Transcatheter Aortic Valve Implantation (TAVI)
for Aortic Stenosis
Robin Chung Mphil MRCp
The Heart Hospital, University College London Hospitals
Honorary Fellow, Great Ormond Street and Imperial College Hospitals
Background
aortic stenosis remains the commonest form of valve disease in modern cardiology. With fifty years’ experience, surgical valve replacement remains the gold standard treatment for survival benefit, durability and symptomatic relief. percutaneous transcatheter aortic valve replacement has recently gained a credible momentum for inoperable and very high risk patients with severe aortic stenosis. Early and medium term results have demonstrated a proven survival benefit over conservative management, with documented complication rates for stroke, vascular complications and pacemaker implantation. The evidence base for cost effectiveness and long-term results are eagerly anticipated.
Mechanisms and Natural History
Degenerative aortic valve disease, characterised by progressive thickening, narrowing and obstruction of the valve leaflets, is a common finding in the elderly population. This triggers initially a chronic compensatory mechanism of elevated inotropic state and ventricular hypertrophy1 to minimise wall stress.
The physiological aorto-ventricular coupling is disturbed with increasing pressure drop and hypertrophy, and the prolonged initially asymptomatic course of the disease is followed by a more rapid symptomatic phase. progressive cavity dilatation leads to decompensation due to falling cardiac output and anginal symptoms.
The prevalence of non-rheumatic, non-congenital aortic valve sclerosis has been reported as 20% in populations aged 65 to 74, rising to 48% by age 85 and beyond. The prevalence of calcific aortic stenosis (as) rises with age -- 1.3% and between 2.8-4%, respectively in the same population.1,2 The
pathogenesis of calcific aortic stenosis has evolved beyond the hypothesis of age-related ‘wear and tear’ to one of a complex interplay of conventional atherosclerotic risks, mechanical leaflet stress, endothelial dysfunction, and calcium deposition.3
Clinically symptomatic aortic stenosis is heralded by chest pain (often in the absence of obstructive coronary artery disease), syncope, and exercise intolerance.4 left untreated,
symptomatic disease results in repeated hospitalisations and confers a mortality risk of 50% at two years5-10 – thus the
natural history of aortic stenosis is strikingly similar to many forms of cancer.11-13
Assessment of aortic stenosis
aortic stenosis may be objectively assessed by valve area or transaortic pressure drop. Non-invasive assessment of aortic stenosis by valve area, regardless of imaging modality, is based on principles of conservation of mass and the continuity equation. Invasive lV catheter pressure measurements of pressure drop are taken at peak-to-peak intervals and may thus differ slightly from Doppler measurements; invasive catheter aortic valve area is calculated using the gorlin equation.15 The
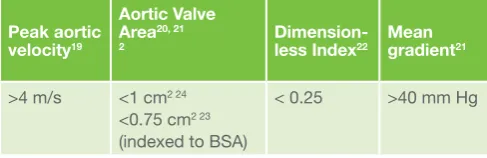
typical definition of ‘severe’ aortic stenosis varies according to assessment method as detailed in Table 1.
all calculated measures of aortic valve area are subject to measurement error15, 22, 23 of the lVoT diameter and Doppler
envelope. Finegold et al.22 reported better reproducibility of aVa
by ratio of peak Doppler velocity compared to Doppler VTI, but with wide confidence limits of +/- 25%.
Predictors of prognosis
several studies have reported that in asymptomatic severe as, change in peak velocity and calcification predicted survival, along with ischaemic heart disease, lung and renal comorbidities,24 whereas aortic valve area was not similarly
predictive of prognosis.10-12 There is no standardised definition
of low flow, “low gradient” aortic stenosis. Typical criteria have included impaired lV with EF < 35 - 40%, mean gradient < 30 -40 mm Hg, and aVa < 1 - 1.2cm2. In low-flow “low-gradient”
as where the apparent transaortic pressure drop falls due to lV impairment, prognosis is dictated by a combination of functional impairment, atrial fibrillation, stress response, and corrected valve area.25,26 low baseline ejection fraction, restrictive lV
filling and raised pulmonary artery pressure have been found as predictors of survival after aVR.27
Paradoxical low-flow low-gradient severe AS
patients with preserved EF (>50%), low indexed stroke volume (< 35ml/m2), low ‘gradient’ (<40mm Hg), aVa <0.7 cm2/m2 [aVa< 1cm2 unindexed) appear to comprise a clinically distinct
subset of as patients. They have a poor prognosis as the severity of disease is underestimated and hence conventional surgical aVR referral happens late in the course of the disease. The conventional hypothesis is that these patients have severe as that is masked by a combination of decreased arterial compliance, increased valvulo-arterial impendance (Zva),
hypertrophied ventricles with smaller cavity volume, and lower lV mid-wall radial shortening, longitudinal shortening and [‘strain’ rate]28. The constellation above implies the pathological
triad of: increased systemic vascular resistance, obstructive valve disease, and intrinsic myocardial disease.
The decreased arterial compliance may be due to hypertensive disease and can be represented by Zva = systolic pressure
+ mean pressure gradient / indexed stroke volume. The obstructive valve disease is manifest as calcific aortic stenosis. Intrinsic myocardial disease may manifest as systolic and Table 1: Equivalent definitions of typical severe aortic stenosis.
Peak aortic velocity19
Aortic Valve Area20, 21
2 Dimension-less Index22 Mean gradient21
>4 m/s <1 cm2 24
<0.75 cm2 23
(indexed to Bsa)
diastolic ‘dysfunction’== typical EF value in the lower-end of normal despite lVH and small cavity volume; this belies a low stroke volume due to pronounced lV fibrosis, fibre architecture disarray and thus deranged remodelling compared to high gradient as. Flett et al.29 found in severe as patients,
increased diffuse myocardial fibrosis correlated with severity of diastolic dysfunction and predicted exercise tolerance by 6-minute walk test. Thus underlying fibrosis may also manifest as a restrictive lV physiology due to high end-diastolic pressures and decreased total lV filling time. ultimately, the patient experiences anginal symptoms and effort intolerance disproportionate to conventional markers of aortic valve disease due to underlying pathological disturbance in Va impedance, decreased coronary diastolic flow reserve, and raised filling pressures. Thus, a unifying theory of arterio-valvulo-ventriculo coupling is required to explain the pathophysiology in
paradoxical low-flow low-gradient severe as.
Management of aortic stenosis
surgical aortic valve replacement (aVR) remains the gold standard treatment for the majority of symptomatic patients. Fifty years’ experience30-33 has resulted in improved survival due
to developments in cardiopulmonary bypass techniques, valve technology, and myocardial preservation. In developed Western economies, the annual volume of aVR ranges from 12,000 in germany34 to more than 60,000 in the usa.35 operative survival
after elective aVR in 1960 was initially 50%35, but now routinely
exceeds 97.5% in low-risk patient groups.24, 36, 37.
surgical aVR techniques differ mainly in terms of valve prosthesis; minor variations occur due to operator choice of bypass or cardioplegia. options for prosthetic valves include mechanical or tissue (allograft, homograft or autograft) in stented or stentless mountings. Mechanical valves offer the advantage of long term durability and reliability balanced against risk of thromboembolism and haemorrhage from requisite anticoagulation38. To date, there are no satisfactory
medical treatments for aortic stenosis that alter progression or mortality. Recent trials (sEas, salTIRE) predicated on pleiomorphic principles of statin and fibrate inhibition of calcium deposition have shown no benefit to alter survival or progression in as39,40
although surgical aVR remains the definitive treatment for as, a significant proportion of patients are denied surgical valve
replacement due to high surgical risk. somewhat surprisingly from the EuroHeart survey, up to one-third of symptomatic severe as patients were denied surgery primarily on the basis of age and lV systolic impairment over and above validated cardiovascular comorbidities.41 Thus, in the absence of
viable medical management or open surgical aVR as options, symptomatic patients with severe as may be managed palliatively or offered percutaneous transcatheter aortic valve intervention (TaVI).
Transcatheter Aortic Valve Implantation (TAVI)
Transcatheter aortic valve implantation (TaVI) was first reported in man by Cribier et al. in 200242 and has sincegained popularity and credibility as a viable treatment option for patients with inoperable and high-risk aortic stenosis. percutaneous valve replacement has a proven evidence base from pulmonary valve replacement in the right ventricular outflow tract (RVoT)43; TaVI procedures offer similar advantages
by avoiding cardiopulmonary bypass and open chest access. Two competing systems with MHRa, CE- and FDa approval from Edwards lifesciences (sapien series) and Medtronic (CoreValve) have been evaluated in high-quality trials. The two devices differ in terms of leaflet and stent material, annulus sizing, deployment method, and can be delivered via transapical, transfemoral, subclavian or axillary access. Evolving experience suggests that TaVI offers improved survival compared to medical or valvuloplasty treatment for inoperable patients,44, 45 and comparable results to high-risk surgical
aVR patients.46, 47 ongoing trial data have also highlighted the
impact of TaVI-associated complications44-47 of stroke, vascular
complications,48 pacemaker implantation and paravalvular aortic
regurgitation (aR) on morbidity and mortality.
Clinical Outcomes after TAVI and the
importance of aortic regurgitation
Even in isolated aortic stenosis, aortic regurgitation remains an important prognostic finding after both surgery or percutaneous intervention. post-procedural aortic regurgitation is a mediator of morbidity and prognosis.50 The incidence of significant
post-operative prosthetic paravalvular aR after surgical aVR is rare at less than 1%,47 but is more common (pooled estimate 7.4%)
and important after transcatheter aVR.46, 47, 50 Major TaVI trials
consistently confirm that post-procedural aortic regurgitation predicts survival.
There is no standardised grading for paravalvular aR, and thus Valve academic Research Consortium (VaRC) definitions have been proposed to standardise definitions for clinical endpoints for TaVI. Central jet aR is graded on criteria for jet density, jet width, Doppler deceleration time. paravalvular aR may be assessed on the percentage of circumferential paraprosthetic leak,53 but this has not yet been validated and remains
controversial.
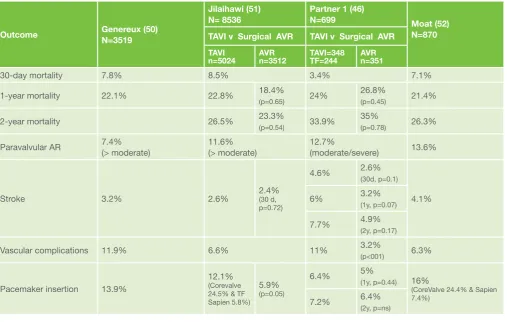
genereux et al.50, Jilaihawi et al.51, and Moat et al.52 reported
separate meta-analyses of TaVI studies across more than 3,500 patients, respectively. pooled TaVI outcomes were broadly similar as illustrated in Table 3. TaVI 30-day mortality was similar at 7.8 – 8.5%; 1-year mortality of 21-22%, and 2-year mortality of 26%. Multivariate predictors of mortality were lV dysfunction (EF<30%), moderate to severe aR, and CopD. overall incidence of stroke was 2.6 ~ 4.1%, moderate aR 13.6%, major vascular complication 6.3%. pooled pacemaker implantation incidence was 16.3% (CoreValve v sapien, 24 – 28.9% v 4.9 - 7.4%, p<0.001), with higher rate of occurrence in the CoreValve groups. This may be due to the self-expansile Table 2: VaRC definitions for selected outcome measures and safety
endpoints.
Device Success (composite endpoint)
Combined safety endpoint (30 days)
• Mortality / Cardiovascular Mortality assessed at 30 days, 1 year, annually to at least 5 years
• Myocardial infarction (periprocedural <72h and spontaneous >72h)
• Stroke – rapid onset focal/global neurological deficit >24h or <24h if confirmed by imaging / thrombolysed/ resulting in death
• TIA – focal neurological deficit with rapid resolution, < 24h, or no enhancement on DWI MRI
• Bleeding
• Vascular Complications
properties of the nitinol mesh and taller implant profile in the lV outflow tract.50
The PARTNER trials
The us partner multi-centre randomised trials recruited patients into two separate arms – high-risk surgical aVR and inoperable surgical as patients -- with the Edwards sapien percutaneous aortic valve prosthesis.
Partner 1A (High-risk operable AS patients --
Non-inferiority of TAVI v Surgical AVR)
The partner 1a46,47 arm recruited 699 patients across 25
centres for randomisation to either conventional surgical aVR or transcatheter aortic valve intervention. The primary end point was non-inferiority of all-cause death in TaVI compared to surgical aVR, predefined as a percentage-difference of 7.5%. all-cause mortality was reported at 3.4% v 6.5% at 30 days (TaVI v surgical aVR, p=0.07), and 24% v 26.8% (p=0.44) at 1 year, (47) respectively. Two-year mortality was also not significantly different between the TaVI and surgical aVR treatment groups – 33.9% v 35% (p=0.78),46 respectively.
secondary end points for major stroke rate were reported as 3.8% v 2.1% (TaVI v surgical aVR p=0.2) at 30 days, and 5.1% v 2.4% (p=0.07) at 1 year (47), respectively. stroke or TIa was more frequent after TaVI at 2 years – 6.5% v 11.2% (p=0.05).46
Major vascular complication rates were reported more
frequently in TaVI v surgical aVR -- 11% v 3.2% (p<0.001) at 30 days. Bleeding and new onset atrial fibrillation (aF) were more common after surgical aVR. Early symptomatic improvement and quality of life (Qol) outcomes were reported better after TaVI, but were equivalent by 1 year.47
at two years, increase in aortic valve area was similar in the two groups. paravalvular aortic regurgitation was more frequent after TaVI (p<0.001), and notably more than mild paravalvular regurgitation was associated with increased late mortality: hazard ratio 2.11 (95% CI 1.43 – 3.1, p<0.001, p<0.001), see Figure 4(D). The partner 1a authors recommended work should be directed toward (1) reducing paravalvular aR (2) techniques for precise valve sizing and positioning and (3) judicious use of post TaVI dilatation.
PARTNER 1B (TAVI v conservative management in
inoperable severe AS patients)
The partner 1B44, 45 trial arm recruited from 21 centres, 358
patients with inoperable severe as randomised to receive either conservative (medical management and/or balloon angioplasty) or TaVI. The primary end point for all-cause mortality at 1 year was reached in 30.7% v 50.7% (TaVI v medical, hazard ratio 0.55 [CI 0.4 to 0.74], p<0.001), Figure 5.44. a composite
end point of death from any cause or repeat hospitalisation similarly favoured TaVI over conventional management, 42.5% v 71.6%, p<0.001). Major vascular complications were more frequent in TaVI patients (16.2% v 1.1%, p<0.001), and there was a trend toward more frequent major strokes following TaVI at 30 days (5.0% v 1.1%, p=0.06). at two years, the survival advantage for TaVI patients remained significant – all-cause mortality was lower in the TaVI group (43.4% v 68%, p<0.001). Major strokes were more common in the TaVI group (13.8% v 5.5% p=0.01) due to more ischaemic strokes in the TaVI group at 30 days (p=0.02), and a non-significant trend for more haemorrhagic strokes in the TaVI group beyond 30 days (p=0.16). Echocardiographic indicators of paravalvular aR and aortic valve area/gradient after TaVI did not significantly worsen at two years.
Table 3: Comparison of TaVI outcome data across pooled studies.
Outcome Genereux (50)N=3519
Jilaihawi (51) N= 8536
Partner 1 (46)
N=699 Moat (52) N=870 TAVI v Surgical AVR TAVI v Surgical AVR
TAVI
n=5024 AVR n=3512 TAVI=348 TF=244 AVRn=351
30-day mortality 7.8% 8.5% 3.4% 7.1%
1-year mortality 22.1% 22.8% 18.4%
(p=0.65) 24%
26.8%
(p=0.45) 21.4%
2-year mortality 26.5% 23.3%
(p=0.54) 33.9%
35%
(p=0.78) 26.3%
paravalvular aR 7.4% (> moderate) 11.6% (> moderate) 12.7%(moderate/severe) 13.6%
stroke 3.2% 2.6% 2.4% (30 d,
p=0.72)
4.6% 2.6%
(30d, p=0.1)
4.1%
6% 3.2%
(1y, p=0.07)
7.7% 4.9%
(2y, p=0.17)
Vascular complications 11.9% 6.6% 11% 3.2%
(p<001) 6.3%
pacemaker insertion 13.9%
12.1% (Corevalve 24.5% & TF sapien 5.8%)
5.9% (p=0.05)
6.4% 5%
(1y, p=0.44) 16%
(CoreValve 24.4% & sapien 7.4%)
7.2% 6.4%
Notably, the data suggested that survival benefit from TaVI may diminish with higher surgical risk (sTs) scores. predictors of survival for TaVI patients were body mass index (hazard ratio 0.95 per unit increase [95% CI 0.91 to 0.98, p=0.005), prior stroke (hazard ratio 2.99, 95% CI 1.19 to 7.51, p=0.01) and CopD requiring supplemental oxygen (hazard ratio 1.69, 95% CI 1.05 to 2.73, p=0.03).48
Vascular complications in TAVI
genereux et al.48 analysed TaVI recipients from both partner 1a
and 1B groups for predictors of major vascular complications. Major vascular complication was defined as any (1) thoracic aortic dissection or (2) any access site vascular injury requiring intervention, surgery, >4u blood transfusion leading to end-organ damage or death. Major vascular complications occurred in 15% of all TaVI patients within 30-days of the procedure, with significantly higher 30-day and 1-year mortality. Female gender was the only identifiable independent predictor of such vascular complications, even after accounting for small femoral artery diameters in women.
Microcirculation and differential function
improvement after TAVI
Both arms of the partner trials demonstrated sustained improvements in functional class, aortic valve area and mean gradient following TaVI. Jin et al.53, 54 documented early
favourable changes in incoordination (asynchrony), myocardial wall stress and power following surgical aVR for as with or without coronary artery disease. Davies et al.55 studied coronary
microcirculation using invasive arterial wave intensity analysis in 11 patients undergoing TaVI (sapien n=10). Their findings support improved coronary reserve after TaVI as documented by increasing coronary diastolic suction wave with rising heart rate, consistent with relief of angina symptoms with unobstructed coronary arteries.
Differential changes in longitudinal, circumferential and radial function are known to occur with progression of aortic stenosis even with preserved global ejection fraction. These changes are successive compensatory mechanisms to wall strain and pressure rise, and normalise following both surgical and transcatheter aortic valve replacement. In contrast, RV function remains preserved after TaVI compared to surgical aVR; Zhao et al.56 postulated RV myocardial preservation, aortic cross clamp,
or right atrial cannulation during open chest cardiopulmonary bypass as putative mechanisms.
Modelling for TAVI and the Heart Team
approach
successful outcomes for TaVI procedures depend on careful patient selection, optimal device implantation, and post-procedural high dependency care. The multidisciplinary team approach is critical for each of these stages. Multi-modality imaging17, 57-58 employing catheter angiogram,
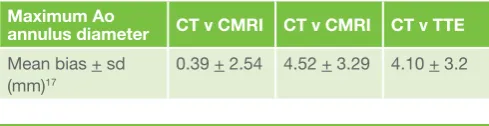
echocardiographic, multi-detector CT and cardiac MRI techniques is becoming the standard approach for anatomical modelling prior to TaVI. Transthoracic and transoesphageal echocardiograms underestimated aortic annulus dimensions due to the limitation of imaging in a single plane thereby contributing to annulus-prosthesis mismatch and hence paravalvular aR.17, 57, 58 Thus, cardiac CT has become the
favoured standard for annular sizing. In native TaVI patients, cardiac MRI was reported by Jabbour et al.17 to be reliable and
equally reproducible to CT and superior to TTE. Furthermore, Quail et al.59 showed that cardiac MRI was comparable to CT
for aortic dimensions and coronary ostia height for valve-in-valve TaVI procedures. Table 4 illustrates agreement between CT, MRI and TTE measurements.
Willson et al57 and Jilaihawi et al58 have shown the importance
of aortic annulus dimensions and calcium burden on predicting TaVI outcomes for paravular aR. Willson showed that the absolute difference between TaVI prosthesis size and pre-procedural annulus measurements by CT and transoesphageal echocardiograms (ToE) predicted paravular aR at discharge. By receiver operating characteristic (RoC) the area under the curve (auC) for CT was 0.81, 95% CI 0.68-0.88) and for ToE was 0.70, 95% CI 0.51 – 0.88), making CT a better predictor of paravalvular aR outcome than ToE. Furthermore, the incidence of paravalvular aR was strikingly higher for undersized TaVI prostheses – paravalvular aR incidence 2.2% v 21.4% for oversized > 1mm vs. undersized 1mm (odds ratio 9.4, 95% CI 2.15 – 88.8, p<0.05). Jilaihawi used retrospectively gated CT cross-sectional and multi-planar reconstructions in 40 patients compared to ToE measurements in 96 TaVI patients, to predict per-procedural paravalvular aR as an outcome. CT was superior to ToE for predicting paravalvular aR by maximum annulus diameter, RoC auC of 0.82 (95% CI 0.7 – 0.94, p<0.001). applying the CT sizing rule prospectively successfully predicted paravalvular aR after TaVI (mild+ paravalvular aR 7.5% v 21.9%, p=0.045). Furthermore, a simplified lVoT calcium score was a powerful risk predictor for paravalvular aR exceeding that of annulus mismatch (odds ratio for lVoT calcium= 9.1, 95% CI 1.6 – 50, p=0.02, v oR for annulus mismatch =1.6, 95% CI 1.3 – 2, p<0.001).
Indications for TAVI
although there has been concern of ‘indication creep’ for TaVI procedures, this is unlikely to be the case at present for several reasons. Total TaVI procedure volumes tend to increase but surgical aVR procedures remained unchanged, owing to increased pickup and constant rate of refusal for surgical aVR in new as patients. This compares favourably to the german aortic Replacement gaRY registry. The gaRY registry reported at the recent EsC congress 2012 that of 13,590 total aVRs, there were 3875 TaVI procedures, thus TaVI volume accounted for 28.5% of all aVR procedures.
Cost-effectiveness of TAVI
Cost-effectiveness data from the partner 1a series59
documented similar outcomes for cost and QalY (Quality-adjusted life Years) between TaVI and high-risk surgical aVR patients. However, sub-group analysis comparing transfemoral and transapical approaches favoured transfemoral-TaVI over surgical aVR for cost-effectiveness and QalYs; whereas transapical-TaVI was economically advantageous in only 7.1% of cases60. However, given the higher rate of pacemaker
implantation and vascular complications with TaVI, overall cost and hospital stay calculations may prove less favourable in TaVI patients experiencing complications.
Table 4: precision of aortic annulus measurements across modalities.
Maximum Ao
annulus diameter CT v CMRI CT v CMRI CT v TTE
Mean bias + sd (mm)17
Endocarditis and TAVI
Endocarditis after TaVI remains low, reported incidence varying from 2.3 to 3.4%61, 62. This compares favourably with that
reported after percutaneous pulmonary valve replacement63.
However, the increased incidence of paravalvular aR complicates assessment of regurgitation attributable to infection, and isolated case reports document involvement of valves other than the original neo-aortic prosthesis.
Conclusion
Transcatheter aortic valve implantation has improved survival and symptom relief for inoperable and high risk aortic stenosis patients, but there remain important limitations. one-year mortality after TaVI compared favourably to conservative management of as (21 – 30% vs. 51%), equating to a number needed-to-treat (NNT) of 5; with one- and two-year TaVI mortality outcomes that are not inferior to high-risk surgical aVR. TaVI outcomes demonstrate sustained relief of valvular obstruction, but significant paravalvular regurgitation remains an important weakness due to limited device sizes. Vascular complications and permanent pacemaker implantations are substantially increased after TaVI, with a trend toward higher stroke rates. Future developments in device choice and pre-implantation modelling may increase the efficacy and benefit from TaVI.
Correspondence to: Robin Chung
NHIR Cardiology academic Clinical Fellow [email protected]
References
1. Nkomo VT , skelton TN, gottdiener Js, scott Cg, Enriquez-sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005-1011.
2. stewart BF , lind BK, gardin JM, gottdiener Js, smith VE, Kitzman DW, otto CM. Clinical factors associated with calcific aortic valve disease. Cardiovascular health study. J Am Coll Cardiol. 1997;29:630-634. 3. Hermans H , Holvoet p, Verbeken E, Meuris B, Flameng W, Herregods
MC. statins for calcific aortic valve stenosis: Into oblivion after saltire and seas? an extensive review from bench to bedside. Curr Probl Cardiol. 2010;35:284-306.
4. Ross J Jr . aortic stenosis. Circulation. 1968;38:61-67
5. schwarz F Bp, Manthey J, Hoffmann M, schuler g, Mehmel HC, schmitz W, Kübler W. The effect of aortic valve replacement on survival. Circulation. 1982;66:1105-1110
6. pellikka pa , Nishimura Ra, Malouf JF, Bailey KR, scott Cg, Barnes ME, Tajik aJ. outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation. 2005;111:3290-3295
7. Rosenhek R , schemper M, Czerny M, Mundigler g, graf s, Bergler-Klein J, grimm M, gabriel H, Maurer g. Natural history of very severe aortic stenosis. Circulation. 2010;121:151-156.
8. Rosenhek R , porenta g, lang I, Christ g, schemper M, Maurer g, Baumgartner H. predictors of outcome in severe, asymptomatic aortic stenosis. N Engl J Med 2000;343:611-617.
9. Rosenhek R , schemper M, scholten C, Heger M, gabriel H, Binder T, Maurer g, Baumgartner H. Mild and moderate aortic stenosis. Natural history and risk stratification by echocardiography. Eur Heart J. 2004;25:199-205.
10. Clark Ma , Duhay Fg, Thompson aK, Keyes MJ, svensson lg, Bonow Ro, stockwell BT, Cohen DJ. Five-year clinical and economic outcomes among patients with medically managed severe aortic stenosis: Results from a medicare claims analysis. Circ Cardiovasc Qual Outcomes. 2012;epub 11. schiller JH , Belani Cp, langer C, sandler a, Krook J, Zhu J, Johnson DH;
Eastern Cooperative oncology group. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346:92-98.
12. sa C. Cancer of the ovary. N Engl J Med. 2004;351:2519-2529. 13. Mandel Js , Ederer F, et al. Colorectal cancer mortality: Effectiveness
of biennial screening for fecal occult blood. J Natl Cancer Inst. 1999;91:434e437.
14. office of National statistics. Cancer survival in england: patients
diagnosed 2005-2009 and followed up to 2010. http://www.ons.gov.uk/ ons/dcp171780_242394.pdf. 2010: accessed 14/09/12.
15. Minners J , gohlke-Baerwolf C, Kienzle Rp, Neumann FJ, Jander N. Inconsistent grading of aortic valve stenosis by current guidelines: Haemodynamic studies in patients with apparently normal left ventricular function. Heart. 2010;96:1463-1468.
16. Reant p , lafitte s, serri K, Montaudon M, Corneloup o, Roudaut R, laurent F. absolute assessment of aortic valve stenosis by planimetry using cardiovascular magnetic resonance imaging: Comparison with transesophageal echocardiography, transthoracic echocardiography, and cardiac catheterisation. Eur J Radiol. 2006;59:276-283.
17. Jabbour a , Moat N, gulati a, Roussin I, alpendurada F, park B, okoroafor F, asgar a, Barker s, Davies s, prasad sK, Rubens M, Mohiaddin RH. Multimodality imaging in transcatheter aortic valve implantation and post-procedural aortic regurgitation: Comparison among cardiovascular magnetic resonance, cardiac computed tomography, and echocardiography. J Am Coll Cardiol. 2011;58:2165-2173.
18. Carabello Ba. aortic stenosis. N Engl J Med. 2002;346:677–682. 19. otto CM. Valvular aortic stenosis: Disease severity and timing of
intervention. J Am Coll Cardiol. 2006;47:2141–2151.
20. lung B , Tornos p, Tribouilloy C, Hall R, Butchart E, Vahanian a. . Recommendations on the management of the asymptomatic patient with valvular heart disease. Eur Heart J. 2002;23:1252–1266
21. Bonow Ro , Chatterjee K, de leon aC Jr, Faxon Dp,Freed MD, gaasch WH, lytle BW, Nishimura Ra, o’gara pT, o’Rourke Ra, otto CM, shah pM, shanewise Js, smith sC Jr, Jacobs aK, adams CD, anderson Jl, antman EM, Fuster V, Halperin Jl, Hiratzka lF, Hunt sa, Nishimura R, page Rl, Riegel B. . aCC/aHa 2006 guidelines for the management of patients with valvular heart disease: a report of the american college of cardiology/ american heart association task force on practice guidelines (writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease) J Am Coll Cardiol. 2006;48:e1–e148. 22. Finegold Ja , Cecaro F, sutaria N, Mayet J, Francis Dp. Choosing between
velocity-time-integral ratio and peak velocity ratio for calculation of the dimensionless index (or aortic valve area) in serial follow-up of aortic stenosis. Int J Cardiol. 2012;In press:epub. pMID: 22575631 23. Minners J , gohlke-Baerwolf C, Kienzle Rp, Neumann FJ, Jander N.
Inconsistencies of echocardiographic criteria for the grading of aortic valve stenosis. Eur Heart J. 2008;29:1043-1048
24. Brennan JM , Zhao Y, o’Brien sM, Douglas ps, peterson ED. long-term survival following aortic valve replacement among high-risk elderly patients in the united states: Insights from the sTs adult cardiac surgery database, 1991-2007. Circulation. 2012;epub 20 aug 2012
25. Clavel Ma , Burwash Ig, Mundigler g, Dumesnil Jg, Baumgartner H, Bergler-Klein J, Beanlands Rs, Mathieu p, Magne J, pibarot p. predictors of outcomes in low-flow, low-gradient aortic stenosis: Results of the multicenter topas study. Circulation. 2008;118:s234-242
26. levy F , Monin Jl, Maillet JM, pasquet a, le Tourneau T, petit-Eisenmann H, gori M, Jobic Y, Bauer F, Chauvel C, leguerrier a, Tribouilloy C. aortic valve replacement for low-flow/low-gradient aortic stenosis operative risk stratification and long-term outcome: a european multicenter study. J Am Coll Cardiol. 2008;51:1466-1472.
27. Ding WH , Duncan a, li W, lim E, Kaya Mg, Chung R, pepper JR, Henein MY. predictors of survival after aortic valve replacement in patients with low-flow and high-gradient aortic stenosis. Eur J Heart Fail. 2009;11:897-902
28. Dumesnil Jg , Carabello B. paradoxical low flow and/or low gradient severe aortic stenosis despite preserved left ventricular ejection fraction: Implications for diagnosis and treatment. Eur Heart J. 2010;31:281-289 29. Flett as , Quarta g, Mirabel M, pellerin D, Herrey as, Hausenloy DJ, ariti
C, Yap J, Kolvekar s, Taylor aM, Moon JC. Diffuse myocardial fibrosis in severe aortic stenosis: an equilibrium contrast cardiovascular magnetic resonance study. Eur Heart J Cardiovasc Imaging. 2012;13:819-826. 30. Bodnar E , Martelli V, Ross DN. long term performance of 580 homograft
and autograft valves used for aortic valve replacement. Thorac Cardiovasc Surg. 1979;27:31-38.
31. Ross DN.. The replacement of the aortic valve with biological tissue. Ann Thorac Surg. 1968;5:383-392.
32. Harken DE , Taylor MC. partial and complete prostheses in aortic insufficiency. J Thorac Cardiovasc Surg. 1960;40:744–762. 33. Barnard CN, goosen C. Total aortic valve replacement. Lancet.
1963;2:856-859.
34. Beckmann a , Figulla HR, Cremer J, Kuck KH, lange R, Zahn R, sack s, schuler gC, Walther T, Beyersdorf F, Böhm M, Heusch g, Funkat aK, Meinertz T, Neumann T, papoutsis K, schneider s, Welz a, Mohr FW; for the gaRY Executive Board. The german aortic valve registry (gary): a nationwide registry for patients undergoing invasive therapy for severe aortic valve stenosis. Thorac Cardiovasc Surg. 2012;60:319-325 35. o’Brien sM , Filardo g, Ferraris Va, Haan CK, Rich JB, Normand sl,
36. Wendt D , Kayser K, Thielmann M, Tossios p, Massoudy p, Kamler M, Jakob H. society of thoracic surgeons score is superior to the euroscore determining mortality in high risk patients undergoing isolated aortic valve replacement. Ann Thorac Surg. 2009;88:474-475.
37. Care Quality Commission . Rates of survival after aortic valve replacement operations in the uk. Heart Surgery UK (CQC) statistics online. 2009, http:// heartsurgery.cqc.org.uk
38. Kvidal p , Malm T, sta°hle E. long-term follow-up of morbidity and mortality after aortic valve replacement with a mechanical valve prosthesis. . Eur Heart J. 2000;21:1099-1100
39. Rossebø aB , Boman K, Brudi p, Chambers JB, Egstrup K, gerdts E, gohlke-Bärwolf C, Holme I, Kesäniemi Ya, Malbecq W, Nienaber Ca, Ray s, skjaerpe T, Wachtell K, Willenheimer R; sEas Investigators. Intensive lipid lowering with simvastatin and ezetimibe in aortic stenosis. N Engl J Med. 2008;359:1343-1356
40. Cowell sJ , prescott RJ, Bloomfield p, Reid J, Northridge DB, Boon Na; scottish aortic stenosis and lipid lowering Trial, Impact on Regression (salTIRE) Investigators. a randomized trial of intensive lipid-lowering therapy in calcific aortic stenosis. N Engl J Med. 2005;352:2389-2397. 41. lung B , Baron g, Messika-Zeitoun D, Delahaye F, Tornos p,
gohlke-Bärwolf C, Boersma E, Ravaud p, Vahanian a. Decision-making in elderly patients with severe aortic stenosis: Why are so many denied surgery? Eur Heart J. . 2005;26:2714-2720
42. Cribier a , Bash a, Borenstein N, Tron C, Bauer F, Derumeaux g, anselme F, laborde F, leon MB. percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: First human case description. Circulation. 2002;106:3006-3008.
43. Bonhoeffer p , saliba Z, Merckx J, aggoun Y, Bonnet D, acar p, le Bidois J, sidi D, Kachaner J. percutaneous replacement of pulmonary valve in a right-ventricle to pulmonary-artery prosthetic conduit with valve dysfunction. Lancet. 2000;356:1403-1405.
44. leon MB , Mack M, Miller DC, Moses JW, svensson lg, Tuzcu EM, Webb, Jg , Makkar RR, Brown Dl, Block pC, guyton Ra, pichard aD, Bavaria JE, Herrmann HC , petersen Jl, akin JJ, anderson WN, Wang D, pocock s;, Investigators pT. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;2010:1597-1607
45. Makkar RR , Jilaihawi H, Kapadia s, pichard aD, Douglas ps,, Thourani VH , Webb Jg, Herrmann HC, Bavaria JE, Kodali s, Brown Dl,, Bowers B DT, svensson lg, Tuzcu M, Moses JW, Williams MR, siegel RJ, akin JJ , pocock s, smith CR, leon MB; paRTNER Trial Investigators. Transcatheter aortic-valve replacement for inoperable severe aortic stenosis. N Engl J Med. 2012;366:1696-1704
46. Kodali sK WM, smith CR, svensson lg, Webb Jg, Makkar RR, Fontana gp, Dewey TM , pichard aD, Fischbein M, szeto WY, lim s, greason Kl,, Teirstein ps , Douglas ps, Hahn RT, Whisenant B, Zajarias a, Wang D,, akin JJ , leon MB; paRTNER Trial Investigators. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med. 2012;366:1686-1695.
47. smith CR , Mack MJ, Miller DC, Moses JW, svensson lg, Tuzcu EM, WebbJg, Makkar RR, Williams M, Dewey T, Kapadia s, Babaliaros V, Thourani, VH Cp, pichard aD, Bavaria JE, Herrmann HC, akin JJ, anderson WN, Wang D,, Investigators . Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198 48. généreux p , svensson lg, Kodali sK, satler lF, Fearon WF, Davidson
CJ, Eisenhauer aC, Makkar RR, Bergman gW, Babaliaros V, Bavaria JE, Velazquez oC, Williams MR, Hueter I, Xu K, leon MB; paRTNER Trial Investigators. Vascular complications after transcatheter aortic valve replacement: Insights from the partner (placement of aortic transcatheter valve) trial. J Am Coll Cardiol. 2012;60:1043-1052.
49. leon MB , Nikolsky E, Blackstone EH, Cutlip DE, Kappetein ap, Krucoff MW, Mack M, Mehran R, Miller C, Morel Ma, petersen J, popma JJ, Takkenberg JJ, Vahanian a, van Es ga, Vranckx p, Webb Jg, Windecker s, serruys pW. standardized endpoint definitions for transcatheter aortic valve implantation clinical trials: a consensus report from the valve academic research consortium. J Am Coll Cardiol. 2011;57:253-269. 50. généreux p , Van Mieghem NM, Kodali s, Kirtane aJ, Xu K, smith C,
serruys pW, Kappetein ap, leon MB. Clinical outcomes after transcatheter aortic valve replacement using valve academic research consortium definitions: a weighted meta-analysis of 3,519 patients from 16 studies. J Am Coll Cardiol. 2012;59:2317-2326
51. Jilaihawi H, Chakravart T, Weiss RE, Fontana gp, Forrester J, Makkar RJ. Meta-analysis of Complications in arotic Valve Replacement: Comparison of Medtronic Corevalve, Edwards-sapien, and surgical aortic Valve Replacement in 8,536 patients. Catheterization and Cardiovascular Interventions 2012; 80: 128-138.
52. Moat NE , de Belder Ma, Bridgewater B, Cunningham aD, Young Cp, Thomas M, Kovac J, spyt T, MacCarthy pa, Wendler o, Hildick-smith D, Davies sW, Trivedi u, Blackman DJ, levy RD, Brecker sJ, Baumbach a, Daniel T, gray H, Mullen MJ. long-term outcomes after transcatheter aortic valve implantation in high-risk patients with severe aortic stenosis: The uK TaVI (united kingdom transcatheter aortic valve implantation) registry). J Am Coll Cardiol. 2011;58:2130-2138
53. Jin XY , gibson Dg. Effects of incoordination on left ventricular
force-velocity relation in aortic stenosis. Heart. 1996;76:495-501.
54. Jin XY , Brecker sJ, Carey Ja, gibson Dg. Early changes in left ventricular function after aortic valve replacement for isolated aortic stenosis. Am J Cardiol. 1994;74:1142-1146.
55. Davies JE , Broyd C, Hadjiloizou N, Baksi J, Francis Dp, Foale Ra, parker KH, Hughes aD, Chukwuemeka a, Casula R, Malik Is, Mikhail gW, Mayet J. arterial pulse wave dynamics after percutaneous aortic valve replacement: Fall in coronary diastolic suction with increasing heart rate as a basis for angina symptoms in aortic stenosis. Circulation. 2011;124:1565-1572
56. Zhao Y, He Y. Echocardiographic Evaluation of cardiac function response to removal of aortic stenosis: surgical and trans-catheter aortic valve implantation. International Cardiovascular Forum 2013; 1: 16-18. 57. Willson aB , labounty TM, achenbach s, Moss R, Wheeler M, Thompson
C, Min JK, gurvitch R, Norgaard Bl, Hague CJ, Toggweiler s, Binder R, Freeman M, poulter R, poulsen s, Wood Da, leipsic J. 3-dimensional aortic annular assessment by multidetector computed tomography predicts moderate or severe paravalvular regurgitation after transcatheter aortic valve replacement: a multicenter retrospective analysis. J Am Coll Cardiol. 2012;59:1287-1294
58. Jilaihawi H , Fontana g, Furugen a, shiota T, Friede g, Makhija R, Doctor N, leon MB, Makkar RR. Cross-sectional computed tomographic assessment improves accuracy of aortic annular sizing for transcatheter aortic valve replacement and reduces the incidence of paravalvular aortic regurgitation. J Am Coll Cardiol. 2012;59:1275-1286
59. Quail Ma , schievano s, Reinthaler M, Mullen MJ, Taylor aM. use of cardiovascular magnetic resonance imaging for tavr assessment in patients with bioprosthetic aortic valves: Comparison with computed tomography. Eur J Radiol. 2012;http://dx.doi.org/10.1016/j.ejrad.2012.07.014 60 Reynolds MR, Magnuson Ea, lei Y, Wang K, Vilain K, li, H, Walczak
J, pinto Ds, Thourani VH, svenson lg, Mack MJ, Miller DC, satler lE, Bavaria J, smith CR, leon MB, Cohen DJ,; paRTNER investigators. Cost-effectiveness of transcatheter aortic valve intervention compared with surgical aortic valve replacement in high risk patients wth severe aortic stenosis: results of the paRTNER Cohort a. J Am Coll Cardiol. 2012;60(25):2683-92.
61. puls M, Eiffert H, Hunlich M, schondube F, Hasenfusse g, seipelt R, schillinger W. prosthetic valve endocarditis after transcatheter aortic valve implantation: the incidence in a single-centre cohort and reflections on clinical, echocardiographic, and prognostic features. EuroIntervention 2013; 8: 1407-18.
62. Eisen a, shpira Y, sagie a, Kornowski B. Infective endocarditis in the transcatheter aortic valve replacement era: comprehensive review of a rare complication.