PRECONCEPTION HEALTH: A STRATEGY TO IMPROVE BIRTH OUTCOMES IN NORTHEASTERN NORTH CAROLINA
By
Megan Carlucci
A paper presented to the faculty of The University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Public Health in the Department of
Maternal and Child Health. Chapel Hill, N.C.
November 2018
Approved by:
_____________________________ First Reader
Introduction
Northeastern North Carolina, which consists of seventeen counties that surround Albemarle Sound and share a border with Virginia, has some of the least favorable birth
outcomes in the state, including low birth weight and high infant mortality. Since North Carolina (NC) ranked 39th of the 50 states in infant mortality in 2016, poor outcomes within the state must be explored to find interventions that will push the needle forward in improving outcomes for women and their families (Tucker & Beatty, 2018). The average infant mortality rate among the 17 Northeastern counties was 8.3 infant deaths per 1,000 live births in the period 2012-2016, compared to a rate of 7.2 infant deaths per 1,000 live births in the same time period in NC. However, the range within the counties varies greatly, with Camden County reporting an infant mortality rate of 0 per 1,000 live births, and Hertford County reporting a rate of 19 per 1,000 live births. The previous five-year period saw a slightly higher infant mortality rate in the region, with an average infant mortality rate of 10.6 infant deaths per 1,000 live births. However, in five counties, the infant mortality rate increased, indicating some geographic disparities (NCDHHS, n.d.).Please see Figure 1 for an illustration of the distribution of infant mortality rates in Northeastern NC.
Figure 1: Infant Mortality Rate in Northeastern North Carolina
individual Northeastern NC counties. NC is divided into six Perinatal Care Regions (PCRs), and the Northeastern NC counties all fall into PCR VI, which covers Eastern NC. For 2012-2016, African Americans had 2.3 times the infant mortality rate as non-Hispanic whites. Non-Hispanic whites had a rate of 6.0 infant deaths per 1,000 live births, and African Americans had a rate of 13.9 per 1,000 live births. In comparison, NC has a slightly higher disparity ratio, with a 2.41 times higher rate of mortality for African American infants than for non-Hispanic white infants (NCDHHS, n.d.). These disparities follow an alarming national trend, where black infant
mortality is higher than white infant mortality in every state. Research has shown that structural racism, defined as racial inequity at a systemic level, contributes to these disparities significantly (Wallace, Crear-Perry, Richardson, Tarver, & Theall, 2017).
Low birth weight and preterm birth are the most frequent causes of infant and neonatal mortality in the US (Lau, Ambalavanan, Chakraborty, Wingate, & Carlo, 2013). Additionally, they are associated with higher risks of other short-term and long-term adverse health conditions. Low birth weight, defined as weight below 2500 grams, has also been connected to later health conditions like diabetes, high blood pressure, intellectual and developmental disabilities, and obesity (March of Dimes, 2018).Preterm birth, or babies born before 37 weeks of gestation, is associated with long term complications such as cerebral palsy, vision and hearing loss, and intellectual disability, and hypertension and diabetes later in life (Howson, Kinney, McDougall, Lawn, & Born Too Soon Preterm Birth Action Group, 2013). In Northeastern NC, the range of percent of babies born with low birth weight in 2012-2016 was a low of 6.2 percent in Dare County to a high of 12.5 percent in Edgecombe County, compared to 9 percent in NC
(NCDHHS, n.d.).The range of percent of babies born preterm in the same period was a low of 6.6 percent in Tyrell County to a high of 13.2 percent in Hertford County, compared to 10.1 percent in NC (NCDHHS, n.d.).
US are unintended, and unintended pregnancies are associated with worse outcomes such as delayed prenatal care, preterm birth, and negative physical and mental effects for children (Guttmacher Institute, 2016). Therefore, in order to reduce poor birth outcomes, a more holistic understanding of pregnancy must occur with the recognition that healthier women have
healthier pregnancies.
Fortunately, a paradigm shift has occurred over the past few decades, recognizing that to improve birth outcomes, proactive measures must be taken preconception and
interconception to ensure women and men of reproductive age “achieve optimal health and wellness, fostering a healthy life course for them and any children they may have” (Frayne, 2017). Preconception health (PCH) envisions a more holistic understanding of pregnancy and the entire reproductive life of all women and men. Using a life course approach, the PCH framework understands that the health of the mother prior to conception impacts her health during and after pregnancy, and the health of her offspring from conception into adulthood. Preconception health care (PCHC) involves a wide spectrum of interventions and health promotion, with the overall aim of reducing risk factors that could affect future pregnancies (Curtis, 2010).
This paper will outline the challenges women and infants face in the Northeastern NC region, and then discuss the advancement of PCH in the area as a solution to improve birth outcomes. It will then discuss how the NC Preconception Health Strategic Plan can provide a way to look at the status of PCH in Northeastern NC, and how the strategies can be adapted to suit the needs of that specific region.
Context
To understand the poor birth outcomes occurring in Northeastern NC and how PCH can improve those outcomes, it is important to first understand the historical and economic context of the region. PCH involves social determinants of health, which includes socioeconomic status, quality of education, housing conditions, and community resources that either support or hinder the wellbeing of women and their families.
History and Early Development
Northeastern NC consists of seventeen counties that surround Albemarle Sound and is bordered in the north by Virginia, and in the east by the Atlantic Ocean. Prior to European settlement, Algonquian-speaking tribes inhabited the area, including the Meherrin, Chowan, Weappomeoc, Moratok, Secotan, Hatteras, and Machapunga tribes (North Carolina
founded on Roanoke Island in 1587 and has become famous for its inhabitants’ mysterious disappearance just three years later (Hogeback, n.d.). Today the site serves as a tourist
attraction on the Outer Banks, where visitors can watch reenactments of events surrounding the colony’s founding and disappearance.
Following the Lost Colony, European settlement in NC slowed dramatically due to difficulty navigating the Outer Banks, high taxes from the Lord Proprietors, attacks by Native Americans, and weak government presence (North Carolina Museum of History, n.d.). NC finally found permanent footing as an English colony in 1705, when NC’s oldest town, Bath, was founded in current Beaufort County (East Carolina University Center for Survey Research, 2014). The Albemarle region was thus the first area settled by Europeans in NC. Newcomers, often arriving through Virginia, established farms scattered around the wilderness, and began to grow crops like corn, wheat, and tobacco (McIlvenna, 2007). Unlike Virginia, which had an established elite by the eighteenth century, NC primarily consisted of small farmers who owned less than 250 acres and relied on subsistence farming rather than cash crops (Barth, 2010). Slavery did not become a large part of the NC culture until the mid-eighteenth century, but between 1730 and 1755, the number of slaves in the colony increased from 6,000 to more than 18,000 as the population expanded and tobacco became an increasingly large part of the economy, particularly in the Northeast (Winer, n.d.). NC became a state in 1789 after joining the fight for independence during the Revolutionary War.
Economy
Today, the Northeastern region of NC is mostly rural. The area suffered during the Great Recession in the late 2000s and has continued to struggle in recovery. For example,
Edgecombe County went from an unemployment rate of 8 percent in 2006, to 15.7 percent in 2010. Tyrrell County saw a spike in unemployment from 5.8 percent to 14.8 percent in the same period (Bureau of Labor Statistics, 2017). Although recent unemployment numbers indicate that the region is slowly recovering, many counties have not yet returned to pre-Recession
employment levels. Both Edgecombe and Tyrrell County had unemployment rates of 8.6 percent and 8.4 percent in 2016, respectively (Bureau of Labor Statistics, 2017).The average unemployment rate in all 17 counties in 2016 was 6.8 percent, compared to NC’s rate of 5.1 percent (North Carolina Institute of Medicine, 2018). Additionally, income inequality in NC has reached historic heights, with the top 1 percent now making 20.6 times more than the bottom 99 percent, surpassing pre-Recession levels (Economic Policy Institute, n.d.).
19.9 percent, compared to the state rate of 15.4 percent. The range varied greatly, with a low of 8.7 percent in Camden County, and a high of 27.3 percent in Tyrrell County (North Carolina Institute of Medicine, 2018).Poverty has a high association with poor health outcomes, so the high rates of poverty in Northeastern NC are concerning. In the US, studies have found an association between higher income and longer lifespans (Chetty et al., 2016). Additionally, socioeconomic status and inequality has an impact on birth outcomes. In a comparison of four countries, Martinson and Reichman found that while low socioeconomic status was positively associated with low birth weight in all four countries, the inequalities were larger in the US due to a lack of social safety nets and universal health care (Martinson & Reichman, 2016).
Unemployment and economic distress create stress, and there is evidence showing that individuals in deteriorating financial situations also suffer from worse health. Pregnant women in particular are at risk from the effect of a stressful life change. In a 2014 analysis of Texas vital records from 1994 to 2003, Helen Scharber found that babies born to women who became unemployed during pregnancy weighed less than babies born to women who remained employed throughout pregnancy (Scharber, 2014). Kyle Carlson found similar results in his analysis of administrative data on mass layoffs and factory closings, concluding that bad news about the economy results in lower birth weights within the community (Carlson, 2015).
Economic distress is clearly connected with health, at a community and individual level. These situations are uniquely complicated when pregnancy is involved, as the mother worries about the future of her child.
Slow recovery from the recession has been accompanied by population decline over the past decade. Although NC’s population overall has steadily increased between 2010 and 2017, that growth has concentrated around urban areas. In fact, 13 of the 17 counties in Northeastern NC have experienced loss in population (NC Office of State Budget and Management, n.d.). Bertie County experienced the largest decrease in the state, with a 6.0 percent decline in population from 2010 to 2016 (NC Office of State Budget and Management, n.d.). Recent estimates predict further declines in many of these rural Northeastern counties. The UNC Carolina Population Center has reported that migration has occurred mostly among young people who often leave for economic reasons. Because of this, they predict continued
These demographic transitions may create a higher burden for individuals of
reproductive age as they take on caregiver roles for older relatives. Family caregivers of older relatives often experience stress and depression. Caregiving in rural areas can have more challenges, as individuals and families may be more isolated, not be aware of available services, or have difficulty accessing services due to distance (Butler, Turner, Kaye, Ruffin, & Downey, 2005). For someone of reproductive age, this could affect fertility decisions, and among pregnant women, the stress and depression could affect birth outcomes.
Access to Health Care
The residents of Northeastern NC share a similar problem with many rural areas in the United States- lack of access to health care services. In particular, there is an alarming shortage of obstetric services in rural areas, and labor and delivery departments are often the first to close when a hospital implements cost-saving measures. The problem is worsening, with 9 percent of US counties losing obstetric services between 2004 and 2014, resulting in nearly half of rural US counties having no hospital obstetric services by 2017 (Hung, Henning-Smith, Casey, & Kozhimannil, 2017). In 2016, eight counties in Northeastern NC had no birth attendants, and four had fewer than one birth attendant per 10,000 people (North Carolina Institute of Medicine, 2018). This is despite the fertility rate in the area (60.1 per 1,000
population, from 2012-2016) being only slightly lower than the state fertility rate (60.6 per 1,000 population, from 2012-2016) (NCDHHS, n.d.).
Preconception Health: A Strategy
PCH, which the CDC defines as “the health of women and men during their reproductive years” to “protect the health of a baby they might have sometime in the future”, started to gain traction as a necessary approach to improving birth outcomes in the 1980s (Centers for Disease Control and Prevention, 2014). The US Department of Health came out with an issue brief including the concept of “prepregnancy care” in 1979, followed soon by a publication by AAP, ACOG, and the March of Dimes in 1983 recommending that men and women be in “optimal physical health” prior to conception. Momentum continued to pick up, and in 1990, Healthy People 2000 included a specific objective for improving PCH in the United States (Freda, Moos, & Curtis, 2006). NC’s concern with PCHC followed a similar trajectory, with a North Carolina Institute of Medicine report about infant sickness and death in the late 1980s including an emphasis on women’s health before pregnancy. This report and other activities in the state eventually led to a Preconception Health Strategic Plan for 2008-2013 (Women’s Health Branch, 2008).
PCH is now a well-recognized framework to improve birth outcomes by improving women and men’s health during their reproductive years, but implementation faces challenges. Despite the prioritizing of PCH in public health organizations, there is a gap between messaging and practice, which can be exacerbated in rural areas due to less access to health care. In a qualitative survey of 19 physicians in rural central Pennsylvania, Chuang et al. found that providers did not prioritize planning for pregnancy during primary care visits. Physicians instead focused on contraceptive care, but none initiated conversations about PCH, partly because they did not believe the topic was part of their role (Chuang et al., 2012).A 2017 cross sectional study in South Dakota, a largely rural state, found low interest in receiving comprehensive PCHC among participants (55.8%) despite a majority believing PCHC could have positive effects on their health (87.6%) (Lammers, Hulme, Wey, Kerkvliet, & Arunachalam, 2017).
Part of the reason PCHC can be challenging to implement is the breadth of activities attached to it. PCH includes interventions that contribute to the whole health of the woman. For all women and men of childbearing age, reproductive life planning can be a meaningful and important tool, and it will be discussed further below. For women planning a pregnancy, PCHC involves traditional behavioral and biomedical changes like tobacco cessation, folic acid intake, HIV and STI screening and counseling, and management of chronic conditions such as
and Prevention, 2014). However, from a socio-ecological perspective, structural and
environmental factors outside individuals’ control can also greatly affect PCH. These factors can include housing quality, transportation access, education, and occupation. Inequalities in behaviors and chronic conditions that affect PCH are often influenced by social class and race, which are in turn influenced by public and social policies. For example, Hogan et al. explain that racialized policies that criminalize people of color and segregate neighborhoods have led to systemic inequalities in poverty (more African-Americans live below the poverty line compared to non-Hispanic whites) and unemployment (a higher proportion of African-Americans are unemployed than non-Hispanic whites). The authors’ analysis of these policies and other social factors describe how the exposures created by institutional racism negatively affect the health of African-American women, which in turn affects their PCH and the health of future children. Thus, the authors conclude, any PCH interventions and frameworks must focus on reforming institutions and structures rather than changing individual behavior (Hogan et al., 2013).
PCH is therefore best looked at from a life course perspective, which takes into account the structural, environmental, historical, and social context of an individual’s life to understand the protective and risk factors that have contributed to their health status and outcomes. Verbiest et. al offer recommendations for improving the health of men and women across the life course to ensure good health across the reproductive lifespan. These strategies, which include implementing universal health insurance, having active dialogues around issues like racism, privilege, and reproductive equity, and expanding opportunities to improve PCH with nontraditional partners all go beyond traditional health interventions (Verbiest, Malin,
Drummonds, & Kotelchuck, 2016). Overall, this vision of PCH asks maternal and child health professionals and their allies to expand their understanding of health interventions and involve community partners across public and private sectors.
Criticism
The emphasis on a woman’s health before pregnancy has given rise to some critics who worry that much PCH campaigning and messaging waxes judgmental and focuses on individual behavior rather than environmental exposures and structural discrimination. In her 2017 book, The Zero Trimester: Pre-Pregnancy Care and the Politics of Reproductive Risk, sociologist Miranda Waggoner offers several criticisms of the preconception health framework. Waggoner argues primarily that PCH treats women solely as vessels for babies, a critique grounded in feminist theory. She also raises doubts about the importance of PCH to birth outcomes, the lack of discussion around men’s PCH, and the emphasis on individual behavior rather than
These criticisms do have validity and deserve a response, particularly since messaging around PCH can become problematic and blaming very easily. For example, in 2016 the CDC came out with a statement recommending that sexually active women of reproductive age avoid drinking alcohol if they are not using birth control. This led to widespread condemnation through social media and publications, with the message being called “puritanical” and “out of step” with most women (Victor, 2016). Indeed, the term “preconception” health can be off putting. A 2015 survey of 65 women found that participants did not like the use of the term “preconception” because of the clinical nature of the word. Some women suggested that a more universal term be used, such as “women’s health” or “healthy lifestyles”, and that messaging geared toward women planning pregnancy use terms such as “positive planning.” The authors suggested creating distinct messages for women planning to become pregnant in the next two years and women who do not plan to become pregnant in the next two years, and they did not find an alternative term that appealed to all audiences. (Squiers et al., 2013)Although the terminology may be in dispute, PCH is still valuable as a framework within women’s health and infant health. While broad, it recognizes the impact women’s health throughout the life course has on their pregnancies and birth outcomes.
Additionally, evidence shows that PCHC is effective. Beckmann et al. conducted a case-control study of 56 women who attended PCHC services and 168 women who did not. They found that women who received PCHC were more likely to have healthier pregnancies than women who planned their pregnancies but did not attend a PCHC consultation. This included less weight gain pre-pregnancy, higher folic acid intake, and less than half the rates of preterm births (Beckmann, Widmer, & Bolton, 2014). Since nearly 50 percent of pregnancies are
unintended, however, PCH interventions cannot only focus on individual level interventions. At a population level, PCH interventions have also found success. In 1998, the US government began fortifying enriched cereal grain product flour with folic acid. As a result, the prevalence of babies born with neural tube defects has decreased by 35 percent in the US (Centers for Disease Control and Prevention, 2017).
the topic. The authors recommend that cohort studies be used to further explore how paternal exposures before conception contribute to their future children’s health (Braun, Messerlian, & Hauser, 2017).O’Brien et. al. described the unmet need for primary PCHC for men,
recommending that a care model for men should include information about health, fathering, and access to services to encourage reduction of risk factors shown to result in poor birth outcomes (O’Brien et al., 2018).In 2015, the Preconception Health and Health Care Initiative came out with a vision that included “the addition of men as a point of focus and intervention” (Verbiest, McClain, & Woodward, 2016).
Proponents of the PCH framework argue that efforts to improve PCH double as efforts to improve women’s health as a whole. Verbiest et al. describe PCH as “a critical component of a comprehensive women’s health package to improve maternal and infant health outcomes.” Additionally, PCH emphasizes family planning and contraceptive access, along with
reproductive life planning, therefore ensuring that men and women become parents only if and when they desire. Finally, with its broad approach, the PCH framework envisions a society where all men and women have an equal opportunity to be physically and mentally healthy and economically secure before having a child.
Preconception Health in a Rural Context: Implementing the NC Preconception Strategic Plan in Northeastern NC
As with many public health issues, improving PCH among men and women of reproductive age has unique challenges in a rural setting. Some of the barriers to providing preventive reproductive services in rural areas include poverty, difficulty in traveling to health services, lack of privacy in small and intimate communities, and conservative, stigmatizing attitudes towards sex (Chuang et al., 2012).The confluence of these factors creates a challenging environment to provide PCH services. Additionally, awareness of PCH among aged populations in rural areas is low. A cross-sectional survey of reproductive-aged women accessing community health services at the South Dakota Department of Health found that half of the women surveyed were uncertain or not interested in receiving
comprehensive PCHC. Participants who did express interest in PCH also reported 23% more PCH health interventions, indicating that PCH care requires active seeking by the target audience. The researchers concluded that the low interest might be caused by lack of
North Carolina’s Preconception Health Strategic Plan, created in 2008, envisions improving the health of women of reproductive age in NC “through a collaborative focus on women’s wellness” to “improve the quality of life for women as well as the health of infants” (NCDHHS, 2008). Specifically, the plan highlights six priority areas: pregnancy intendedness, obesity and related conditions, substance abuse, mental health, collaborative research on preconception-focused topics, and policy development and access to care. In response to input from stakeholders, the plan was updated in 2014 to include men in the target population, add life planning as a priority area, and redefine mental health and access to care as mental wellness and access to services, respectively (NC DHHS, 2014). In this section I will discuss each current state priority, present relevant data from Northeastern NC, and analyze relevant issues for the region. To further illustrate some of the PCH indicators discussed in this section, Appendix A has maps visualizing PCH-related county-level data.
Pregnancy Intendedness & Life Planning
NC’s PCH Strategic Plan listed pregnancy intendedness as one of the top priorities among the identified focus areas because unintended pregnancies are highly associated with poor birth outcomes (NCDHHS, 2008). Planning pregnancy allows men and women to reduce risk factors prior to pregnancy. This is why life planning was added to the NC PCH Strategic Plan in the 2014 supplement. Since pregnancy intendedness and life planning overlap in many ways, I will discuss them together.
Some of the main strategies to reduce unintended pregnancy include increasing access to birth control, providing comprehensive sex education to ensure women and men have the knowledge to plan when and if they want to have children, and encouraging individuals of reproductive age to establish a reproductive life plan. The American College of Obstetricians and Gynecologists (ACOG) has recommended comprehensive and culturally appropriate reproductive life planning as an essential strategy to reduce unintended pregnancies in the US (American College of Obstetricians and Gynecologists’ Committee on Health Care for
desired, and contextual life conditions such as employment and financial security, relationship status, chronic disease management, and other areas an individual feels are important to their reproductive choices.
To be successful, reproductive life planning needs to be paired with programs that increase access to and availability of effective contraceptive methods. A report from Guttmacher has shown that in Northeastern NC, approximately 28,000 women aged 13-44 were in need of publicly funded contraceptive services and supplies in 2014 (Frost, Frohwirth, & Zolna, 2016). Abortion access is equally essential to ensuring women have a choice regarding a pregnancy after conception. NC has some restrictions on abortion, including a 72 hour waiting period, an ultrasound requirement, and limited access to coverage under Marketplace or public health insurance plans. Additionally, a recent study found a drastic decline in abortion access in NC over the past few decades. Since 1980 the number of counties in the state reporting at least one abortion performed went from 38 counties to 11 counties in 2010. None of the counties in the Northeastern part of the state reported performing any abortion (Alvey et al., 2017).
Reproductive life planning and prevention of unintended pregnancy also require a foundational understanding of contraceptive options. The Healthy Youth Act was passed by the NC General Assembly in 2009 and requires that all 7th-9th grade students in NC public schools receive both abstinence-until-marriage and comprehensive sex education (General Assembly of North Carolina, 2009). However, the state did not provide a standard curriculum for use, and local school districts are responsible for determining what topics to teach in their district. As a result, there may be vast discrepancies in the quality of content students are given in different regions of the state. More work needs to be done to assess content quality in school districts around the state to address these potential differences.
Unintended pregnancy is an important piece of the conversation around PCH, since nearly half of all pregnancies in the US are unintended (Guttmacher Institute, 2016).
Unfortunately, there is a shortage of accurate local data. NC’s Process Outcome Objectives (POOs), which guides family planning services in the state, measures unintended pregnancy prevalence as the sum of abortions, births to teens 18 years old or younger, and out-of-wedlock births to women over 18 years of age divided by the number of pregnancies (Women’s Health Branch, 2018). However, the way this indicator is defined and measured makes invalid
numbers reported in NC’s POOs are therefore likely an overestimate, and unreliable. To better understand the burden of unintended pregnancy in Northeastern NC, better measurements are needed.
Obesity and Related Conditions
Over the past few decades, rates of obesity have increased among people of reproductive age. Being overweight or obese increases a person’s risk of certain chronic conditions, including hypertension, diabetes and cardiovascular disease. Obesity during pregnancy carries a higher risk of developing gestational diabetes and preeclampsia, and a higher risk for infants to be born with certain heart and neural tube defects, preterm, or stillborn. As a result, the recommendation is that women who are obese lose weight before getting pregnant to decrease risk of pregnancy complications (ACOG, 2016). The original NC PCH Strategic Plan emphasized obesity as a priority focus area, recognizing the extensive work that needs to be done in this area. Figure 2 outlines the prevalence of obesity and related risk factors at a regional and state level, along with a summary of the significance of those indicators. Overall, Northeastern NC is doing worse than NC in prevalence of obesity and diabetes rates.
Indicator Range Regional Average
NC Data Source Significance
Obesity Among
Women, 2013 (%) 26.2 (Dare) - 43.6(Edgecombe) 35.2 31.1
1 CDC Obesity rates across the United States have been consistently increasing over the past few decades. Obesity is associated with health conditions such as diabetes and hypertension, which can adversely affect a pregnancy.
Women with diabetes, 2013 (%)
9 (Dare) - 16.9 (Edgecombe)
13.5 10.2 CDC PCHC has been advised for women with diabetes for decades, because of high prevalence of congenital malformations among the offspring of women with diabetes. Women with diabetes also have a higher risk of spontaneous abortion. Studies of women with type 1 diabetes have shown an association between PCHC and a reduction in congenital malformations, as well as generally improved pregnancy outcomes (Temple, 2011). As the percentage of women with diabetes increases, PCHC for this population becomes more essential.
Women reporting leisure-time physical inactivity, 2013 (%)
24.7 (Currituck) -
34.3 (Hertford) 30.5 39.1 CDC The CDC recommends at least 150 minutes a week of moderate-intensity, or 75 minutes a week of vigorous intensity aerobic activity to improve cardiovascular, muscle and bone health. Exercise can help prevent chronic conditions such as high blood pressure, heart conditions, and diabetes (Centers for Disease Control and Prevention, 2018a).
Population With Low 0 (Gates) - 90 17.5 n/a NCIOM In rural communities, “food deserts” are defined as areas
Access to a Grocery
Store, 2015 (%)2 (Hyde) where median family income is lower than the surrounding area, and residents live more than 10 miles from a supermarket or grocery store. Residents of food deserts have lower fruit and vegetable intake and higher systolic blood pressure (Suarez et al., 2015). Living farther from a grocery store indicates fewer opportunities to access healthy foods.
Figure 2: Risk Factors Related to Obesity and Significance.
The region does better than the state in physical activity. In a CDC survey that asked, “During the past month, other than your regular job, did you participate in any physical activities or exercises such as running, calisthenics, golf, gardening, or walking for exercise?”, the
percent of women in all of NC who answered no was 39.1%, while the regional average percent of women who responded no in Northeastern NC was 30.5% (Centers for Disease Control and Prevention, 2018b). Additionally, the area has many public recreational facilities, including beaches, parks, and walking communities, and access to outdoor activities was listed as a strength by residents in multiple community health assessments (CHAs). These features could be further leveraged to improve population health. Collaborative efforts can be made to enhance access to these resources and implement programs to increase rates of physical activity for people of reproductive age. For example, employers can implement wellness programs, schools can encourage participation in sports and outdoor activities, and faith and community
organizations can increase structured recreational programs for families and individuals. Increased physical activity could help reduce rates of obesity and improve mental wellness.
Diet is another important piece of maintaining a healthy weight and preventing conditions such as diabetes. NC’s PCH Strategic Plan includes a goal to “increase the supply of healthy food that is easily accessible, affordable and culturally appropriate for women of childbearing age.” Strategies outlined to achieve this goal include addressing barriers to healthy foods, encouraging small store owners in underserved areas to carry healthier food items, increase affordability and availability of local food, connecting locally grown food to local retail
establishments, and advocating for local initiatives to improve access to healthy food (NCDHHS, 2008). Northeastern NC certainly has some work to do in this area.At 90 percent, Hyde County has the highest percentage of residents with low access to a grocery store in the region. The county is an outlier, with the next highest county at 30.6 percent (Dare County), but this indicates a critical issue that needs to be addressed. In the 2014 Hyde County CHA, focus group members identified limited access to healthy foods as a barrier to a healthy lifestyle. One
participant stated that Hyde County residents “have a lot of fast food in their diets”, and in a community survey, almost 25 percent of respondents reported eating fast food more than two days a week (Hyde County Health Department, Vidant Beaufort Hospital, The Outer Banks Hospital, & Hyde Partners for Health, 2015). In tailoring and adapting some of the strategies from the state plan for this area, local leaders and stakeholders should consider using local schools and faith communities as resources to implement programs like community gardens and cooking classes. Structural changes like opening farmer’s markets, grocery stores, and food banks in certain areas, and increasing awareness around food assistance programs like WIC and SNAP, are also essential to improving healthy food access in Northeastern NC. Mental Wellness
It is increasingly recognized that mental wellness is important to overall health. More research and interventions are being done to address perinatal and postpartum mental health, but there is a gap in research about preconception mental health. A population-based study found an association between poor preconception mental health and pregnancy complications (AOR 1.4, 95% CI: 1.02-1.92), having a miscarriage or stillbirth (AOR 1.48, 95% CI: 0.96-2.27), and having a low birth weight baby (AOR 1.99, 95% CI: 1.00-3.98) (Witt, Wisk, Cheng,
Hampton, & Hagen, 2012). Additionally, a woman’s own history of depression or bipolar disorder, or a family member’s diagnosis with depression or other mental illness is associated with an increased risk for developing postpartum depression (National Institute of Mental Health, n.d.). It is clear that a lifecourse approach should be used when addressing mental health, and that improving preconception mental health can have a positive effect on maternal and infant health.
The state strategic plan’s linguistic shift from “mental health” to “mental wellness” indicates a commitment to looking beyond diagnosable mental health conditions. The plan also includes emotional and spiritual health and recognizes that adverse events, social isolation and poor diet can lead to poor coping mechanisms like substance use. Therefore, they encourage strategies like promoting healthy activities that include exercise, friendships and meditation, educating non-traditional partners about mental wellness, and supporting programs that increase mental wellness (NC DHHS, 2014).
Some of these topics are particularly important in rural areas such as Northeastern NC. There is little county-level data available on mental health, but fourteen of the seventeen
Region 9 reported that their mental health was not good for at least 14 days out of the past 30 days. Among people of reproductive age (18-44), 20 percent of respondents reported their mental health was not good for at least 14 days out of the past 30 days. Participants with less than $50,000 in household income were more than twice as likely as those with at least $50,000 in household income to report poor mental health for at least 14 days (NC SCHS, 2017).
Improving mental wellness in a rural area like Northeastern NC needs to be collaborative and community-based. A common theme found in a review of the Northeastern NC CHAs is community resilience. Participants in a survey of Edgecombe County commented on the strong sense of community in the area, and participants in a Dare County survey noted that the sense of community was one of the best things about living in the county (Dare County Department of Health & Human Services, The Outer Banks Hospital, & Vidant Health System, 2016; Vidant Edgecombe Hospital, Edgecombe County Health Department, & East Carolina University, 2013). A resident of Hyde County remarked that “there are so many people that will step in to help if something needs to be done” (Hyde County Health Department et al., 2015). The community strength in this largely rural area could be a boon to improving mental wellness and PCH promotion overall, by limiting social isolation and utilizing the strong social infrastructure that exists.
Substance Abuse
Substance abuse, which includes dependence on tobacco, alcohol and/or drugs, is a common and concerning problem that affects people’s health, relationships, and general well-being in life. Consensus is very strong that alcohol, tobacco, and illicit substance use during pregnancy can result in adverse pregnancy outcomes such as preterm delivery, low birth weight, stillbirth, and infant mortality. Use of these substances outside pregnancy can also be harmful depending on dosage. Alcohol is the most commonly used substance, and in LHD Region 9, 31 percent of males and females surveyed reported heavy drinking (defined as more than two drinks a day for men and more than one drink a day for women) (NC SCHS, 2017). Tobacco use rates are also high, with the regional average of live births where the mother smoked during pregnancy at 12.5 percent, which is higher than the state average of 8.9 percent (NCDHHS, n.d.) (Figure 3). Although the opioid epidemic has been a major focus for public health over the past few years, there is limited data on rates of opioid use in Northeastern NC.
implementation of programs to combat drug, alcohol, and tobacco use, and working with community partners to raise awareness about substance abuse (NC DHHS, 2014).
Indicator Range Regional
Average NC Data Source Significance
Live Births Where Mother Smoked During Pregnancy, 2016 (%)
9.5 (Pasquotank) - 16.9 (Martin)
12.5 8.9 NCDHHS This does not capture electronic or other, non-cigarette products, so it is likely an undercounting.
Figure 3: Risk Factors Related to Substance Use.
Collaborative research on preconception-focused topics
Since PCH involves a broad understanding of health, which necessitates individual, community, and societal level interventions, improving PCH must include non-traditional partners. The NC PCH Strategic Plan calls for “influencers” in the community to develop and support programs that improve PCH. The plan recommends enlisting non-traditional partners from different sectors, including religious organizations, recreation departments, hair stylists and barbers, transportation services, and employers (NC DHHS, 2014). In many ways, this is particularly important for rural areas, where access to traditional health services may be limited or far, but communities are tight-knit.
Community coalitions should be created to raise awareness about PCH in the
community, to identify community needs, and to address the lack of local data. There are many gaps in the data available for the Northeastern counties because there is limited data on PCH collected on a county level. Further, it is difficult to find data that is disaggregated by sex and race/ethnicity, which could lead to difficulty tracking outcomes even if interventions are initiated in the region. Additionally, many state and national datasets do not do a good job capturing data in rural areas, and local residents rarely have assistance in analyzing any data they access. Finally, the low populations in some of the counties mean some of the rates can fluctuate widely. To address some of these data gaps, local partnerships could be established to share data or find new ways to collect data. For example, CHAs could be better utilized in collecting targeted information on PCH indicators.
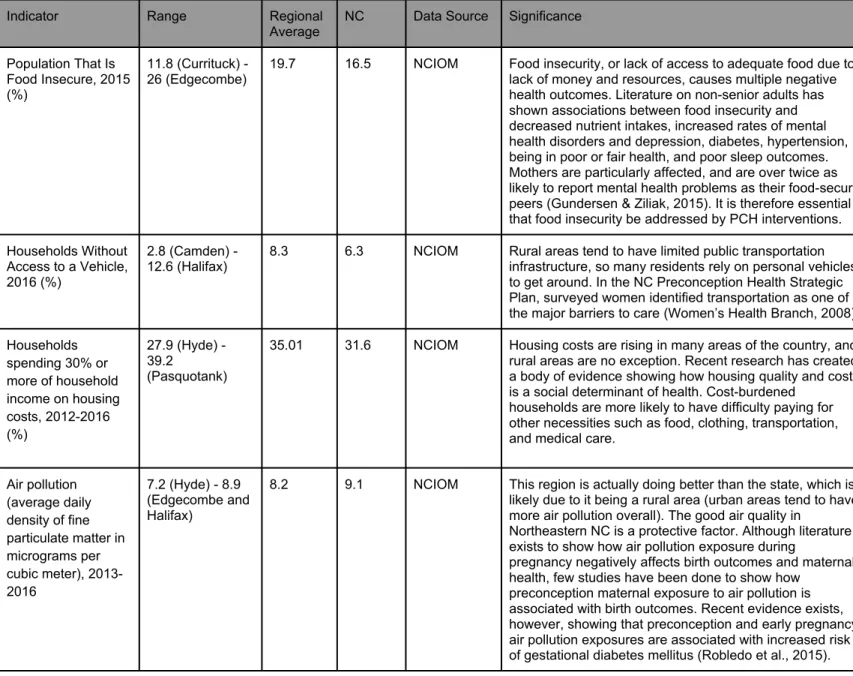
Some of these exposures have resulted in reproductive effects in farmworkers and their families (NC Farmworker Institute, 2008). Additionally, other environmental and structural conditions such as poverty, food insecurity, pollution, and affordable housing are factors that affect PCH, as described above in this paper. Figure 4 displays some of the available county-level data that illuminates how these structural conditions affect Northeastern NC.
Indicator Range Regional Average
NC Data Source Significance
Population That Is Food Insecure, 2015 (%)
11.8 (Currituck) -
26 (Edgecombe) 19.7 16.5 NCIOM Food insecurity, or lack of access to adequate food due to lack of money and resources, causes multiple negative health outcomes. Literature on non-senior adults has shown associations between food insecurity and decreased nutrient intakes, increased rates of mental health disorders and depression, diabetes, hypertension, being in poor or fair health, and poor sleep outcomes. Mothers are particularly affected, and are over twice as likely to report mental health problems as their food-secure peers (Gundersen & Ziliak, 2015). It is therefore essential that food insecurity be addressed by PCH interventions.
Households Without Access to a Vehicle, 2016 (%)
2.8 (Camden) - 12.6 (Halifax)
8.3 6.3 NCIOM Rural areas tend to have limited public transportation infrastructure, so many residents rely on personal vehicles to get around. In the NC Preconception Health Strategic Plan, surveyed women identified transportation as one of the major barriers to care (Women’s Health Branch, 2008).
Households spending 30% or more of household income on housing costs, 2012-2016 (%)
27.9 (Hyde) - 39.2
(Pasquotank)
35.01 31.6 NCIOM Housing costs are rising in many areas of the country, and rural areas are no exception. Recent research has created a body of evidence showing how housing quality and cost is a social determinant of health. Cost-burdened
households are more likely to have difficulty paying for other necessities such as food, clothing, transportation, and medical care.
Air pollution (average daily density of fine particulate matter in micrograms per cubic meter), 2013-2016
7.2 (Hyde) - 8.9 (Edgecombe and Halifax)
8.2 9.1 NCIOM This region is actually doing better than the state, which is likely due to it being a rural area (urban areas tend to have more air pollution overall). The good air quality in
Northeastern NC is a protective factor. Although literature exists to show how air pollution exposure during
pregnancy negatively affects birth outcomes and maternal health, few studies have been done to show how
preconception maternal exposure to air pollution is associated with birth outcomes. Recent evidence exists, however, showing that preconception and early pregnancy air pollution exposures are associated with increased risk of gestational diabetes mellitus (Robledo et al., 2015).
Figure 4: Risk Factors Related to Environmental and Social Indicators.
Policy development and access to services
there are other policies that could benefit all men and women of childbearing age. Access to health care has become a well-documented recommendation for improving population health. The US is one of the few developed countries without universal health care and, as a
consequence, US citizens face unique barriers to accessing health care. In particular,
unemployed and low-income people rely on public insurance programs created to fill some of the gaps of the patchy health insurance system currently in place. Historically, eligibility
categories for Medicaid included pregnant women and mothers of children 18 and younger, but not childless women. The Affordable Care Act (ACA) gave states the option to eliminate
categories and allow any adult with an income less than 138% of the Federal Poverty Level (FPL) to enroll in Medicaid. However, as of 2018 fourteen states, including NC, have opted not to expand Medicaid (The Henry J. Kaiser Family Foundation, 2018). Therefore, childless adults and parents of children 18 or older above 43% FPL are excluded from Medicaid coverage in NC, but do not qualify for financial assistance under Marketplace plans unless they are above 100% FPL. In 2016, approximately 208,000 people fell into the coverage gap in NC (Garfield, Damico, & Orgera, 2018).
Since women and men of reproductive age without children fall into the coverage gap in NC, PCH for this population is affected by non-expansion of Medicaid. One of the identified focus areas by NC’s PCH Strategic Plan is Access to Services, and it specifically identifies increasing the number of women and men with a medical home as an objective to improve PCH (NC DHHS, 2014). To accomplish this goal, health insurance must be made available and affordable to all individuals. Research supports health coverage as a strategy for improving PCH. A study of women in New York City found that women with private or public health insurance before pregnancy had a better PCH score than women with no insurance. However, this positive association did not occur among the non-white population, indicating interventions to improve PCH must go beyond health insurance coverage (Hawks, McGinn, Bernstein, & Tobin, 2018).
salons, and barbershops. By taking advantage of the social network already in place, the community can connect people to existing services.
Conclusion
Bibliography
ACOG. (2016, April). Obesity and Pregnancy. Retrieved November 1, 2018, from https://www.acog.org/Patients/FAQs/Obesity-and-Pregnancy.
Alvey, J., Bryant, A. G., Curtis, S., Speizer, I. S., Morgan, S. P., Tippett, R., Hodgkinson, J. C., et al. (2017). Trends in Abortion Incidence and Availability in North Carolina, 1980-2013. Southern Medical Journal, 110(11), 714–721.
American College of Obstetricians and Gynecologists’ Committee on Health Care for Underserved Women. (2016). Committee opinion no. 654: reproductive life planning to reduce unintended pregnancy. Obstetrics and Gynecology, 127(2), e66-9.
Barth, J. E. (2010). “The Sinke of America”: Society in the Albemarle Borderlands of North Carolina, 1663-1729. Society in the Albemarle Borderlands of North Carolina, 87(1).
Beckmann, M. M., Widmer, T., & Bolton, E. (2014). Does preconception care work? The Australian & New Zealand Journal of Obstetrics & Gynaecology, 54(6), 510–514.
Braun, J. M., Messerlian, C., & Hauser, R. (2017). Fathers matter: why it’s time to consider the impact of paternal environmental exposures on children’s health. Current epidemiology reports, 4(1), 46–55.
Bureau of Labor Statistics. (2017). Local Area Unemployment Statistics. Retrieved September 19, 2018, from https://www.bls.gov/lau/#cntyaa
Burke, B., & Daniel, K. (2009). Preventing Neural Tube Birth Defects: A Prevention Model and Resource Guide. CDC.
Butler, S. S., Turner, W., Kaye, L. W., Ruffin, L., & Downey, R. (2005). Depression and
caregiver burden among rural elder caregivers. Journal of gerontological social work, 46(1), 47–63.
Carlson, K. (2015). Fear itself: The effects of distressing economic news on birth outcomes. Journal of Health Economics, 41, 117–132.
Centers for Disease Control and Prevention. (2014, August 29). Before Pregnancy. Retrieved September 20, 2018, from https://www.cdc.gov/preconception/overview.html
Centers for Disease Control and Prevention. (2017, November 3). Folic acid fortification continues to prevent NTDs . Retrieved October 6, 2018, from
https://www.cdc.gov/ncbddd/folicacid/features/folicacid-prevents-ntds.html
https://www.cdc.gov/cancer/dcpc/prevention/policies_practices/physical_activity/ guidelines.htm
Centers for Disease Control and Prevention. (2018b, March 14). Diabetes Data & Statistics. Retrieved November 2, 2018, from https://www.cdc.gov/diabetes/data/
Chetty, R., Stepner, M., Abraham, S., Lin, S., Scuderi, B., Turner, N., Bergeron, A., et al. (2016). The Association Between Income and Life Expectancy in the United States, 2001-2014. The Journal of the American Medical Association, 315(16), 1750–1766.
Chuang, C. H., Hwang, S. W., McCall-Hosenfeld, J. S., Rosenwasser, L., Hillemeier, M. M., & Weisman, C. S. (2012). Primary care physicians’ perceptions of barriers to preventive reproductive health care in rural communities. Perspectives on Sexual and Reproductive Health, 44(2), 78–83.
Curtis, M. (2010). Preconception Care: Clinical and Policy Implications of the Preconception Agenda. Journal of clinical outcomes management : JCOM, 17(4), 167–172.
Dare County Department of Health & Human Services, The Outer Banks Hospital, & Vidant Health System. (2016). 2016 Dare County Community Health Assessment. Dare County Department of Health & Human Services.
East Carolina University Center for Survey Research. (2014). Beaufort County Community Health Needs Assessment. East Carolina University Center for Survey Research.
Economic Policy Institute. (n.d.). Interactive: The Unequal States of America. Retrieved October 5, 2018, from https://www.epi.org/multimedia/unequal-states-of-america/
Frayne, D. J. (2017, May 23). A Paradigm Shift in Preconception and Interconception Care: The Right Time is Every Time. Presented at the Zero to Three Webinar.
Freda, M. C., Moos, M.-K., & Curtis, M. (2006). The history of preconception care: evolving guidelines and standards. Maternal and Child Health Journal, 10(5 Suppl), S43-52.
Frost, J. J., Frohwirth, L. F., & Zolna, M. R. (2016). Contraceptive Needs and Services, 2014 Update. Guttmacher Institute.
Garfield, R., Damico, A., & Orgera, K. (2018). The Coverage Gap: Uninsured Poor Adults in States that Do Not Expand Medicaid. The Henry J. Kaiser Family Foundation.
General Assembly of North Carolina. (2009). House Bill 88.
Gundersen, C., & Ziliak, J. P. (2015). Food insecurity and health outcomes. Health Affairs (Project Hope), 34(11), 1830–1839.
Guttmacher Institute.
Guttmacher Institute. (2017). Adolescent Sexual and Reproductive Health in the United States. Guttmacher Institute.
Hawks, R. M., McGinn, A. P., Bernstein, P. S., & Tobin, J. N. (2018). Exploring Preconception Care: Insurance Status, Race/Ethnicity, and Health in the Pre-pregnancy Period. Maternal and Child Health Journal, 22(8), 1103–1110.
Health ENC. (2018). Community Dashboard. Health ENC. Retrieved September 20, 2018, from http://www.healthenc.org/indicators/index/dashboard?alias=alldata
Hogan, V. K., Culhane, J. F., Crews, K. J., Mwaria, C. B., Rowley, D. L., Levenstein, L., & Mullings, L. P. (2013). The impact of social disadvantage on preconception health, illness, and well-being: an intersectional analysis. American Journal of Health Promotion, 27(3 Suppl), eS32-42.
Hogeback, J. (n.d.). The Lost Colony of Roanoke. Britannica. Retrieved September 20, 2018, from https://www.britannica.com/story/the-lost-colony-of-roanoke
Howson, C. P., Kinney, M. V., McDougall, L., Lawn, J. E., & Born Too Soon Preterm Birth Action Group. (2013). Born too soon: preterm birth matters. Reproductive Health, 10 Suppl 1, S1.
Hung, P., Henning-Smith, C. E., Casey, M. M., & Kozhimannil, K. B. (2017). Access To
Obstetric Services In Rural Counties Still Declining, With 9 Percent Losing Services, 2004-14. Health Affairs (Project Hope), 36(9), 1663–1671.
Hyde County Health Department, Vidant Beaufort Hospital, The Outer Banks Hospital, & Hyde Partners for Health. (2015). 2014 Hyde County Community Health Assessment. Hyde County Health Department.
Lammers, C. R., Hulme, P. A., Wey, H., Kerkvliet, J., & Arunachalam, S. P. (2017).
Understanding women’s awareness and access to preconception health care in a rural population: A cross sectional study. Journal of Community Health, 42(3), 489–499.
Lau, C., Ambalavanan, N., Chakraborty, H., Wingate, M. S., & Carlo, W. A. (2013). Extremely low birth weight and infant mortality rates in the United States. Pediatrics, 131(5), 855–860.
March of Dimes. (2018, March). Low birthweight. March of Dimes. Retrieved September 20, 2018, from https://www.marchofdimes.org/complications/low-birthweight.aspx
McIlvenna, N. (2007). Settlers of the Albemarle. Tar Heel Junior Historian.
Morse, J. E., & Moos, M.-K. (2018). Reproductive life planning: raising the questions. Maternal and Child Health Journal, 22(4), 439–444.
Mullen, C. (2011, November). The Affordable Care Act and Preconception Health. Pulse.
National Institute of Mental Health. (n.d.). Postpartum Depression Facts. Retrieved November 2, 2018, from https://www.nimh.nih.gov/health/publications/postpartum-depression-facts/ index.shtml
NC DHHS. (2014). North Carolina Preconception Health Strategic Plan Supplement 2014-2019. NC DHHS.
NC DHHS. (2008). North Carolina Preconception Health Strategic Plan: September 2008-September 2013. NCDHHS.
NC DHHS (n.d.). NC SCHS: Statistics and Reports: County Health Data Book. Retrieved September 19, 2018, from https://schs.dph.ncdhhs.gov/data/databook/
NC Farmworker Institute. (2008). North Carolina Farmworker Health.
NC Office of State Budget and Management. (n.d.). State Demographer. NC Budget and Management. Retrieved September 20, 2018, from https://www.osbm.nc.gov/
NC SCHS. (2017, August 15). BRFSS: Survey Results 2016. Retrieved October 31, 2018, from https://schs.dph.ncdhhs.gov/data/brfss/2016/
North Carolina Commission of Indian Affairs. (1983). North Carolina Indians. North Carolina, United States: NC Commission of Indian Affairs.
North Carolina Institute of Medicine. (2018). NC County Health Data. Retrieved September 20, 2018, from http://nciom.org/map/
North Carolina Museum of History. (n.d.). Settlement and Migration | NC Museum of History. North Carolina Museum of History. Retrieved September 20, 2018, from
https://www.ncmuseumofhistory.org/workshop/nc-geography/session-1
O’Brien, A. P., Hurley, J., Linsley, P., McNeil, K. A., Fletcher, R., & Aitken, J. R. (2018). Men’s Preconception Health: A Primary Health-Care Viewpoint. American journal of men’s health, 12(5), 1575–1581.
(2015). Preconception and early pregnancy air pollution exposures and risk of gestational diabetes mellitus. Environmental Research, 137, 316–322.
Scharber, H. (2014). Does “Out of Work” Get into the Womb? Exploring the Relationship between Unemployment and Adverse Birth Outcomes. Journal of Health and Social Behavior, 55(3), 266–282.
Squiers, L., Mitchell, E. W., Levis, D. M., Lynch, M., Dolina, S., Margolis, M., Scales, M., et al. (2013). Consumers’ perceptions of preconception health. American Journal of Health Promotion, 27(3 Suppl), S10-9.
Stanford, J. (2017, July 5). Examining Decline in North Carolina’s Municipalities. Carolina Demography. Retrieved September 20, 2018, from
https://demography.cpc.unc.edu/2017/07/05/examining-decline-in-north-carolinas-municipalities/
Suarez, J. J., Isakova, T., Anderson, C. A. M., Boulware, L. E., Wolf, M., & Scialla, J. J. (2015). Food access, chronic kidney disease, and hypertension in the U.S. American Journal of Preventive Medicine, 49(6), 912–920.
Temple, R. (2011). Preconception care for women with diabetes: is it effective and who should provide it? Best Practice & Research. Clinical Obstetrics & Gynaecology, 25(1), 3–14.
The Henry J. Kaiser Family Foundation. (2018, September 11). Status of State Action on the Medicaid Expansion Decision. KFF. Retrieved October 1, 2018, from
https://www.kff.org/health-reform/state-indicator/state-activity-around-expanding-medicaid-under-the-affordable-care-act/?currentTimeframe=0&sortModel=%7B%22colId
%22:%22Location%22,%22sort%22:%22asc%22%7D
Tippett, R. (2014, December 4). NC in Focus: Unauthorized Immigrant Population. Carolina Demography. Retrieved October 6, 2018, from
https://demography.cpc.unc.edu/2014/12/04/nc-in-focus-unauthorized-immigrant-population/
Tucker, W., & Beatty, L. (2018). Giving Birth in North Carolina Is Still A Risky Business: Promoting Women’s Health to Improve Birth Outcomes. NC Child.
Verbiest, S., Malin, C. K., Drummonds, M., & Kotelchuck, M. (2016). Catalyzing a reproductive health and social justice movement. Maternal and Child Health Journal, 20(4), 741–748.
Verbiest, S., McClain, E., & Woodward, S. (2016). Advancing preconception health in the United States: strategies for change. Upsala journal of medical sciences, 1–5.
Vidant Edgecombe Hospital, Edgecombe County Health Department, & East Carolina University. (2013). Edgecombe County Community Health Assessment. Edgecombe County Health Department.
Waggoner, M. R. (2017). The zero trimester: Pre-pregnancy care and the politics of reproductive risk. Oakland, California: University of California Press.
Wallace, M., Crear-Perry, J., Richardson, L., Tarver, M., & Theall, K. (2017). Separate and unequal: Structural racism and infant mortality in the US. Health & Place, 45, 140–144.
Winer, S. (n.d.). A brief history of slavery in North Carolina. NC Runaway Slave Advertisements. Retrieved September 20, 2018, from
http://libcdm1.uncg.edu/cdm/history/collection/RAS#ftnt4
Witt, W. P., Wisk, L. E., Cheng, E. R., Hampton, J. M., & Hagen, E. W. (2012). Preconception mental health predicts pregnancy complications and adverse birth outcomes: a national population-based study. Maternal and Child Health Journal, 16(7), 1525–1541.
Women’s Health Branch. (2008). North Carolina Preconception Health Strategic Plan: September 2008-September 2013. NC DHHS.
Women’s Health Branch. (2018). Process Outcome Objectives: SFY2018-2019 Family Planning Agreement Addenda Data.