0095-1137/09/$08.00⫹0 doi:10.1128/JCM.01597-08
Copyright © 2009, American Society for Microbiology. All Rights Reserved.
Longer Intestinal Persistence of
Enterococcus faecalis
Compared to
Enterococcus faecium
Clones in Intensive-Care-Unit Patients
䌤
Patricia Ruiz-Garbajosa,
1,2Rosa del Campo,
1,2Teresa M. Coque,
1,2Angel Asensio,
3Marc Bonten,
4Rob Willems,
4Fernando Baquero,
1,2and Rafael Canto
´n
1,2*
Servicio de Microbiología, Hospital Universitario Ramo´n y Cajal, and CIBER en Epidemiología y Salud Pu´blica (CIBERESP), Madrid 28034, Spain1; Unidad de Resistencia a Antibio´ticos y Virulencia Bacteriana, Asociada al Consejo Superior de
Investigaciones Científicas (CSIC), Hospital Ramo´n y Cajal, Madrid 28034, Spain2; Servicio de Medicina Preventiva,
Hospital Universitario Puerta de Hierro, Madrid 28035, Spain3; and Department of Medical Microbiology,
University Medical Center, Utrecht 3584 CX, The Netherlands4
Received 18 August 2008/Returned for modification 4 November 2008/Accepted 25 November 2008
The dynamics of intestinal colonization with enterococcal clones in intensive-care-unit (ICU) patients was evaluated. Eight patients admitted directly to the neurosurgical ICU at the Ramo´n y Cajal University Hospital (Madrid, Spain) from the community and with no overlapping stay during a 10-month period in 2006 were studied. Rectal swab specimens were collected on admission and daily until the patients were discharged. Clonality was determined by pulsed-field gel electrophoresis and multilocus sequence typing. Clonal coloni-zation dynamics were estimated by using two new parameters: the clonal diversity per patient per day (CDPD) and the clonal persistence ratio (CPR).Enterococcus faecalis isolates (n ⴝ 123) andEnterococcus faecium isolates (nⴝ66) were resolved into 13 and 15 clones, respectively. The CDPD ofE. faecalissteadily increased during admission, andE. faecalis showed a higher (P ⴝ0.001) CPR value than E. faecium(0.86 and 0.42, respectively).E. faecium, with the exception of an ampicillin-resistant clone belonging to clonal complex 17, frequently appeared as a short-term colonizer, even though theE. faecalisclones had significantly (Pⴝ0.03) more days under antibiotic exposure thanE. faecium(77.5 and 65 days/100 colonization days, respectively).E. faecalishad a longer persistence thanE. faecium, except for the CC17 ampicillin-resistant clone, andE. faecalis showed a cumulative increase in CDPD, whereasE. faeciumdid not. CDPD and CPR were useful for measuring the dynamics of intestinal colonization with enterococcal clones.
Intensive care units (ICUs) are hospital compartments that present the highest frequencies of nosocomial infection with multiresistant bacteria due to the combination of the presence of seriously ill patients, frequent events of cross transmis-sion, and high levels of antibiotic pressure. Enterococci have emerged as a significant cause of nosocomial infections, caus-ing about 7% of infections among ICU patients (28). Tradi-tionally, enterococcal infections were thought to be of endog-enous origin, but modern typing systems have permitted the identification of genotypes that are well adapted to the hospital setting and that are frequently cross transmitted. Population structure studies based on multilocus sequence typing (MLST) data forEnterococcus faecalis(25) andEnterococcus faecium
(14), the enterococcal species most often isolated from clinical infections, have revealed the existence of particular clonal complexes (CCs) that are frequently selected in the hospital environment. These CCs have been named high-risk CCs (HrCCs), as they are the cause of most enterococcal infections and hospital outbreaks all over the world (18).
Bacterial persistence in hosts constitutes an important factor driving both bacterial transmission and infection. Different studies that have focused on the longitudinal follow-up of patients colonized with multiresistant enterococci, especially
vancomycin-resistant isolates, demonstrated the prolonged persistence of vancomycin-resistant enterococci in the intesti-nal tract of hospitalized patients (3, 22). Exposure to extended-spectrum cephalosporins and long ICU or hospital stays are commonly associated with prolonged colonization with multi-drug-resistant enterococci (2, 4). Studies that have focused on the dynamics of colonization with enterococci have demon-strated a trend for the increased acquisition of resistant geno-types and cross-transmission episodes during patients’ hospi-talizations (11, 21). However, prospective studies on the persistence of specific enterococcal clones and the colonization dynamics during patients’ ICU stays are still lacking. The same is true for the investigation of differences in persistence among
E. faecalisandE. faeciumclones, both multiresistant and non-multiresistant ones. To address these points, we designed the present study to evaluate the dynamics of the enterococcal clonal populations in the intestinal compartment of ICU pa-tients and introduced new indexes that can be used to measure bacterial persistence.
MATERIALS AND METHODS
Patients and study design.The Ramo´n y Cajal University Hospital is a 1,100-bed university hospital in Madrid, Spain. The study was conducted in the neu-rosurgical ICU (N-ICU) over 10 months in 2006. The N-ICU has eight beds, and during the time of the study, the occupancy rate was 0.81 and the rotation rate was 0.71. The nurse/patient ratio was 0.46. Patients were included in the study if
they met all of the following criteria: (i) they wereⱖ18 years of age; (ii) they had
an expected length of stay (LOS) of⬎4 days (which is longer than the average
for this ICU); (iii) they were admitted to the N-ICU directly from the community setting due to an acute trauma; (iv) they had had no previous admissions to other * Corresponding author. Mailing address: Servicio de
Microbi-ología, Hospital Universitario Ramo´n y Cajal, Madrid 28034, Spain. Phone: 34913368330. Fax: 34913368809. E-mail: rcanton.hrc@salud .madrid.org.
䌤Published ahead of print on 3 December 2008.
345
on May 16, 2020 by guest
http://jcm.asm.org/
ICUs and/or hospital wards during the previous 3 months or during the same hospitalization period in another ICU or ward of the hospital; (v) they had no previous stay in day care centers; and (vi) there was no overlap in time with another patient already included in the study, in order to avoid biases in clonal composition due to direct patient-to-patient transmission. Rectal swab speci-mens were collected from each patient on admission and daily until they were discharged from the N-ICU. Medical records were reviewed; and the following information was collected: sex, age, reason for admission, LOS, previous hospital admissions, and antibiotic therapy during the hospitalization. The study was approved by the local ethics committee.
Sampling.The rectal swab specimens were suspended in 1 ml of saline; and
aliquots of 100l were seeded on m-Enterococcus agar (Difco, Detroit, MI)
plates with and without 125g/ml of gentamicin, 256g/ml of kanamycin, 512
g/ml of streptomycin, 4g/ml of tetracycline, 6g/ml of vancomycin, 2g/ml
of erythromycin, and 10g/ml of ampicillin. Five colonies of each different
morphology were subcultured from each agar plate with and without antibiotics. In order to reduce duplicate isolates, all colonies recovered were newly seeded on the antibiotic plates described above to determine the resistance phenotype. Only one colony of each resistance phenotype and morphology was finally se-lected for further analysis.
Bacterial identification and susceptibility testing.Identification ofE. faecalis andE. faeciumwas performed by amplification of species-specific genes coding
for EfaA and and AAC(6⬘)-Ii, respectively (6). OtherEnterococcusspecies were
identified by using API Rapid galleries (bioMe´rieux, la Balme les Grottes,
France). Antibiotic susceptibility testing was performed by the standard microdi-lution technique, and the results were interpreted according to the guidelines of the CLSI (5).
Clonal diversity analysis.Clonal relatedness was established by pulsed-field
gel electrophoresis (PFGE) (6). One representative strain of each one of theE.
faecalisandE. faeciumPFGE types was further studied by MLST (14, 25). Sequence types (STs) were assigned according to the STs in the MLST database (http://www.mlst.net). The PFGE patterns were interpreted by using the criteria suggested by Tenover et al. (30), with isolates with closely related patterns (no more than three bands of difference) being designated as belonging to a single
clone. The genetic diversity (GD) of theE. faecalisandE. faeciumpopulations
was expressed as the ratio of distinguishable PFGE and MLST genotypes among the total number of recovered isolates. A hospital-acquired clone was defined as a strain that was first isolated more than 48 h after patient admission to the ICU and that was absent in the admission culture samples. An endogenous patient clone was defined as a strain isolated at admission or during the first 48 h of the hospital stay.
Clonal colonization parameters.Two new parameters were designed to
eval-uate the dynamics ofE. faecalisandE. faeciumclonal colonization among the
N-ICU patients. Both of them are ecological parameters, in which the sequen-tially enrolled patients serve as successive observation points for clonal persis-tence in the N-ICU environment. The first parameter was the clonal diversity per patient per day (CDPD), expressed as the number of clones detected per day divided by the number of patients per day, and was computed for every single day of the hospital stay for all patients under observation. Changes in this ratio
describe variations in the genetic diversity of theE. faecalisandE. faecium
isolates from N-ICU patients across their hospitalizations. The second parame-ter, the clonal persistence ratio (CPR), expresses the ratio of the number of days in which a specific clone was found to colonize a patient to the number of hospitalization days since the first positive culture with that specific clone.
Clonal selective antimicrobial exposure.The antimicrobial treatment that every patient received might influence the enterococcal clonal diversity and/or persistence. The number of days that antimicrobial agents were administered among the N-ICU patients was calculated, and the results were expressed as the number of days of antimicrobial exposure per 100 colonization days for individ-ualE. faecalisorE.faeciumclones and for the total number of clones of both enterococcal species identified. Furthermore, antimicrobial agents were divided into effective and ineffective categories, according to their corresponding
intrin-sic and in vitro activities against everyE. faeciumandE. faecalisclone. The
numbers of days of exposure to effective and ineffective antimicrobials per 100
colonization days for theE. faecalisandE. faeciumclones were also calculated.
When a patient received simultaneous therapy with an effective antimicrobial and an ineffective antimicrobial, the combination was considered effective against enterococci.
Statistical analysis.Categorical variables were compared by the2test, while
the mean CDPD indexes were compared by the pairedttest. Linear regression
and the Spearman coefficient were used to correlate CDPD and the length of hospitalization. All tests of significance were two tailed and were set at 0.05. Mean values are reported with standard deviations.
RESULTS
Patient characteristics.Eight patients (five females) with a mean age of 50.6⫾18.6 years (age range, 26 to 88 years) were enrolled during the study period (one patient per month). The mean LOS in the N-ICU was 12.2⫾4 days (LOS range, 7 to 17 days). None of the patients were hospitalized at the same time, and all patients were admitted directly to the N-ICU because of subarachnoidal hemorrhage and/or head trauma. Two of eight patients (patients 1 and 8) had already been hospitalized 12 and 5 months before their N-ICU admissions, respectively. The previous admissions were in medical or sur-gical wards.
Bacterial isolates and genetic diversity.Two hundred eight enterococcal isolates (123 E. faecalis isolates, 66 E. faecium
isolates, 17Enterococcus avium isolates, and 2 Enterococcus casseliflavus isolates) were recovered from 100 rectal swab specimens from the eight patients according to the stated cri-teria. All swabs contained enterococcal isolates. These isolates were grouped into 32 PFGE types (13 forE. faecalis, 15 forE. faecium, 3 for E. avium, and 1 forE. casseliflavus) (Tables 1 and 2). The PFGE patterns for isolates from the same patient were nearly stable during the observation time, as only two clones, E. faecalis 3 (Efc-3) (ST17) and Efc-4 (ST16), pre-sented two different PFGE patterns (differences of one or two bands) and coexisted in the same patient on the same day.E. faecalisisolates belonging to each PFGE type corresponded to 13 different STs (Table 1).E. faecium isolates belonging to each PFGE type corresponded to 14 different STs, since theE. faecium13 (Efm-13) and Efm-19 PFGE types were grouped in ST32 (Table 2). Among theseE. faeciumPFGE types, only one ampicillin-resistant clone (Efm-6, ST18) belonged to the pre-viously described cloneE. faeciumHrCC17 (4) (Table 2). The GDs determined by using the results of PFGE were higher for theE. faeciumpopulation (GD⫽0.23) than for theE. faecalis
(GD ⫽ 0.11) and the E. avium (GD ⫽ 0.18) populations. The GDs were similar forE. faecium (GD ⫽ 0.21) and E. faecalis(GD⫽0.11) when MLST data were used.
Dynamics of enterococcal clonal colonization.E. faecalisand
E. faeciumclones were detected in all patients with the excep-tion of patient 4, who was colonized only byE. faecium. The numbers of enterococcal populations between the patients var-ied considerably, such that the number of clones detected ranged from 2 (in patients 4, 6, and 7) to 15 in patient 2. Three
E. faecalisclones (clones Efc-1 [ST44], Efc-3 [ST17], and Efc-4 [ST16]) (Table 1) and fiveE. faecium clones (clones Efm-6 [ST18], Efm-7 [ST22], Efm-14 [ST228], Efm-21 [ST289], and Efm-22 [ST416]) (Table 2) were isolated from different pa-tients, whereas all threeE. aviumclones were detected only in patient 5 and theE. casseliflavus clone was detected only in patient 8.
Six of the 13E. faecalisclones (46%) were acquired during the patient’s N-ICU admission. Clone Efc-3, which belonged to HrCC9 (18), was acquired by patients 1 and 2. Clone Efc-4, which corresponded to ST16, was acquired by patients 1 and 2 and was found to be endogenous in patients 5 and 8 (Table 1). Among the 15E. faeciumclones, 9 of them were considered acquired (60%). Clone Efm-6, which belonged to HrCC17 (18), was isolated from patient 1 from the beginning of the N-ICU stay, whereas it was acquired by patient 5 (Table 2).
on May 16, 2020 by guest
http://jcm.asm.org/
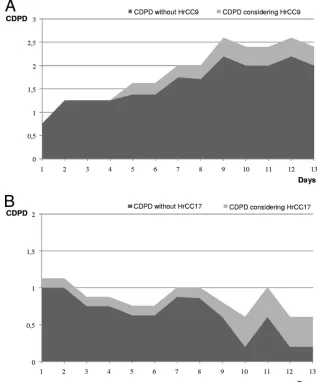
CDPD.On average, we observed a higher index of CDPD forE. faecalis(1.74) than forE. faecium(0.85). Furthermore, throughout the hospitalization period the CDPD showed a statistically significant positive trend forE. faecalis(regression coefficient⫽0.089; 95% confidence interval⫽0.071 to 0.955;
r2 ⫽ 0.51), while this trend was negative forE. faecium (re-gression coefficient ⫽ ⫺0.031; 95% confidence interval ⫽
⫺0.025 to⫺0.037;r2⫽0.53). Furthermore, the CDPD among the E. faecalis isolates increased, irrespective of whether HrCC9 was included. In contrast, the CDPD among theE. faeciumisolates increased only when HrCC17 was included in the analysis (Fig. 1).
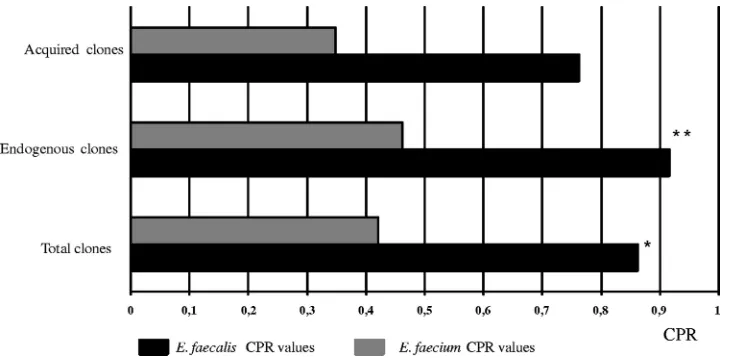
CPR. The CPR value was significantly higher for the E. faecalisclones (0.86) than for theE. faeciumclones (0.42) (P⫽
0.001) (Fig. 2). During the study period and by considering the entire patient population, theE. faecalisclones accounted for 169 colonization days, whereas the E. faecium clones ac-counted for 80 colonization days. The mean numbers of colo-nization days per clone were 13⫾12.6 and 5.3⫾ 5.35 days, respectively. The pooled CPR was significantly (P ⫽ 0.001) higher for endogenous E. faecalis clones (0.92) than for endogenous E. faecium clones (0.46) (Fig. 2). Endogenous E. faecalisclones, detected from the beginning of the N-ICU stay, were able to persist for 120 colonization days, which represents an average of 15⫾9.25 colonization days per clone. This value was 56 days forE. faecium, with an average of 7⫾3.9 coloni-zation days per clone. No statistically significant differences in pooled CPRs were found among the acquiredE. faecalis(0.75) and E. faecium (0.35) clones, with the average numbers of colonization days being 8 ⫾ 8.5 and 2.6⫾ 2.6, respectively. Nevertheless, a clear tendency was observed. Nine of 13E. faecalis clones were recovered almost every day during the study period and thus had CPR values of 1 or nearly 1 (Table 1). On the other hand, only oneE. faeciumclone, which cor-responded to HrCC17, showed a CPR value of 1 (Table 2).
Clonal selective antimicrobial exposure.All patients except patient 4 received systemic antimicrobial therapy; patient 4 did not receive any antimicrobial agent during the N-ICU stay. Monotherapy was administered to seven patients, and three of these seven patients also received antimicrobial combinations. These combinations are shown in Table 1 and 2.
Overall, per 100 days of colonization withE. faecalisclones, patients received 77.5 days of antibiotic treatment. The corre-sponding value was significantly (P⫽0.03) lower (65 days) for
E. faeciumclones. The number of days with ineffective selec-tive antimicrobial exposure was slightly higher forE. faecium
than forE. faecalis(46% of the colonization days forE. fae-ciumand 33% forE. faecalis;P⫽0.04). In general, the number of days under effective antimicrobial exposure was higher for
E. faecalis(44%) than forE. faecium(19%) (P⫽0.0001). The threeE. faecalisclones detected in more than one pa-tient were obviously challenged by the highest antibiotic pres-sure: Efc-1 (ST44), Efc-3 (ST17), and Efc-4 (ST16) had 13.6, 10.6, and 21.3 days of antibiotic exposure per 100 colonization days, respectively (Table 1). The clones persisted, despite ex-posure to effective selective antibiotics. This was true not only for multiresistant clones, like Efc-3 (ST17, HrCC9) and Efc-4 (ST16), which were partly exposed to effective antibiotics (5 effective days versus 6 ineffective days/100 colonization days for Efc-3 and 14 effective days versus 7 ineffective exposure days/
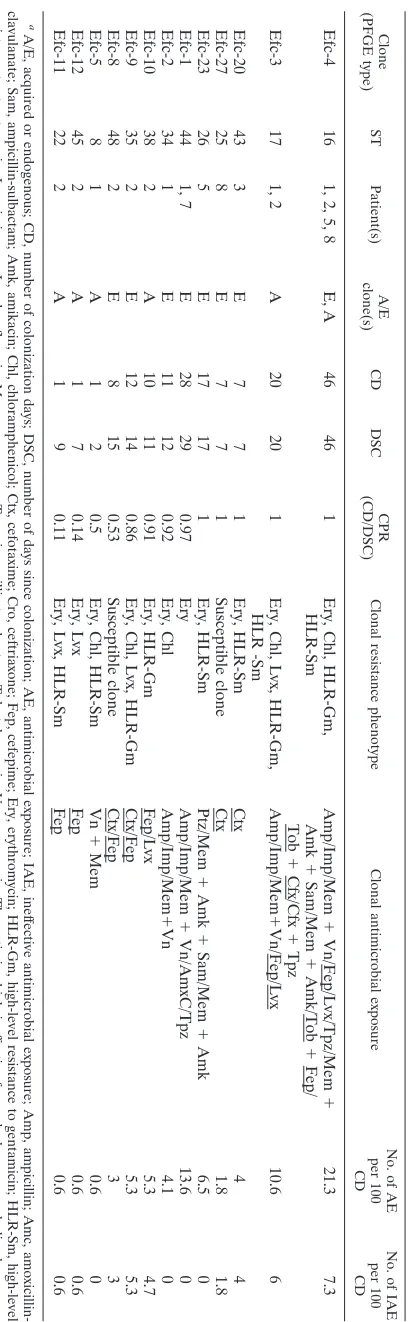
TABLE 1. Characteristics of E. faecalis clones a Clone (PFGE type) ST Patient(s) A/E clone(s) CD DSC CPR (CD/DSC) Clonal resistance phenotype Clonal antimicrobial exposure No. of AE per 100 CD No. of IAE per 100 CD Efc-4 16 1, 2, 5, 8 E, A 46 46 1 Ery, Chl, HLR-Gm, HLR-Sm Amp/Imp/Mem ⫹ Vn/Fep/Lvx/Tpz/Mem ⫹ Amk ⫹ Sam/Mem ⫹ Amk/Tob ⫹ Fep/ Tob ⫹ Cfx/Cfx ⫹ Tpz 21.3 7.3 Efc-3 17 1, 2 A 20 20 1 Ery, Chl, Lvx, HLR-Gm, HLR -Sm Amp/Imp/Mem ⫹ Vn/Fep/Lvx 10.6 6 Efc-20 43 3 E 7 7 1 Ery, HLR-Sm Ctx 44 Efc-27 25 8 E 7 7 1 Susceptible clone Ctx 1.8 1.8 Efc-23 26 5 E 17 17 1 Ery, HLR-Sm Ptz/Mem ⫹ Amk ⫹ Sam/Mem ⫹ Amk 6.5 0 Efc-1 44 1, 7 E 28 29 0.97 Ery Amp/Imp/Mem ⫹ Vn/AmxC/Tpz 13.6 0 Efc-2 34 1 E 11 12 0.92 Ery, Chl Amp/Imp/Mem ⫹ Vn 4.1 0 Efc-10 38 2 A 10 11 0.91 Ery, HLR-Gm Fep/Lvx 5.3 4.7 Efc-9 35 2 E 12 14 0.86 Ery, Chl, Lvx, HLR-Gm Ctx/Fep 5.3 5.3 Efc-8 48 2 E 8 15 0.53 Susceptible clone Ctx/Fep 33 Efc-5 8 1 A 1 2 0.5 Ery, Chl, HLR-Sm Vn ⫹ Mem 0.6 0 Efc-12 45 2 A 1 7 0.14 Ery, Lvx Fep 0.6 0.6 Efc-11 22 2 A 1 9 0.11 Ery, Lvx, HLR-Sm Fep 0.6 0.6 a A/E, acquired or endogenous; CD, number of colonization days; DSC, number of days since colonization; AE, antimicrobial exposure; IAE, inef fective antimicrobial exposure; Amp, ampicillin; Amc, amoxicillin-clavulanate; Sam, ampicillin-sulbactam; Amk, amikacin; Chl, chloramphenicol; Ctx, cefotaxime; Cro, ceftriaxone; Fep, cefepime; Ery, erythromy cin; HLR-Gm, high-level resistance to gentamicin; HLR-Sm, high-level resistance to streptomycin; Imp, imipenen; Lvx, levofloxacin; Mem, meropenem; Tzp, piperacillin-tazobactam; Tob, tobramycin; Vn, vancomycin. Th e antimicrobials inef fective for each clone are underlined.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:3.585.58.265.64.725.2]100 colonization days for Efc-4), but also for susceptible clone Efc-1 (ST44) (13.6 effective antibiotic exposure days/100 colo-nization days) (Table 1). Among theE. faeciumclones, Efm-6 (ST18, HrCC17) encountered the highest antibiotic exposure (18.7 days per 100 colonization days) (Table 2). For this clone, the ineffective antimicrobial exposure was similar to the effective exposure (7.5 ineffective days versus 10 effective days per 100 colonization days). OtherE. faeciumclones received shorter periods of antimicrobial exposure, which was ineffective in most cases (Table 2). During the observation period, no van-comycin-resistant enterococcal clones were recovered in the hospital.
DISCUSSION
This study documents different features of the dynamics of enterococcal intestinal colonization in patients admitted to an N-ICU. However, the aim of this work was not to document the rates of transmission or acquisition as an epidemiological type of study but to report the rates of persistence of the different clones from an ecological perspective. Therefore, we designed a narrow observational protocol that included a lim-ited but sequential number of patients who had no overlapping stays in the ICU and who were admitted over a 10-month period. The enterococcal populations present in the patients on ICU admission were assumed to be part of the healthy gut microbiota before hospitalization and were considered endog-enous clones, whereas clonal variation was considered to be a result of hospitalization.
Previous studies of hospital enterococcal colonization fo-cused on the prevalence of multiresistant clones or described only the dynamics of colonization (11, 21). In our ecological study, we evaluated the role of persistence in the dynamics of enterococcal colonization using two new indexes. The first was CDPD and the second was CPR. These parameters allowed us to measure and compare changes in the GD and the persis-tence among patients’ enterococcal populations during their
stays in the N-ICU. Similar rates have been used in hospital epidemiology for other purposes, for instance, to document device-associated infection rates in ICU patients (10).
Overall, our results showed a significant increase in the clonal diversity ofE. faecalisisolates during patient hospital stays. This was a consequence of the increase in the number of different clones instead of the replacement of preexisting ones after clonal acquisition and might be associated with the higher overall persistence ofE. faecalis(as a species). It is well known that E. faecalis is a species that is well adapted for human intestinal colonization (29). This adaptation could be the result of certain physiological properties, including its ability to de-grade mucin, its mucosal adherence properties, and a specific host tolerance (15). We cannot discard the possibility that a number of the apparently newE. faecalisclones could respond to minority populations that were already present in the gut. In contrast, the clonal diversity of E. faeciumdecreased during the patients’ ICU stays, andE. faeciumfrequently appeared to be a transient colonizer. Nevertheless, we cannot rule out the possibility of fluctuations in the population density and the low sensitivity of culture. Remarkably, the ampicillin-resistantE. faeciumHrCC17 clone showed significantly higher persistence rates than the otherE. faeciumclones.
Mathematical modeling suggested that persistent gastroin-testinal colonization with vancomycin-resistant enterococci re-sulted in an increased prevalence of endemicity in particular wards (8). In our institution, an ampicillin-resistantE. faecium
clone (Efm-6, ST18) belonging to HrCC17 and a multiresistant
[image:4.585.46.541.82.263.2]E. faecalisclone (Efc-3, ST17) belonging to HrCC9 were en-demic and caused several bacteremic episodes (P. Ruiz-Gar-bajosa et al., unpublished data). Unlike other clones, they persisted for a long time in certain wards and ICUs in our hospital (7, 26). The specific role of the accessory genome involved in clonal persistence is not yet known, but inE. fae-calisandE. faecium, hospital-acquired clones have been shown to be enriched in adaptive mechanisms, like the presence of
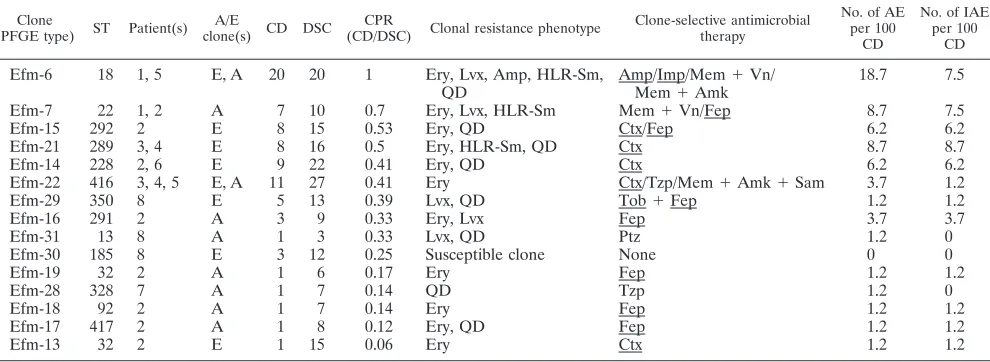
TABLE 2. Characteristics ofE. faeciumclonesa
Clone
(PFGE type) ST Patient(s)
A/E
clone(s) CD DSC
CPR
(CD/DSC) Clonal resistance phenotype
Clone-selective antimicrobial therapy
No. of AE per 100
CD
No. of IAE per 100
CD Efm-6 18 1, 5 E, A 20 20 1 Ery, Lvx, Amp, HLR-Sm,
QD
Amp/Imp/Mem⫹Vn/ Mem⫹Amk
18.7 7.5
Efm-7 22 1, 2 A 7 10 0.7 Ery, Lvx, HLR-Sm Mem⫹Vn/Fep 8.7 7.5
Efm-15 292 2 E 8 15 0.53 Ery, QD Ctx/Fep 6.2 6.2
Efm-21 289 3, 4 E 8 16 0.5 Ery, HLR-Sm, QD Ctx 8.7 8.7
Efm-14 228 2, 6 E 9 22 0.41 Ery, QD Ctx 6.2 6.2
Efm-22 416 3, 4, 5 E, A 11 27 0.41 Ery Ctx/Tzp/Mem⫹Amk⫹Sam 3.7 1.2
Efm-29 350 8 E 5 13 0.39 Lvx, QD Tob⫹Fep 1.2 1.2
Efm-16 291 2 A 3 9 0.33 Ery, Lvx Fep 3.7 3.7
Efm-31 13 8 A 1 3 0.33 Lvx, QD Ptz 1.2 0
Efm-30 185 8 E 3 12 0.25 Susceptible clone None 0 0
Efm-19 32 2 A 1 6 0.17 Ery Fep 1.2 1.2
Efm-28 328 7 A 1 7 0.14 QD Tzp 1.2 0
Efm-18 92 2 A 1 7 0.14 Ery Fep 1.2 1.2
Efm-17 417 2 A 1 8 0.12 Ery, QD Fep 1.2 1.2
Efm-13 32 2 E 1 15 0.06 Ery Ctx 1.2 1.2
aA/E, acquired or endogenous; CD, number of colonization days; DSC, number of days since colonization; AE, antimicrobial exposure; IAE, ineffective antimicrobial
exposure; Amp, ampicillin; Sam, ampicillin-sulbactam; Amk, amikacin; Ctx, cefotaxime; Fep, cefepime; Ery, erythromycin; HLR-Gm, high-level resistance to gentamicin; HLR-Sm, high-level resistance to streptomycin; Imp, imipenen; Lvx, levofloxacin; Mem, meropenem; QD, quinupristin-dalfopristin; Tzp, piperacillin-tazobactam; Tob, tobramycin; Vn, vancomycin. The antimicrobials ineffective for each clone are underlined.
on May 16, 2020 by guest
http://jcm.asm.org/
putative virulence genes and novel metabolic pathways (12, 13, 17, 19, 27). Some of these traits might facilitate tenacity in the intestinal gut and could also help the organism to reach a high cell density, which might increase the chance of transmission and persistence (27).
It is well known that antimicrobial agents cause disturbances in the intestinal microbiota, particularly those agents that reach high concentrations in the bile, such as certain expanded-spectrum cephalosporins and fluoroquinolones. Moreover, it has been considered that antimicrobials with activities against anaerobic organisms promoted high-density and persistent en-terococcal colonization through the inhibition of intestinal anaerobes (9). More recently, some studies suggested that an-timicrobial exposure could induce functional changes in en-terococcal populations, resulting in the expression of factors other than resistance that could promote adherence to the intestinal epithelial lining (1, 16, 24). This effect of antibiotics
as signaling molecules that modify bacterial adaptive pheno-types has also recently been suggested to exist in chronic bac-terial colonizers (20). The results of our study might indicate that the persistence of enterococcal clones during patients’ ICU stays might not be greatly affected by systemic antimicro-bial treatments, but more detailed studies are required to as-certain whether this point is true. Even though theE. faecalis
clones exhibited a higher CPR than theE. faeciumclones, the former were under effective antimicrobial treatment for signif-icantly more days than the latter. This was not the case forE. faecium HrCC17, whose behavior was similar to that of E. faecalis. E. faecium HrCC17 andE. faecalis are possibly en-riched populations that undergo functional changes after ex-posure to certain antibiotics, thus facilitating colonization and persistence in the gastrointestinal tract. Nevertheless, in vitro susceptibility phenotypes cannot explain the effects of antimi-crobials in the intestinal enterococcal population, since
differ-FIG. 1. CDPD values forE. faecalis(A) andE. faecium(B) throughout the hospital stay. The gray areas represent the CDPD values for allE. faecalis(A) and allE. faecium(B) clones, with the exception ofE. faecalisHrCC9 andE. faeciumHrCC17, respectively. The light gray areas represent the increases in the CDPD values whenE. faecalisHrCC9 andE. faeciumHrCC17 are included. No statistically significant difference in theE. faecalisCDPD increase when HrCC9 was considered was found, while the differences in theE. faeciumCDPD values with and without HrCC17 were statistically significant (P⫽0.03).
on May 16, 2020 by guest
http://jcm.asm.org/
[image:5.585.131.448.71.453.2]ent factors, including the amount of active drug attained in the intestinal tract and the interference of antimicrobials with the bowel content or the intestinal mucosa, should be considered. We are conscious that our conclusions might be limited be-cause of the small number of patients included in this study and also because sampling was performed with rectal swabs and the samples obtained might not represent the contents of the upper intestine. The recovery of fresh feces from these patients was difficult; however, we confirmed visually that the swabs in our study contained feces.
Our approach was more ecological than epidemiological, as it explored persistence on the basis of the recovery and the characterization of a high number of enterococcal clones (32 clones) at a number of sequential observation points (eight noncohospitalized patients) over a relatively long period of time (10 months).
In summary, we used two new indexes, CDPD and CPR, to measure the dynamics ofE. faecalisandE. faeciumclonal gut colonization and persistence among ICU patients in this piv-otal study. These indexes could be applied to other hospital colonization studies. Our results suggest more persistent col-onization abilities for the ensemble ofE. faecalis clones and also for an ampicillin-resistantE. faeciumclone belonging to HrCC17, in contrast to the non-CC17E. faeciumclones. The cumulative increase in the clonal diversity ofE. faecalis over time might be a consequence of the long persistence rates in both the individual patient and the ICU. On the contrary, the lower rates of persistence ofE. faeciumprevent the cumulative increase in clonal diversity. Knowledge of the dynamics of colonization of the different enterococcal clones, including HrCCs, could help provide an understanding of the epidemi-ology of enterococci in hospitals and could also be useful in the design and implementation of infection control measures.
ACKNOWLEDGMENTS
P. Ruiz-Garbajosa was the recipient of a post-MIR contract from the Instituto de Salud Carlos III, Ministerio de Sanidad y Consumo, Spain (contract CM04/0013). This work was partially supported by grants from the Ministerio de Sanidad y Consumo of Spain (grant
PI061141), the European Union (grant LSHE-CT-2007-037410), and the DeReMicrobiana Project of the Madrid Autonomous Community. We are grateful to Vicente Pintado for being a permanent advisor and for support of the infection control team.
REFERENCES
1.Aakra, A., H. Vebo, L. Snipen, H. Hirt, A. Aastveit, V. Kapur, G. Dunny, B. Murray, and I. F. Nes.2005. Transcriptional response ofEnterococcus fae-calisV583 to erythromycin. Antimicrob. Agents Chemother.49:2246–2259. 2.Austin, D. J., M. J. Bonten, R. A. Weinstein, S. Slaughter, and R. M. Anderson.1999. Vancomycin-resistant enterococci in intensive-care hospital settings: transmission dynamics, persistence, and the impact of infection
control programs. Proc. Natl. Acad. Sci. USA96:6908–6913.
3.Baden, L. R., W. Thiemke, A. Skolnik, R. Chambers, J. Strymish, H. S. Gold, R. C. Moellering, Jr., and G. M. Eliopoulos.2001. Prolonged colonization
with vancomycin-resistantEnterococcus faeciumin long-term care patients
and the significance of “clearance.” Clin. Infect. Dis.33:1654–1660.
4.Carmeli, Y., G. M. Eliopoulos, and M. H. Samore.2002. Antecedent treat-ment with different antibiotic agents as a risk factor for vancomycin-resistant
Enterococcus. Emerg. Infect. Dis.8:802–807.
5.CLSI.2008. Performance standards for antimicrobial susceptibility testing; 18th informational supplement M100-S18. CLSI, Wayne, PA.
6.Coque, T. M., P. Seetulsingh, K. V. Singh, and B. E. Murray.1998. Appli-cation of molecular techniques to the study of nosocomial infections caused
by enterococci, p. 469–493.InN. Woodford and A. P. Johnson (ed.),
Meth-ods in molecular medicine. Humana Press Inc., Totowa, NJ.
7.Coque, T. M., R. J. Willems, J. Fortu´n, J. Top., S. Diz, E. Loza, R. Canto´n, and F. Baquero.2005. Population structure ofEnterococcus faeciumcausing bacteremia in a Spanish university hospital: setting the scene for a future
increase in vancomycin resistance? Antimicrob. Agents Chemother.49:
2693–2700.
8.D’Agata, E. M., M. A. Horn, and G. F. Webb.2002. The impact of persistent gastrointestinal colonization on the transmission dynamics of
vancomycin-resistant enterococci. J. Infect. Dis.185:766–773.
9.Donskey, C. J., T. K. Chowdhry, M. T. Hecker, C. K. Hoyen, J. A. Hanrahan, A. M. Hujer, R. A. Hutton-Thomas, C. C. Whalen, R. A. Bonomo, and L. B. Rice.2000. Effect of antibiotic therapy on the density of vancomycin-resistant
enterococci in the stool of colonized patients. N. Engl. J. Med.343:1925–
1932.
10.Edwards, J. R., K. D. Peterson, M. L. Andrus, J. S. Tolson, J. S. Goulding, M. A. Dudeck, R. B. Mincey, D. A. Pollock, and T. C. Horan.2007. NHSN Facilities. National Healthcare Safety Network (NHSN) report, data
sum-mary for 2006, issued June 2007. Am. J. Infect. Control35:290–301.
11.Ha¨llgren, A., L. G. Burman, B. Isaksson, B. Olsson-Liljeqvist, L. E. Nilsson, B. Saeedi, S. Walther, and H. Hanberger.2005. Rectal colonization and frequency of enterococcal cross-transmission among prolonged-stay patients
in two Swedish intensive care units. Scand. J. Infect. Dis.37:561–571.
12.Heikens, E., M. J. Bonten, and R. J. Willems.2007. Enterococcal surface
protein Esp is important for biofilm formation of Enterococcus faecium
E1162. J. Bacteriol.189:8233–8240.
[image:6.585.112.477.67.246.2]13.Hendrickx, A. P., W. J. van Wamel, G. Posthuma, M. J. Bonten, and R. J. Willems.2007. Five genes encoding surface-exposed LPXTG proteins are FIG. 2. CPR values forE. faecalisandE. faeciumclones. The CPR value forE. faecaliswas significantly (*,P⫽0.001) higher than that for
E. faecium. There were no significant differences in CPR values among acquired clones, but the CPR values for endogenousE. faecalisclones were significantly (**,P⫽0.001) higher than those for endogenousE. faeciumclones.
on May 16, 2020 by guest
http://jcm.asm.org/
enriched in hospital-adaptedEnterococcus faeciumclonal complex 17
iso-lates. J. Bacteriol.189:8321–8332.
14.Homan, W. L., D. Tribe, S. Poznanski, M. Li, G. Hogg, E. Spalburg, J. D. Van Embden, and R. J. Willems.2002. Multilocus sequence typing scheme forEnterococcus faecium. J. Clin. Microbiol.40:1963–1971.
15.Huycke, M. M.2002. Physiology of enterococci, p. 133–175.InM. S. Gil-more, D. B. Clewell, P. Courvalin, et al. (ed.). The enterococci: pathogenesis, molecular biology, and antibiotic resistance. ASM Press, Washington, DC. 16.Lakticova´, V., R. Hutton-Thomas, M. Meyer, E. Gurkan, and L. B. Rice.
2006. Antibiotic-induced enterococcal expansion in the mouse intestine oc-curs throughout the small bowel and correlates poorly with suppression of
competing flora. Antimicrob. Agents Chemother.50:3117–3123.
17.Leavis, H., J. Top., N. Shankar, K. Borgen, M. Bonten, J. van Embden, and R. J. Willems. 2004. A novel putative enterococcal pathogenicity island
linked to theespvirulence gene ofEnterococcus faeciumand associated with
epidemicity. J. Bacteriol.186:672–682.
18.Leavis, H. L., M. J. Bonten, and R. J. Willems. 2006. Identification of high-risk enterococcal clonal complexes: global dispersion and antibiotic
resistance. Curr. Opin. Microbiol.9:454–460.
19.Leavis, H. L., R. J. Willems, W. J. van Wamel, F. H. Schuren, M. P. Caspers, and M. J. Bonten.2007. Insertion sequence-driven diversification creates a
globally dispersed emerging multiresistant subspecies ofE. faecium. PLoS
Pathog.3:e7.
20.Linares, J. F., I. Gustafsson, F. Baquero, and J. L. Martínez.2006. Antibi-otics as intermicrobial signaling agents instead of weapons. Proc. Natl. Acad.
Sci. USA103:19484–19489.
21.Lund, B., C Agvald-Ohman, A. Hultberg, and C. Edlund.2002. Frequent transmission of enterococcal strains between mechanically ventilated
pa-tients treated at an intensive care unit. J. Clin. Microbiol.40:2084–2088.
22.Mascini, E. M., K. P. Jalink, T. E. Kamp-Hopmans, H. E. Blok, J. Verhoef, M. J. Bonten, and A. Troelstra.2003. Acquisition and duration of
vancomy-cin-resistant enterococcal carriage in relation to strain type. J. Clin.
Micro-biol.41:5377–5383.
23. Reference deleted.
24.Rice, L. B., V. Lakticova, M. S. Helfand, and R. Hutton-Thomas.2004. In vitro antienterococcal activity explains associations between exposures to antimicrobial agents and risk of colonization by multiresistant enterococci.
J. Infect. Dis.190:2162–2166.
25.Ruiz-Garbajosa, P., M. J. Bonten, D. A. Robinson, J. Top., S. R. Nallapa-reddy, C. Torres, T. M. Coque, R. Canto´n, F. Baquero, B. E. Murray, R. del Campo, and R. J. Willems.2006. Multilocus sequence typing scheme for Enterococcus faecalisreveals hospital-adapted genetic complexes in a
back-ground of high rates of recombination. J. Clin. Microbiol.44:2220–2228.
26.Ruiz-Garbajosa, P., R. Canto´n, V. Pintado, T. M. Coque, R. Willems, F. Baquero, and R. del Campo. 2006. Genetic and phenotypic differences
amongEnterococcus faecalisclones from intestinal colonisation and invasive
disease. Clin. Microbiol. Infect.12:1193–1198.
27.Singh, K. V., S. R. Nallapareddy, and B. E. Murray.2007. Importance of the
ebp(endocarditis- and biofilm-associated pilus) locus in the pathogenesis of
Enterococcus faecalisascending urinary tract infection. J. Infect. Dis.195:
1671–1677.
28.Streit, J. M., R. N. Jones, H. S. Sader, and T. R. Fritsche.2004. Assessment of pathogen occurrences and resistance profiles among infected patients in the intensive care unit: report from the SENTRY Antimicrobial Surveillance
Program (North America, 2001). Int. J. Antimicrob. Agents24:111–118.
29.Tannok, G. W., and G. Cook.2002. Enterococci as members of the intestinal
microflora in humans, p. 101–132. InM. S. Gilmore, D. B. Clewell, P.
Courvalin, et al. (ed.), The enterococci: pathogenesis, molecular biology, and antibiotic resistance. ASM Press, Washington, DC.
30.Tenover, F. C., R. D. Arbeit, R. V. Goering, P. A. Mickelsen, B. E. Murray, D. H. Persing, and B. Swaminathan.1995. Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for
bacterial strain typing. J. Clin. Microbiol.33:2233–2239.