MDGs as TABLE 1 The MDGs10
1. Eradicate extreme poverty and hunger. 2. Achieve universal primary education. 3. Promote gender equality and empower women. 4. Reduce child mortality.
5. Improve maternal health.
6. Combat HIV/AIDS, malaria, and other diseases. 7. Ensure environmental sustainability. 8. Develop a global partnership for development.
TABLE 2 MDG 410
Goal 4: Reduce child mortality
Target 4A: Reduce by two-thirds, between 1990
Ć and 2015, the mortality rate in children
Ć younger than 5 y
Indicator 4.1: Mortality rate in children
Ć younger than 5 y
Indicator 4.2: Infant mortality rate Indicator 4.3: Proportion of 1-year-old
Ć children immunized against measles
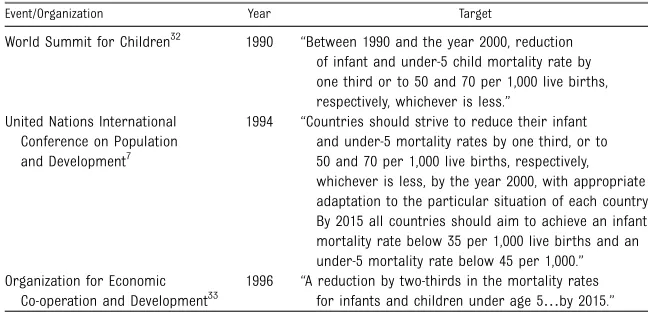
TABLE 3 Global Target Setting for Child Mortality Preceding MDG 4
Event/Organization Year Target
World Summit for Children32 1990 “Between 1990 and the year 2000, reduction of infant and under-5 child mortality rate by one third or to 50 and 70 per 1,000 live births, respectively, whichever is less.”
United Nations International Conference on Population and Development7
1994 “Countries should strive to reduce their infant and under-5 mortality rates by one third, or to 50 and 70 per 1,000 live births, respectively, whichever is less, by the year 2000, with appropriate adaptation to the particular situation of each country. By 2015 all countries should aim to achieve an infant mortality rate below 35 per 1,000 live births and an under-5 mortality rate below 45 per 1,000.” Organization for Economic
Co-operation and Development33
1996 “A reduction by two-thirds in the mortality rates for infants and children under age 5…by 2015.”
806 SPECTOR
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news
a whole. A shared cross-sectoral theory of development was not the starting place for their development, and the case has been made that the narrow focus of specific goals fosters vertical programming and“sectoral silos.”6 A
major implication is competition among groups for funding and attention while end goals are the same.6
Judging performance of individual countries has come under fire. The capacity curve for reducing the U5MR in any country is likely to be S-shaped: requiring large inputs for small gains initially, then realizing more improve-ments with less effort as health sys-tems are upgraded, and in the end, needing greater inputs again to close
final remaining gaps.6,16 All countries
are not equally positioned to achieve similar progress. The MDGs were con-structed as global goals, and charac-terizing as “failures” those countries that have made important gains but fallen short of meeting MDG targets has been called unfair and potentially harmful.5
Another MDG 4 criticism relates to the construction of the target in pro-portional terms. Reducing rates, ver-sus absolute numbers, is considerably harder for countries that are worse off initially.5,16Lastly, the MDGs have been
subject to accusations of widening equity gaps within countries. Because the target is stated in terms of soci-etal averages, progress in better-off groups can lead to “success,” even without health improvements in the most disadvantaged populations.5,14,29
MDG 4 2.0
The post-2015 debate has not com-menced openly among dominant stake-holders for fear of distraction from work to achieve the current MDGs.30
Those who have examined scenarios af-ter expiration propose the need to con-sider both process and framework.6,30
Among the possibilities are maintaining
existing targets and extending the deadline, keeping and expanding on the existing framework, generating entirely new framework content, or doing nothing.30 One survey in
low-income countries found reluctance to simply extend the deadline for fear of undermining accountability and the value of time-bound goals.30 At this
early stage, there appears to be sup-port for some form of follow-up, one that incorporates a spirit of equity, reduced fragmentation, and focus on development.6,31
CONCLUSIONS
Jeffrey Sachs, Special Advisor to UN Secretaries-General Kofi Annan and Ban-Ki Moon on the MDGs, character-izes them as a revolution in thinking and practice in public health.3,11To call
the MDGs a success is not to say that considerable work does not need to be done; it does. Whether by design or by accident, the message spelled out by MDG 4 was brilliantly simple. List-ing principles that should inform global human development is not
dif-ficult. But translating them into ac-cessible, actionable ideas that capture excitement, motivate, and effect change is far from straightforward. Those work-ing to improve child health who have been driven by MDG 4 and the sense of inclusion in a vital global effort will agree that this goal was worth setting.
ACKNOWLEDGMENTS
The author thanks Grace Galvin for her assistance with research for this article.
REFERENCES
1. Hulme D. The Making of the Millennium Development Goals: Human Development Meets Results-based Management in an Imperfect World. BWPI Working Paper 16. Manchester, United Kingdom: Brooks World Poverty Institute; 2007
2. UN Millennium Project.Investing in Devel-opment: A Practical Plan to Achieve the Millennium Development Goals. New York: UN Millennium Project; 2005
3. Sachs JD. Health in the developing world: achieving the Millennium Development Goals. Bull World Health Organ. 2004;82(12):947– 949; discussion 950–952
4. Wagstaff A, Claeson M. The Millennium Development Goals for Health: Rising to the Challenge. Washington, DC: World Bank; 2004
5. Vandermortele J. The MDG conundrum: meeting the targets without missing the point.Dev Policy Rev. 2009;27(4):355–371
6. Waage J, Banerji R, Campbell O, et al. The Millennium Development Goals: a cross-sectoral analysis and principles for goal setting after 2015 Lancet and London In-ternational Development Centre Commis-sion.Lancet. 2010;376(9745):991–1023
7. Cairo Declaration on Population & De-velopment. ICPPD. Available at: www.un. org/popin/icpd/conference/bkg/egypt. Accessed December 23, 2011
8. Millennium Summit. Available at: www. un.org/millennium. Accessed December 21, 2011
9. United Nations General Assembly. United Nations Millennium Declaration. New York, NY: United Nations; 2000
10. United Nations General Assembly. Road Map Towards the Implementation of the United Nations Millennium Declaration. New York, NY: United Nations; 2001
11. Sachs J. The MDG decade: looking back and conditional optimism for 2015.Lancet. 2010; 376(9745):950–951
12. Lozano R, Wang H, Foreman KJ, et al. Progress towards Millennium Development Goals 4 and 5 on maternal and child mor-tality: an updated systematic analysis. Lancet. 2011;378(9797):1139–1165
13. Rajaratnam JK, Marcus JR, Flaxman AD, et al. Neonatal, postneonatal, childhood, and under-5 mortality for 187 countries, 1970-2010: a systematic analysis of progress towards Millennium Development Goal 4. Lancet. 2010;375(9730):1988–2008
14. Requejo J, Bryce J. Countdown to 2015 Decade Report (2000–2010): Taking Stock of Maternal, Newborn and Child Survival. Geneva, Switzerland: World Health Organi-zation; 2011
15. Lawn J. Are the millennium development goals on target? BMJ. 2010;341(Sep 14): c5045
16. Easterly W. How the Millennium Develop-ment Goals are unfair to Africa.World Dev. 2009;37(1):26–35
17. Clemens MA, Kenny CJ, Moss TJ. The trouble with the MDGs: confronting expectations of aid and development success. World Dev. 2007;35(5):735–751
18. Byass P, Graham WJ. Grappling with
uncertainties along the MDG trail. Lancet. 2011;378(9797):1119–1120
19. Chan M, Kazatchkine M, Lob-Levyt J, et al.
Meeting the demand for results and ac-countability: a call for action on health data
from eight global health agencies. PLoS Med. 2010;7(1):e1000223
20. Murray CJ, Frenk J. Health metrics and eval-uation: strengthening the science.Lancet. 2008;371(9619):1191–1199
21. AbouZahr C, Boerma T. Health information systems: the foundations of public health.
Bull World Health Organ. 2005;83(8):578– 583
22. Institute for Health Metrics and Eval-uation. History. Available at: www.
healthmetricsandevaluation.org/about-ihme/ history. Accessed December 21, 2011
23. UN establishes high-level commission to
track results and resources for women’s
and children’s health. Available at: www.un. org/millenniumgoals/pdf/Press_Release_
Accountability_16Dec_final.pdf. Accessed December 10, 2011
24. Sanders D, Haines A. Implementation
re-search is needed to achieve international health goals.PLoS Med. 2006;3(6):e186
25. Madon T, Hofman KJ, Kupfer L, Glass RI.
Public health. Implementation science. Science. 2007;318(5857):1728–1729
26. Whitworth J, Sewankambo NK, Snewin VA.
Improving implementation: building research capacity in maternal, neonatal, and child
health in Africa.PLoS Med. 2010;7(7):e1000299
27. Martines J, Paul VK, Bhutta ZA, et al; Lancet Neonatal Survival Steering Team. Neonatal
survival: a call for action.Lancet. 2005;365 (9465):1189–1197
28. Lawn JE, Cousens SN, Darmstadt GL, et al; Lancet Neonatal Survival Series steering
team. 1 year after The Lancet Neonatal Survival Series—was the call for action
heard?Lancet. 2006;367(9521):1541–1547
29. Gwatkin DR. Who Would Gain Most from Efforts to Reach the Millennium Development
Goals for Health?Washington, DC: World Bank’s Working Group on the Millennium Development Goals for Health, Nutrition, and
Population; 2002
30. Pollard A, Sumner A, Polato-Lopes M, de
Mauroy A. 100 voices: Southern NGO
per-spectives on the Millennium Development Goals and beyond.IDS Bull. 2011;42(5):120– 123
31. Vandermortele J, Delamonica E. Taking the
MDGs beyond 2015: hasten slowly.IDS Bull. 2010;41(1):60–69
32. Major Goals for Child Survival. Development and protection. Available at: www.unicef.org/
wsc/goals.htm#Major. Accessed December
28, 2011
33. Development Assistance Committee of the
Organisation for Economic Cooperation and Development.Shaping the 21st Century: The Contribution of Development Co-operation. 1996. Available at: www.oecd.org/dataoecd/ 23/35/2508761.pdf. Accessed February 24,
2012
FINANCIAL DISCLOSURE:The author has indicated he has nofinancial relationships relevant to this article to disclose. FUNDING:No external funding.
808 SPECTOR
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2011-3885 originally published online April 2, 2012;
2012;129;805
Pediatrics
Jonathan M. Spector
Inside Millennium Development Goal 4
Services
Updated Information &
http://pediatrics.aappublications.org/content/129/5/805 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/129/5/805#BIBL This article cites 19 articles, 1 of which you can access for free at:
Subspecialty Collections
alth_sub
http://www.aappublications.org/cgi/collection/international_child_he International Child Health
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2011-3885 originally published online April 2, 2012;
2012;129;805
Pediatrics
Jonathan M. Spector
Inside Millennium Development Goal 4
http://pediatrics.aappublications.org/content/129/5/805
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2012 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 28, 2020
www.aappublications.org/news