A Program to Immunize Hospitalized Preschool-aged Children:
Evaluation and Impact
Louis M. Bell, MD*‡; Michele Pritchard, RN*; Rebecca Anderko, BA*; and Robert Levenson, MBA§
ABSTRACT. Objective. The Standards for Pediatric Immunization Practices suggest that hospitalization be viewed as an opportunity to vaccinate children. The pur-pose of the present study is 1) to determine the immuni-zation status of an urban population of hospitalized pre-school-aged children, 2) to study the impact of an immunization program designed to vaccinate hospital-ized 0 to 2-year-old children who are underimmunhospital-ized at admission, and 3) to make immunization a routine part of care for the hospitalized child.
Methods. Prospective evaluation of the immuniza-tion status of hospitalized 0 to 2-year-old residents of Philadelphia admitted to an urban children’s hospital was performed. With verification of the child’s immuni-zation record through the primary care provider (PCP), needed immunizations were given and records were for-warded to notify the PCP. Educational information was provided to families and health care providers.
Main Outcome Measure. The percentage of children fully immunized on admission compared with the per-centage at the time of discharge.
Results. Two thousand three hundred twenty-nine children from 0 to 2 years of age were hospitalized dur-ing the 22-month study period. Immunization records were verified in 86% (2006), requiring an average of 1.5 phone calls to the PCP. The mean patient age was 10 months. Average hospital length of stay was 4 days. On admission, 49% (980) of the 2006 study patients were fully immunized. The remaining 51% (1026) were eligi-ble for vaccination. Immunizations were delayed greater than or equal to 2 months in 18% (355) of the children. Neither type of health care insurance nor site of primary care affected the immunization status of those evaluated at the time of admission.
Sixty-six percent (N5674) of eligible patients received at least one vaccination before hospital discharge. Med-ical contraindications accounted for only 4% of the rea-sons eligible patients were not immunized. Of the 2006 children evaluated, the percentage of those fully vacci-nated for age increased significantly from 44% on admis-sion to 70% on discharge.
Conclusion. As a result of this program, there was a significant improvement in vaccination percentage at the time of hospital discharge in this group of urban
pre-school-aged children. The development of an immuniza-tion program to vaccinate hospitalized preschool chil-dren is an opportunity to immunize in the urban setting where there is a high prevalence of underimmunization. In addition, it provides an opening for educational programs for families, nurses, and housestaff and link-age to the community PCPs.Pediatrics 1997;100:192–196; immunization rates, hospitalization, underimmunization, preschool age children.
ABBREVIATIONS. CDC, Centers for Disease Control and Preven-tion; PCP, primary care provider; OPV, oral polio vaccine; MMR, measles-mumps-rubella.
D
espite some improvement over the last 5 years, vaccine coverage for preschool-aged children falls short of goals set in the recent Childhood Immunization Initiative of 1993 of full immunizations for at least 90% of children by their second birthday.1The most recent data from the Centers for Disease Control and Prevention (CDC) (National Health In-terview Survey) reveals that as of July 1994 to June 1995, approximately 71% of 2-year-old children are fully vaccinated.1 The urban preschool-aged child
may be at even greater risk for underimmunization. Vaccination coverage at 24 months of age among Latino and African-Americans living in south central and east Los Angeles was 42% and 26%, respectively, in 1992.2Furthermore, urban children are more likely
to experience substantial barriers in access to and use of primary care and these barriers may worsen if congressional initiatives to reduce spending for pro-grams designed to improve access to healthcare are successful.3Therefore, it seems reasonable that
com-munity-based primary care and hospital-based prac-tices caring for urban children join to eliminate missed opportunities to immunize using every inter-action with the health care system as an opportunity to vaccinate, including hospitalization.
The purpose of the current study is to determine the need for immunizations in an urban population of hospitalized preschool-aged children and to re-port the impact of an immunization program that was designed to:
1. Identify hospitalized 0 to 2-year-old children who are underimmunized and provide needed vacci-nation before discharge,
2. Communicate with PCPs about vaccines
provided, From the *Divisions of Immunologic and Infectious Diseases, and
‡Emer-gency Medicine, Children’s Hospital of Philadelphia, University of Penn-sylvania; and §Philadelphia Department of Public Health, Philadelphia, Pennsylvania.
Presented at the meeting of the Ambulatory Pediatric Association, May, 1995, San Diego, CA and at the 30th National Immunization Conference, April, 1996, Washington, DC.
Received for publication Jun 11, 1995; accepted Feb 15, 1996.
Reprint requests to (L.M.B.) Section of Infectious Diseases, 34th Street and Civic Center Blvd, Philadelphia, PA 19104.
3. Make immunization a routine part of care for the hospitalized child, and
4. Provide education about the importance of elimi-nating missed opportunities to nursing, hous-estaff physicians, PCPs, and parents.
METHODS The Immunization Team Organization
In January 1994, The Children’s Hospital of Philadelphia, with funding from the Philadelphia Health Department and the CDC, established an immunization team (consisting of a physician, a nurse coordinator, and an assistant) to implement a program designed to immunize hospitalized preschool aged children be-fore discharge. The hospital, located in west Philadelphia, serves the local communities in the western and southern sections of the city with 15 000 inpatient admissions and 200 000 combined emer-gency department and outpatient visits each year. In this section of the city, there are approximately 47 000 children from birth to 4 years of age, 85% are African-American.
Implementation of the program required communication and planning within the hospital and with the external, PCP groups. Hospital preparation involved informing nursing, resident and attending physician groups, inpatient pharmacy (who had to set up a system to ensure that the patients were charged for the vaccine they dispensed), and the unit base clerks. External prep-aration required letters and phone calls to different health care providers in our community to explain the program and address their concerns, if any.
The immunization nurse coordinator organized the inpatient nursing staff on six different medical and surgical units orienting one new unit a month for the first 6 months. Patients in the intensive care units and the oncology unit were not included. The inpatient nursing staff on each unit chose representatives to serve on an immunization task force for that unit. During the start up of the program, quarterly meetings with the task force were held to provide education and updates on immunization practices and to discuss problems and progress of the inpatient program. Subse-quently, the task force representatives acted as a link between the inpatient units and the immunization nurse coordinator.
Patient Identification and Vaccination
Prospective evaluation of the immunization status of all hospi-talized 0 to 2-year-old residents of Philadelphia admitted to an urban children’s hospital was begun in February 1994. On a daily basis, the immunization nurse coordinator and assistant identified all age appropriate children admitted to six different medical and surgical units. The PCP of each child was contacted to verify the child’s utilization of the primary care site as well as to retrieve the immunization record.
After discussions with the PCP and review of the child’s medical status and immunization record, the pediatric resident assigned to the patient was contacted and in the first 2 years of the program, was told what immunizations were needed if the child was delayed. Subsequently, the entire immunization record and the recommended immunization are taped to the front cover of the patient chart. Before vaccination, informed consent was obtained and educational infor-mation and teaching were provided about future immunizations by the inpatient nursing staff and/or the immunization nurse coordina-tor. The vaccine was distributed by the hospital pharmacy without charge under the CDC vaccine program. Immunizations were ad-ministered by the nursing staff on the day of discharge from the hospital. Once the child received the vaccine, an updated immuni-zation record was mailed or faxed to the PCP.
Definitions
The child’s immunization status was determined on admission. Delays were determined based on the consensus or harmonized schedule agreed upon by the American Academy of Pediatrics, the American Academy of Family Practice and the CDC Advisory Committee on Immunization Practices.4The harmonized schedule
includes an extended acceptable period over which oral polio vaccine (OPV) and measles-mumps-rubella (MMR) vaccines may be administered. The immunization status was designated due for next vaccination if the child was eligible for any vaccination at the time of hospitalization but was less than 2 months delayed for age.
The immunization status was designated delayed if the child was more than 2 months delayed for age.
Contraindications to immunization were determined during discussion with the team of physicians caring for the child while hospitalized (attending and housestaff) and the PCP. In general, children were considered medically eligible for vaccination before discharge with the diphtheria-pertussis and tetanus vaccine if they had no fever (,38°C), were recovering from illness, and appeared well. Likewise, children were eligible for OPV, MMR, and/or
Haemophilus influenzae type b vaccinations if they were
immuno-competent and had fevers,39°C, were recovering from illness, and appeared well before discharge.5If the patient did not meet
the above criteria and/or the PCP or inpatient attending physician requested no vaccination for other reasons not covered above, then immunizations were withheld.
Data Collection and Analysis
Demographic information on all evaluated children was col-lected from the inpatient record including PCP, insurance type, and length of stay in the hospital. In addition, dates and types of immunizations were recorded. Information on the success and effort required to obtain the immunization records was moni-tored. Finally, the number and types of vaccines given to each child and the immunization status at the time of discharge were recorded for all children receiving vaccinations during their hos-pitalization.
x2analysis was used for analysis of categorical data. P values
,.05 were considered statistically significant. Finally, the cost of the program was analyzed. The cost of vaccine is based on CDC cost per dose from a price list published January 25, 1996 (DOC#2639).
RESULTS
During the first 22 months (February 1994 to No-vember 1995) of the inpatient vaccination program, there were 2329 admissions of 0 to 2-year-old children to the medical and surgical units involved in the pro-gram. Of this group, 2080 (89%) children were primar-ily evaluated by the immunization team. The majority of the 249 children not evaluated were missed during the first 6 months of the start-up phase of the program, a time when a new medical or surgical unit was intro-duced to the program each month. The remainder of patients who were missed included those infants in a neonatal transitional unit (not included until year 2 of the program), children on the oncology unit or patients who were admitted and discharged from the hospital in a single weekend. Immunization records were avail-able for review for 2006 or 96% of the 2080 children. The immunization records of 73 children (or 4% of the group of 2006) arrived after the children were dis-charged and were included in the analysis. The number 2006 comprises the group of children who were fully evaluated for immunization status and need for vacci-nation.
All children evaluated lived in the city of Philadel-phia, 71% were from west and south Philadelphia. The mean age of the evaluated group was 10 months (66.5), 57% were boys. The average length of hospi-talization was 4.3 days (64.2) (range 0 to 99). An average of 1.5 phone call attempts, (61.1) (range 0 to 11), were required to obtain the immunization records from the PCP. On average, it took 4 hours each day to retrieve the immunization records. Only a few of the parents had immunization records with them. During the course of the program, more than 219 different primary care sites were contacted to verify immunization records.
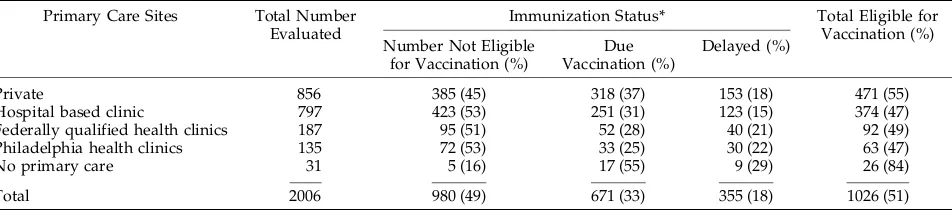
(1026) were eligible for vaccination during hospital-ization. Of those who were eligible for immuniza-tion, 65% (671) were designated as due for next vac-cination, and 35% (355) were delayed. There were no significant differences in immunization status be-tween the sites of primary care (Table 1). Eighty-two percent of the evaluated group were cared for either in privately owned practices or in hospital-based clinics.
The majority of children (55%) were insured by Medicaid managed care (Table 2). Children with pri-vate insurance were just as likely to be underimmu-nized as Medicaid-insured families. Furthermore, there was no difference in immunization status be-tween Medicaid managed care insurers and Medic-aid fee for service. The families who listed self-pay on admission (ie, no insurance), while 6% of the total group, were significantly more likely (P,.05; odds ratio 1.5, 95% confidence interval, 1.0 to 2.5) to be underimmunized than the insured families.
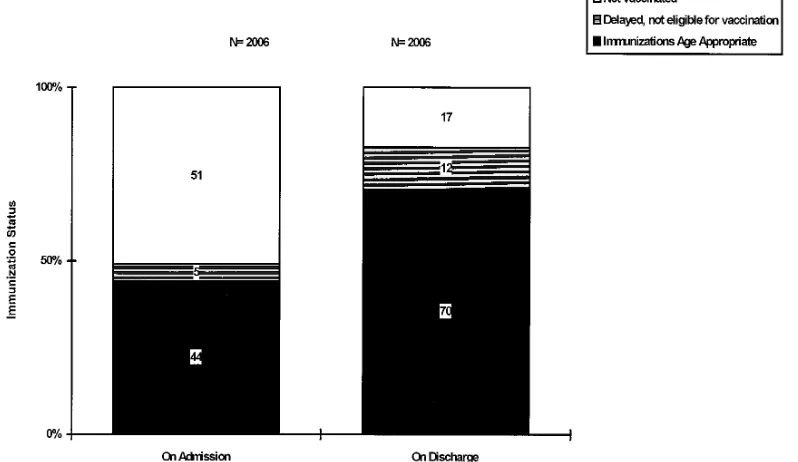
Of 1026 children eligible for vaccination, 66% (674) received at least one immunization before discharge. Eighty-five percent of those vaccinated received mul-tiple immunizations. Over 1504 immunizations were given. Seventy-seven percent of the vaccinated group were brought up to date during their hospi-talization. Of the 2006 children evaluated, the per-centage of hospitalized children who were up to date or fully immunized for age increased significantly from 44% on admission to 70% on discharge (P , .0001; Figure).
Thirty-four percent of the 1026 children who could have been vaccinated while hospitalized did not re-ceive any immunizations. Table 3 outlines the rea-sons for not vaccinating these children. Interestingly, after the change in the way we informed the nurses and physicians of the immunizations that the hospi-talized child required (see “Methods”) the number of ordered, not administered, missed opportunities de-creased by 53%. Note that in 41 children (4%), im-munizations were withheld because it was consid-ered a medical contraindication.
Although all vaccines are provided free under the Federal Immunization Program, cost of the vaccines used (based on CDC cost per dose from price list DOC#2639, January 25, 1996) averaged $505 per month. Salary support for the immunization team was $6354 per month.
DISCUSSION
In 1988, Tifft and Ledermann6 found that 19% of
hospitalized children in Baltimore needed vaccination and suggested that programs be developed to improve immunizations among hospitalized children. In 1994, eighteen standards for Pediatric Immunization Prac-tices were recommended by the National Vaccine Ad-visory Committee and endorsed by the American Academy of Pediatrics. Among the standards is one that requests that each encounter with a health care provider, including an emergency room visit or hospi-talization, is an opportunity to screen the immuniza-tion status and, if indicated, administer needed vac-cines. The standard also calls for informing the child’s regular health care provider about the immunizations administered.5The purpose of the standard is to
elim-inate missed opportunities. Furthermore, recent data suggests that these nontraditional sites may be fertile areas to vaccinate preschool aged children.2,7 In the
current study, 1026 hospitalized children (51% of those evaluated) were eligible to receive immunization(s) during hospitalization and 35% were significantly de-layed on admission.
Interestingly, the site of primary care or the type of insurance had no affect on the immunization status of the children evaluated on admission. Children from private clinics were no more likely to be de-layed than children from other sites (Table 1). This result differs from a recent study in New York where only 26% of children who attended private clinics were up to date for their age for diphtheria-pertussis and tetanus, OPV, and MMR compared with a city-wide coverage of 49%.8Furthermore, in the current
study, Medicaid-managed care insured children were not more likely to be adequately immunized than children with Medicaid, fee for service (Table 2). The main obstacle to providing immunization in nontraditional settings is verification of the immuni-zation records. Parent or caretaker memory of what immunizations have been given or missed has been shown to be inaccurate.9An effective immunization
program in the emergency department, for example, requires a method of rapid retrieval of the immuni-zation record; a requirement that renders emergency department immunization impractical in most set-tings.7Conversely, hospitalization allows for time to
obtain the immunization record. With an average length of stay of 4 days, 96% of records were
ob-TABLE 1. Status of Hospitalized 0 to 2-Year-Old Immunization Children by Primary Care Site
Primary Care Sites Total Number Evaluated
Immunization Status* Total Eligible for Vaccination (%) Number Not Eligible
for Vaccination (%)
Due Vaccination (%)
Delayed (%)
Private 856 385 (45) 318 (37) 153 (18) 471 (55)
Hospital based clinic 797 423 (53) 251 (31) 123 (15) 374 (47)
Federally qualified health clinics 187 95 (51) 52 (28) 40 (21) 92 (49)
Philadelphia health clinics 135 72 (53) 33 (25) 30 (22) 63 (47)
No primary care 31 5 (16) 17 (55) 9 (29) 26 (84)
Total 2006 980 (49) 671 (33) 355 (18) 1026 (51)
tained for review before discharge, the most time-consuming task of the immunization team. On aver-age, more than one phone call attempt was required to the primary care site to obtain the record. Facsim-ile transmission of these records has recently become the most frequent mode of communication.
Indeed, obtaining the immunization record was extremely time consuming requiring one full-time person 4 to 5 hours a day to make the calls to the primary providers office. Two things helped to facil-itate record retrieval. First, an introductory letter, phone call, and an occasional visit by the immuniza-tion team to the primary providers office was neces-sary to explain the program and establish a contact person at each office. Second, the Philadelphia De-partment of Public Health made it known to all providers that exchange of immunization records between health care providers was appropriate as a public health measure and did not require parental consent. Much of the work of the immunization team could be eliminated if an accessible computerized immunization data base existed for preschool aged children. Certainly, easy on line access to immuniza-tion records will become even more vital as health care reform encourages shorter and shorter lengths of stay in the hospital.
Although (51%) 1026 hospitalized children were eli-gible to receive immunization during hospitalization,
TABLE 2. Immunization Status of Hospitalized 0 to 2-Year-Old Children by Insurance Type
Insurance Type Total Number Evaluated
Immunization Status* Total Eligible for
Vaccination (%) Number Not Eligible
for Vaccination (%)
Due Vaccination (%)
Delayed (%)
Medicaid, fee for service
254 123 (48) 87 (35) 44 (17) 131 (52)
Medicaid, managed care
1098 545 (50) 366 (33) 187 (17) 553 (50)
Private 537 270 (50) 182 (34) 85 (16) 267 (50)
Self Pay 117 42 (36) 36 (31) 39 (33) 75 (64)†
Total 2006 980 (49) 671 (33) 355 (18) 1026 (51)
* The immunization status was determined upon admission. Status was “due vaccination” if child was eligible for any vaccination at the time of hospitalization but was less than 2 months delayed for age. “Delayed” was defined as more than 2 months delayed for age. † P,.05, (or 1.5 95% confidence interval, 1.0, 2.5) when compared with other insurance types.
Figure. Comparison of the immunization status of 2006 hospitalized 0 to 2-year-old children at the time of admission and on discharge. (P,.0001 for the difference between the immunizations age appropriate category between admission and discharge).
TABLE 3. Reasons for Not Vaccinating Hospitalized 0 to 2-Year-Old Children
Reasons Number Percent
of Children Eligible for Vaccination (N51026)
Discharged before records obtained 73 7%
Medical contraindication 41 4%
Order not written 54 5%
Ordered, not administered 65 6%
Primary care appointment scheduled* 58 6%
Parent refused 59 6%
Total 350
only 66% received at least one immunization. As com-pliance with the program was evaluated, the number of immunizations that were not ordered (ordered, not written) or not administered (ordered, not adminis-tered) was unacceptably high (Table 3). Thirty-four percent of the not vaccinated children represented missed opportunities by the health care workers in these two categories. Reasons for this involved misun-derstanding about contraindications to vaccinate and orders being overlooked by nursing during a transition to a computerized ordering system. It was discovered that taping the patients immunization record with the recommended vaccines to be given on the front cover of the child’s inpatient chart was more effective than calling the resident and prescribing the needed vac-cines. The nurses and resident physicians had a visual reminder on the patient chart that the child needed to be vaccinated and they could see and decide for them-selves that the patient was indeed delayed by glancing at the immunization record. In only 41 children (4% of cases) were immunizations withheld for medical rea-sons. This low percentage is similar in other studies that found illness to be an unusual reason to withhold needed immunizations in both the inpatient and out-patient settings.10–12Only 6% of parents refused
immu-nizations for their children.
In the current study, 49% of 2006 preschool aged children were up to date on admission to the hospi-tal. These results are similar to a report from Mem-phis in 1992 to 1993, in which 44% of 142 hospitalized children less than 2 years of age were up to date in their immunizations.13 Furthermore, the National
Immunization Survey implemented by the CDC, performed a single survey for July 1994 to June 1995 of caretakers for children 19 to 35 months of age in the US. In Philadelphia, 67 (67.5)% were found to be fully immunized, receiving 4 diphtheria, pertussis and tetanus; 3 oral polio; 1 MMR; and 3 Haemophilus
influenzae type b vaccines. There is no data
specifi-cally for west and south Philadelphia. But in general, immunization rates for the children admitted to the hospital were lower than the National Immunization Survey immunization rates for Philadelphia, 49% compared with 67%.1
Despite the fact that immunizations were not given to 34% of children eligible to receive them, the percent of those who were fully immunized for age significantly improved from 47% on admission to 70% (P . .0001) on discharge from the hospital. In other words, 19% of the preschool-aged children evaluated were brought up to date for immuniza-tions during their hospitalization.
Funding for this program provided salaries for a full-time nurse, an assistant, and a very small amount for a physician director. However, this type of immu-nization program could potentially be started with only minimal funding. Obtaining the records is a vital time-consuming aspect of the program that may require at least a dedicated person working half-time. Nursing education, especially in the first 6 months, may require a coordinator. The hospital, health maintenance orga-nizations, or vaccine manufacturers may be willing to provide the relatively small amount of funds needed to get the program started. Once started, if the work of the
immunization team can be incorporated into the rou-tine care of hospitalization then no funding is needed. Finally, side benefits of this program, that were not formally studied but felt to be a very positive aspect, were in the realm of communication and education. Over 219 different primary care sites were contacted to verify immunization records. The team approach to vaccinating the children of our community was felt to be a positive aspect of the program. The importance of eliminating missed opportunities was an implicit mes-sage in these communications both before and after immunizations were given. Heightened awareness of the importance of immunization and the use of nontra-ditional sites for immunizations was also an important concept learned by the nursing staff and housestaff. Another benefit was related to the Joint Commission on Accreditation of Healthcare Organizations which ex-pects that hospitals support and develop community outreach programs related to health care. This program certainly fills part of that goal.
Further research is underway to study the impact of different types of in hospital educational interven-tions on immunization rates and subsequent visits to the primary care clinic for preschool-aged children.
ACKNOWLEDGMENTS
This work was supported through a contract with the CDC and the Philadelphia Department of Public Health.
The authors wish to thank Flaurence Dong and Travis Quinn for their help in data collection, Tracey Sampson for preparation, Barbara Watson, MD and Evaline A. Alessandrini, MD for their careful review of the manuscript.
REFERENCES
1. National, State, and Urban Area Vaccination Coverage Levels Among Children Aged 19 to 35 Months—United States—July 1994 to June 1995. MMWR. 1996;45:508 –513
2. Wood D, Donald-Sherbourne C, Halfon N, et. al. Factors related to immunization status among inner-city Latino and African-American preschoolers. Pediatrics. 1995;96:295–301
3. Newacheck PW. Children’s access to primary care. Differences by race, income, and insurance status. Pediatrics. 1996;97:26 –32
4. Hall CB. The recommended childhood immunization schedule of the United States. Pediatrics. 1995;95:135–137
5. Centers for Disease Control and Prevention. Standards for Pediatric Im-munization Practices. 6th printing. Atlanta, GA: Centers for Disease Control and Prevention; 1994:10
6. Tifft CJ, Ledermann HM. Immunization status of hospitalized preschool age children. Am J Dis Child. 1988;142:719 –720
7. Bell LM, Lopez NI, Pinto-Martin J, Casey R, Gill FM. Potential impact of linking and emergency department and hospital affiliated clinics to immunize preschool age children. Pediatrics. 1994;93:99 –103
8. Fairbrother G, Friedman S, DuMont KA, Lobach KS. Markers for pri-mary care: missed opportunities to immunize and screen for lead and tuberculosis by private physicians serving large numbers of inner-city Medicaid-eligible children. Pediatrics. 1996;97:785–790
9. Goldstein KP, Kviz FJ, Daum RS. Accuracy of immunization histories provided by adults accompanying preschool children to a pediatric emergency department. JAMA. 1993;207:2190 –2194
10. McConnochie KM, Roghmann KJ. Immunization opportunities missed among urban poor children. Pediatrics. 1992;89:1019 –1026
11. Szilagyi PG, Rodewald LE, Humiston SG, et al. Immunization practices of pediatricians and family physicians in the United States. Pediatrics. 1994;94:517–523
12. Kum-Nji P, James D, Herrod HG. Immunization status of hospitalized preschool children: risk factors associated with inadequate immuniza-tion. Pediatrics. 1995;96:434 – 438
DOI: 10.1542/peds.100.2.192
1997;100;192
Pediatrics
Louis M. Bell, Michele Pritchard, Rebecca Anderko and Robert Levenson
Impact
A Program to Immunize Hospitalized Preschool-aged Children: Evaluation and
Services
Updated Information &
http://pediatrics.aappublications.org/content/100/2/192
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/100/2/192#BIBL
This article cites 12 articles, 9 of which you can access for free at:
Subspecialty Collections
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.100.2.192
1997;100;192
Pediatrics
Louis M. Bell, Michele Pritchard, Rebecca Anderko and Robert Levenson
Impact
A Program to Immunize Hospitalized Preschool-aged Children: Evaluation and
http://pediatrics.aappublications.org/content/100/2/192
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.