A Clinical Decision Rule to Identify Children at Low Risk
for Appendicitis
Anupam B. Kharbanda, MD*; George A. Taylor, MD‡; Steven J. Fishman, MD§; and Richard G. Bachur, MD*
ABSTRACT. Objective. Computed tomography (CT)
has gained widespread acceptance in the evaluation of children with suspected appendicitis. Concern has been raised regarding the long-term effects of ionizing radia-tion. Other means of diagnosing appendicitis, such as clinical scores, are lacking in children. We sought to develop a clinical decision rule to predict which children with acute abdominal pain do not have appendicitis.
Methods. Prospective cohort study was conducted of children and adolescents who aged 3 to 18 years, had signs and symptoms suspicious for appendicitis, and presented to the emergency department between April 2003 and July 2004. Standardized data-collection forms were completed on eligible patients. Two low-risk clin-ical decision rules were created and validated using lo-gistic regression and recursive partitioning. The sensitiv-ity, negative predictive value (NPV), and negative likelihood ratio of each clinical rule were compared.
Results. A total of 601 patients were enrolled. Using logistic regression, we created a 6-part score that con-sisted of nausea (2 points), history of focal right lower quadrant pain (2 points), migration of pain (1 point), difficulty walking (1 point), rebound tenderness/pain with percussion (2 points), and absolute neutrophil count of>6.75ⴛ103/L (6 points). A score<5 had a sensitivity of 96.3% (95% confidence interval [CI]: 87.5–99.0), NPV of 95.6% (95% CI: 90.8 –99.0), and negative likelihood ratio of .102 (95% CI: 0.026 – 0.405) in the validation set. Using recursive partitioning, a second low-risk decision rule was developed consisting of absolute neutrophil count of
<6.75ⴛ103/L, absence of nausea, and absence of max-imal tenderness in the right lower quadrant. This rule had a sensitivity of 98.1% (95% CI: 90.1–99.9), NPV of 97.5% (95% CI: 86.8 –99.9), and negative likelihood ratio of 0.058 (95% CI: 0.008 – 0.411) in the validation set. The-oretical application of the low-risk rules would have resulted in a 20% reduction in CT.
Conclusions. Our low-risk decision rules can predict accurately which children are at low risk for appendicitis and could be treated safely with careful observation
rather than CT examination.Pediatrics2005;116:709–716;
appendicitis, children, decision rule.
ABBREVIATIONS. CT, computed tomography; ED, emergency department; US, ultrasound, PEM, pediatric emergency medicine; RLQ, right lower quadrant; WBC, white blood cell; ANC, absolute neutrophil count; NPV, negative predictive value; LR, likelihood ratio; CI, confidence interval.
A
ppendicitis is the most common surgical emergency in children, with⬎70 000 pediat-ric appendectomies performed annually in the United States.1,2The diagnosis of appendicitis in children remains challenging because of the overlap-ping symptoms of many childhood illnesses and the preverbal state of young children.3,4Delayed diagnosis of appendicitis is associated with increased morbidity, mortality, and health care costs.5–9 Recent advances in computed tomography (CT) have led to modest improvements in the nega-tive appendectomy rate and in the diagnosis of ap-pendicitis.10–14 However, the indiscriminate use of CT carries significant risks as a result of increased exposure to ionizing radiation and may result in increased health care costs.15–17These concerns have led to renewed interest in clinical scores to better diagnose appendicitis.
The “MANTRALS” score was proposed by Al-varado in 1986 as a method to predict appendicitis in adults.18 Subsequent studies to validate the score in adult and pediatric cohorts have had mixed re-sults.19–22 Other clinical scores have been proposed to predict appendicitis in children; however, they have suffered from small sample size or have not been validated.23–25 In this study, we prospectively enrolled children who were under evaluation for appendicitis to develop a clinical rule that is specific to a pediatric population. We sought to develop and validate low-risk criteria to define patients who could be observed or discharged safely without reli-ance on CT.
METHODS Study Setting and Population
This study was conducted at an urban, tertiary-care, pediatric emergency department (ED) that has⬃52 000 visits per year. From April 2003 to July 2004, we prospectively enrolled children who were between 3 and 18 years of age and underwent surgical consultation for possible appendicitis. The hospital’s clinical prac-tice guideline mandates that a surgeon (a fourth-year surgical resident or attending) evaluate all patients who present to the ED
From the *Division of Emergency Medicine and Departments of ‡Radiology and §Surgery, Children’s Hospital Boston, Harvard Medical School, Boston, Massachusetts.
Accepted for publication May 2, 2005. doi:10.1542/peds.2005-0094
No conflict of interest declared.
This study was presented in part at the annual meeting of the Pediatric Academic Societies; May 2, 2004; San Francisco, CA; and the annual meeting of the American Academy of Pediatrics; October 8, 2004; San Francisco, CA. Reprint requests to (A.B.K.) Division of Emergency Medicine, Children’s Hospital Boston, 300 Longwood Ave, Boston, MA 02115. E-mail: [email protected]
with signs and symptoms suspicious for appendicitis before any diagnostic imaging, such CT or ultrasound (US). The decision to obtain a CT, US, or both was left to the joint decision of the surgeon and pediatric emergency medicine (PEM) attending. Commonly, female adolescents would undergo US before any CT evaluation. Patients were excluded when they were pregnant, had undergone previous abdominal surgery, had a chronic medical conditions (eg, cystic fibrosis, inflammatory bowel disease, sickle cell anemia), or had radiologic studies (CT or US) of the abdomen within the previous 2 weeks. Patients who had laboratory studies or plain radiographs before their ED evaluation were not ex-cluded.
Standardized Patient Assessment and Data Collection
Data-collection forms were completed by the PEM attending who was responsible for the patient’s care. Forms were completed before diagnostic imaging and independent of the surgeon’s eval-uation. Physicians were introduced to the data-collection forms during a 1-hour session before the beginning of the study. The standardized data-collection forms consisted of 24 demographic, historical, and physical examination variables. Historical elements were history of fever, nausea, anorexia, emesis, and diarrhea; number of hours of pain; migration of pain; history of focal right lower quadrant (RLQ) pain; pain onset; pain quality; and ability to walk. Physical examination variables were location of abdom-inal tenderness and point of maximal tenderness; presence of tenderness with percussion/cough/hopping; rebound tenderness; guarding; rectal tenderness; bowel sounds; costovertebral angle tenderness; and psoas, obturator, or Rovsing’s sign. For patients who underwent a pelvic examination, presence of adnexal pain and/or cervical motion tenderness was recorded.
The patient’s medical record was abstracted by one author (A.B.K.) for laboratory (white blood cell [WBC] count, percentage of neutrophils, and absolute neutrophil count [ANC]), radiology, pathology, and operative reports. Data were entered into a secure data management program by a single, supervised research assis-tant. All entered data were double-checked for accuracy. To de-termine our capture rate, we reviewed the ED electronic charting system, the ED admission log, and the pathology database.
Outcome Measures
Our main outcome was the presence or absence of appendicitis. Final diagnosis was determined by pathology for patients who had an appendectomy. A perforated appendix was determined by the attending surgeon’s written postoperative diagnosis. For pa-tients who did not have surgery, the outcome was confirmed by a follow-up telephone call 2 to 4 weeks after the ED visit. When the family could not be reached, the patient’s pediatrician was con-tacted to determine the final diagnosis.
Consent
This study was approved by the hospital’s committee on clin-ical investigations. Informed consent was obtained from all par-ticipating PEM physicians. Informed consent was also obtained from all parents, and assent was obtained from children who were older than 7 years.
Data Analysis: Derivation of Clinical Decision Rule
We performed2testing for categorical variables to identify
potential predictors for appendicitis (SPSS 11.5; SPSS Inc, Chicago, IL). Threshold values (cutoffs) for continuous variables (WBC count and ANC) were obtained from univariate recursive parti-tioning analyses. Variables that were highly associated with ap-pendicitis (P⬍.001) were analyzed by 2 separate statistical meth-ods, logistic regression and recursive partitioning, to create a clinical decision rule (see below). Patients who were enrolled from April 2003 through February 2004 were included in the derivation set.
Logistic Regression
Variables that were highly associated with appendicitis (P⬍
.001 on2testing) and had⬍10% missing data were selected for
model creation. Selected predictors were entered in a logistic-regression model using backward stepwise elimination. To de-velop the clinical score, thecoefficients for the retained
predic-tors were converted into integer values by dividing by the lowest value and rounding any decimals. The score that maximized the negative likelihood ratio and negative predictive value (NPV) was chosen as the low-risk score cutoff.
Recursive Partitioning
We used recursive partitioning (CART 5.0; Salford Systems, San Diego, CA) software to create decision trees. Variables that were highly associated with appendicitis (P⬍.001 on2testing) were
entered into the model. The Gini method for classification trees and 10-fold cross-validation was used. Misclassifying a patient with appendicitis as low risk was weighted to be 20 times worse than misclassifying a patient without appendicitis as non–low risk.
Validation of Clinical Decision Rules and Score Performance
The validation set was composed of patients who were enrolled consecutively from March 2004 to July 2004. The clinical decision rules that were derived from logistic regression and recursive partitioning were applied to the validation set. Sensitivity, speci-ficity, and negative likelihood ratio of the clinical scores were determined.
RESULTS Study Population
During the 15-month study period, 4140 patients who were between 3 and 18 years of age presented to the ED with a chief complaint of abdominal pain. Of these, 767 (19%) underwent surgical consultation to evaluate for possible appendicitis. A total of 113 patients met criteria for exclusion, leaving 654 pa-tients eligible for enrollment. Fifty-three papa-tients were missed or not approached to participate, and 601 patients were enrolled (425 in the derivation set and 176 in the validation set), for a capture rate of 92%.
The median age was 11.6 years (interquartile range: 8.2–14.6). A total of 307 (51%) patients were male. A total of 211 (35%) patients received a diag-nosis of appendicitis. Thirty-eight (22%) of the 211 patients with appendicitis had a perforated appen-dix. Follow-up was completed on 593 (99%) patients. No patient who was discharged presented to another hospital for an appendectomy. The derivation and validation groups did not differ significantly by age, gender, or proportion with appendicitis or perfo-rated appendicitis (Table 1). The clinical characteris-tics of the patients enrolled are detailed in Table 1. The eligible patients who were not enrolled were of a similar age and gender as the enrolled cohort but had a significantly lower rate of appendicitis (13%).
Clinical Course and Disposition
Derivation of Clinical Decision Rule: Univariate Analysis
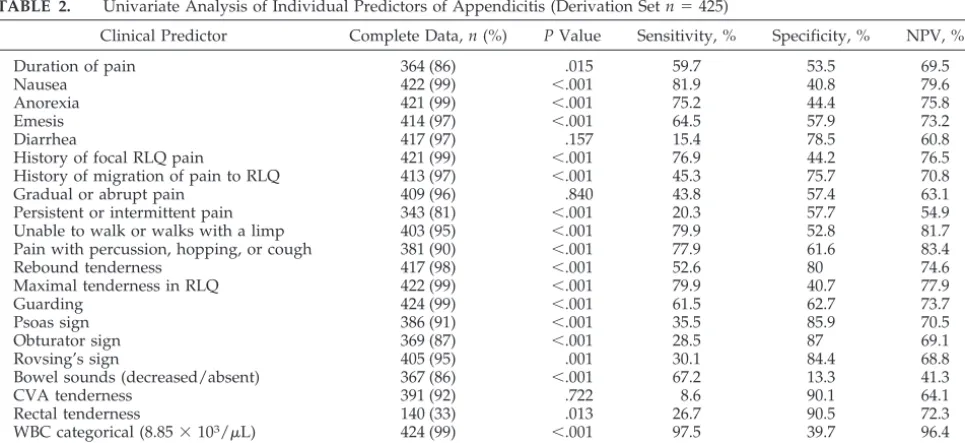
Recursive partitioning analysis determined the ideal cut points for the continuous variables ANC and WBC count to be 6.75 ⫻ 103/L and 8.85 ⫻ 103/L, respectively. These variables were converted to categorical variables on the basis of these cut points. The relationship between each categorical variable and appendicitis was evaluated with 2 analysis (Table 2).
Logistic Regression
Twelve of 24 clinical predictors met criteria for entry into backward step-wise bivariate logistic re-gression. Six predictors were retained from this anal-ysis: (1) nausea, (2) history of focal RLQ pain, (3) migration of pain, (4) difficulty walking, (5) rebound tenderness, and (6) ANC⬎6.75⫻ 103/L (Table 3). Rebound pain and pain with percussion had a high degree of co-linearity and clinical overlap; therefore,
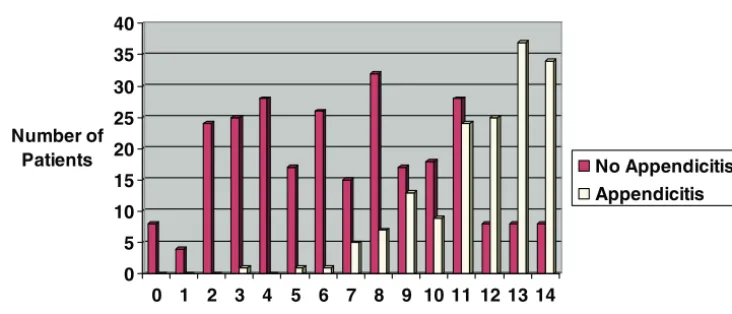
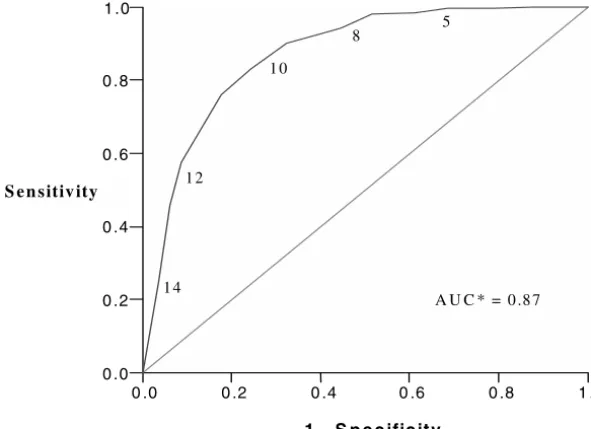
the variables were combined. The diagnostic weights that were applied to each of the 6 predictors are listed in Table 3. The clinical score that was devel-oped using logistic regression was applied to the derivation group of patients. A score ofⱕ5 identified 108 (25%) patients, 106 who did not have appendici-tis and 2 who did (Fig 1). The sensitivity and the NPV for this score cutoff are 98.7% (95% confidence interval [CI]: 95.5–99.9) and 98.1% (95% CI: 93.5– 99.7), respectively. The sensitivity and the specificity are described graphically in a receiver-operator curve (Fig 2). The negative likelihood ratio (LR) for a score ⱕ5 is .032 (95% CI: 0.008 – 0.128).
Validation of Logistic-Regression Model
The clinical score that was created with logistic regression was applied to the 176 patients in the validation set. Table 4 outlines the performance of the score on this validation set. A score ofⱕ5 would identify 46 patients, 44 who did not have
appendici-TABLE 1. Comparison of Clinical Characteristics of Derivation and Validation Groups
Derivation Set Validation Set Overall
Age, y
Median 11.4 12.1 11.6
IQR 8.2–14.4 8.2–14.8 8.2–14.6
Gender,n(%) 228 male (54) 79 male (45) 307 male (51)
History,n(%)
Nausea 285 (68) 106 (61) 391 (66)
Anorexia 264 (63) 104 (60) 368 (62)
Focal RLQ pain 268 (64) 118 (69) 386 (65)
Migration of pain 132 (32) 66 (39) 198 (34)
Inability to walk or walks with limp 239 (59) 83 (51) 322 (57) Physical examination,n(%)
Maximal pain in RLQ 283 (68) 132 (75)* 415 (69)
Abdominal tenderness 410 (97) 173 (99) 583 (98)
Rebound pain 133 (32) 52 (30) 185 (31)
Laboratory,n(%)
ANC⬎6.75⫻103/L 274 (67) 104 (64) 378 (65)
Appendicitis,n(%) 157 (37) 54 (31) 211 (35)
Perforated appendicitis,n(%) 30 (6.6) 8 (4.5) 38 (6.3)
IQR indicates interquartile range. *P⬍.05.
TABLE 2. Univariate Analysis of Individual Predictors of Appendicitis (Derivation Setn⫽425)
Clinical Predictor Complete Data,n(%) PValue Sensitivity, % Specificity, % NPV, %
Duration of pain 364 (86) .015 59.7 53.5 69.5
Nausea 422 (99) ⬍.001 81.9 40.8 79.6
Anorexia 421 (99) ⬍.001 75.2 44.4 75.8
Emesis 414 (97) ⬍.001 64.5 57.9 73.2
Diarrhea 417 (97) .157 15.4 78.5 60.8
History of focal RLQ pain 421 (99) ⬍.001 76.9 44.2 76.5
History of migration of pain to RLQ 413 (97) ⬍.001 45.3 75.7 70.8
Gradual or abrupt pain 409 (96) .840 43.8 57.4 63.1
Persistent or intermittent pain 343 (81) ⬍.001 20.3 57.7 54.9
Unable to walk or walks with a limp 403 (95) ⬍.001 79.9 52.8 81.7 Pain with percussion, hopping, or cough 381 (90) ⬍.001 77.9 61.6 83.4
Rebound tenderness 417 (98) ⬍.001 52.6 80 74.6
Maximal tenderness in RLQ 422 (99) ⬍.001 79.9 40.7 77.9
Guarding 424 (99) ⬍.001 61.5 62.7 73.7
Psoas sign 386 (91) ⬍.001 35.5 85.9 70.5
Obturator sign 369 (87) ⬍.001 28.5 87 69.1
Rovsing’s sign 405 (95) .001 30.1 84.4 68.8
Bowel sounds (decreased/absent) 367 (86) ⬍.001 67.2 13.3 41.3
CVA tenderness 391 (92) .722 8.6 90.1 64.1
Rectal tenderness 140 (33) .013 26.7 90.5 72.3
WBC categorical (8.85⫻103/L) 424 (99) ⬍.001 97.5 39.7 96.4
tis. The sensitivity and the NPV for this score cutoff are 96.3% (95% CI: 87.5–99) and 95.6% (95% CI: 90.8 – 99), respectively. The negative LR is 0.102 (95% CI: 0.026 – 0.405).
Recursive Partitioning
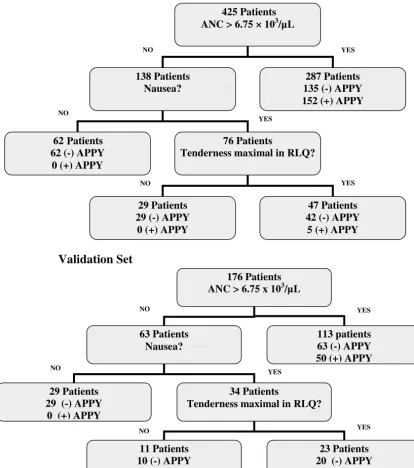
Sixteen variables met criteria for entry into the recursive partitioning model. Recursive partitioning analysis created a tree that used ANC⬎6.75⫻ 103/ L, nausea, and maximal tenderness in the RLQ. The low-risk decision tree identified 91 (21%) patients, none of whom had appendicitis (Fig 3). Surrogate variables for nausea included the presence of emesis and anorexia. A history of focal RLQ pain was a surrogate for maximal tenderness in the RLQ. In the derivation set, the sensitivity for this low-risk deci-sion rule is 100% (95% CI: 97.7–100) with an NPV of 100% (95% CI: 96.0 –100). The negative LR for the decision tree is 0 (upper 95% CI estimated to be
⬍0.001; Table 4).
Validation of Recursive Partitioning Model
The decision tree that was created by recursive partitioning was applied to the 176 patients in the validation set. The low-risk decision rule identified 40 patients, 1 of whom had appendicitis. This pro-vides a sensitivity of 98.1% (95% CI: 90.1–99.9) and an NPV of 97.5% (95% CI: 86.8 –99.9; Table 4). The negative LR is 0.058 (95% CI: 0.008 – 0.411).
Reduction in CT Utilization and Operative Care We applied to our entire study cohort the clinical decision rules that were created from logistic regres-sion and recursive partitioning to determine which patients theoretically could have avoided CT or op-erative care. Application of the clinical rules such
that low-risk patients were observed rather than im-aged would have reduced the use of CT by 23% for the logistic regression model and 20% for the recur-sive partitioning model. Appendectomies were per-formed in 6 low-risk patients, as classified by both models; all of these low-risk patients had a false-positive CT examination, a normal appendix on pa-thology, and no other indications for surgery.
Patients Who Were Missed by Clinical Decision Rules A total of 4 patients with appendicitis were mis-classified as low risk in our models. Logistic regres-sion missed 2 patients in the derivation set and 2 in the validation set. Recursive portioning missed 0 patients in the derivation set and 1 patient in the validation set. None of these 4 patients was found to have a perforated appendix in the operating room. Table 5 summarizes the clinical characteristics of these 4 patients.
DISCUSSION
We report the largest prospectively designed and validated study to create a decision rule for appen-dicitis in children. We evaluated 601 children with signs and symptoms suggestive of appendicitis. Us-ing logistic regression and recursive partitionUs-ing, we derived and validated 2 clinical decision rules to identify children who were at low risk for appendi-citis. Application of either low-risk rule to patients with signs and symptoms suspicious for appendicitis would lead to decreased reliance on CT. In addition, use of our clinical rules could potentially prevent a small group of patients who are identified as low risk for appendicitis from undergoing an appendectomy. Previous authors have developed clinical scores to predict appendicitis in adults and children. The first
0 5 10 15 20 25 30 35 40
Number of Patients
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Clinical Scores
No Appendicitis Appendicitis
Fig 1. Score performance of logistic-regression model.
TABLE 3. Diagnostic Weights for Variables Retained in Logistic-Regression Analysis
Data Elements  Significance Weight
ANC categorical (⬎6.75⫻103/L) 3.32 ⬍.001 6
Rebound pain or pain with percussion 1.08 ⬍.001 2 Unable to walk or walks with limp .681 .033 1
Nausea .920 .003 2
History of migration of pain to RLQ .505 .117 1
score to gain widespread attention was described by Alvarado. The score components were migration (1 point), anorexia (1 point), nausea (1 point), tender-ness in the RLQ (2 points), rebound pain (1 point), elevated temperature (1 point), leukocytosis (2 points), and neutrophilia (1 point). This score was derived retrospectively in adults and had a reported sensitivity of 75% and specificity of 84%.18 Prospec-tive evaluation of the Alvarado score in children has shown varied results, with sensitivities of 76% to 90% and specificities of 72% to 79%.20,21,26 The Al-varado score’s performance is unacceptably low for current clinical practice.
To address this issue further, investigators have attempted to derive clinical scores for appendicitis in pediatric cohorts. Samuel derived the “Pediatric Ap-pendicitis Score” prospectively over 5 years in 1170 children using logistic regression. Variables that were included in the score were anorexia, nausea/ emesis, migration of pain, tenderness in the RLQ, cough/hopping/percussion tenderness, pyrexia, leukocytosis, and neutrophilia. He reported a sensi-tivity of 100%, specificity of 92%, positive predictive value of 96%, and NPV of 99%.24Unfortunately, the score was not validated. We applied the Samuel score to our cohort and found a significantly lower sensitivity (83%) and NPV (88%). More recently, van den Broek et al25 prospectively derived a clinical score to predict appendicitis in 99 children, also us-ing logistic regression. The score was validated at 2 other clinical centers in the Netherlands. They found a temperature of ⬎38°C, WBC count of ⬎10.10 ⫻
103/L, and rebound tenderness to be correlated with appendicitis. The sensitivity and specificity were 89% and 85%, respectively. The authors con-cluded that pediatric patients who have a leukocyte count of⬍10.10⫻103/L and lack rebound tender-ness could be observed safely.25Although this study contained small numbers of patients and was con-ducted in an era before significant use of CT (1994 – 1995), it revealed that a low-risk group of patients with suspected appendicitis could be identified.
Our clinical decision rules expand on this previous research by defining further a group of children who have significant abdominal pain and do not have appendicitis. Our goal was to identify children who could be observed safely without CT examination. Low-level exposure to ionizing radiation is not with-out risks.27,28For example, Brenner et al17estimated that of the 600 000 children who undergo CT scans each year, 500 will develop cancer as a direct result of their radiation exposure. Given this concern, physi-cians should consider strategies that minimize radi-ation exposure. Use of our clinical decision rules theoretically would have led to a 20% reduction in CT utilization in our cohort. An unanticipated addi-tional benefit of the models was the identification of several patients who were classified as low risk by the models and had false-positive CT scans that led to a negative appendectomy.
Physicians may be reluctant to adopt our low-risk decision rules given previous studies that demon-strated a reduction in negative appendectomy rates and perforation rates associated with the use of
0 .0 0.2 0.4 0 .6 0.8 1 .0
1 - S p ec ificity 0.0
0.2 0.4 0.6 0.8 1.0
A U C * = 0.87
Sensitivity
5 8
10
12
14
Fig 2. Receiver-operator curve for logistic-regression model. Numbers represent clinical score. AUC indicates area under curve.
TABLE 4. Comparison of Performance of Clinical Decision Rules
Clinical Decision Rule Derivation Validation
Sensitivity, % (95% CI)
NPV, % (95% CI)
LR (⫺) (95% CI)
Sensitivity, % (95% CI)
NPV, % (95% CI)
CT.12–14,29–32 However, diagnostic imaging may not be as useful as previously believed. Recently, Par-trick et al33 and Martin et al34 reported in large cohorts that despite increase in CT scan utilization, the negative appendectomy rates and perforation rates remained unchanged. In addition, in 1999, Karakas et al35reported on the utility of CT and US in 633 children with suspected appendicitis. Ironi-cally, in this study, the perforation rate increased substantially among pediatric patients who under-went a CT scan and US before appendectomy. The authors postulated that the delay associated with obtaining these studies before surgery could be re-sponsible for the increased perforation rate.35Finally,
in 2001, Flum et al36 published a population-based analysis of appendicitis in Washington State. They reviewed 85 790 patients who underwent an appen-dectomy and found no change in the negative ap-pendectomy rate despite an increase in CT utiliza-tion.36 It is interesting that the authors of the first major study on the utility of CT in children foresaw potential for problems, writing “the indiscriminate use of CT rectal contrast could potentially result in delay in diagnosis as well as unnecessary radiation exposure.”10
Our study has several strengths. First, our decision rules were derived prospectively in a large pediatric cohort. We were able to follow up on essentially all
Derivation Set
425 Patients ANC > 6.75 × 103/µL
138 Patients Nausea?
287 Patients 135 (-) APPY 152 (+) APPY
62 (-) APPY 0 (+) APPY
76 Patients
Tenderness maximal in RLQ?
29 Patients 29 (-) APPY
0 (+) APPY
47 Patients 42 (-) APPY
5 (+) APPY
NO YES
NO
NO YES
YES
176 Patients ANC > 6.75 x 103/µL
63 Patients Nausea?
113 patients 63 (-) APPY 50 (+) APPY
29 Patients 29 (-) APPY
0 (+) APPY
34 Patients
Tenderness maximal in RLQ?
11 Patients 10 (-) APPY
1 (+) APPY
23 Patients 20 (-) APPY
3 (+) APPY
Validation Set
NO
NO NO
YES YES
YES 62 atients P
patients who were enrolled in our study, thus con-firming the patients’ final diagnosis. By using 2 sta-tistical techniques, we have provided the clinician the option of a clinical score (logistic regression) or a decision tree (recursive partitioning), recognizing that some may prefer one type to the other. By val-idating our decision rules in a separate group of patients, we have accounted for the possibility of overfitting of data in our derivation set. Most impor-tant, our models’ high NPVs and low likelihood ratios in the validation groups indicate significant clinical utility.
One surprising finding of our study is the strong association between low ANC and the absence of appendicitis among patients with signs and symp-toms suspicious for appendicitis. In support of our finding, a recently published meta-analysis of clinical and laboratory predictors of appendicitis found that low levels of serum inflammatory markers were strongly associated with the absence of appendicitis. In this study, the presence of a WBC count of⬍9.0⫻ 103/L and⬍75% neutrophils had a negative likeli-hood ratio of 0.17 (95% CI: 0.07– 0.42) for appendici-tis.37 In addition, our results are similar to those of Garcia Pena et al,11 who also used recursive parti-tioning to stratify children into risk groups for ap-pendicitis. This retrospective study evaluated 958 children who were admitted to the hospital with suspected appendicitis and found that neutrophils
⬍67% and bands⬍5% could identify patients who did not have appendicitis. This relationship between low ANC and absence of appendicitis may exist only among a highly selective group of patients in whom the clinician has a strong clinical suspicion of appen-dicitis.
It is important to note the following limitations of our study. We used data-collection forms, an inher-ently subjective method for gathering data. In addi-tion, we did not calculate values for the clinical variables that we collected on individual patients. Ethically, it would have been concerning to have multiple physicians conduct physical examinations on children who were in pain if these additional examinations would be unlikely to affect the pa-tients’ care. Despite these limitations, our findings agreed with previous research that nausea, emesis, migration of pain to RLQ, and rebound pain were clinical variables strongly associated with appendi-citis.23,38–43 Furthermore, our recursive partitioning analysis revealed that anorexia and emesis were
sur-rogates for nausea in the low-risk rule, supporting the clinical utility of this variable. Next, the decision to obtain a surgical consultation, part of the entry criteria into our study, was based on a clinical prac-tice guideline specific to this institution. The thresh-old for obtaining a surgical consult is likely to vary at other institutions. Last, our decision rules were not perfect. In the validation sets, 2 patients were missed by the logistic-regression model and 1 patient was missed by the recursive partitioning model. The pa-tient who was misclassified by recursive partitioning was an 11-year-old girl who underwent US and CT during her first visit in the ED, both of which were negative for appendicitis. She was discharged from the hospital but returned 48 hours later for an ap-pendectomy (no perforation). Before our low-risk rules are applied clinically, they must be validated in other clinical settings. Most important, the decision rules can be used only for this highly selective pop-ulation of pediatric patients with suspected appen-dicitis; application of the rules to all pediatric pa-tients with abdominal pain would be inappropriate and thereby mislead the clinician.
CONCLUSIONS
We have derived 2 clinical rules to identify pa-tients who are at low risk for appendicitis. Although both decision rules performed similarly, some clini-cians may prefer a clinical score rather than a deci-sion tree. Logistic regresdeci-sion was used to develop a 6-part score that consists of nausea (2 points), history of focal RLQ pain (2 points), migration of pain (1 point), difficulty walking (1 point), rebound tender-ness/pain with percussion (2 points), and ANC
⬎6.75⫻103/L (6 points). A scoreⱕ5 achieved high sensitivity and NPV in both our derivation and val-idation groups. Using recursive partitioning, we de-termined that the combination of ANC⬍6.75⫻103/ L, absence of nausea (or emesis or anorexia), and absence of maximal tenderness in the RLQ essen-tially excluded appendicitis in our derivation and validation groups. Our opinion is that the recursive partitioning model has the advantage of simplicity and therefore should be the model of choice. Pediat-ric patients who have suspected appendicitis and are low risk by either model should be considered for observation rather than undergo CT scan or opera-tive care.
TABLE 5. Clinical Characteristics of Patients Who Were Misclassified as Low Risk by Logistic Regression and Recursive Partitioning in the Derivation and Validation Sets
Age/Gender Nausea History of Focal RLQ Pain
Migration of Pain
Unable to Walk
Maximal Pain in RLQ
Rebound Pain
ANC,
⫻103/L
CT Disposition Final Diagnosis
11 y/F*‡ ⫹ ⫺ ⫺ NA ⫺ ⫺ 6.5 ⫺ Home Appy
10 y/F†‡ ⫹ ⫺ ⫺ ⫹ ⫹ ⫺ 5.6 ⫺ OR Appy
11 y/M†‡ ⫹ ⫹ ⫹ ⫺ ⫹ ⫺ 2.7 ⫹ OR Appy
10 y/M‡ ⫹ ⫹ ⫺ ⫹ ⫹ ⫺ 4.2 ⫹ OR Appy
⫹indicates presence of finding, positive test;⫺, absence of finding, negative test; NA, not obtained or tested; OR, operating room; Appy, appendicitis (no perforation).
* Patient missed by recursive partitioning rule. † Patients missed in derivation set.
ACKNOWLEDGMENTS
We thank Robert Wright, MD, MPH, and Elyse Olshen, MD, MPH, for statistical assistance and thoughtful reviews of this manuscript. We also thank the PEM attending physicians, fellows, surgeons, and radiologists at Children’s Hospital Boston for assis-tance with this study.
REFERENCES
1. Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States.Am J Epidemiol.
1990;132:910 –925
2. HCUPnet, Healthcare Cost and Utilization Project. Available at: http:// hcup.ahrq.gov/HCUPnet.asp. Accessed August 1, 2004
3. Scholer SJ, Pituch K, Orr DP, Dittus RS. Clinical outcomes of children with acute abdominal pain.Pediatrics.1996;98:680 – 685
4. Rothrock SG, Skeoch G, Rush JJ, Johnson NE. Clinical features of misdiagnosed appendicitis in children.Ann Emerg Med.1991;20:45–50 5. Lund DP, Murphy EU. Management of perforated appendicitis in
children: a decade of aggressive treatment. J Pediatr Surg. 1994;29: 1130 –1133; discussion 1133–1134
6. Brender JD, Marcuse EK, Koepsell TD, Hatch EI. Childhood appendicitis: factors associated with perforation. Pediatrics.1985;76: 301–306
7. Rappaport WD, Peterson M, Stanton C. Factors responsible for the high perforation rate seen in early childhood appendicitis.Am Surg.1989;55: 602– 605
8. Flum DR, Koepsell T. The clinical and economic correlates of misdiag-nosed appendicitis: nationwide analysis.Arch Surg.2002;137:799 – 804; discussion 804
9. Fishman SJ, Pelosi L, Klavon SL, O’Rourke EJ. Perforated appendicitis: prospective outcome analysis for 150 children.J Pediatr Surg.2000;35: 923–926
10. Garcia Pena BM, Mandl KD, Kraus SJ, et al. Ultrasonography and limited computed tomography in the diagnosis and management of appendicitis in children.JAMA.1999;282:1041–1046
11. Garcia Pena BM, Cook EF, Mandl KD. Selective imaging strategies for the diagnosis of appendicitis in children.Pediatrics.2004;113:24 –28 12. Rao PM, Rhea JT, Novelline RA, Mostafavi AA, McCabe CJ. Effect of
computed tomography of the appendix on treatment of patients and use of hospital resources.N Engl J Med.1998;338:141–146
13. Pena BM, Taylor GA, Lund DP, Mandl KD. Effect of computed tomog-raphy on patient management and costs in children with suspected appendicitis.Pediatrics.1999;104:440 – 446
14. Smink DS, Finkelstein JA, Garcia Pena BM, Shannon MW, Taylor GA, Fishman SJ. Diagnosis of acute appendicitis in children using a clinical practice guideline.J Pediatr Surg.2004;39:458 – 463; discussion 458 – 463 15. Lee SL, Walsh AJ, Ho HS. Computed tomography and ultrasonography do not improve and may delay the diagnosis and treatment of acute appendicitis.Arch Surg.2001;136:556 –562
16. Safran DB, Pilati D, Folz E, Oller D. Is appendiceal CT scan overused for evaluating patients with right lower quadrant pain?Am J Emerg Med.
2001;19:199 –203
17. Brenner D, Elliston C, Hall E, Berdon W. Estimated risks of radiation-induced fatal cancer from pediatric CT.AJR Am J Roentgenol.2001;176: 289 –296
18. Alvarado A. A practical score for the early diagnosis of acute appendi-citis.Ann Emerg Med.1986;15:557–564
19. Ohmann C, Yang Q, Franke C. Diagnostic scores for acute appendicitis. Abdominal Pain Study Group.Eur J Surg.1995;161:273–281
20. Bond GR, Tully SB, Chan LS, Bradley RL. Use of the MANTRELS score in childhood appendicitis: a prospective study of 187 children with abdominal pain.Ann Emerg Med.1990;19:1014 –1018
21. Macklin CP, Radcliffe GS, Merei JM, Stringer MD. A prospective eval-uation of the modified Alvarado score for acute appendicitis in chil-dren.Ann R Coll Surg Engl.1997;79:203–205
22. Lamparelli MJ, Hoque HM, Pogson CJ, Ball AB. A prospective evalua-tion of the combined use of the modified Alvarado score with selective laparoscopy in adult females in the management of suspected appen-dicitis.Ann R Coll Surg Engl.2000;82:192–195
23. Dado G, Anania G, Baccarani U, et al. Application of a clinical score for the diagnosis of acute appendicitis in childhood: a retrospective analy-sis of 197 patients.J Pediatr Surg.2000;35:1320 –1322
24. Samuel M. Pediatric appendicitis score.J Pediatr Surg.2002;37:877– 881 25. van den Broek WT, van der Ende ED, Bijnen AB, Breslau PJ, Gouma DJ. Which children could benefit from additional diagnostic tools in case of suspected appendicitis?J Pediatr Surg.2004;39:570 –574
26. Kwok MY, Kim MK, Gorelick MH. Evidence-based approach to the diagnosis of appendicitis in children. Pediatr Emerg Care. 2004;20: 690 – 698; quiz 699 –701
27. Brenner DJ, Elliston CD, Hall EJ, Berdon WE. Estimates of the cancer risks from pediatric CT radiation are not merely theoretical: comment on “point/counterpoint: in x-ray computed tomography, technique factors should be selected appropriate to patient size.against the propo-sition.” Med Phys.2001;28:2387–2388
28. Radiation and Pediatric Computed Tomography. Available at: www. nci.nih.gov/cancertopics/causes/radiation-risks-pediatric-CT. Ac-cessed October 22, 2004
29. Applegate KE, Sivit CJ, Salvator AE, et al. Effect of cross-sectional imaging on negative appendectomy and perforation rates in children.
Radiology.2001;220:103–107
30. Pena BM, Taylor GA, Fishman SJ, Mandl KD. Costs and effectiveness of ultrasonography and limited computed tomography for diagnosing appendicitis in children.Pediatrics.2000;106:672– 676
31. Pena BM, Taylor GA, Fishman SJ, Mandl KD. Effect of an imaging protocol on clinical outcomes among pediatric patients with appendi-citis.Pediatrics.2002;110:1088 –1093
32. Rao PM, Rhea JT, Rattner DW, Venus LG, Novelline RA. Introduction of appendiceal CT: impact on negative appendectomy and appendiceal perforation rates.Ann Surg.1999;229:344 –349
33. Partrick DA, Janik JE, Janik JS, Bensard DD, Karrer FM. Increased CT scan utilization does not improve the diagnostic accuracy of appendi-citis in children.J Pediatr Surg.2003;38:659 – 662
34. Martin AE, Vollman D, Adler B, Caniano DA. CT scans may not reduce the negative appendectomy rate in children.J Pediatr Surg. 2004;39: 886 – 890; discussion 886 – 890
35. Karakas SP, Guelfguat M, Leonidas JC, Springer S, Singh SP. Acute appendicitis in children: comparison of clinical diagnosis with ultra-sound and CT imaging.Pediatr Radiol.2000;30:94 –98
36. Flum DR, Morris A, Koepsell T, Dellinger EP. Has misdiagnosis of appendicitis decreased over time? A population-based analysis.JAMA.
2001;286:1748 –1753
37. Andersson RE. Meta-analysis of the clinical and laboratory diagnosis of appendicitis.Br J Surg.2004;91:28 –37
38. Williams N, Kapila L. Acute appendicitis in the preschool child.Arch Dis Child.1991;66:1270 –1272
39. Williams N, Kapila L. Acute appendicitis in the under-5 year old.J R Coll Surg Edinb.1994;39:168 –170
40. Williams NM, Johnstone JM, Everson NW. The diagnostic value of symptoms and signs in childhood abdominal pain.J R Coll Surg Edinb.
1998;43:390 –392
41. Rothrock SG, Pagane J. Acute appendicitis in children: emergency de-partment diagnosis and management.Ann Emerg Med.2000;36:39 –51 42. O’Shea JS, Bishop ME, Alario AJ, Cooper JM. Diagnosing appendicitis
in children with acute abdominal pain. Pediatr Emerg Care. 1988;4: 172–176
DOI: 10.1542/peds.2005-0094
2005;116;709
Pediatrics
Anupam B. Kharbanda, George A. Taylor, Steven J. Fishman and Richard G. Bachur
A Clinical Decision Rule to Identify Children at Low Risk for Appendicitis
Services
Updated Information &
http://pediatrics.aappublications.org/content/116/3/709
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/116/3/709#BIBL
This article cites 41 articles, 7 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/emergency_medicine_ Emergency Medicine
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2005-0094
2005;116;709
Pediatrics
Anupam B. Kharbanda, George A. Taylor, Steven J. Fishman and Richard G. Bachur
A Clinical Decision Rule to Identify Children at Low Risk for Appendicitis
http://pediatrics.aappublications.org/content/116/3/709
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.