The Experience of Pediatric Sibling Bone Marrow Transplant Donors: A Literature Review
By: Erin Mares
Senior Honors Thesis Bachelor of Science in Nursing University of North Carolina at Chapel Hill
April 13th, 2020
Approved:
2
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS Abstract
The Experience of Pediatric Sibling Bone Marrow Transplant Donors: A Literature Review Introduction
Hematopoietic stem cell transplantation (HSCT) is a routinely used treatment for children suffering from malignant and non-malignant hematopoiesis disorders (D’Auria, Fitzgerald, Presler, & Kasow, 2015). A HSCT is the process of infusing healthy hematopoietic stem cells into the body to reestablish bone marrow function in the affected individual (Vogel 2011). The cells used for transplant can either be extracted from the bone marrow or the peripheral blood (Switzer, Bruce, & Kiefer, 2016). Recipients can receive this treatment in two ways: either autologous, the use of their own cells, or allogenic, the use of a donor’s (related or unrelated) cells (Bollard, Krance, & Heslop, 2011). The success of an allogenic HSCT transplantation is based on how similar the donors and recipients human leukocyte antigen (HLA) are to each other (D’Auria et al., 2015). Since full siblings share biological parents and have a 25% chance of having identical HLA, HLA-matched siblings are considered the donor of choice in allogenic transplants (D’Auria et al., 2015). These siblings are preferred over other donors because there is a greater rate of success due to a lower risk of graft-versus-host disease and graft rejection, two complications of HCST transplant (Committee on Bioethics, 2010).
Conventional bone marrow donation is a procedure where stem cells are collected from the bone marrow space, most often in the posterior iliac crest, using needle aspiration (Vogel 2011). The procedure is usually done in the operating room under general anesthesia and the needle is passed approximately 50-200 times (Vogel 2011). This procedure is considered
4
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
tissue injury (Bendorf and Kerridge, 2011; Committee on Bioethics, 2010; Styczynski et al., 2012).
Sibling donors not only suffer from potential physical harm, but psychological and psychosocial problems may present themselves as well. Psychological challenges, such as emotional distress and poor cognitive function, is often experienced by siblings of children with chronic illnesses and can lead to a negative impact on the sibling’s development (White,
Hendershot, & Dixon, 2017). However, the psychological issues associated with sibling bone marrow transplant donors is only partially related to their sibling. It also includes other stressors stimulated by the donation process, such as not having a choice in the decision to be a donor, responsibility for the outcome of the recipient, not being adequately prepared on what to expect, and lack of support (Committee on Bioethics, 2010; Pentz, Alderfer, & Pelletier, 2014; Weaver, Diekema, Carr, & Triplett, 2015; Wiener et al. 2019).
In order to decrease the negative complications associated with bone marrow donation, the American Academy of Pediatrics created guidelines that must be met for minors to ethically participate as hematopoietic stem cell donors (2010). The criteria are as follows: (1) there is no histocompatible adult relative who is willing or able to donate, (2) there is a strong personal and emotionally positive relationship between the donor and the recipient, (3) there is some
experience psychological benefit from improved family relationships and a stronger sense of self (Wiener et al. 2019).
In the United States, about one third of the pediatric HSCTs performed involve a donor who is both a sibling of the recipient and under the age of 18 (Wiener et al. 2019). However, there is minimal information regarding the sibling experience with bone marrow transplant donation (Committee on Bioethics, 2010). Specifically, limited knowledge exists concerning the psychological, psychosocial, emotional, and physical impacts of being a sibling bone marrow transplant donor. This literature review of the current research strives to answer the following question: What are the experiences of pediatric sibling bone marrow transplant donors?
Methods
This literature review was conducted following the methodology described by
Whittemore and Knafl (2005), including problem identification, literature search, data analysis, and organization. CINAHL, PubMed, and PsychInfo were searched using the key terms
“psychosocial OR psychological OR quality of life OR stress OR stressors OR social support” “Bone marrow transplant OR bone marrow transplantation OR hematopoietic stem cell
transplant” “sibling OR siblings OR brother OR brothers OR sister OR sisters” “donor” “pediatrics”. Hand searches of the references of articles were also conducted.
6
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
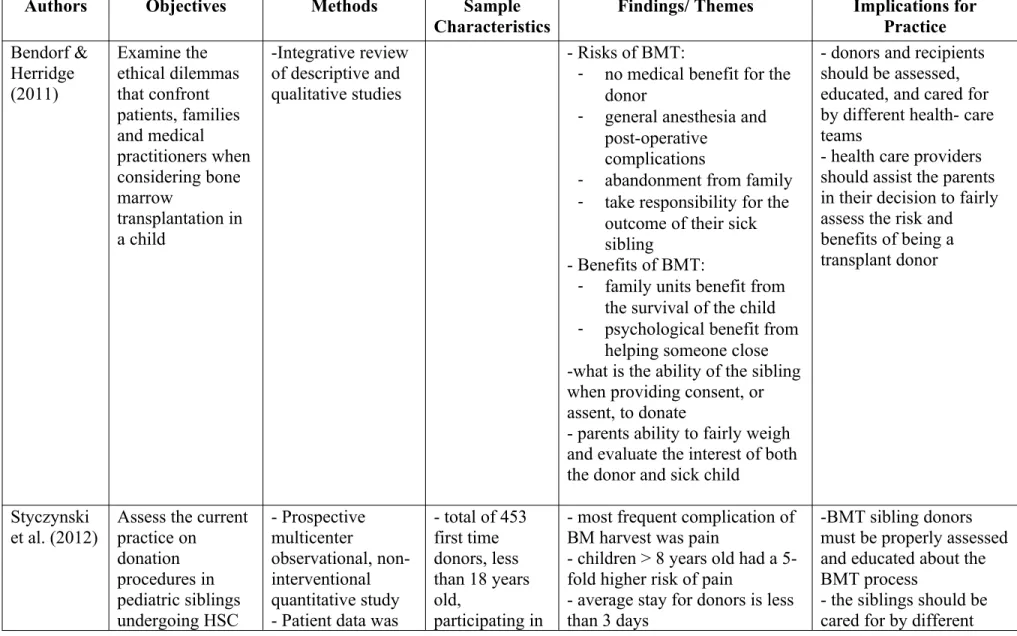
The selected articles were reviewed and analyzed for common themes. Information extracted from the articles were organized into a matrix, including references, objectives of the research, methods used to conduct the research, sample characteristics, themes, and implications for nursing practice. The matrix can be found in Table A. The matrix facilitated organization of the data set, and allowed information extracted from each source to be more easily compared to the rest of the studies.
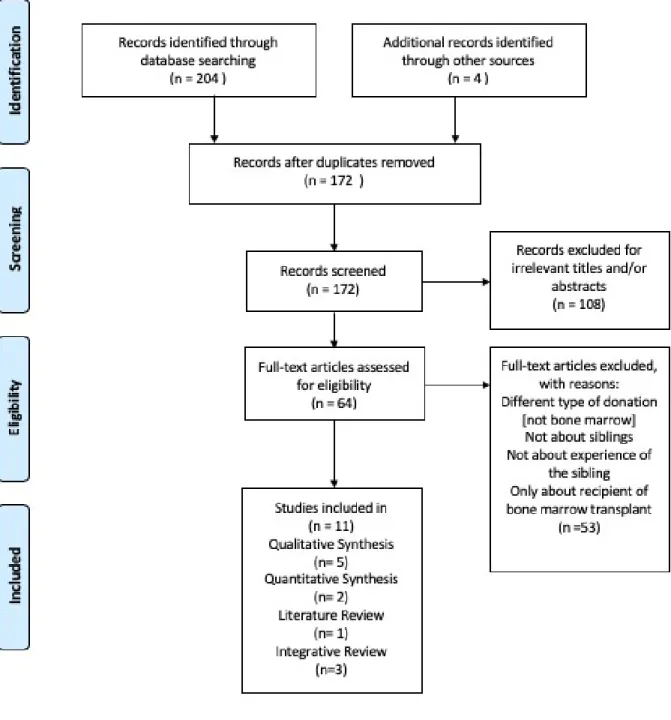
Inclusion Criteria
Figure A: PRISMA 2009 flow diagram*
From: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for
Running Head: THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
Table A: Summary of the experiences of sibling bone marrow transplant donors
Authors Objectives Methods Sample
Characteristics
Findings/ Themes Implications for Practice Bendorf & Herridge (2011) Examine the ethical dilemmas that confront patients, families and medical practitioners when considering bone marrow transplantation in a child -Integrative review of descriptive and qualitative studies
- Risks of BMT:
- no medical benefit for the donor
- general anesthesia and post-operative
complications
- abandonment from family - take responsibility for the
outcome of their sick sibling
- Benefits of BMT:
- family units benefit from the survival of the child - psychological benefit from
helping someone close -what is the ability of the sibling when providing consent, or assent, to donate
- parents ability to fairly weigh and evaluate the interest of both the donor and sick child
- donors and recipients should be assessed, educated, and cared for by different health- care teams
- health care providers should assist the parents in their decision to fairly assess the risk and benefits of being a transplant donor
Styczynski et al. (2012)
Assess the current practice on donation procedures in pediatric siblings undergoing HSC - Prospective multicenter observational, non-interventional quantitative study - Patient data was
- total of 453 first time donors, less than 18 years old,
participating in
- most frequent complication of BM harvest was pain
- children > 8 years old had a 5-fold higher risk of pain
- average stay for donors is less than 3 days
-BMT sibling donors must be properly assessed and educated about the BMT process
collection as well as describe adverse events or complications of BM harvest and PBSC collection
collected from donor medical history and physical exam
- functional impairment status was assessed using the Lansky/
Karnofsky score
38 EBMT
centers - life threatening complication indonors are rare (0.39%) and are related to general anesthesia - Children under 4 years belong to the highest risk group for complications
- Children under 4 undergoing BM harvest were at higher risk for anemia and the need for a blood transfusion after donation
health- care teams - the health care team should assist the parents in making decisions that treat each child as their own
Erden et al. (2019) Analyze the development of psychopathology in recipients, donors siblings, and nondonor siblings during the BMT process to determine if sibling donors are affected more than nondonor siblings - Qualitative, Cross-Sectional Study - Semi-structured interviews conducted
- Assessed mental health using Kiddie Schedule for Affective Disorders and Schizo- phrenia (KSADS), Children’s Depression Inventory, State- Trait Inventory for Children, State- Trait Inventory, and the Rosenberg Self-Esteem Scale -Sociodemographic and Clinical
Information Form
- Children and families whose transplantation was successful. 20 donor siblings, 30 nondonor siblings, 30 recipients, and parents of the participants. Siblings ages ranged from 6 to 18 years old.
-depressive symptoms were higher in the donor group when compared to both the nondonor and recipient’s groups
-depressive disorder rates were high during the period before and after transplantation in donor siblings
- Anxiety scores were higher in the donor group then compared to the nondonor groups
- Children in the donor group where found to have higher self-esteem when compared to the BMT recipients
- positive correlation found between anxiety scores and self-esteem scores in the donor group
-Depression scores were above the cutoff for the depressive scale in all three groups
- assist sibling bone marrow donors with the psychological and emotional distress that they may experience during the donation process
- provide the sibling donator with an
independent medical team including child a life specialist, a social worker, a nurse, and a physician
- assent should be collect if applicable because the sibling has better
10
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS included
sociodemographic characteristics, developmental, mental disease, and medical history
before parental consent -utilize a third party focused on the best interest of the sibling donor
- Sibling donors should undergo physiological and psychosocial
assessments to determine if the child is fit for donation D’Auria et al. (2015) Understand the perceptions of pediatric sibling donors who participated in a successful transplant outcome -Grounded Theory Exploratory Qualitative Study - Semi-Structured, open ended Interview guide utilized
- 8 donors of successful transplants with ages ranging from 2 to 23 years old with a median age of 13 years.
- siblings felt that they were “saving their sisters or brothers life”
- 5 themes:
1. Being a perfect match: pressure of being the match, fear of the labs and tests
2. Stepping Up: donors felt they needed to do the procedure to save a life, there was no choice 3. Worrying about the
Outcome: sibling donors felt responsible for the outcome of the procedure
4. The Waiting Process: sibling donors lacked knowledge about the recovery process 5. Sharing a Special
- donor and nondonor siblings are at risk for developing psychiatric diseases due to the BMT process
Bond: the donors felt closer to the recipient. It was a source of pride for the siblings
- Successful transplant can positively contribute to emotional and social development
- being a young donor strengthen the sibling bond during early to mid-adolescents - emotional benefit of saving a life outweighs the physical pain of the process
Pulsipher et al. (2019)
Assess the levels of pain,
symptoms, and long-term
recovery in BM or PBSC transplant sibling donors
- Quantitative Cohort study - Phone interviews conducted by the CIBMTR Survey Research Group - Pre-donation and post-donation forms included the
patients’ medical history and specifics of their donation
- Toxicity measured using the Modified Toxicity Criteria and Common Toxicity Criteria
-294 pediatric first or second time BM or PBSC sibling donors. All participants were less than 18 years old. The sample was broken into different age groups to compare findings (0-6 years old, 7-12 years old, and 13-18 years old)
- 24-48 hours post donation, patients reported skeletal, back, hip, and throat pain.
- The rate and intensity of pain and toxicity increased with age - older donators (13-17 years old) reported pain 80% of the time. 44% of these participants reported grade 2-4 (moderate- disabling) symptoms
- female donors reported more grade 2-4 pain
- older children had higher risk of failure to return to pre-donation levels of pain and toxicity at 1 month and I year after donation
- females aged 13-17 have a
12
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
Scale fold greater risk of having pain
when compared to younger males
- majority of donors experience mild to moderate temporary discomfort with full recovery Bauk et al.
(2013)
Explorer and describe the emerging body of published research literature focused on the experiences of pediatric HSCT donors
-Integrated Review - Research articles included focused on the experiences of pediatric sibling HSCT donors.
- Age of the donors across all studies were 11 to 19.6 years old
- sibling donors under 18 years old reported lower levels of anxiety compared to older donors due to a less complete understanding of the transplant process
-no choice in the donation decision
- improved sibling relationship - brought the family closer and led to improved family
relationships
- improved school performance - anxiety, depression, guilt, anger, low self-esteem, psychological distress, and behavioral problems were reported
- isolation and separation from the family
- siblings of recipients where BMT failed lead to greater feelings of guilt and responsibility
- donor siblings reported that they needed more support from
-Educate parents and health care providers about the donors experience: physically, psychologically, and emotionally
providers during the transplant trajectory
- donors under the age of 18 felt that the information about the donation process was difficult to understand
- donors wanted to have an active role in the decision- making process
Switzer at el. (2016)
Examine the health- related quality of life among sibling pediatric hematopoietic stem cells donors from pre donation through 1 year post donation
- Qualitative Study - Phone Interviews conducted
- The Pediatric Quality of Life Inventory (PedsQL) 4.0 Generic Core Scale was used to assess quality of life
- Demographic data of the parents and the donor are included
- 94 first time donors and 1 parent of the sibling donor across 24 transplant centers
participated in the study. The donors ages varied from 5 to 18 years old
- parents ranked the donor’s quality of life higher than the children scored themselves - approximately 20% of patients were scored at or below the Pediatric Quality of Life cut-off score meaning that they have a health-related quality of life similar to a chronically ill child - children aged 5-7 were most likely to be at risk for poor health related quality of life - donor children had poorer quality of life at pre and shortly after post donation but return to normal levels by 1 year post donation
- pediatric care team must provide patients with a comprehensive approach to the support services available for sibling donors
- consistent follow-up with the donor is needed - the health care team needs to provide the pediatric donor with age-appropriate information during each phase of the donation process
Weaver et al. (2015)
Understanding the health needs and developmental challenges surrounding transplant - Integrative Review - adolescent aged siblings
- positive effects of donation include: better family
relationships, increased feelings about self, decreased
helplessness, and insight into their sibling’s illness
- Providing the donor with a psychosocial clinician to identify health related quality of life
14
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS donation in
adolescent siblings - death of a recipient leads to guilt and are less likely to experience positive
psychological effects
- sibling donors perceive that they have no choice in being a donor
- adolescents have a risk of unresolved developmental crisis
adequate psychosocial support throughout the donation process - educate parents about the importance of support for the donor child
- allow the donor the opportunity to speak about their experience Packman et
al. (2010) Review the psychosocial and cognitive effects on patients, as well as the psychosocial effects on siblings and parents
-Literature Review - 10 studies analyzed for the psychosocial reactions of siblings to HSCT
- Donors across all studies were 2.5 to 22 years old at the time of donation
- Sibling donors are at risk for developing post-traumatic stress disorder, anxiety, and overall low self-esteem
- new behavior problems occurred more often in siblings who donated compared to non-donors
- donors reported loneliness, limited comprehension of the transplant process, and lack of attention from parents
- donors reported having good and bad days that mirrored their ill sibling
- After transplant there was an interruption in the family dynamics
- maturation of the child must be considered as part of the psychosocial donor assessment and care
- health care givers must optimize the welfare of the donor by minimizing harm, eliciting, and respecting the donor’s feelings and choice - language of the provider is important, focusing on depersonalization of the donated cells and non-coercive nature of the conversations
Pentz et al. (2014)
Collect the family members views on choice, concerns, regrets, and benefits of sibling HLA typing and
-Prospective Qualitative Study - Interviews were conducted
- Donor decision was assessed with
-33 families total, 119 individuals, sibling donors were between 9-18 years old
- 68 individuals across 29 families reported that the
siblings have no choice in being HLA typed.
- Post transplant, 5 families reported the procedure that they
- implement familial interventions to enhance protective factors and improve communication are needed
stem cell donation. the Satisfaction with Decision Scale and the Decision Regret Scale.
were not upset or regretful - Post transplant, 4 donors wished that they had been better informed about the HSC process - 59 individuals from 23
families perceived that there was no choice regarding donation for the matched sibling
- The perception of having no choice for the donating sibling was universal seen across 14 families
- all family members of the 2 families headed by a
grandparent stated that the siblings had choice
- group interventions such as discussion, art-therapy, role playing, and social information sessions could improve
psychological well-being of the sibling donors
White et al. (2017)
Describe the strategies families report using to address the needs and concerns of siblings of children, adolescents, and young adults undergoing hematopoietic stem cell
transplant as well as explain sibling issues during HSCT
- Secondary Analysis of 86 Qualitative interviews - Prospective interviews were conducted after secondary analysis -Children, adolescents, and young adults undergoing HSCT at 4 HSCT Centers. – there were 11 donors aged 9-22 years old
- 3 (27%) donor siblings
experienced emotional difficulty - 4 (36%) felt negative effects of separation from the patient and caregiver
- 2 (18%) felt as though they had additional responsibilities or burdens to face
- 3 (27%) lacked information about the recipients’ medical condition and process
- 1 (9%) of donors felt as though they were excluded through the family battle with cancer
- lack of information was reported more frequently by
- screening before HLA typing should only be initiated if there are concerns for the family circumstances
- more complete and direct information and education about the donation process - systematic post-transplant donor
16
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
siblings (23%) than parents (4%)
Results of Thematic Analysis
Analysis of the data set revealed four common themes that captured the experience of sibling bone marrow transplant donors: (a) psychological/ psychosocial impacts, (b) physical impacts, (c) lack of knowledge, and (d) not having a choice. These themes were highly present across the data set and are important for nurses to consider when understanding the experience of sibling bone marrow transplant donors.
Impacts on Psychological and Psychosocial Well-being
Psychological impacts refer to the mental and emotional state of a person whereas psychosocial impacts pertain to the social factors affecting an individual’s mind or behavior (Psychology, n.d; Psychosocial, n.d). Participating as a bone marrow transplant sibling donor appears to be associated with both negative and positive psychosocial and psychological
implications—a finding reported in nine of the articles within the data set. Negative implications of bone marrow transplant were seen more commonly than positive impacts.
18
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
pertained to the sick child (Bauk et al., 2013, Bendorf and Kerridge, 2011; Pentz et al., 2014; White et al., 2017). Furthermore, serious psychological reactions in sibling donors were noted by some authors. For instance, Packman et al. (2010) noted that sibling donors are at higher risk of developing post-traumatic stress disorder, anxiety, and behavioral problems. Erden et al. (2019) reported that sibling donor subjects had higher depressive symptom levels than that of the recipient and non-donor siblings, and higher anxiety scores were prevalent when compared to non-donor siblings.
Switzer et al. (2016) evaluated sibling donors’ health-related quality of life through physical function as well as psychological health. Psychosocial health was evaluated based on emotional, social, and school functioning (Switzer et al., 2016). These authors found that 20% of sibling donors’ health-related quality of life scores were similar to that of critically ill children, and younger sibling donors, under the age of 8, had the lowest quality of life scores (Switzer et al., 2016). This finding differs when compared to D'Auria et al. (2015), Erden et al. (2019), Weaver et al. (2015), and Bauk et al. (2013) who reported that adolescents will face more
psychosocial distress due to the vulnerable emotional and social life transition that this age group is progressing through.
bond between the recipient and the sibling donor (Bauk et al., 2013; D’Auria et al., 2015; Pentz et al., 2014; Weaver et al., 2015). Not only was the relationship between the ill child and the donor reported to be stronger, but the family’s interpersonal relationship improved as successful bone marrow transplants allowed for the family’s life to return to normal (Bauk et al., 2013; Bendorf and Kerridge, 2011; Packman et al., 2010; Pentz et al., 2014). Lastly, sibling donors were found to have better performance in school due to stronger behavioral adaptive skills, which was believed to have stemmed from the socially and cognitively challenging bone marrow transplant experience (Bauk et al., 2013; Packman et al., 2010).
Physical Implications
Physical impacts of bone marrow donation are the side effects that donors experienced during and after the donation process. The majority of the articles, eight total, referenced side effects and physical complications as a part of sibling donors’ experience. The most common side effect of undergoing bone marrow donation was pain. Styczynski et al. (2012) found that 50.2% of donors had pain requiring non- opioid analgesics. Donors reported skeletal pain in their back and hips as well as stiffness at the collection site (Pulipher; Styczynski et al., 2012). Pain persisted for a median of 1 day but there were instances where it lasted up to 14 days after the donation procedure (Styczynski et al., 2012). Pain was noted as a concern for both the parents and the donors, but after undergoing the procedure, the donor did not regret their choice because the pain was minimal compared to what the recipient was enduring (Bauk et al., 2013; D’Auria et al., 2015; Pentz et al., 2014).
Both Styczynski et al. (2012) and Pulsipher et al. (2019) found that older donors,
20
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
a 5-fold higher risk of experiencing pain than donors under the age of 4 (Styczynski et al., 2012; Pulsipher et al., 2019). 22% of males and 23% of females aged 13 to 17 years reported minor discomfort and/or persistent symptoms one year post-donation (Pulsipher et al., 2019).
Adolescent females donors were more susceptible to pain in comparison to any other age or sex group, reporting a 2-fold greater rate of pain than adolescent males (Pulsipher et al., 2019).
In contrast, Styczynski et al. (2012) and Weaver et al. (2015) found that children under 4 years of age, or under 20kg, are the highest risk group for complications of bone marrow
donation. These complications include severe anemia and the need for a blood transfusion or complications related to the anesthesia (Pulsipher et al., 2019; Styczynski et al., 2012). The negative implications that younger donors face may be due to their smaller size and immature bodies. However, serious complications are rarely seen with bone marrow harvesting. Pulsipher et al. (2019) found only 2 out of 294 patients suffered from severe adverse events (SAE) while no pediatric donors in Styczynski et al. (2012) population of 313 experienced SAEs.
Lack of Knowledge
A less prevalent theme noted across the data set is the donors’ knowledge gap
surrounding bone marrow transplant. Six of the articles in the data set found that sibling bone marrow donors are at risk for receiving inadequate information surrounding the condition of their ill siblings as well as the bone marrow transplant procedure. For example, White et al. (2017) reported that 23% of donors did not believe that they received adequate knowledge of the
that this knowledge gap lead to increased anxiety commonly seen in bone marrow donors. D'Auria et al. (2015) also noted that the children she interviewed were not properly educated on the transplantation process, including recovery, as they thought the donated bone marrow would work immediately to save their brother or sister’s life. Pentz et al. (2014) found that four donors and one mother wished that they had been better informed about side effects, medication, and the hospital process for donation. Similar to Pentz et al. (2014), Weaver et al. (2015), and Packman both observed that siblings wanted to know more information about the procedure that they were undergoing and what their part in the treatment of their ill sibling was.
Not having a Choice
The last theme revealed through analysis of the data set was a sentiment of not having a choice. One of the major ethical considerations surrounding sibling bone marrow donors is that they often are not the ones to make the decision and feel that they have no choice in the matter. This lack of autonomy was evident as a key aspect of the donors’ experience in the majority of the data set, with six of the eleven articles referencing this issue. Pentz et al. (2014) found that 77% of individuals across 23 families perceived that there was no choice in the decision to become a bone marrow transplant donor for their sibling. Donors also felt as though the doctors and the family members were limiting their opportunity to say no (Weaver et al., 2015).
22
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
Weaver et al., 2015). Regardless of the donors’ perceptions, Bauk et al. (2013) found that sibling donors did want to be part of the decision-making process and desired control over their choices.
Discussion
An analysis of the literature revealed that pediatric sibling bone marrow transplant donors exhibited common patterns in their experiences. It is important for nurses to recognize the sibling’s experience, which include their struggles and concerns, so they can provide better holistic care. Focusing on the sibling donor and their well-being will help to create a more positive donation experience.
Sibling bone marrow transplant donors experience unique circumstances as they have to deal with the psychological and psychosocial impact of both the procedure itself as well as having a sibling with a chronic illness (White et al., 2017). Since the bone marrow transplant typically occurs at a critical point of their sibling’s illness, the focus of the parents is centered around the critically ill child rather than the donor. This review brings to light that seclusion of the sibling donor negatively impacts the their well-being as they are isolated and
underappreciated in their donation journey (Bauk et al., 2013; Bendorf and Kerridge, 2011; Pentz et al., 2014; White et al., 2017). Nurses should work with the donor siblings to ensure they are feeling included and supported through the donation process as well as encourage family members to spend time with both patients.
because the sibling donor is viewed as the one who sacrificed a piece of themselves to save their sibling’s life. It is important that nurses recognize this trend so that they can anticipate the emotional reactions that will occur in response to compromised or failed bone marrow transplant. If nurses are more knowledgeable about these trends, they can recognize signs and symptoms of psychological distress in the donor, such as anxiety or depression, and intervene more quickly.
It is evident throughout the data set that pain is the most common side effect of bone marrow donation and typically requires the use of analgesics (Styczynski et al., 2012; Weaver et al., 2015; Pulsipher et al., 2019). A key aspect of this physiological impact is that pain affects age groups differently as the rate, intensity, and duration increases with the age of the sibling donor (Pulsipher et al., 2019; Styczynski et al., 2012). Not only are adolescents more at risk for experiencing negative psychosocial effects of bone marrow donation as they navigate through a critical developmental period, but they are also at risk of incurring disabling pain levels and an inability to recover fully up to a year after the donation process (Pulsipher et al., 2019, D’Auria et al., 2015; Erden et al., 2019; Styczynski et al., 2012; Weaver et al., 2015). Nurses need to recognize pain as a major factor in the donor siblings’ experience so they can advocate for and provide adequate relief for quicker recovery. Also, it is essential that nurses understand the vulnerable developmental time that adolescent donors are faced with while undergoing the donation process. Knowing and expecting that adolescents are more likely to experience the negative psychological impacts with donation as well as more intense pain, nurses can advocate for the use of a psychiatric therapist or child life specialists and start them on higher level analgesics to decrease their pain.
24
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
siblings condition (Bauk et al., 2013; D’Auria et al., 2015; Pentz et al., 2014; White et al., 2017). Providing inefficient education to the sibling donors can be catastrophic to their experience. Lack of knowledge surrounding the bone harvesting process can cause anxiety and fear to build in the patient prior to transplant. Isolation during their hospitalization could also be amplified if they aren’t receiving information about their procedure or the status of their ill sibling. Additionally, lack of knowledge on how the transplant works, specifically what the donors bone marrow cells will be used for and how the recipients body could react to those cells, may be the reason as for why the donors accept so much responsibility over the success or failure of transplant. If the donor lacks education on and understanding of the possible outcomes of bone marrow transplant, negative psychosocial and psychological emotions could arise.
Nurses should provide proper education by explaining the full magnitude of the disease state that their sibling is in, informing them that bone marrow transplant is usually performed as a last effort treatment when prognosis is not favorable or when other treatments have failed. Also, nurses should include the possible outcomes of the treatment and adverse effects that could occur. These should be emphasized as effects that the donor is unable to control, so they don’t internalize bone marrow transplant failure as their fault. Parents should be provided with educational materials to encourage parental sharing of information and enhance family
communication as well as inclusion. All educational resources used should be tailored to the age and developmental stage of the donor so they can easily understand the information.
Technically, this decision should only be made in the best interest of the donor child. However, it is difficult for parents to fairly weigh the interests of the donors when the ill recipient is also their child. Parents are typically unable to separate their own interests and the interest of other family members when making this decision and, therefore, feel as though they have no choice but to proceed with the bone marrow transplant (Bendorf and Kerridge, 2011). Because of this, many of the donors feel that they have no choice in whether or not they want to be a donor for their sick sibling (Bauk et al., 2013; Pentz et al., 2014; Weaver et al., 2015). The data set revealed that there are two different ways that the donors perceive not having a choice.
Some donors perceived that they were unable to exercise their free will because they did not receive a choice in whether or not they wanted to donate their bone marrow. This lack of autonomy stems from being left out of the decision making process, being influenced by family members and the healthcare team into agreeing, as well as not be asked to providing consent or assent if appropriate for that age group (Bauk et al., 2013; Packman et al., 2010; Pentz et al., 2014; Weaver et al., 2015). The other perception of not having a choice in their decision to become a donor was that children felt there was no decision to be made; that saying no was not an option because they had a moral obligation to save their siblings life (D’Auria et al., 2015; Pentz et al., 2014; Weaver et al., 2015). The differing responses of donors who felt they did not have a choice in their decision suggests that this procedure is both ethically and morally
challenging for sibling donors. Nurses should recognize that pediatric sibling donors are a vulnerable population who are at risk for persuasion and may lack autonomy over their body, and therefore should create environments where the child’s opinion may be heard and valued.
26
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
Pediatric bone marrow donation is an ethically, legally, and clinically challenging process that is amplified when the recipient and the donor are related (Bauk et al., 2013). The way that nurses approach this delicate situation and how they care for the sibling donor can help to decrease the negative aspects of the donation experience. In order to prevent negative
implications of bone marrow donation, nurses should advocate for physiologic and psychosocial assessments of child donors to ensure that they are mentally and physically fit for donation. This includes observing family circumstances and ensuring that there is an emotionally strong donor-recipient relationship before the transplant is attempted (Pentz et al., 2014). Nurses should be aware of and constantly monitor the psychosocial and psychological status of the donor before, during, and after transplantation as well as the donor’s developmental state and how that could influence their mental well-being (Bauk et al., 2013; D’Auria et al., 2015; Packman et al., 2010; Weaver et al., 2015; White et al., 2017). Nurses should advocate for long-term psychosocial and emotional support for each donor to address complications that may have arisen from bone marrow donation, especially for donors of failed bone marrow transplants.
(Wiener et al. 2019). Education should also be provided to family and communication between parents and the donor should be encouraged (Pentz et al., 2014).
Lastly, to address the ethical issues surround sibling bone marrow donation, sibling donors should be cared for by an independent medical team separate from the one caring for the recipient (Bendorf and Kerridge, 2011; Erden et al., 2019; Styczynski et al., 2012). This creates a safe environment where the donor is the center of focus. Here, the child’s opinion regarding donation can be heard separately from the recipient’s needs. The nurse should be an advocate for the donor and ensure that their concerns, desires, and needs are being recognized and voiced.
Limitations and Recommendations for Future Research
Although a thorough review of the literature was conducted to create the data set, not all search engines were utilized. Also, different search terms could have resulted in additional research that may have presented new information. This data set did not contain any systematic reviews, which is considered the highest quality of evidence.
28
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
The research suggest that long-term support should be provided for sibling donors, but the type and timing of these interventions need further study.
Conclusion
This literature review aimed to understand the experiences of pediatric sibling bone marrow transplant donors. The data set revealed that donors’ experiences have psychosocial, psychological, and physical implications, and are also marked by a lack of knowledge
References
Committee on Bioethics (2010). Policy Statement- Children as hematopoietic stem cell donors. Pediatrics,125(2), 392–404.
Bauk, K., D’Auria, J.P., Andrews, A. and Presler, C.M. (2013). The pediatric sibling donor experience in hematopoietic stem cell transplant: an integrative review of the literature.
Journal of Pediatric Nursing,28(3), 235–242.
Bendorf, A., & Kerridge, I. H. (2011). Ethical issues in bone marrow transplantation in children. Journal of Paediatrics and Child Health, 47(9), 614–619.
https://doi.org/10.1111/j.1440-1754.2011.02165.x
Bollard, C. M., Krance, R. A., & Heslop, H. E. (2011). Hematopoietic stem cell transplantation in pediatric oncology. In P. A. Pizzo, & D. G. Poplack (Eds.), Principles and practice of
pediatric oncology (pp. 467 – 469) (6th ed.). Philadelphia, PA: Lippincott Williams &
Wilkins.
D’Auria, J.P., Fitzgerald, T.M., Presler, C.M. and Kasow, K.A. 2015. Through the eyes of young sibling donors: the hematopoietic stem cell donation experience. Journal of
Pediatric Nursing,30(3), 447–453.
Erden, S., Kuşkonmaz, B.B., Çetinkaya, D.U., Ünal, F. and Özsungur, B. 2019. Pediatric bone marrow transplantation: psychopathologic features in recipients along with siblings.
Psycho-Oncology,28(10), 1995–2001.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & The PRISMA Group (2009). Preferred reporting items for systematic reviews and meta analyses: The PRISMA statement. ‐
PLOS Medicine, 6(7), e1000097. https://doi.org/10.1371/journal.pmed1000097
30
THE EXPERIENCE OF PEDIATRIC SIBLING BONE MARROW DONORS
hematopoietic SCT on pediatric patients, siblings and parents: a review. Bone Marrow
Transplantation,45(7), 1134–1146.
Pentz, R. D., Alderfer, M. A., Pelletier, W., Stegenga, K., Haight, A. E., Hendershot, K. A., … Hinds, P. (2014). Unmet needs of siblings of pediatric stem cell transplant
recipients. Pediatrics, 133(5), e1156-62. https://doi.org/10.1542/peds.2013-3067 Psychology. (n.d) In Oxford Online Dctionary. Retrieved from
https://www.lexico.com/en/definition/psychology
Psychosocial. (n.d) In Oxford Online Dctionary. Retrieved from https://www.lexico.com/en/definition/psychosocial
Pulsipher, M. A., Logan, B. R., Kiefer, D. M., Chitphakdithai, P., Riches, M. L., Rizzo, J. D., … Switzer, G. E. (2019). Higher risks of toxicity and incomplete recovery in 13- to 17-year-old females after marrow donation: RDSafe peds results. Biology of Blood and Marrow
Transplantation, 25(5), 955–964. https://doi.org/10.1016/j.bbmt.2018.12.765
Styczynski, J., Balduzzi, A., Gil, L., et al. 2012. Risk of complications during hematopoietic stem cell collection in pediatric sibling donors: a prospective european group for blood and marrow transplantation pediatric diseases working party study. Blood,119(12), 2935–2942.
Switzer, G. E., Bruce, J., Kiefer, D. M., Kobusingye, H., Drexler, R., Besser, R. M., … Pulsipher, M. A. (2016). Health-related quality of life among pediatric hematopoietic stem cell donors. The Journal of Pediatrics, 178, 164-170.e1.
https://doi.org/10.1016/j.jpeds.2016.07.009
Vogel, R.J. 2011. The management of the sibling hematopoietic stem cell donor. Journal of
Weaver, M. S., Diekema, D. S., Carr, A., & Triplett, B. (2015). Matched marrow, sibling
shadow: the epidemiology, experience, and ethics of sibling donors of stem cells. Journal
of Adolescent and Young Adult Oncology, 4(3), 100–104.
https://doi.org/10.1089/jayao.2014.0051
White, T. E., Hendershot, K. A., Dixon, M. D., Pelletier, W., Haight, A., Stegenga, K., … Pentz, R. D. (2017). Family strategies to support siblings of pediatric hematopoietic stem cell transplant patients. Pediatrics, 139(2). https://doi.org/10.1542/peds.2016-1057
Whittemore, R., & Knafl, K. (2005). The integrative review: Updated methodology. Journal of
Advanced Nursing, 52(5), 546–553. https://doi. org/10.1111/j.1365 2648.2005.03621.x‐
Wiener, L., Hoag, J. A., Pelletier, W., Shah, N. N., Shaw, B. E., Pulsipher, M. A., … Switzer, G. E. (2019). Transplant center practices for psychosocial assessment and management of pediatric hematopoietic stem cell donors. Bone Marrow Transplantation.