Northumbria Research Link
Citation: McCullogh, Nicola (2019) The efficacy of school-based classroom learning and physical activity interventions for children’s cognitive performance and wellbeing. Doctoral thesis, Northumbria University.
This version was downloaded from Northumbria Research Link: http://nrl.northumbria.ac.uk/41886/
Northumbria University has developed Northumbria Research Link (NRL) to enable users to access the University’s research output. Copyright © and moral rights for items on NRL are retained by the individual author(s) and/or other copyright owners. Single copies of full items can be reproduced, displayed or performed, and given to third parties in any format or medium for personal research or study, educational, or not-for-profit purposes without prior permission or charge, provided the authors, title and full bibliographic details are given, as well as a hyperlink and/or URL to the original metadata page. The content must not be changed in any way. Full items must not be sold commercially in any format or medium without formal permission of the copyright holder. The full policy is available online:
http://nrl.northumbria.ac.uk/pol i cies.html
The Efficacy of School-Based
Classroom Learning and Physical
Activity Interventions for Children’s
Cognitive Performance and Wellbeing
N McCullogh
PhD
The Efficacy of School-Based
Classroom Learning and Physical
Activity Interventions for Children’s
Cognitive Performance and Wellbeing
Nicola McCullogh
A thesis submitted in partial fulfilment of
the requirements of the University of
Northumbria at Newcastle for the degree
of Doctor of Philosophy
Research undertaken in the Faculty of
Health and Life Sciences
Abstract
This programme of research investigated children’s cognitive performance, academic achievement and wellbeing in association with their participation in primary school-based interventions in which healthy lifestyle/positive choices messages were delivered through classroom learning and physical activity.
A positive correlation was found between the time children spent in moderate-to-vigorous physical activity during intervention sessions and their post-session long-term memory performance (Study 2). Taking a more chronic perspective of intervention participation, in a quasi-experiment testing whether children experienced improvements in cognitive performance, academic achievement and wellbeing over and above those of a control group, results were inconclusive but potentially suggestive of increases in reading and mathematics achievement for the intervention group at the conclusion of the 6-week programme (Study 3). Finally, qualitative data from interviews/focus groups with stakeholders including children, parents and school staff showed that interventions were viewed favourably in relation to children’s engagement and outcomes (Study 4); pupils enjoyed their participation, particularly in the physical activity, and they were thought to benefit in terms of their wellbeing and personal development (e.g. increased healthy lifestyle knowledge, enhanced self-esteem). Parents did however feel that they themselves were not well informed about the interventions and that they could have reinforced programme messages had they known more. In the long term, these findings will assist in informing policy and practice regarding school provision of healthy lifestyle and physical activity opportunities, for instance supporting their inclusion in the timetable despite pressures for schools to prioritise core curriculum subjects.
The thesis contributes to the literature in its focus on cognitive performance and academic achievement, outcomes not often measured for physical activity and positive choices interventions. It also recognises a lack of consistency in the measurement of cognitive performance in the existing research, with Study 1 piloting a cognitive test battery for use in school settings.
List of Contents
Abstract ... 1
List of Contents ... 2
List of Tables and Figures ... 10
Acknowledgements ... 12
Author’s Declaration ... 13
Chapter 1: Background Context ... 14
1.1 Physical Activity, Health and Wellbeing Provision in Schools ... 14
1.2 Research Setting ... 16
1.3 Details of the Interventions ... 17
1.4 Intervention Participation and Physical Activity ... 20
1.5 Overview of the Thesis ... 24
Chapter 2: Literature Review ... 29
2.1 Definitions of Key Constructs in the Thesis... 29
2.1.1 Defining Cognitive Performance ... 30
2.1.1.1 Processing Speed ... 30
2.1.1.2 Attention ... 31
2.1.1.3 Executive Function ... 31
2.1.1.4 Long-Term Memory ... 32
2.1.2 Defining Academic Achievement ... 33
2.1.3 Defining Wellbeing ... 33
2.1.4 Defining Physical Activity ... 34
2.2 Relationships between the Key Constructs ... 35
2.2.1 Cognitive Performance and Academic Achievement ... 35
2.2.3 Physical Activity and Cognitive Performance ... 43
2.2.3.1 Acute Physical Activity and Cognitive Performance ... 44
2.2.3.2 Chronic Physical Activity and Cognitive Performance... 53
2.2.4 Physical Activity and Academic Achievement ... 61
2.2.5 Physical Activity and Wellbeing ... 64
2.3 Additional Variables Associated with the Key Constructs ... 69
2.4 Stakeholder Perspectives on PSHE and Physical Activity Interventions .... 73
Chapter 3: Methodology ... 76
3.1 Ontological and Epistemological Assumptions... 76
3.2 Methodology: Mixed Methods Approach ... 77
3.3 Quantitative Approach ... 80
3.3.1 Quantitative Reliability and Validity ... 83
3.3.2 Quantitative Methods ... 84
3.3.2.1 Cognitive Performance: Cognitive Testing ... 84
3.3.2.2 Academic Achievement: Teacher Assessment ... 85
3.3.2.3 Wellbeing: Questionnaire ... 87
3.3.2.4 Physical Activity: Accelerometry... 90
3.4 Qualitative Approach ... 93
3.4.1 Qualitative Methods: Semi-Structured Focus Groups/Interviews ... 94
3.4.2 Qualitative Analysis: Thematic Analysis ... 96
3.4.3 Qualitative Rigour ... 98
Chapter 4: Study 1 – The Creation and Reliability and Validity Testing of CogS: 9– 11, a Cognitive Test Battery for Researchers Working with 9–11-year-olds in School Settings ... 100
4.1 Introduction ... 100
4.2 Method ... 102
4.2.1 Selection of Cognitive Tests ... 102
4.2.1.2 Match-Up! ... 104
4.2.1.3 Find ‘M’ ... 104
4.2.1.4 Memorise! ... 105
4.2.1.5 3-Back ... 106
4.2.1.6 Colours and Shapes ... 107
4.2.1.7 Which Colour?... 109 4.2.1.8 Remembering Backwards! ... 110 4.2.2 Ethical Approval ... 111 4.2.3 Recruitment ... 111 4.2.4 Procedure ... 113 4.2.5 Data Analysis ... 114
4.2.5.1 Parallel Forms Reliability ... 114
4.2.5.2 Test–Retest Reliability ... 115
4.2.5.3 Construct Validity ... 115
4.3 Results ... 116
4.3.1 Participants ... 116
4.3.2 Preliminary Data Analysis ... 116
4.3.3 Parallel Forms Reliability ... 118
4.3.4 Test–Retest Reliability ... 119
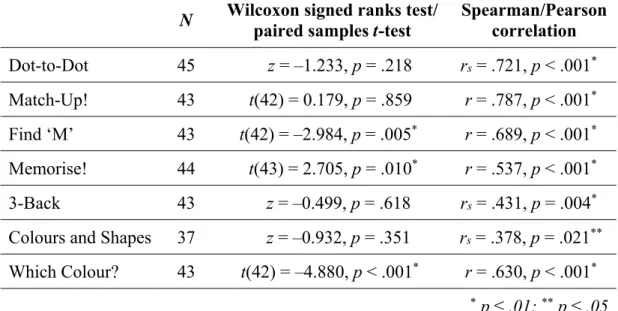
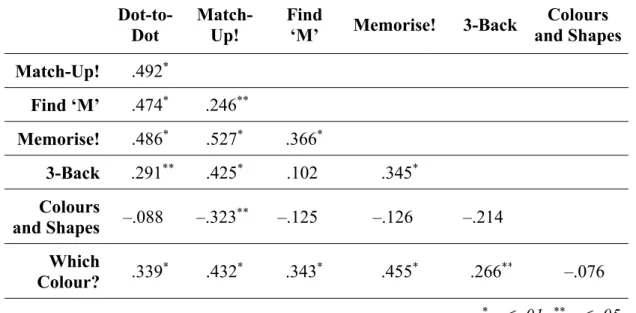
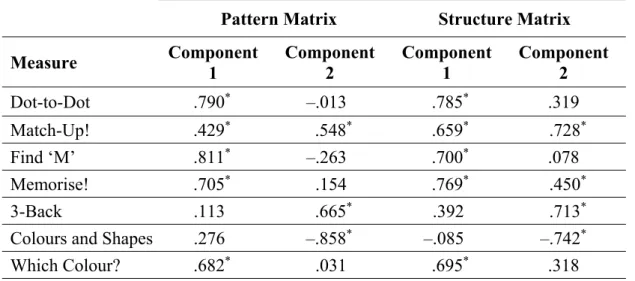
4.3.5 Construct Validity ... 120
4.4 Discussion ... 121
4.4.1 Parallel Forms Reliability ... 121
4.4.2 Test–Retest Reliability ... 122
4.4.3 Construct Validity ... 123
4.4.4 Limitations ... 124
4.5 Conclusion and Potential Impact ... 126
Chapter 5: General Methods – Studies 2 and 3 ... 128 5.1 Experimental Design ... 128 5.2 Ethical Approval ... 130 5.3 Recruitment ... 131 5.4 Procedure ... 134 5.5 Measurements ... 135
5.5.1 Cognitive Testing (CogS: 9–11 Test Battery) ... 135
5.5.2 Academic Achievement (Teacher Report) ... 137
5.5.3 Wellbeing (KIDSCREEN-27 Questionnaire) ... 137
5.5.4 Physical Activity (Accelerometry) ... 140
5.5.4.1 Anthropometric Measurements ... 141
5.6 Sample Size Calculation ... 141
Chapter 6: Study 2 – The Effects of Acute Physical Activity Participation during Classroom- and Physical Activity-Based Intervention Sessions on Children’s Cognitive Performance... 143 6.1 Introduction ... 143 6.2 Method ... 145 6.2.1 Data Analysis ... 145 6.3 Results ... 145 6.3.1 Participants ... 145
6.3.1.1 Participants in the Cognitive Performance Analyses ... 145
6.3.1.2 Participants with Physical Activity Data ... 146
6.3.2 Preliminary Data Analysis ... 146
6.3.2.1 Cognitive Performance Data ... 146
6.3.2.2 Physical Activity Data ... 149
6.3.3 Post-PA vs. Post-Classroom Cognitive Performance ... 150
6.3.4 Partial Correlations between Cognitive Performance and MVPA ... 151
6.4.1 Limitations ... 154
6.5 Conclusion and Potential Impact ... 155
Chapter 7: Study 3 – Children’s Wellbeing, Cognitive Performance and Academic Achievement Following Participation in a Combined Classroom Learning and Physical Activity Intervention... 156
7.1 Introduction ... 156
7.2 Method ... 158
7.2.1 Data Analysis ... 158
7.3 Results ... 159
7.3.1 Participants ... 159
7.3.2 Preliminary Data Analysis ... 159
7.3.3 Intervention Participation and Wellbeing ... 163
7.3.4 Intervention Participation and Cognitive Performance ... 164
7.3.5 Intervention Participation and Academic Achievement ... 164
7.4 Discussion ... 165
7.4.1 Limitations ... 168
7.5 Conclusion and Potential Impact ... 169
7.6 Study 3a: Pilot Study of Children’s Intervention Participation and Daily Physical Activity ... 169 7.6.1 Introduction ... 169 7.6.2 Method ... 170 7.6.2.1 Procedure ... 170 7.6.2.2 Data Analysis... 171 7.6.3 Results ... 172 7.6.3.1 Participants ... 172
7.6.3.2 Preliminary Data Analysis ... 172
7.6.3.3 Children’s Intervention Participation and Daily Physical Activity 173 7.6.4 Discussion ... 174
Chapter 8: Study 4 – The Views of Stakeholders on Combined Classroom Learning and Physical Activity PSHE Interventions for Schoolchildren: A Thematic Analysis
... 175 8.1 Introduction ... 175 8.2 Method ... 177 8.2.1 Ethical Approval ... 177 8.2.2 Interventions ... 178 8.2.3 Participants ... 179 8.2.4 Materials ... 182 8.2.5 Procedure ... 183 8.2.6 Data Analysis ... 184 8.2.6.1 Saturation ... 186 8.3 Findings ... 186
8.3.1 Research Question 1: The Role of Physical Activity ... 187
8.3.1.1 Theme 1: Suitability for a Range of Children ... 187
8.3.1.2 Theme 2: Rest and Reward... 188
8.3.1.3 Theme 3: Reinforcement ... 189
8.3.2 Research Question 2: Engagement ... 190
8.3.2.1 Theme 1: Children’s Enjoyment ... 190
8.3.2.2 Theme 2: Delivery by a Non-Teacher ... 196
8.3.2.3 Theme 3: Association with Football Club ... 197
8.3.2.4 Theme 4: Children’s Personal Circumstances and Characteristics 201 8.3.3 Research Question 3: Outcomes ... 206
8.3.3.1 Theme 1: Wellbeing and Personal Development ... 206
8.3.3.2 Theme 2: Increased Physical Activity ... 212
8.3.3.3 Theme 3: Teacher Development ... 217
8.3.4 Research Question 4: Sustainability... 218
8.3.4.2 Theme 2: School Awareness and Acceptance of Interventions ... 222
8.4 Discussion ... 226
8.4.1 The Role of Physical Activity ... 228
8.4.2 Engagement ... 228
8.4.3 Outcomes ... 230
8.4.4 Sustainability ... 233
8.4.5 Limitations ... 235
8.5 Conclusion and Potential Impact ... 236
Chapter 9: General Discussion ... 238
9.1 Summary of the Findings ... 240
9.2 Further Discussion on Study 1 ... 242
9.3 Further Discussion on Studies 2, 3, 3a and 4 ... 244
9.4 Strengths and Limitations of the Research ... 250
9.5 Directions for Future Research ... 252
9.6 Conclusion and Recommendations ... 253
Appendices ... 256
Appendix A(i): Initial Version of the CogS: 9–11 Cognitive Test Battery, as used in Study 1 (Example: Red Booklet) ... 256
Appendix A(ii): Stimuli for the CogS: 9–11 Memorise! Task, as used in Studies 1– 3 (All Booklet Versions) ... 268
Appendix A(iii): Stimuli for the CogS: 9–11 3-Back Task, as used in Studies 1–3 (All Booklet Versions) ... 269
Appendix B: Example Consent Form (Study 4, Child Participants) ... 273
Appendix C: Example Information Sheet for Children (Study 1) ... 275
Appendix D: Example Information Sheet for Parents/Guardians (Studies 2 and 3, Intervention Group) ... 276
Appendix E: Example Debrief for Parents/Guardians (Studies 2 and 3, Intervention Group) ... 280
Appendix F: Example Debrief for Children (Studies 2 and 3, Control Group) ... 282
Appendix G: Study 1 – Summary of Results for Participants and Schools ... 283
Appendix H: Final Version of the CogS: 9–11 Cognitive Test Battery, as used in Studies 2 and 3 (Example: Green Booklet) ... 284
Appendix I: Studies 2–3 – Summary of Results for Participants and Schools .... 295
Appendix J: School Permission Slip ... 296
Appendix K: Study 4 – Summary of Results for Participants and Schools ... 297
Appendix L(i): Study 4 – Focus Group Guide for Children ... 298
Appendix L(ii): Study 4 – Interview/Focus Group Guide for Parents/Guardians 300 Appendix L(iii): Study 4 – Interview Guide for School Staff ... 302
Appendix L(iv): Study 4 – Interview Guide for Intervention Staff... 304
Appendix M(i): Study 4 – List of Initial Codes ... 306
Appendix M(ii): Study 4 – Coding Framework ... 308
Appendix M(iii): Study 4 – Development of Initial Thematic Maps ... 310
Appendix M(iv): Study 4 – Analysis Trail: Theme Summary Tables ... 316
Appendix M(v): Study 4 – Themes Saturation ... 327
List of Abbreviations ... 331
List of Tables and Figures
Tables
Table 4.1. Characteristics of schools at the time of their involvement in Study 1 .. 112
Table 4.2. Order of presentation of research booklets, Study 1 ... 114
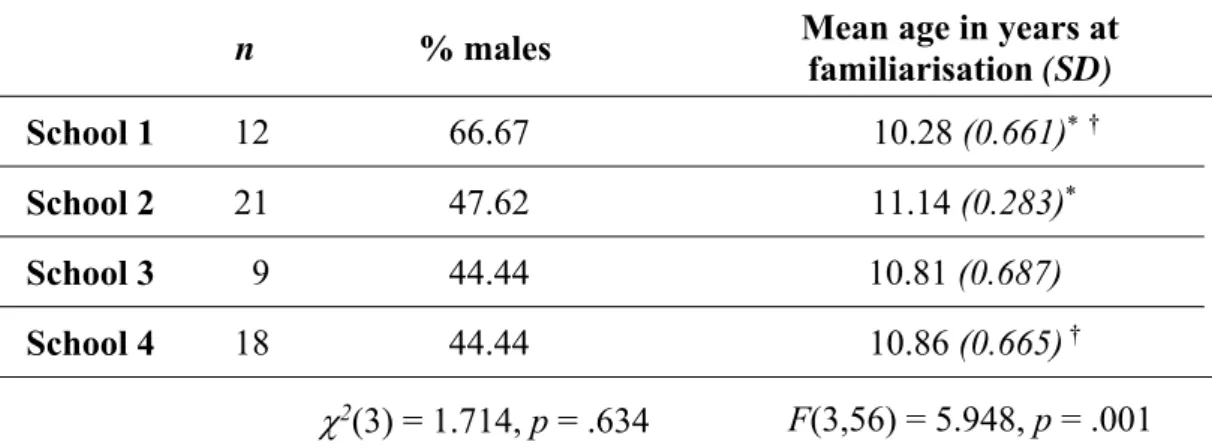
Table 4.3. Participant characteristics, Study 1 ... 116
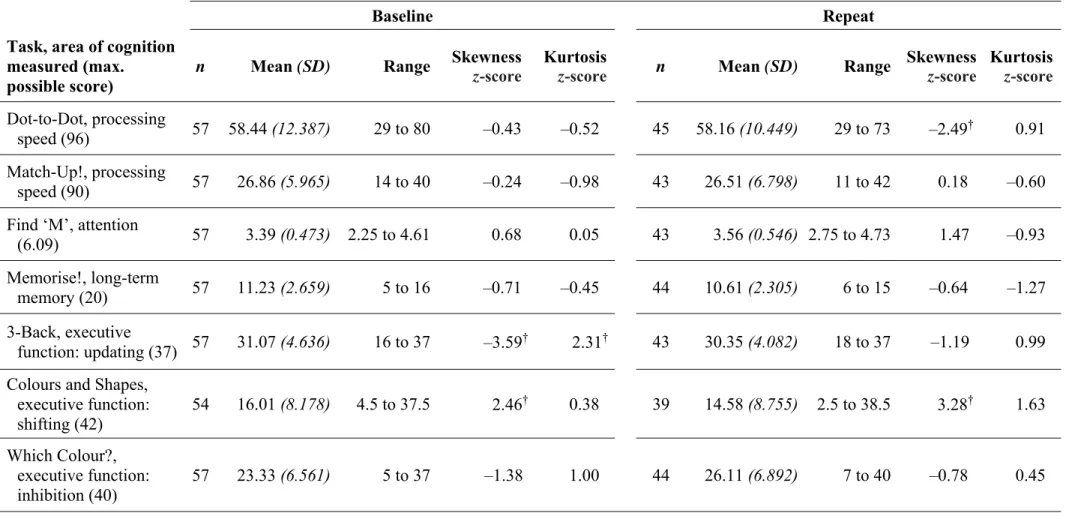
Table 4.4. Descriptive statistics for the dependent measures at baseline and repeat testing, Study 1 ... 117
Table 4.5. Test–retest reliability for scores at baseline and repeat, Study 1 ... 119
Table 4.6. Principal component analysis, Study 1: Correlation matrix ... 120
Table 4.7. Principal component analysis, Study 1: Loadings ... 121
Table 5.1. Characteristics of schools at the time of their involvement in Studies 2 and 3 ... 132
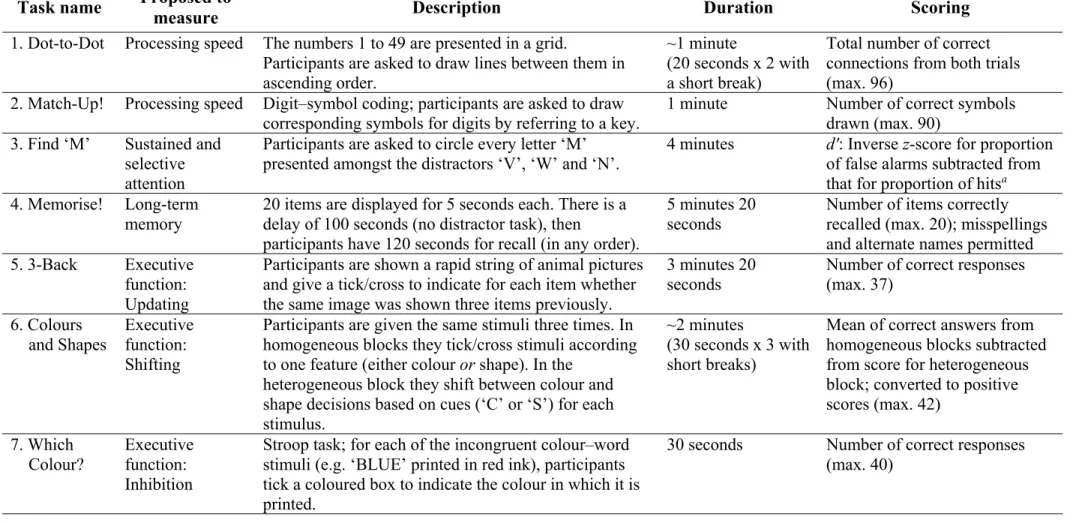
Table 5.2. Summary of cognitive tests used in Studies 2 and 3 ... 136
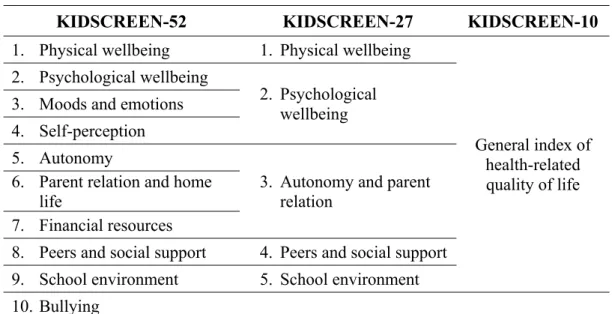
Table 5.3. Dimensions of health-related quality of life assessed by the three versions of the KIDSCREEN questionnaire ... 138
Table 6.1. Participant characteristics by PA/classroom group, Study 2 ... 146
Table 6.2. Descriptive statistics for the dependent measures at pretest, Study 2 .... 148
Table 6.3. Partial correlations between time spent in MVPA during the PA component of the intervention session and post-PA cognitive test scores, Study 2 ... 151
Table 7.1. Participant characteristics by intervention/control group, Study 3 ... 159
Table 7.2. Descriptive statistics for the dependent measures at pretest, Study 3 .... 161
Table 7.3. Follow-up analyses for the main effect of group in the intervention participation and wellbeing MANCOVA, Study 3 ... 163
Table 7.4. Participant characteristics by intervention/control group, Study 3a ... 172
Table 8.1. Characteristics of the interventions discussed by participants in Study 4
... 179
Table 8.2. Characteristics of schools at the time of their involvement in Study 4 .. 181
Figures Figure 1.1. Summary of the programme of work ... 24
Figure 4.1. Example stimulus grid for the Dot-to-Dot task ... 103
Figure 4.2. Example stimuli from the heterogeneous trial of the Colours and Shapes task, Study 1 ... 108
Figure 4.3. Example stimuli from the Which Colour? task ... 109
Figure 5.1. Protocol for Studies 2 and 3 ... 129
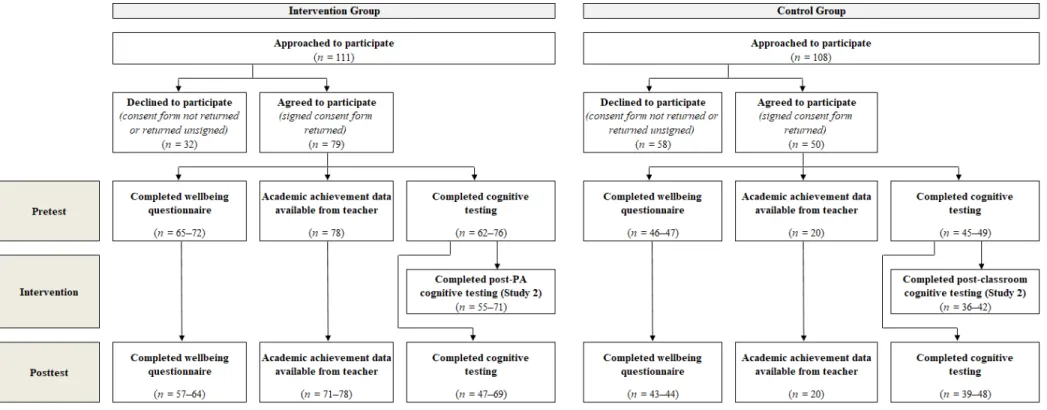
Figure 5.2. Flow of participants through Studies 2 and 3 ... 133
Figure 6.1. Mean number of minutes spent by participants in sedentary behaviour, light intensity physical activity (light PA) and moderate-to-vigorous intensity physical activity (MVPA) in the physical activity component of the intervention sessions ... 150
Figure 8.1. Final thematic map for research question 1: The role of physical activity in the interventions ... 187
Figure 8.2. Final thematic map for research question 2: Children’s engagement in the intervention sessions ... 190
Figure 8.3. Final thematic map for research question 3: Intervention outcomes .... 206
Figure 8.4. Final thematic map for research question 4: Sustainability of intervention delivery ... 218
Acknowledgements
I undertook this programme of research in the hopes of supporting school staff in delivering a varied, engaging curriculum for their pupils. Many of my friends and family work in primary schools and I am aware there are a lot of pressures on you all; I hope the findings from this research help to give you confidence that you are all doing great and that you know your work is appreciated.
I would like to thank my primary supervisor, Dr Spencer E. Boyle, for all of his academic and moral support throughout my research programme – having a mentor with a level head and a ready smile really does make all the difference! Thanks also to the other members of my supervisory team, Dr Melissa Fothergill and Professor Greta Defeyter, for their much appreciated guidance through the tricky times, and to Northumbria University for providing the studentship fund that enabled me to undertake the research programme.
Many thanks go to the football club foundations who allowed me to conduct research into their intervention programmes, and to the members of intervention staff, school staff, parents and children who took part in the studies. Special thanks to my family and friends who were able to suggest schools that might be willing to take part, and to the schools who said yes – this project would not have been possible without you. As always, I could never have undertaken this project without all of the brilliant people in my life spurring me on. To Dr Sarah Partington and Dr Elizabeth Partington, thank you for inspiring me to go on to further study. To the friends I have made at Northumbria, to my fellow archers and to my family, you are all amazing. To the cast and crew of Marvel’s Agents of S.H.I.E.L.D., thank you for some much-needed escapism!
To Mam, Dad and my brother Andy, this thesis is dedicated to you. Thank you all for always being there for me.
Author’s Declaration
I declare that the work contained in this thesis has not been submitted for any other award and that it is all my own work. I also confirm that this work fully acknowledges opinions, ideas and contributions from the work of others.
Any ethical clearance for the research presented in this thesis has been approved. Approval has been sought and granted by the Faculty of Health and Life Sciences Research Ethics Committee on 15.02.17 for Study 1, 18.07.16 for Studies 2, 3 and 3a, and 13.06.16 for Study 4.
I declare that the Word Count of this Thesis is 83,560 words. Name:
Signature: Date:
Chapter 1: Background Context
This thesis provides an account of a PhD programme of research examining combined classroom learning and physical activity (PA) interventions delivered by football club foundations to primary schools in the North East of England. The interventions deliver content mapping to Personal, Social, Health and Economic education (PSHE) topics such as maintaining a healthy lifestyle via diet and exercise, developing an awareness of drugs and recognising the effects of bullying and discrimination (PSHE Association, 2017), and their target audience is 9–11-year-old pupils. The issues of central interest in the thesis are the unusual inclusion of PA to complement the classroom component of the sessions, and also the outcomes of programme participation for pupils’ cognitive performance and academic achievement, as well as for their wellbeing.
The programme of research comprised four studies. Study 1 assessed the reliability and validity of a cognitive test battery designed for use in Studies 2 and 3, which constituted an acute quantitative study into children’s cognitive performance immediately following the PA component of one of the intervention sessions (Study 2) and a chronic quantitative study into children’s cognitive performance, academic achievement and wellbeing following intervention participation (Study 3). Study 3 also contained a pilot study (Study 3a) into daily PA participation as a potential mechanism for intervention outcomes. Finally, Study 4 took a qualitative approach and explored stakeholders’ views on classroom/PA-format PSHE interventions. A more detailed overview of the studies is provided at the end of this chapter.
1.1 Physical Activity, Health and Wellbeing Provision in Schools
In England, PSHE is a non-statutory subject in which schools can deliver programmes of their own design in order to help their pupils to understand risks and develop the skills and knowledge for making safe and informed decisions (Department for Education, 2013). Some PSHE topics are however statutory requirements in other subjects, for instance with the impact of diet, exercise and drugs on the body being covered in science. Schools are not obliged to allocate a certain amount of their
teaching time to PSHE, but the PSHE Association (2018) recommends 1 hour per week of discrete PSHE education.
The national curriculum in England does make stipulations regarding the delivery of Physical Education (PE) in primary schools, some of the aims of this subject being to ensure that children lead healthy, active lives, that they develop physical competence and that they have the opportunity to communicate, collaborate and compete with others (Department for Education, 2015). Although academy schools are not required to follow the national curriculum, it was clear from their published curricula that all of the schools involved in the studies in this research programme pertaining directly to interventions (i.e. Studies 2, 3 and 4) followed the national curriculum for PE or very similar programmes with the same aims regarding children’s health, movement skills and teamwork.
While the amount of school time to be spent on PE is again unspecified, an Office for Standards in Education, Children’s Services and Skills (Ofsted) report based on inspections conducted between 2008 and 2012 stated that most primary schools provided 2 hours of PE per week for their pupils (Ofsted, 2013). In a similar manner, despite being valued by pupils and school staff as a chance for children to engage in PA, as well as to socialise, there is no clear guidance regarding the provision of recreational breaks during the school day, and the duration of breaks in England and Wales has declined over time (Blatchford & Baines, 2006). Further opportunities for PA might exist through before- and after-school clubs but the current discussion will focus on only structured school time provision (e.g. PE) as this is available to all children and explicitly aims for children to be active.
A recent article by Bailey (2017) discusses the place of PA in education and identifies as “the heart of the issue” (p. 779) that the value placed on educational attainment by parents/guardians (referred to throughout the thesis as parents for brevity), teachers and policymakers often results in priority being given in the school day to core subjects such as mathematics and reading over non-core subjects including PE. Indeed, reading, writing and mathematics receive almost exclusive attention in the primary school performance tables for England (Department for Education, 2018). However, both PA, as a central component of PE, and wellbeing, as an anticipated outcome of
PA and PSHE, have been positively associated with academic achievement (as discussed in Chapter 2). It has been suggested that teachers and administrators may not be aware of the benefits of PA for learning, possibly therefore missing opportunities to integrate it into the curriculum (Castelli et al., 2014). On the other hand, there have been few UK studies into school-based health and wellbeing interventions which report on educational outcomes (White, 2017), so the relationship between participation in PSHE-type programmes and learning requires further exploration. The interventions explored in this research programme provide a window into the contribution of PSHE and PA to children’s cognitive performance and academic achievement, with the research results being anticipated in the long term – when combined with the results of other research into PSHE and PA delivery – to help shape policy and practice around the provision of PSHE and PA opportunities in primary school education.
1.2 Research Setting
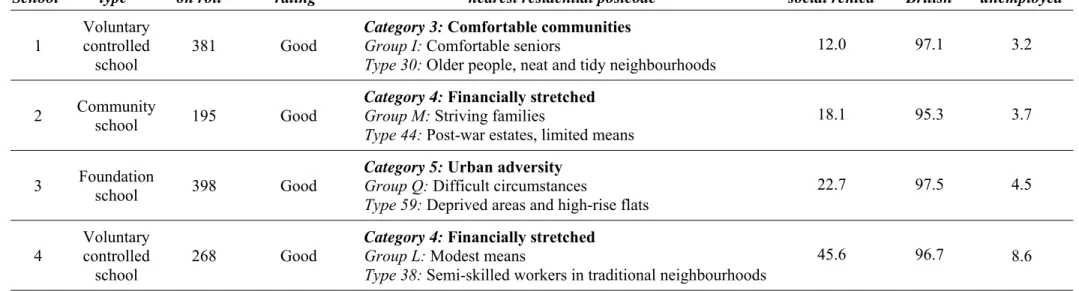
To place the research in context, all of the studies were conducted in the North East of England. A statistical bulletin released in 2014 by the Office for National Statistics, reporting on data from 2012, calculated the Gross Disposable Household Income for the North East of England to be the lowest of all of the UK regions, at a figure of £14,393 per head compared to £17,066 per head for England overall. Furthermore, the English Indices of Deprivation 2015 placed the local authority districts of seven of the nine schools involved in the studies pertaining directly to the interventions (Studies 2, 3 and 4) amongst the most deprived 20% of local authority districts – and the remaining two schools amongst the most deprived 30% – according to the Index of Multiple Deprivation. This measure combines information on seven domains of deprivation: income; employment; education; health; crime; barriers to housing and services; and living environment (Department for Communities and Local Government, 2015). As outlined in ‘The impact of social and economic inequalities on children’s health’, a report by the All-Party Parliamentary Group on a Fit and Healthy Childhood (2018), socioeconomically disadvantaged children are more likely than those in more affluent areas to experience poor health including overweight/obesity and poorer mental wellbeing, adverse educational outcomes and lower levels of sport participation. It would therefore appear to be particularly
appropriate for PSHE interventions with a PA component to be conducted with children from deprived geographical areas; however, the purpose of the research programme was not to comment on socioeconomic status (SES) as an impetus for intervention delivery, nor to explore its role for children’s outcomes; the information in this section is provided simply to assist the reader in understanding the context of the studies.
Data for all of the studies constituting the research programme were collected between August 2016 and July 2018. The data collection period was a time of political and economic uncertainty for the UK in the wake of the June 2016 referendum in which the country voted to leave the European Union (“EU Referendum: England Leads UK to Exit,” 2016). As such, the continuation of one of the interventions explored in Study 4 was under question at the point of data collection due to the intervention being funded by the local council: an issue noted by the intervention staff to have been of concern. Furthermore, school staff had been primed to anticipate changes to the targets to which they were working, the UK government having announced as part of its goal for all schools in England to convert to academies that in the north of the country there would be a new focus on school performance (Sellgren, 2016). This may have increased the pressure discussed by Bailey (2017) upon schools to prioritise core curriculum subjects.
1.3 Details of the Interventions
The main intervention investigated in this research programme – explored in Studies 2 and 3 and discussed by nine of the participants in Study 4 – ran as a 6-week course for Key Stage 2 pupils (upper primary school; 7–11-year-old children). Year 5 pupils (9–10-year-olds) took part in the research. The intention was for each of the weekly intervention sessions to constitute 60 minutes of classroom work and 60 minutes of physical activity; a sense check conducted through the researcher’s observation of a number of sessions and via reports from school and intervention staff in Study 4 revealed that these time allocations were sometimes reduced due to the need to accommodate school events such as assemblies, and the PA component sometimes included time for children to change into their PE kits.
Two PSHE topics were taught within the classroom/PA intervention model, one addressing fitness and nutrition and the other addressing discrimination. The fitness and nutrition programme had five aims: to improve children’s knowledge in relation to health and wellbeing; to develop their understanding of a healthy, balanced diet; to improve their physical fitness through PA participation; to promote increased PA participation; and to increase their confidence in participating in PA. Intervention staff reported in Study 4 that further messages included the roles for health of hydration, adequate sleep and not smoking. The discrimination programme similarly aimed to promote increased PA participation and children’s confidence in this, as well as raising their awareness of discrimination and hate crime and increasing their knowledge and understanding around topics including bullying, sexism, racism and disability awareness.
The organisation behind the intervention was a football club foundation, with charitable foundations being common to many professional football clubs in the UK as a means through which to provide PA- and education-related opportunities for their local communities. Two facilitators wearing football club-branded clothing delivered each of the intervention sessions. The classroom component included group/class discussions and activities and centred around the completion of tasks in a workbook provided for each child; workbooks were produced specifically for the programmes, such that their structure and content directly complemented the delivery of the sessions. Where possible, materials such as videos featured players from the football team. The PA component involved various games and challenges including football, handball, tag-style games and activities such as passing a ball alternately over and under members of the group; these aimed to encourage movement, balance, agility and speed, and incorporated teamwork through regularly asking pupils to take part in group or paired tasks. School and intervention staff reported links between the classroom and PA content, for example that when the association between PA and heart rate was explained in the classroom, the PA session asked children to check their pulses before and after their PA participation. The planned structure for the sessions was for the PA component to take place after the classroom component but again researcher observation and the reports of intervention staff established that children took part in the PA first when this was practical for timetabling reasons, for instance
when two classes from a school were taking part in a programme simultaneously and changed over between the classroom and PA aspects at the halfway point.
Intervention outcomes were monitored by the football club foundation through a comparison of pupils’ performance during the first and final sessions of the programmes on: i) a multiple-choice quiz, measuring their knowledge of nutrition and PA or discrimination – a mode of assessment in line with the recommendations of the PSHE Association (2017) – and ii) walking and balance tests, measuring their physical fitness.
A second intervention was additionally investigated in Study 4. It had been intended for this intervention to be the focus of the thesis but this unfortunately became impossible due to its replacement with separate PSHE and PE programmes. While this very occurrence demonstrates the need to consider issues around sustainability (e.g. the funding and potential adaptation of programmes) in any analysis of intervention delivery, the inclusion of two interventions in Study 4 did allow for the exploration of stakeholders’ views of classroom/PA-format PSHE programmes more broadly. Where recommendations are made for intervention development, these are still expressed in the plural as those responsible for the design and delivery of the second intervention may reinstate it in the future.
The second intervention was also provided by a football club foundation, ran for 6 weeks and consisted of classroom and PA components, but its sessions were shorter at approximately 30 rather than 60 minutes per component. The researcher observed that the sessions were generally delivered by a single facilitator, with the classroom activities preceding the PA. Intervention facilitators reported that on occasion, for instance if the school hall was in use and the weather was poor, they would run two classroom sessions back-to-back and compensate for this by providing a 60-minute PA session the following week.
By following one of a number of workbooks with an assortment of themes, the second intervention model again contained a series of programmes. These aimed to challenge the attitudes and perceptions of young people towards issues including self-esteem, substance misuse and racism. Classroom activities were of a similar pupil-centred
nature to those in the intervention described above, and the PA was observed by the researcher and reported by participants in Study 4 to include football, tag-style games and coordination challenges. Facilitators linked PA to classroom content through offering examples such as for the children to consider how success affected their self-esteem. As in the first intervention, a quiz was employed at the beginning and end of the programmes to measure improvements in pupils’ knowledge but there was no physical fitness test because the focus of the intervention was on children’s understanding of the PSHE content.
Although neither of the interventions was explicitly based on theory, it became apparent during the Study 4 interviews that some behaviour change techniques were employed. These are considered in Chapter 8.
1.4 Intervention Participation and Physical Activity
Even when the primary aim of an intervention programme was to support children in making positive choices (e.g. resisting peer pressure), the inclusion of a PA component and encouragement of a healthy lifestyle meant that both interventions additionally went some way to addressing an issue of recent concern in the UK: that of physical inactivity and its consequences. This was a particular goal of the first intervention, which explicitly aimed to promote increased PA participation and to increase children’s confidence in participating in PA. With such emphasis being placed upon children’s activity by the main intervention in the research programme (investigated in Studies 2, 3 and 4), one of the themes running throughout the thesis is on PA and its promotion to schoolchildren.
At the time of the research, UK PA guidelines recommended that all 5–18-year-olds took part in at least 60 minutes – and up to several hours – of moderate-to-vigorous intensity physical activity (MVPA) every day, defined as activity that raises one’s temperature, heart rate and breathing rate (Department of Health and Social Care, 2011). Although the need for daily engagement in PA has been called into question because it is not yet known whether there are greater benefits to participation in 1 hour of activity every day as compared to 7 hours of activity distributed unevenly over the course of a week (Janssen & LeBlanc, 2010) – which is one of the factors being
considered in the current review of the PA guidelines (Foster, 2018) – it is generally acknowledged that children are not as active as they should be. The exact figures vary but tend to indicate that less than 50% of children in England meet the activity guidelines (Health and Social Care Information Centre, 2015) and show that boys spend significantly more time in MVPA than girls (e.g. van Sluijs et al., 2008). Furthermore, it is well recognised that there is a decline in PA with age (e.g. Sallis, 2000). A recent longitudinal study in which the habitual PA of participants from the North East of England was measured via accelerometry between the ages of 7 and 15 years demonstrated that total volume of PA (from light to vigorous intensity) declined for both males and females across this period; this objectively-measured, contemporary finding of a childhood reduction in PA being contrary to the prevailing view that there is a dramatic decline in PA in adolescence, particularly for females (Farooq et al., 2018). The same study indicated a reduction in MVPA between the ages of 7 and 15 years for most participants.
It may be difficult for some young people to engage in 60 minutes of MVPA per day, with lack of time having long been recognised as a barrier to PA participation (e.g. National Center for Chronic Disease Prevention and Health Promotion and Centers for Disease Control and Prevention, 1997). However, including opportunities for PA participation within school hours – as in the intervention sessions – reduces the onus on self- or parent-directed PA and may make the goal seem more attainable. On the other hand, 8–9-year-olds from Essex were found to spend on average only 9.5% of their time in PE lessons in MVPA (Wood & Hall, 2015), so if interventions are to contribute to children meeting the PA recommendations then it is important that participants are sufficiently active during the sessions.
The main limitation of the interventions in increasing children’s MVPA is that the PA component of the sessions lasts for only 30–60 minutes per week. On the other hand, as acknowledged in articles such as Fox, Cooper and McKenna (2004) and Gortmaker et al. (1999), school-based interventions are able to reach almost all of the target population and – perhaps because they have the potential to increase children’s PA self-efficacy, where low self-efficacy is another well-recognised barrier to PA participation (Bandura, 1977) – school-based PA sessions appear to encourage children’s PA participation at other times in the day.
Studies into interventions promoting physical activity in primary school settings have however reported mixed results in relation to PA outcomes. For instance, the ‘Be Smart’ intervention, designed to prevent obesity and based on the principles of social learning theory, was delivered over four school terms to groups of 5–7-year-old children in Oxford to promote PA alone, nutrition alone or PA and nutrition combined. Intervention participation did not affect children’s PA patterns outside of school, as reported in questionnaires completed by their parents, despite the intervention having both school- and family-based components (Warren, Henry, Lightowler, Bradshaw & Perwaiz, 2003). Similarly, the year-long ‘Active Programme Promoting Lifestyle Education in Schools’ (APPLES) was delivered to 7–11-year-olds in Leeds in a whole-school approach which included environmental changes (e.g. whole-school lunches) and playground activities, and no difference in self-reported PA was found between children from intervention schools and children from control schools (Sahota et al., 2001). Intervention children did however show higher levels of knowledge and understanding of the health benefits of diet and PA in end-of-year focus groups with facilitators who were blind to the schools’ intervention status.
Counter to the above evidence, the more recent ‘Sport for LIFE’ healthy lifestyle intervention for 8–9-year-olds in Northern Ireland led to significant increases in light, moderate and vigorous intensity PA between baseline and the conclusion of the programme, measured via accelerometry (Breslin, Brennan, Rafferty, Gallagher & Hanna, 2012). This 12-week programme was based on elements of social cognitive theory, with sports outreach officers and class teachers delivering lessons of 1 hour per week covering the topics of nutrition, indoor/outdoor games and the effects of PA on health. The programme culminated in a PA festival attended by an Olympic gold medal winning guest. Another study used accelerometry to measure the outcomes in the North East of England of the ‘GreatFun2Run’ intervention, again based on social cognitive theory but this time running over the course of 10 months and supplemented with a local media campaign and an interactive website for pupils, teachers and parents (Gorely, Nevill, Morris, Stensel & Nevill, 2009). The 7–11-year-old participants in intervention schools increased their total time in MVPA by 9 minutes per day while those in control schools decreased this time by 10 minutes per day; a significant difference between the groups.
As can be seen from even this short summary, it can be difficult to draw comparisons across studies due to the heterogeneity of intervention formats and outcome measures used, a matter discussed throughout the thesis. Despite the mixed findings, the
‘Everybody Active, Every Day’ framework (Public Health England, 2014a) recommends the increased use of professionals and volunteers outside of the field of health to drive PA participation, including those in education. Speaking to the difficulty discussed earlier concerning limited time in the school day, publication of the framework was closely followed by a briefing for staff in education settings on
‘The link between pupil health and wellbeing and attainment’ (Public Health England, 2014b). This emphasised the value of promoting health for children’s social and emotional development and for their academic achievement, as an outcome especially likely to appeal to school staff. In a similar vein, Bailey, Hillman, Arent and Petitpas (2013) noted that “the physical health outcomes of regular exercise… are so compelling and urgent that they are in danger of excluding other outcomes” (p. 302), their Human Capital Model by contrast encompassing a total of 88 benefits of PA from the literature including wellbeing and education-related outcomes such as improved self-esteem, the development of prosocial behaviour, improved concentration and higher academic assessment scores.
It is possible that the interventions under investigation in this research programme are especially well-positioned to aid academic achievement by not only addressing PSHE issues which would be expected to improve children’s wellbeing and potentially therefore their achievement, but by additionally including a PA component with complementary benefits. Furthermore, it was raised as recently as April 2018 at the Fuse Physical Activity Group Workshop for academics and practitioners in the field of PA promotion that much of the research in this area investigates interventions designed specifically for the purposes of the research studies, rather than exploring existing interventions. As the current research programme reflects intervention provision as it naturally occurs in school settings, it therefore makes a valuable contribution to the evidence base.
1.5 Overview of the Thesis
The thesis contains nine chapters: in addition to the background context presented in the current chapter, there is a literature review (Chapter 2), details of the methodology (Chapter 3), the chapters reporting on each of the individual studies (Chapters 4, 6, 7 and 8, with Chapter 5 providing an account of the general methods for Studies 2 and 3), and finally the general discussion, integrating the findings from across the research programme (Chapter 9). By way of an overview of the developing argument throughout the thesis, the rationale and research questions/aims and hypotheses for each of the individual studies are given below, with Figure 1.1 providing a visual representation of the programme of work. Literature supporting the hypotheses is presented in Chapter 2.
Figure 1.1. Summary of the programme of work
Study 1: The creation and reliability and validity testing of CogS: 9–11, a cognitive test battery for researchers working with 9–11-year-olds in school settings.
Rationale: Studies 2 and 3 were to involve an assessment of children’s cognitive performance as a possible outcome of participation in a PSHE intervention delivered via classroom learning and PA participation, but the tools used to measure cognitive performance in past research have differed from study to study, making it difficult to compare results. Study 1 therefore set out to design and to assess the reliability and validity of a pilot cognitive test battery suitable for research with upper-Key Stage 2 pupils in a whole-class testing situation. The four alternate forms of the resultant Cognition in Schools: 9–11-year-olds (CogS: 9–11) test battery would be employed
in the repeated measures testing in Studies 2 and 3, and in the long-term it is hoped that CogS: 9–11 will be further developed in order to provide researchers with an instrument for regular use in studies into cognitive performance with 9–11-year-olds in school settings.
Aim: To assess the parallel forms reliability, test–retest reliability and construct validity of the pilot CogS: 9–11 test battery.
Hypotheses:
1. There will be no significant difference in the performance of 9–11-year-old children on each of the seven cognitive tests between the four alternate versions of the CogS: 9–11 test battery, demonstrating parallel forms reliability; 2. There will be no significant difference in the performance of 9–11-year-old
children on each of the seven CogS: 9–11 tests between the first and second testing sessions, conducted 1–2 weeks apart, demonstrating test–retest reliability; and
3. In principal component analysis, children’s scores for the seven CogS: 9–11 tests will load onto four components representing processing speed, attention, long-term memory and executive function, demonstrating construct validity.
Study 2: The effects of acute physical activity participation during classroom- and physical activity-based intervention sessions on children’s cognitive performance.
Rationale: Research suggests there may be positive effects of acute PA on cognition (Chapter 2), and due to the relationship between cognitive performance and academic achievement any effects of an intervention on cognition are likely to be of interest to school staff and other intervention/education stakeholders. Children’s cognitive performance was therefore assessed immediately following their participation in the PA component of one of the intervention sessions – or following a normal classroom lesson for the control group – in relation to pretest measurements. The duration and intensity of PA in which children engaged during the PA session was also recorded via accelerometry to explore the role of PA more deeply than simply participation/non-participation, with a positive relationship being anticipated between time spent in MVPA and post-PA cognitive performance, accounting for pretest cognitive performance.
Aim: To assess the effects of participation in the PA component of one of the intervention sessions – as an acute bout of PA – on children’s cognitive performance, assessing cognitive performance in comparison with a control group and in relation to pretest measurements.
Hypotheses:
1. Participants’ cognitive performance – recorded as scores for the CogS: 9–11 test battery – will improve to a significantly greater extent from pretest following participation in an acute bout of PA (PA group) than following a normal classroom lesson (classroom group); and
2. Accounting for prettest scores, there will be significant positive correlations between time spent by children in MVPA during the PA component of the intervention session and their post-PA cognitive performance scores.
Study 3: Children’s wellbeing, cognitive performance and academic achievement following participation in a combined classroom learning and physical activity intervention.
Rationale: The literature indicates that primary school teachers are under pressure to prioritise core curriculum subjects in the school timetable, the reason for this appearing to be the argument that more time spent in lessons focused on these subjects will correspond with children’s greater educational achievement in core areas of learning. Reading, writing and mathematics are key aspects of the primary school performance tables for England and it is easy to see why the school day can become concentrated on these subjects. However, if participation in other aspects of the curriculum is shown to boost educational achievement – or at least not to have a detrimental impact upon it – then this would support practice and policy concerning the provision of a varied timetable potentially offering additional outcomes such as improved wellbeing. Study 3 constituted an investigation of the same PSHE intervention as Study 2 but from a chronic perspective. Quantitative data were gathered regarding the cognitive performance, academic achievement and wellbeing of intervention and control children, it being more reasonable to expect changes in academic achievement and wellbeing over the course of a complete intervention than in an acute study. As
described further in Chapter 2, there is evidence suggesting that benefits for these three constructs might be anticipated from PSHE and/or PA participation; however, research tends to be restricted to measuring a limited number of variables, with studies of PSHE interventions tending to favour outcomes pertaining to subject-specific knowledge and studies of PA interventions most frequently measuring post-intervention PA participation. It is also common for studies to investigate post-interventions delivered in schools for the purposes of the research as opposed to provision as it is currently occurring, whereas Study 3 represented an opportunity to investigate an intervention unusually combining PSHE and PA elements and already taking place in primary school settings.
Aim: To examine children’s cognitive performance, academic achievement and wellbeing following participation in a 6-week school-based PSHE intervention delivered via classroom learning and PA, assessing these variables in comparison with a control group and in relation to pretest measurements.
Hypotheses:
1. There will be a significantly greater increase from pretest to posttest in the wellbeing scores (physical wellbeing, psychological wellbeing, wellbeing pertaining to peers and social support, and wellbeing pertaining to the school environment, measured via the KIDSCREEN-27 questionnaire; Ravens-Sieberer et al., 2005; The KIDSCREEN Group Europe, 2006) of intervention participants compared to control participants;
2. There will be a significantly greater increase from pretest to posttest in the cognitive performance (scores for the seven CogS: 9–11 tests) of intervention participants compared to control participants; and
3. There will be a significantly greater increase from pretest to posttest in the academic achievement (reading, writing and mathematics scores, as tracked via school assessment systems and reported by class teachers) of intervention participants compared to control participants.
Pilot Study (Study 3a): In addition to the above measurements, a small number of participants were asked to wear accelerometers to record their physical activity for 9 days at pretest and posttest. This allowed for a preliminary investigation into whether
intervention children increased their MVPA levels to a greater extent than control children, with such an increase being one mechanism via which intervention participation might lead to any improvements in cognitive performance, academic achievement and wellbeing. It was hypothesised that there would be a significantly greater increase from pretest to posttest in the percentage of time spent in MVPA by intervention participants compared to control participants.
Study 4: The views of stakeholders on combined classroom learning and physical activity PSHE interventions for schoolchildren: A thematic analysis.
Rationale: Conducted concurrently with Studies 2 and 3, the purpose of Study 4 was to explore the views of stakeholders (children, parents/guardians, school staff and intervention staff) in relation to primary school-based PSHE interventions delivered via classroom learning and PA participation. An appreciation of the value placed particularly by parents/guardians and children upon PSHE/PA interventions and their outcomes would support school staff in making decisions about the inclusion of such PSHE and PA opportunities in the school day, consistent with the goals of Studies 2 and 3. The qualitative data gathered on the interventions would also provide contextual information regarding the outcomes investigated in the quantitative studies, as factors such as whether participants buy into the combined classroom learning and PA format and the extent to which children engage in the sessions are likely to influence intervention outcomes. In addition, stakeholders were asked questions relating to the likely continued provision of the interventions because recommendations for their future development would be informed by their anticipated sustainability.
Research Questions: What are the views of stakeholders on: 1. The role of PA in the interventions?
2. Children’s engagement in the sessions? 3. The outcomes of intervention participation? 4. The sustainability of intervention delivery?
Chapter 2: Literature Review
As indicated in Chapter 1, the outcomes of children’s participation in PSHE and PA programmes are anticipated to extend beyond improvements in subject knowledge and physical health. A child’s wellbeing in areas additional to physical health, for instance in relation to their psychological wellbeing and interactions with others, would be expected to improve as a result of their understanding of concepts such as self-esteem and development of their ability to work in a team. Indeed, wellbeing is at the centre of PSHE delivery in schools and pupils’ wellbeing is further promoted through the provision of opportunities for PA participation. However, of particular note to education stakeholders following pupils’ participation in school-based programmes of any variety are likely to be any benefits for children’s learning, for example achievement in core curriculum subjects and cognitive processes supportive of the completion of classroom activities.
This chapter presents a review of the literature pertaining to the relationships between each of the four main constructs explored in the quantitative arm of the research programme: cognitive performance, academic achievement, wellbeing and physical activity, providing a background as to why positive associations might be expected between participation in a classroom/PA-format PSHE intervention and children’s cognitive performance and academic achievement if such an intervention were to improve participants’ wellbeing and increase their PA as anticipated. Study 3 investigates cognitive performance, academic achievement and wellbeing as potential outcomes of children’s participation in a PSHE/PA intervention, with the focus of Study 2 being the more immediate effect of the PA component of the intervention on cognitive performance. The chapter concludes with a discussion of research into stakeholders’ views on PSHE and PA interventions from a feasibility and acceptability perspective, for instance considering children’s engagement in intervention sessions as one of the matters of interest in the qualitative arm of the research programme. 2.1 Definitions of Key Constructs in the Thesis
of the key terms has been applied in the thesis. There have been inconsistencies in the definitions of constructs in the literature and differences in the application of terms are highlighted where appropriate in the literature review as discrepancies constitute possible reasons for conflicting results.
2.1.1 Defining Cognitive Performance
Although the description, categorisation and assessment of different aspects of cognitive performance is still the subject of much debate, which has unfortunately complicated the research in this area (Best & Miller, 2010), this thesis will focus on the cognitive domains of processing speed, attention, executive functioning and long-term memory (LTM), defined as outlined below. These are domains recognised – often under different names – in the literature in cognitive psychology and neuropsychology (e.g. Reisberg, 2007), which additionally refers to elements such as knowledge and expertise. They were selected due to their likely roles in school learning, for instance in attending and responding to information presented, in working through classroom tasks, and in retaining what has been learnt.
2.1.1.1 Processing Speed
It has been argued that there are two aspects to processing speed: simple speed/reaction time, which concerns basic elements of attention and concentration and which is measured using tasks involving the recognition of and production of motor responses to stimuli; and complex information processing speed, which refers to attention and concentration involving mental manipulations (Chiaravalloti, Christodoulou, Demaree & DeLuca, 2003). The current research sought to capture processing speed in its most fundamental form, with mental manipulations being explored separately (see the ‘Executive Function’ section); while it is therefore simple speed/reaction time which is being measured, this is henceforth referred to as ‘processing speed’ for concision. As with all of the aspects of cognition under investigation, processing speed has been associated with classroom learning, an inverse relationship having been identified between 7–11-year-olds’ reaction time variability and on-task behaviour for a mathematics task mimicking self-directed classwork in a laboratory setting (Antonini, Narad, Langberg & Epstein, 2013).
2.1.1.2 Attention
The definitions for both aspects of processing speed refer to attention, indicating an overlap in these two areas of cognition. A further complication in defining attention is recognised in that there are a variety of forms of attention, with researchers sometimes considering the same task to measure different types; the article by Chiaravalloti et al. (2003), for example, states that the Paced Auditory Serial Addition Test, in which participants add a series of digits presented in sequence, has been referred to as a test of simple attention, attention maintenance and divided attention (used when completing multiple tasks at once), as well as of processing speed. The current research employed a test designed to measure sustained attention, or “the ability to maintain attention on a series of stimuli over a period of time” (Coull, Frith, Frackowiak & Grasby, 1996, p. 1085), and selective attention, which allows a person “to select and focus on particular input for further processing while simultaneously suppressing irrelevant or distracting information” (Stevens & Bavelier, 2012, p. 30). These types of attention were chosen because schoolchildren are routinely tasked with keeping their attention on task throughout a lesson whilst ignoring any distractors.
2.1.1.3 Executive Function
‘Executive function’ is a term used to refer to cognitive processes which pertain to the control and regulation of cognitive subprocesses and behaviour in pursuit of a goal (Banich, 2009; Miyake & Friedman, 2012). Components of executive function include, amongst others: planning; updating and processing information in working memory; shifting between multiple tasks and operations; and inhibiting prepotent responses (Anderson, 2002; Miyake et al., 2000). As with most cognitive functions there are differential uses of terms between papers and potential overlaps with other cognitive domains: it might be argued, for example, that selective attention involves inhibition, but on the other hand sustained and selective attention have been found to be distinct from ‘attention control’ (measured via tasks involving inhibition and switching) in 6–16-year-olds (Manly et al., 2001). This issue is discussed further in Chapter 4.
Executive function develops throughout childhood and adolescence, with implications not only for an individual’s cognitive performance and behaviour but also for their
emotional control and social interactions (Anderson, 2002). It is the cognitive aspect which has been of interest to researchers in the field of physical activity (Etnier & Chang, 2009), particularly with the suggestion that PA has a larger effect on executive function than other cognitive domains, as discussed later in the chapter. In this thesis, the term ‘executive function’ refers specifically to cognitive function; emotional and social functioning are assessed as aspects of wellbeing.
Studies often differentiate between updating, shifting and inhibition as three core dimensions of executive function, though there is some variation of terms particularly for shifting, with researchers using the same tasks sometimes referring to the concept being measured as ‘switching’ or ‘cognitive flexibility’. The three dimensions are notable not just due to their prevalence in the literature but also because they are relevant for classroom learning: updating means pupils can keep the contents of working memory relevant to current tasks by adding new information and deleting now-irrelevant information, shifting allows them to switch between tasks when required, and inhibition helps them to resist distraction (Daly-Smith, McKenna, Defeyter & Manley, 2018). Evidence for the distinction between the dimensions comes from Miyake et al. (2000), although it was later proposed that inhibition plays a role in updating and shifting (Miyake & Friedman, 2012). This is discussed further in Chapter 4.
2.1.1.4 Long-Term Memory
LTM is the system in which information including knowledge, experiences and rules is stored and from which it can be retrieved (Rumelhart, Lindsay & Norman, 1972). Intervention research tends to assess changes in participants’ intervention-related knowledge between the beginning and end of a programme; however, despite the storage and retrieval of information being essential in education, memory has received little research interest in relation to children’s PA, and LTM was thus felt to be an important inclusion in the current work.
LTM has been distinguished from short-term or working memory, a system which contains information relating to the current task for active processing (Baddeley, 2007) and which is therefore considered within the context of executive function in the
current thesis. The two are generally defined by duration, with information thought to be held in working memory for ≤30 seconds before it is lost through decay (Shiffrin & Atkinson, 1969), and information which is to be held for longer than this requiring rehearsal and/or transfer to LTM.
2.1.2 Defining Academic Achievement
On conducting a review of studies into youth PA and academic performance, Castelli et al. (2014) noted a change in terminology in this area, with earlier studies referring to academic behaviours and attitudes and more recent ones referring to academic
achievement. This is suggestive of a narrowing of the focus of research interest to test scores rather than behaviours that support learning (e.g. time spent on-task, completion of homework, school attendance). The current programme of research places a similar emphasis on achievement, while also investigating cognitive performance as a possible supporting factor.
Throughout the thesis, the term ‘academic achievement’ is used when referring to measures such as grades, standards (e.g. ‘working towards the expected standard’, one of the standards in use at the time of the research programme; Standards and Testing Agency, 2017) or quantification of standards in an examination or across a child’s classwork in a specified subject. Although the term ‘attainment’ is also used when referring to test results, ‘achievement’ was favoured with the educational applications of the work in mind because every child’s pretest performance will differ and it is improvement in the subject(s) under study which stakeholders can use as an indication of the value added by an intervention (for a discussion of value-added in education, see Brown, McNamara & O’Hara, 2016).
2.1.3 Defining Wellbeing
Of the four constructs under investigation, wellbeing has been defined in by far the greatest number of ways. There is broad agreement that wellbeing refers to a positive state – rather than simply the absence of problems as it has sometimes previously been understood (Sancassiani et al., 2015) – and that it consists of several dimensions, for instance physical, psychological and social. However, the dimensions of interest often differ from study to study. Further complicating the issue are that an individual’s sense of feeling ‘well’ is by its very nature personal and subjective, and that the expression
‘wellbeing’ has been used synonymously with ‘happiness’, ‘life satisfaction’ and other terms which are undoubtedly related but which have slightly different emphases (McLellan & Steward, 2015). This difficulty may stem from researchers’ varied philosophical standpoints (see Waterman, 1993): some may feel that wellbeing relates to the experience of pleasure (a hedonistic conceptualisation); others may favour an interpretation that wellbeing relates to self-realisation and personal expressiveness (a eudaimonic conceptualisation); and yet others may believe that it incorporates both (e.g. Seligman’s (2011) PERMA model of flourishing, which proposes that wellbeing comprises Positive emotion, Engagement, Relationships, Meaning and Achievement). In the absence of a unified definition of wellbeing, the key for researchers is perhaps to bear in mind the impact they wish to achieve and to ensure that the way in which they conceptualise and measure wellbeing is compatible with their goals and is transparent to the reader. Mashford-Scott, Church and Tayler (2012) identified four major perspectives on wellbeing upon which researchers can draw to explain their positions: social and economic perspective; psychological and mental health perspective; philosophical perspective; and educational perspective. As might be expected, an educational perspective is adopted here. This position is described as exploring learning dispositions and behaviours (e.g. motivation), as concerning social-emotional-behavioural competencies and as being orientated towards the monitoring of affect. Social-emotional-behavioural competencies are however also of interest from a psychological and mental health perspective, meaning this perspective is represented to some extent in the thesis.
2.1.4 Defining Physical Activity
Physical activity is defined as “any bodily movement produced by skeletal muscles that results in energy expenditure” (Caspersen, Powell & Christenson, 1985, p. 126). It should not be confused with exercise, which is a structured form of PA involving the repetition of certain movements in order to improve or maintain one’s physical health or fitness (Dishman et al., 2006). PA consequently encompasses a greater range of activities than exercise, including playing, active transportation (e.g. walking to school) and taking part in recreational activities such as sports (World Health Organization, 2016).