Early Intervention Improves Behavioral Outcomes for
Preterm Infants: Randomized Controlled Trial
WHAT’S KNOWN ON THIS SUBJECT: Prematurely born children have an increased prevalence of behavioral problems in the long term. Knowledge regarding the effects of early intervention programs is sparse, and more randomized controlled trials are warranted.
WHAT THIS STUDY ADDS: A modified version of the Mother-Infant Transaction Program showed beneficial effects on behavioral outcomes reported by both parents of preterm infants with birth weights of,2000 g at a corrected age of 5 years.
abstract
OBJECTIVES:The aim of this study was to examine the effectiveness of an early intervention program on behavioral outcomes at corrected age of 5 years for children with birth weights (BWs) of,2000 g.
METHODS:A randomized controlled trial of a modified version of the Mother-Infant Transaction Program was performed. Outcomes were measured by the Child Behavior Check List report (parents) and Strengths and Difficulties Questionnaire at 5 years (parents and preschool teachers).
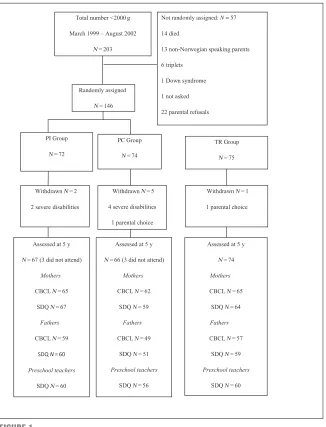
RESULTS:A total of 146 infants were assigned randomly (intervention group: 72 infants; reference group: 74 infants). A term group was re-cruited (75 infants). The mean BWs were 13966429 g for the inter-vention group, 13816436 g for the control group, and 36196490 g for the term reference group. Parents in the intervention group reported significantly fewer behavioral problems measured by both instruments at 5 years. There were no differences in behavior problems reported by preschool teachers. Significantly more children in the preterm control group scored within the clinical area of both instruments.
CONCLUSION:This modified version of the Mother-Infant Transaction Program led to fewer behavioral problems reported by parents at corrected age of 5 years for children with BWs of,2000 g.Pediatrics 2012;129:e9–e16
AUTHORS:S. Marianne Nordhov, MD, PhD,a,b
John A. Rønning, PhD,a,bStein Erik Ulvund, PhD,b,c
Lauritz B. Dahl, MD, PhD,a,band Per Ivar Kaaresen, MD, PhD,a,b
aDepartment of Pediatrics, University Hospital of North Norway Trust, Tromsø, Norway;bInstitute of Clinical Medicine, University of Tromsø, Tromsø, Norway; andcDepartment of Educational Research, University of Oslo, Oslo, Norway
KEY WORDS
preterm infants, early intervention, behavior, randomized controlled trial, Mother-Infant Transaction Program
ABBREVIATIONS
BW—birth weight
CBCL—Child Behavior Check List CI—confidence interval EI—early intervention ES—effect size GA—gestational age LBW—low birth weight
MITP—Mother-Infant Transaction Program
NIDCAP—Newborn Individualized Developmental Care and Assessment Program
OR—odds ratio PC—preterm control PI—preterm intervention
SDQ—Strengths and Difficulties Questionnaire TR—term reference
Dr Nordhov analyzed and interpreted the data, drafted the article, and critically revised it for intellectual content; Dr Rønning substantially contributed to conception, design, and implementation of the study and critically revised the article for interpretation of the data and intellectual content; Dr Ulvund substantially contributed to conception and design of the study and critically revised the article for intellectual content; Dr Dahl substantially contributed to the design and implementation of the study and critically revised the article for the intellectual content; and Dr Kaaresen substantially contributed to the design and performance of the study and critically revised the statistical analyses and the article for intellectual content.
This trial has been registered at www.clinicaltrials.gov (identifier NCT00222456).
www.pediatrics.org/cgi/doi/10.1542/peds.2011-0248
doi:10.1542/peds.2011-0248
Accepted for publication Sep 15, 2011
Address correspondence to Dr Nordhov, Department of Pediatrics, University Hospital of North Norway, N-9038 Tromsø, Norway. E-mail: [email protected] and solveig. [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
incidence of behavior and emotional problems1,2and psychiatric disorders,3 which persist into adolescence and young adulthood.4,5 It is well docu-mented that preterm born children have an increased prevalence of attention problems,1,2but results on the preva-lence of internalizing (eg, withdrawn, anxious/depressed behavior) and exter-nalizing (eg, aggressive and delinquent behavior) problems are less consis-tent.1,2 However, shyness, conduct disorders, unassertiveness, withdrawn behavior, and social skills deficits occur more frequently in LBW children com-pared with normal birth weight (BW) children.3,5,6Among different etiological factors there is increasing evidence that parenting is important and that behav-ior problems in children, at least partly, are mediated by the mother-child re-lationship and the family environment.7 Crucial factors in infant development are parental responsiveness and their ability to respond contingently to their child’s behavior and initiatives.8,9 How-ever, as preterm infants are described to be more fussy, give less eye contact, are easily overaroused, and have less capacity for social interaction,10,11 re-sponsive parenting is often more diffi -cult and challenging. The combination of insecure parenting and a vulnerable preterm infant may forestall a down-ward spiral of negative transactions and thereby contribute to the devel-opment of child behavior problems in the long term.12,13
In an attempt to improve capabilities in LBW infants, early intervention (EI) pro-grams have been developed to improve the parent-infant interaction,14–16 re-duce parenting stress,17and emphasize self-regulation in the infant.18 A review showed that programs focusing on parent-infant interaction are more effec-tive than EI focused only on infant stim-ulation or parent support.19 However,
study by Achenbach et al,21 which revealed that children had significantly fewer behavior problems at 9 years after their mothers had received the Mother-Infant Transaction Program (MITP).21 The theoretical framework for the MITP is the transactional model of development where infant develop-ment is seen as a product of mutual transactions between the child and the environment involving complex feedback systems and with equal em-phasis put on both parts.22
Project “Early Intervention 2000” was designed to test the efficacy of a modi-fied version of the MITP on long-term infant development. We hypothesized that this sensitizing EI program would promote better parenting and thereby optimize long-term child cognitive and behavioral development. We found no significant effects on behavioral out-comes at corrected age of 2 years, but children in the intervention group scored consistently lower on all symp-tom scales compared with controls.23 The main purpose of this report is to evaluate the effects of the MITP on be-havioral and emotional outcomes re-ported by both parents and preschool teachers at corrected age of 5 years.
METHODS
Study Groups and Randomization
Detailed descriptions of participant characteristics, the randomization pro-cess, and the intervention program have been published previously.23,24In sum-mary, preterm infants with BW,2000 g born at the University Hospital of North Norway between March 1999 and Sep-tember 2002, with no major neurologic impairments and whose mothers first language was Norwegian were eligible for this study. Within gestational age (GA) strata of ,28 and $28 weeks, infants were randomly assigned to a preterm intervention (PI) or a preterm
allocated to the same group, and trip-lets were excluded. A group of term infants (GA of $37 weeks and BW
.2800 g) were recruited to a term reference (TR) group. This group was recruited by using the hospital’s birth registry; the parents of thefirst term in-fant born after a preterm inin-fant allocated to the PI group were asked to participate. If they declined, parents of the next born infant were approached and so on. The study was approved by the regional committee for medical ethics and the Norwegian Data Inspectorate.
Intervention
The home visits addressed topics such as adjustment to the home environ-ment, parent-infant interaction through play, discussion of self-regulation, and temper. To maintain the consistency of the intervention, a detailed logbook of every intervention session was regu-larly reviewed and supervised by the by the coordinating nurse and a clinical child psychologist. The participants in the PI group did not have access to the intervention nurses outside the sched-uled intervention dates. The PC group followed the department’s standard protocol for discharge of preterm in-fants (discharge consultation for the infant and their parent with a medical doctor, offer of training in infant mas-sage by a physiotherapist, and visual/ hearing screening), and the TR group was examined routinely on the third day of life only. For the purpose of the study, all participants received the same med-ical, developmental, and psycho-social assessments (corrected ages of 6, 12, 24, 36, and 60 months) with referrals to other services if needed. All assessors were blinded to the children’s group allocation.
Baseline Data
Perinatal variables were collected from medical records. GA was based on ul-trasound examination at 16 to 18 weeks of gestation. The Score of Neonatal Acute Physiology25and the Clinical Risk Index for Babies26were calculated as a measure of the severity of initial illness. Small for GA was defined as BW more than 2 SD below mean for GA. Norwegian BW data were used.27 Intraventricular hemorrhage was graded according to Papile28 and periventricular leukoma-lacia was defined by the presence of echolucencies by cerebral ultrasound. Transient fluid attenuated inversion recovery29 as a sign of white-matter injury was not evaluated. Social vari-ables used in the analyses were col-lected from parents at discharge in a separate questionnaire.
Main Outcomes
The main outcomes for this study were differences in behavioral problems re-ported by parents and preschool teach-ers at corrected age of 5 years.
Outcome Measures
Behavioral outcomes were assessed by the Norwegian translation of the Child Behavior Check List (CBCL)/4-18 (parents)30 and the extended version of the Strengths and Difficulties Ques-tionnaire (SDQ; parents and preschool teachers).31The 2 questionnaires have been described to be equally useful for detecting children in need for psycho-logical support32; however, the SDQ care-taker report is more specific and the CBCL more sensitive in detecting be-havioral problems.33The problem items of the CBCL are scored on a Likert scale from 0 to 2 and yield 9 narrow-banded syndrome scales: withdrawn, somatic complaints, anxious/depressed, delin-quent and aggressive behavior, social, thought, attention, and sex problems. The syndrome scales withdrawn, somatic complaints, and anxious/depressed yields the internalizing broadband syn-drome, whereas aggressive and delin-quent yields the externalizing broadband syndrome. Higher score indicates more problems. Cutoff for borderline and clin-ical ranges on the main scales was scores$82nd and $90th percentiles, and on the subscales$95th and$98th, respectively.30
The extended SDQ consists of a 25-item informant rated questionnaire and an impact supplement. The 25 items generate 5 subscales: emotional symptoms, con-duct problems, hyperactivity-inattention, peer problems, and prosocial behav-ior; all but the last one is summed to a total difficulties score.31Scores$90th percentile were considered to be in the clinical range.34Thefirst question (per-ceived difficulties) of the impact sup-plement asks if the respondent thinks the child has a problem in 1 or more of
the following areas: emotions, concen-tration, behavior, or being able to get along with others. Perceived difficulties were dichotomized into low (0–1) and high (2–3).31The scores in the TR group were used to derive cutoffs for both the CBCL and SDQ.
Power Calculations
The study size was originally calculated to detect a difference in Bayley Scales of Infant Development II, Mental Develop-mental Index at corrected age of 2 years of ∼0.5 SD (a = .05; b = .80). This analysis indicated that 63 infants were needed in each preterm group. To allow for withdrawals, the target size was 70 infants in each group.
Statistical Analyses
Differences in continuous variables be-tween the preterm groups were tested by using linear mixed models, which make it possible to account for the potential clustering effects by including twin pairs when family is included as a random effect. Differences in contin-uous variables are given as mean dif-ferences with 95% confidence intervals (CIs). Binary outcomes were analyzed through logistic regression, with robust SEs and differences given as odds ratios (ORs) with 95% CIs. Cohen’sdwas used as an estimate of effect sizes (ESs) and is the ratio between the mean differ-ence and the pooled SDs for the sam-ple. An ES of 0.20 was considered small; 0.50, moderate; and 0.80, large.35 P values of,.05 were considered sig-nificant. All tests were 2-sided. All results are reported on the basis of intention to treat. Stata 10 (Stata Corp, College Station, TX) was used for the analyses.
RESULTS
A total of 203 infants with BWs of,2000 g were born during the study period. One hundred sixty-eight infants fulfilled the inclusion criteria, and 146 infants
line characteristics were similar in the preterm groups except a slight differ-ence in maternal education (Table 1). In the TR group, 75 infants were recruited. At corrected age of 5 years, 133 (91%) children were assessed. Parents not in-cluded in the analyses due to incomplete questionnaires had shorter education and lower income compared with those completing the questionnaires (data not shown), but there were no differences in GA and BW. All mothers in the PI group participated in every intervention
terquartile range: 4–9 sessions).
OUTCOMES
CBCL scores reported by mothers at 5 years are presented in Table 2. The results remained essentially unchanged after adjusting for maternal education and other potential confounders such as GA, BW, number of siblings, and maternal age. The ESs were small to moderate, and the largest ES of 0.56 was found on the subscale attention. Thirty (48%) of
problems compared with 19 (29%) in the PI group (OR: 0.44 [95% CI: 0.21–0.92];P= .03). On the subscale attention, children in the PI group were less likely to have scores$95th percentile (cutoff 5.0) (OR: 0.25 [95% CI: 0.08–0.81];P= .02). Fathers in the PI group reported significant lower scores on attention and aggres-sive behaviors (Table 3).
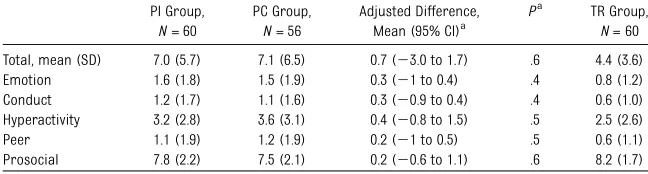
SDQ scores reported by both parents are presented in Table 4. There were significant differences in favor of the PI group on total problems, and the sub-scale hyperactivity reported by both parents. Additionally, fathers in the PI group reported significantly fewer con-duct problems compared with controls. Mothers of 20 (34%) children in the PC group scored$90th percentile (cutoff 10.0) on total problems compared with 14 (21%) of the mothers in the PI group (OR: 0.50 [95% CI: 0.22–1.12];P = .09). Significantly fewer mothers in the PI group reported SDQ scores within the clinical range (cutoff 5.0) on the hyper-activity subscale (OR: 0.39 [95% CI: 0.18– 0.85];P= .02) compared with controls. There were no significant differences between the 2 preterm groups in be-havior problems reported by preschool teachers (Table 5). Ten (17%) mothers in the PC group reported high perceived difficulties scores compared with 4 (6%) in the PI group (OR: 0.32 [95% CI: 0.09– 1.07];P= .06). Similarly, 6 (12%) fathers in the PC group compared with 1 (2%) in the PI group reported high perceived difficulties (OR: 0.13 [95% CI: 0.15–1.12]; P= .06). Preschool teachers reported high perceived difficulties scores in 12 (22%) children in the PC group com-pared with 10 (17%) in the PI group (OR: 0.73 [95% CI: 0.28–1.9];P= .51).
DISCUSSION
In this study, we documented that par-ents who received this modified version of the MITP reported significantly
fewer behavior problems at 5 years compared with parents in the PC group and there was reported lower perceived difficulties in the PI group. This might
be important as both a high per-ceived difficulty score and CBCL scores predict the risk of later psychiatric illness.31,36
To our knowledge, the only interven-tion study that has shown beneficial effects on parent-reported behavioral outcomes in the long term (9 years) is the Vermont study.37The authors sug-gested that the intervention facilitated infant development indirectly through more favorable mother–infant trans-action patterns, the“sleeper effect” (when transactions cause change over time)38 or both.21 However, there are several limitations of this study such as few rather mature infants born in the presurfactant era and before antenatal steroids were widely used. Among other studies, Westrup et al39found a positive impact on behavior 5.5 years after Newborn Individualized Developmental Care and Assessment Program (NID-CAP) care, and Newnham et al40found higher scores in the“communication” dimension of Ages and Stages41after a modified version of the MITP. In a study by Spittle et al,16parents reported less externalizing and dysregulation behav-ior at 2 years corrected age after receiving an educating intervention program (Victorian Infant Brain Studies Plus). Other studies have revealed ben-eficial effects of EI in the preschool age,19,42but at 5 years the effects were not sustained.43,44The investigators have suggested that the programs might have been more effective if they were intro-duced before discharge43or targeted heavier LBW infants.45
The main goals of EI programs are to enhance parent-infant interactions and thus stimulate the wiring process of the neurons in the immature brain in a beneficial way.46 Thefirst study to doc-ument that interventions could alter brain structure and function was repor-ted by Als et al.47They followed up 30 low-risk preterm infants who received NIDCAP and found better neurobehavioral scores, more mature white matter at corrected age of 2 weeks, and behav-ioral advantages at the corrected age of 9 months.47Milgrom et al48demonstrated
TABLE 1 Perinatal and Social Data
PI Group, N= 72
PC Group, N= 74
TR Group, N= 75
Infant characteristics
BW, mean6SD, g 13966429 13816436 36196490 400–1000 g,n(%) 20 (28) 20 (27)
1001–1500 g,n(%) 15 (21) 20 (27) 1501–2000 g,n(%) 37 (51) 34 (46)
GA, mean6SD, wk 30.263.1 29.963.5 39.361.3 ,28 wk,n(%) 17 (24) 19 (27)
28–32 wk,n(%) 36 (50) 37 (50) $33 wk,n(%) 19 (26) 18 (24)
Boy,n(%) 38 (53) 39 (53) 40 (54)
Twin,n(%) 16 (22) 14 (19) 0
Prenatal steroid use,n(%) 53 (74) 57 (77) SNAP II, mean6SD 8.3610.9 10.4611.3 CRIB score, mean6SD,N= 85 3.262.8 2.762.9 Received ventilation,n(%) 29 (40) 37 (50) Duration of ventilation, mean6SD, d,N= 62 7.0618.6 7.1617.3 Postnatal steroid use,n(%) 9 (13) 10 (14) Oxygen therapy at 36 wk of gestation,n(%) 11 (15) 14 (19) Abnormal cerebral ultrasound,n(%)
IVH grade 1 or 2 7 (10) 8 (11) IVH grade 3 or 4 3 (4) 5 (7) Periventricular leukomalacia 4 (6) 8 (11) Maternal and social characteristics
Mother’s age, mean6SD, y 30.866.1 29.166.4 29.766.1 Firstborn child,n(%) 40 (56) 37 (54) 27 (37) Mother’s education, mean6SD, y,N= 131a,b 14.662.8 13.563.2 14.962.8
Father’s education, mean6SD, y,N= 131a 13.863.1 13.563.2 14.463.2
Mother’s monthly income, mean6SD, 1000 Norwegian kroner,N= 131a
15.867.7 14.666.7 15.968.0
Father’s monthly income, mean6SD, 1000 Norwegian kroner,N= 131a
21.168.7 19.968.1 21.969.8
CRIB, Clinical Risk Index for Babies (includes BW, GA, congenital malformations, maximum base deficit in thefirst 12 hours, minimal appropriate fraction of inspired oxygen in thefirst 12 hours, and maximal appropriate fraction of inspired oxygen in thefirst 12 hours); IVH, intraventricular hemorrhage; SNAP II, Score of Neonatal Acute Physiology II (includes mean blood pressure, lowest temperature, PO2/fraction of inspired oxygen ratio, serum pH, multiple seizures, and urine output). aCalculated for 131 families due to 15 twin pairs.
bMean difference: 1.1 years (95% CI: 0.03–2.2 years);P= .04.
TABLE 2 Behavioral Outcomes (CBCL) Reported by Mothers at Corrected Age of 5 Years
PI Group,
N= 65
PC Group,
N= 62
Adjusted Difference, Mean (95% CI)a
Pa d TR Group,
N= 65
Total, mean (SD) 16.7 (12.0) 22.8 (17) 26.1 (211.3 to20.8) .02 0.42 13.5 (8.9) Internalizing 3.6 (3.5) 4.6 (4.4) 21.1 (22.6 to 0.3) .1 0.28 2.8 (3.2) Externalizing 5.8 (5.0) 8.0 (6.7) 22.0 (24.1 to 0.1) .06 0.34 5.1 (3.8) Withdrawn 0.9 (1.0) 1.5 (1.7) 20.6 (21.2 to20.02) .04 0.45 0.8 (1.0) Social 1.1 (1.5) 1.8 (2.2) 20.7 (21.4 to20.2) .04 0.38 0.7 (1.2) Thought 0.2 (0.6) 0.6 (1.4) 20.5 (20.9 to20.08) .02 0.50 0.08 (0.3) Attention 1.7 (2.0) 3.2 (3.4) 21.5 (22.5 to20.5) .003 0.56 1.3 (1.5) Aggressive 4.8 (4.1) 6.8 (6) 21.8 (23.6 to20.02) .05 0.36 4.2 (3.4) Somatic 1.0 (1.5) 1.0 (1.4) 20.2 (20.8 to 0.3) .4 0.14 1.0 (1.5) Anxious/depressed 1.7 (2.0) 2.0 (2.2) 20.3 (21.0 to 0.4) .4 0.11 1.1 (1.8) Delinquent 1 (1.2) 1.2 (1.3) 20.2 (20.7 to 0.2) .4 0.16 0.9 (1.0) Sexual problems 0.2 (0.6) 0.3 (0.7) 20.02 (20.3 to 0.3) .8 0.03 0.2 (0.5)
aAdjusted for clustering effect of twin pairs.
that preterm infants in an intervention group had better maturation and con-nectivity of the white matter at 40 weeks postmenstrual age compared with controls after the parents had re-ceived a modified version of the MITP. Such changes in the white matter have been shown to predict more favorable neurodevelopmental
outcomes in the long term.49 One suggested cause of white matter in-jury is alterations of the hypothalamic-pituitary-adrenal axis50due to chronic stress.51As both NIDCAP and the MITP aim to reduce chronic stress and opti-mize the interaction between the care-giver and the preterm infant, this may at least partly explain the beneficial
We speculate that the MITP sensitize parents to the infants cues, which leads to more adjusted and dynamic parent-infant interactions, and thereby en-hanced infant development according to the transactional model of develop-ment.22 Furthermore, we suggest that the increasing intervention effect over time might be consequence of the“the Matthew effect,”52 in which small dif-ferences in early development amplify through positive feedback mechanisms into larger differences across time.
We found no differences between the preterm groups in behavioral problems reported by preschool teachers. Reports from different informants are important and may contribute to get a better pic-ture of behavior problems in children.31 However, a meta-analysis33revealed that the correlations between different infor-mants are low due to the fact that chil-dren behave differently in different situations, the informants perceive behavior differently, or the informant is influenced by the relationship with the child. Another possible explanation of our findings is parental bias due to lack of blinding for the intervention. Further-more, our results are in line with a study with similar aims and methods where child behavior was evaluated with a neuropsychological test battery.39
Few EI studies have actively involved fathers, and to our knowledge this is thefirst study to report father-reported behavioral outcomes in preterm children. Unfortunately, an attrition of fathers in the intervention group may have infl u-enced the results. An interestingfinding, however, was that fathers scored their children consistently lower in all sub-groups regardless of group affiliation. This may illustrate that fathers perceive behavior based on a cultural or societal context and not prematurity per se.
Major strengths of this study are that it is a population-based randomized
N= 59 N= 49 Mean (95% CI)a N= 57
Total, mean (SD) 13.0 (9.0) 17.6 (16.3) 24.7 (29.6 to 0.3) .07 0.38 10.7 (10.6) Internalizing 2.8 (2.6) 3.0 (3.2) 20.3 (21.4 to 0.8) .6 0.10 2 (3.0) Externalizing 4.4 (3.5) 6.4 (7.3) 21.9 (24.0 to 0.2) .08 0.36 4.0 (4.2) Withdrawn 0.8 (1.0) 1.2 (1.5) 20.3 (20.8 to 0.2) .2 0.24 0.5 (1.0) Social 1.2 (1.4) 1.6 (2.2) 20.4 (21.1 to 0.3) .3 0.23 0.6 (1.5) Thought 0.1 (0.5) 0.4 (0.8) 20.3 (20.5 to 0) .06 0.47 0.1 (0.2) Attention 1.7 (2.2) 3.0 (3.3) 21.2 (22.2 to20.1) .04 0.44 1.4 (2.0) Aggressive 3.5 (0.6) 5.3 (0.7) 21.7 (23.4 to20.04) .04 0.64 3.3 (3.6) Somatic 0.7 (1.1) 0.7 (1.3) 0.001 (20.5 to 0.5) .9 0.01 0.7 (1.3) Anxious/depressed 1.3 (1.4) 1.2 (1.7) 20.03 (20.6 to 0.6) .9 0.02 0.9 (1.5) Delinquent 0.8 (1.1) 1.1 (1.9) 20.2 (20.7 to 0.4) .6 0.14 0.8 (1.0) Sexual problems 0.2 (0.6) 0.3 (0.7) 20.16 (20.4 to 0.1) .2 0.26 0.1 (0.6)
aAdjusted for clustering effect of twin pairs.
TABLE 4 Behavioral Outcomes (SDQ) Reported by Mothers and Fathers at Corrected Age of 5 Years
PI Group PC Group Adjusted Difference, Mean (95% CI)a
Pa d TR Group
Mothers N= 67 N= 59 N =64
Total, mean (SD) 6.7 (5.3) 9.0 (5.5) 2.1 (0.1 to 4.1) .04 0.43 4.9 (3.3) Emotion 1.8 (3.1) 2.0 (1.9) 0.2 (20.7 to 1.2) .6 0.08 1.0 (1.4) Conduct 1.1 (1.5) 1.5 (1.1) 0.3 (20.2 to 0.8) .2 0.30 0.7 (0.9) Hyperactivity 2.8 (2.2) 4.1 (2.8) 1.3 (0.4 to 2.1) .01 0.52 2.5 (1.9) Peer 1.0 (1.6) 1.5 (1.8) 0.5 (20.1 to 1.1) .1 0.30 0.6 (1.0) Prosocial 7.9 (2.1) 7.6 (2.1) 0.1 (20.9 to 0.7) .8 0.14 8.2 (1.4)
Fathers N= 60 N= 51 N= 59
Total, mean (SD) 6.1 (3.6) 8.0 (5.1) 1.6 (20.03 to 3.3) .05 0.44 4.9 (3.7) Emotion 1.5 (1.4) 1.6 (1.6) 0.1 (20.5 to 0.7) .7 0.07 0.7 (1.1) Conduct 0.8 (0.9) 1.4 (1.5) 0.5 (0.0 to 0.9) .04 0.52 0.8 (0.8) Hyperactivity 2.7 (2.0) 3.8 (2.4) 0.9 (0.1 to1.8) .03 0.51 2.4 (1.8) Peer 1.2 (1.4) 1.4 (1.7) 0.2 (20.4 to 0.7) .6 0.13 1.0 (1.5) Prosocial 7.9 (1.7) 7.5 (2.0) 0.2 (20.9 to 0.5) .5 0.22 8.0 (1.6)
aAdjusted for clustering effect of twin pairs.
TABLE 5 Behavioral Outcomes (SDQ) Reported by Preschool Teachers at Corrected Age of 5 Years
PI Group,
N =60
PC Group,
N =56
Adjusted Difference, Mean (95% CI)a
Pa TR Group,
N= 60
Total, mean (SD) 7.0 (5.7) 7.1 (6.5) 0.7 (23.0 to 1.7) .6 4.4 (3.6) Emotion 1.6 (1.8) 1.5 (1.9) 0.3 (21 to 0.4) .4 0.8 (1.2) Conduct 1.2 (1.7) 1.1 (1.6) 0.3 (20.9 to 0.4) .4 0.6 (1.0) Hyperactivity 3.2 (2.8) 3.6 (3.1) 0.4 (20.8 to 1.5) .5 2.5 (2.6) Peer 1.1 (1.9) 1.2 (1.9) 0.2 (21 to 0.5) .5 0.6 (1.1) Prosocial 7.8 (2.2) 7.5 (2.1) 0.2 (20.6 to 1.1) .6 8.2 (1.7)
clinical trial with a high overall follow-up rate at 5 years. Additional strengths are the multi-informant approach and the use of 2 different questionnaires. One limitation is the use of BW rather than GA as the inclusion criterion, which led to the inclusion of more mature small for GA infants. However, they were evenly distributed between the groups and should not bias the group difference. Another limitation is possible parental bias due to the lack of blinding. We do not exactly know if the positive effects in the PI group were due to the EI or the inter-action with the intervention nurses per
se. To clarify this, a randomized clinical trial with a dummy-treated control group must be performed.
CONCLUSIONS
This EI demonstrated a reduction of parent-reported behavioral problems in LBW infants. The largest effects were seen in the attention and aggressive subscales, which is important as these are among the most prevalent behavior problems in preterm born children.1The increasing intervention effect during the study period underlines the
impor-tance of long-term follow-up when eval-uating the effectiveness of EI programs.
ACKNOWLEDGMENTS
This study was funded by grants from the Norwegian Research Council, The Norwegian Council for Mental Health, the Norwegian Foundation for Health and Rehabilitation, and the Northern Regional Health Authority. We thank the families and infants for participat-ing in this study. In addition, we thank the neonatal nurses who implemented the intervention program and the study coordinating nurse, Mrs J. Tunby.
REFERENCES
1. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJ. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis.JAMA. 2002; 288(6):728–737
2. Aarnoudse-Moens CS, Weisglas-Kuperus N, van Goudoever JB, Oosterlaan J. Meta-analysis of neurobehavioral outcomes in very preterm and/or very low birth weight children.Pediatrics. 2009;124(2):717–728
3. Elgen I, Sommerfelt K, Markestad T. Pop-ulation based, controlled study of behav-ioural problems and psychiatric disorders in low birthweight children at 11 years of age.Arch Dis Child Fetal Neonatal Ed. 2002; 87(2):F128–F132
4. Lund LK, Vik T, Skranes J, Brubakk AM, Indredavik MS. Psychiatric morbidity in two low birth weight groups assessed by di-agnostic interview in young adulthood.
Acta Paediatr. 2011;100(4):598–604
5. Hack M, Taylor HG, Schluchter M, Andreias L, Drotar D, Klein N. Behavioral outcomes of extremely low birth weight children at age 8 years. J Dev Behav Pediatr. 2009;30(2): 122–130
6. Sommerfelt K, Troland K, Ellertsen B, Markestad T. Behavioral problems in low-birthweight preschoolers. Dev Med Child Neurol. 1996;38(10):927–940
7. Forcada-Guex M, Pierrehumbert B, Borghini A, Moessinger A, Muller-Nix C. Early dyadic patterns of mother-infant interactions and outcomes of prematurity at 18 months.
Pediatrics. 2006;118(1). Available at: www. pediatrics.org/cgi/content/full/118/1/e107
8. Zelkowitz P, Na S, Wang T, Bardin C, Papageorgiou A. Early maternal anxiety
pre-dicts cognitive and behavioural outcomes of VLBW children at 24 months corrected age.
Acta Paediatr. 2011;100(5):700–704
9. Wijnroks L. Mother-infant interaction and contingency learning in pre-term infants.
Early Dev Parent. 1997;6(1):27–36
10. Beckwith L. Evaluating Effects of Inter-vention With Parents of Preterm Infants. Norwood, NJ: Ablex; 1992
11. Eckerman CO, Hsu HC, Molitor A, Leung EH, Goldstein RF. Infant arousal in an en-face exchange with a new partner: effects of
prematurity and perinatal biological risk.
Dev Psychol. 1999;35(1):282–293
12. Field TM. Affective displays of high-risk infants during early interactions. In: Field TM, Fogel A, eds.Emotion and Early Inter-action. Hillsdale, NJ: Erlbaum; 1982:102–125
13. Sameroff AJ, Mackenzie MJ. Research strat-egies for capturing transactional models of development: the limits of the possible.Dev Psychopathol. 2003;15(3):613–640
14. Rauh VA, Nurcombe B, Achenbach T, Howell C.
The Mother-Infant Transaction Program: the content and implications of an intervention for the mothers of low-birthweight infants.
Clin Perinatol. 1990;17(1):31–45
15. Johnson S, Whitelaw A, Glazebrook C, et al.
Randomized trial of a parenting intervention
for very preterm infants: outcome at 2 years.
J Pediatr. 2009;155(4):488–494
16. Spittle AJ, Anderson PJ, Lee KJ, et al. Preventive care at home for very preterm infants improves infant and caregiver out-comes at 2 years. Pediatrics. 2010;126(1). Available at: www.pediatrics.org/cgi/content/ full/126/1/e171
17. Melnyk BM, Alpert-Gillis LJ. The COPE pro-gram: a strategy to improve outcomes of critically ill young children and their parents.Pediatr Nurs. 1998;24(6):521–527
18. Als H, Butler S, Kosta S, McAnulty G. The Assessment of Preterm Infants’ Behavior (APIB): furthering the understanding and measurement of neurodevelopmental com-petence in preterm and full-term infants.
Ment Retard Dev Disabil Res Rev. 2005;11(1): 94–102
19. Spittle AJ, Orton J, Doyle LW, Boyd R. Early developmental intervention programs post hospital discharge to prevent motor and cognitive impairments in preterm infants.
Cochrane Database Syst Rev. 2007; (2): CD005495
20. Vanderveen JA, Bassler D, Robertson CM, Kirpalani H. Early interventions involving parents to improve neurodevelopmental out-comes of premature infants: a meta-analysis.
J Perinatol. 2009;29(5):343–351
21. Achenbach TM, Howell CT, Aoki MF, Rauh VA. Nine-year outcome of the Vermont interven-tion program for low birth weight infants.
Pediatrics. 1993;91(1):45–55
23. Kaaresen PI, Rønning JA, Tunby J, Nordhov SM, Ulvund SE, Dahl LB. A randomized controlled trial of an early intervention program in low birth weight children: out-come at 2 years.Early Hum Dev. 2008;84(3): 201–209
24. Nordhov SM, Rønning JA, Dahl LB, Ulvund SE, Tunby J, Kaaresen PI. Early intervention im-proves cognitive outcomes for preterm in-fants: randomized controlled trial.Pediatrics. 2010;126(5). Available at: www.pediatrics.org/ cgi/content/full/126/5/e1088
25. Richardson DK, Corcoran JD, Escobar GJ, Lee SK. SNAP-II and SNAPPE-II: simplified newborn illness severity and mortality risk scores.J Pediatr. 2001;138(1):92–100
26. The International Neonatal Network. The CRIB (clinical risk index for babies) score: a tool for assessing initial neonatal risk and comparing performance of neonatal intensive care units.Lancet. 1993;342(8865): 193–198
27. Skjaerven R, Gjessing HK, Bakketeig LS. Birthweight by gestational age in Norway.
Acta Obstet Gynecol Scand. 2000;79(6):440– 449
28. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm.J Pediatr. 1978;92(4):529–534 29. Iwata S, Iwata O, Bainbridge A, et al.
Ab-normal white matter appearance on term FLAIR predicts neuro-developmental out-come at 6 years old following preterm birth.
Int J Dev Neurosci. 2007;25(8):523–530
30. Achenbach TM. Manual for the Child
Behavior Checklist/4-18 & 1991 Profile. Burlington, VT: University of Vermont De-partment of Psychiatry; 1991
31. Goodman R. The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. J Child Psychol Psy-chiatry. 1999;40(5):791–799
32. Goodman R, Scott S. Comparing the Strengths and Difficulties Questionnaire and the Child
33. Warnick EM, Bracken MB, Kasl S. Screening efficiency of the Child Behavior Checklist and Strengths and Difficulties Question-naire: a systematic review. Child Adolesc Ment Health. 2008;13(3):140–147
34. Smedje H, Broman JE, Hetta J, von Knorring AL. Psychometric properties of a Swedish version of the“Strengths and Difficulties Questionnaire”. Eur Child Adolesc Psychia-try. 1999;8(2):63–70
35. Cohen J.Statistical Power Analysis for the Behavioral Sciences, 2nd ed. Hillsdale, NJ: Lawrence Erlbaum; 1988
36. Kroes M, Kalff AC, Steyaert J, et al. A longitudinal community study: do psycho-social risk factors and child behavior checklist scores at 5 years of age predict psychiatric diagnoses at a later age?J Am Acad Child Adolesc Psychiatry. 2002;41(8): 955–963
37. Achenbach TM, Phares V, Howell CT, Rauh VA, Nurcombe B. Seven-year outcome of the Vermont Intervention Program for Low-Birthweight Infants. Child Dev. 1990;61(6): 1672–1681
38. Kumkale GT, Albarracín D. The sleeper ef-fect in persuasion: a meta-analytic review.
Psychol Bull. 2004;130(1):143–172
39. Westrup B, Böhm B, Lagercrantz H, Stjernqvist K. Preschool outcome in children born very prematurely and cared for according to the Newborn Individualized Developmental Care and Assessment Program (NIDCAP). Acta Paediatr. 2004;93(4):498–507
40. Newnham CA, Milgrom J, Skouteris H. Ef-fectiveness of a modified Mother-Infant Transaction Program on outcomes for pre-term infants from 3 to 24 months of age.
Infant Behav Dev. 2009;32(1):17–26 41. Bricker DSJ, Squires J, Mounts L.Ages and
Stages Questionnaires: A Parent- Com-pleted Child-Monitoring System, 2nd ed. Baltimore, MD: Paul H. Brookes; 1999
42. Kleberg A, Westrup B, Stjernqvist K. De-velopmental outcome, child behaviour and mother-child interaction at 3 years of age fol-lowing Newborn Individualized Developmental
123–135
43. Johnson S, Ring W, Anderson P, Marlow N. Randomised trial of parental support for families with very preterm children: out-come at 5 years.Arch Dis Child. 2005;90(9): 909–915
44. Brooks-Gunn J, McCarton CM, Casey PH, et al. Early intervention in low-birth-weight premature infants: results through age 5 years from the Infant Health and Devel-opment Program.JAMA. 1994;272(16):1257– 1262
45. McCarton CM, Brooks-Gunn J, Wallace IF, et al. Results at age 8 years of early in-tervention for low-birth-weight premature infants: The Infant Health and Development Program.JAMA. 1997;277(2):126–132
46. Westrup B. Newborn Individualized Devel-opmental Care and Assessment Program (NIDCAP): family-centered developmentally supportive care.Early Hum Dev. 2007;83(7): 443–449
47. Als H, Duffy FH, McAnulty GB, et al. Early experience alters brain function and struc-ture.Pediatrics. 2004;113(4):846–857
48. Milgrom J, Newnham C, Anderson PJ, et al. Early sensitivity training for parents of preterm infants: impact on the developing brain.Pediatr Res. 2010;67(3):330–335
49. Krishnan ML, Dyet LE, Boardman JP, et al. Relationship between white matter appar-ent diffusion coefficients in preterm infants at term-equivalent age and developmental outcome at 2 years.Pediatrics. 2007;120(3). Available at: www.pediatrics.org/cgi/content/ full/120/3/e604
50. Kapoor A, Dunn E, Kostaki A, Andrews MH,
Matthews SG. Fetal programming of
hypothalamo-pituitary-adrenal function: pre-natal stress and glucocorticoids.J Physiol. 2006;572(Pt 1):31–44
51. Rangon CM, Fortes S, Lelièvre V, et al. Chronic mild stress during gestation wor-sens neonatal brain lesions in mice.J Neu-rosci. 2007;27(28):7532–7540
DOI: 10.1542/peds.2011-0248 originally published online December 19, 2011;
2012;129;e9
Pediatrics
Ivar Kaaresen
S. Marianne Nordhov, John A. Rønning, Stein Erik Ulvund, Lauritz B. Dahl and Per
Randomized Controlled Trial
Early Intervention Improves Behavioral Outcomes for Preterm Infants:
Services
Updated Information &
http://pediatrics.aappublications.org/content/129/1/e9 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/129/1/e9#BIBL This article cites 46 articles, 10 of which you can access for free at:
Subspecialty Collections
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2011-0248 originally published online December 19, 2011;
2012;129;e9
Pediatrics
Ivar Kaaresen
S. Marianne Nordhov, John A. Rønning, Stein Erik Ulvund, Lauritz B. Dahl and Per
http://pediatrics.aappublications.org/content/129/1/e9
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.