University of Kentucky University of Kentucky
UKnowledge
UKnowledge
Theses and Dissertations--Public Health (M.P.H.& Dr.P.H.) College of Public Health
2016
Evaluations of Patients’ Appointment Duration by Type in an
Evaluations of Patients’ Appointment Duration by Type in an
Ophthalmology Practice
Ophthalmology Practice
Brittany U'WrenUniversity of Kentucky, [email protected]
Follow this and additional works at: https://uknowledge.uky.edu/cph_etds
Part of the Public Health Commons
Right click to open a feedback form in a new tab to let us know how this document benefits you. Right click to open a feedback form in a new tab to let us know how this document benefits you.
Recommended Citation Recommended Citation
U'Wren, Brittany, "Evaluations of Patients’ Appointment Duration by Type in an Ophthalmology Practice" (2016). Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.). 135.
https://uknowledge.uky.edu/cph_etds/135
This Graduate Capstone Project is brought to you for free and open access by the College of Public Health at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Public Health (M.P.H. & Dr.P.H.) by an
STUDENT AGREEMENT: STUDENT AGREEMENT:
I represent that my capstone and abstract are my original work. Proper attribution has been given to all outside sources. I understand that I am solely responsible for obtaining any needed copyright permissions. I have obtained needed written permission statement(s) from the owner(s) of each third-party copyrighted matter to be included in my work, allowing electronic distribution (if such use is not permitted by the fair use doctrine) which will be submitted to UKnowledge as Additional File.
I hereby grant to The University of Kentucky and its agents the irrevocable, non-exclusive, and royalty-free license to archive and make accessible my work in whole or in part in all forms of media, now or hereafter known. I agree that the document mentioned above may be made available immediately for worldwide access unless an embargo applies.
I retain all other ownership rights to the copyright of my work. I also retain the right to use in future works (such as articles or books) all or part of my work. I understand that I am free to register the copyright to my work.
REVIEW, APPROVAL AND ACCEPTANCE REVIEW, APPROVAL AND ACCEPTANCE
The document mentioned above has been reviewed and accepted by the student’s advisor, on behalf of the advisory committee, and by the Director of Graduate Studies (DGS), on behalf of the program; we verify that this is the final, approved version of the student’s capstone including all changes required by the advisory committee. The undersigned agree to abide by the
statements above.
Brittany U'Wren, Student Sarah Wackerbarth, PhD, Committee Chair Corrine Williams, ScD, MS, Director of Graduate Studies
Evaluations of Patients’ Appointment Duration
by Type in an Ophthalmology Practice
CAPSTONE PROJECT PAPER
A paper submitted in partial fulfillment of the Requirements for the
degree of Master of Public Health in the University of Kentucky
College of Public Health
By
Brittany Flowers U’Wren
Albany, KY
Lexington, Kentucky
November 29, 2016
Capstone Committee Sarah Wackerbarth, PhD (Chair)
Richard C. Ingram, DrPH (Committee Member) Martha C. Riddell, DrPH (Committee Member)
Table of Contents
Abstract ... 3 Introduction ... 4 Methods ... 6 Results ... 7 Discussion ... 13 Limitations ... 14Abstract
Objective: The Affordable Care Act expanded health care coverage and provided more access to physicians, resulting in potentially longer wait times. Large portions of ophthalmology patients are on Medicare. Two thirds of the expansion populations were Hispanic or African Americans, which have higher rates of eye disease. Another contributoring factor leading to the increase for eye care is the surge of baby boomers. More specifically, these are individuals reaching sixty-five and are beginning to utilize Medicare. Access to care has increased but the capacity of the practice has not. An important goal, therefore, is to maximize efficiency of current resources.
Methods: Empirical research to analyze existing data of arrival time, service time, patient types and the flow of patients between June 1 – August 31, 2016. The data was collected using a practice management system, “Nextech.”
Results: A total of 823 patient appointments were evaluated. The weighted average of appointments was 77 minutes. Four patient types exceeded that amount. According to data recorded, appointment slots should be reevaluated to account for the longer average. Conclusions: Every health care organization should know how to choose the most
appropriate method of appointment scheduling based on patient needs. Examination of patient scheduling is an important tool for efficient outpatient department management.
Introduction
The Affordable Care Act (ACA) has influenced the health care landscape in many ways; this includes greater coverage, higher cost sharing, narrow networks, value-based
purchasing and new payment models. Expanded coverage brought millions of previously uninsured people insurance in 2014 through Medicaid or through subsidies in the new health insurance exchanges. Not only have these new patients potentially delayed treatment, but as a group they are also inherently more likely to have eye disease than others their age. Two thirds of the expansion groups were Hispanic or African American, and studies have shown that Hispanics have higher rates of diabetic retinopathy and other eye diseases1 while the African American population has a higher incidence of
glaucoma2. There is also a continued surge in older patients who will be seeking eye care
under Medicare, as millions of baby boomers reach the age of 65. Another part of ACA, requires all insurance plans to reimburse individuals or small groups for comprehensive eye exams for children. In recent years, the public and healthcare administrators have placed a strong emphasis on quality of care.
Overcrowding of health care facilities and inefficient patient flow affect quality of care, timeliness of care and patient satisfaction. Patient satisfaction scores may be considered as a measure of care quality. The patients’ perception of how long they waited has been associated with satisfaction scores. To improve patient appointment time, the goal is to figure out the number of patients per day based on appointment type. In a typical
degree. The amount of daily clinic hours per physician is a fixed asset which is portioned out by patient demand or volume. On average, the more time a specific physician spends with an individual patient, the longer the patients have to wait to see that physician.
Ophthalmology is provided primarily as an outpatient service. The patient population is largely healthy but elderly. This study was based on an ophthalmology practice that is located in central Kentucky. The practice consisted of one physician and 5 staff members. The practice provided outpatient, surgical and tertiary services for eye disease and its related structures. The eye center was a well-established full-service eye care practice. This practice offers a full range of services; Couple examples involve comprehensive eye exams for the entire family and comprehensive eye surgery, including cataract surgery with multifocal and toric intraocular lens implants. Other surgical services performed were cosmetic eyelid surgery and glaucoma surgery.
Long waiting time is common across healthcare providers and is a main contributor to patient dissatisfastion.4 This study used survey research to examine the impact of changing clinic scheduling on patient satisfaction.4 Through modifications in clinical
processes, as well as education lectures for the staff to enhance patients’ services, the waiting time was reduced from 92 ± 10 minutes to 42 ± 5 minutes with significant improvement in patients' satisfaction with minimal costs.4
Studies show a positive correlation between the patient experiences and desirable clinical outcomes 3,4 and conversely, an association between low patient satisfaction scores and
thoroughness and provider time were the three most important attributes patients associate with provider quality of care. Thoroughness, listening, punctuality and clear instruction were the key drivers that moved patients’ overall perceptions of provider quality of care from “very good” to excellent.” 6
In the context of healthcare, patient satisfaction is an individual’s evaluation of his or her experience in receiving health care in a specific setting. Limited cross-sectional studies show a positive relationship between patient satisfaction and adherence to medications (7-11). Likewise, adherence to medications clearly impacts clinical outcomes. (12-13).
Satisfaction also has been associated with patient switching behavior in regards to
provider and insurance plans. (14-15). Future more, studies using national CAHPS Hospital survey data show a significant albeit modest correlation between patient satisfaction and objective clinical performance measures. (16-17)
Methods
The study was conducted at a well-established ophthalmology clinic located in central Kentucky. The clinic had twelve appointment types, described in Table 1. Observation was used to examine patient flow. Descriptive statistics and frequency analysis were used to examine appointment type and duration; this study was based on observational data of patients seen between June 1 and August 31, 2016. The patient service times between the arrival and the departure time were recorded. Each patient was considered marked “in” once they signed in at the reception desk. This information was pulled from Nextech, which is a practice management system that most ophthalmology practices use.
Follow Up One-day & Two week cataract follow up. Eye Exam, New Patient First time visiting our clinic. Scheduled by
the patient.
Eye Exam, Established Patient Patient who has visited the practice in the past three years.
Diagnostic Testing Patients who return for visual fields and optical coherence tomography (OCT) Disability Exam Appointments scheduled by The
Disability Determination Services.
Glaucoma Interim Glaucoma patients are expected to be seen every four, six or 12 month intervals. Diabetic Exam Primary Care Physicians schedule these
appointments. (New patient) Contact Lens Fitting
Glasses Problem The order prescription does not meet their needs effectively.
Glasses Purchase
Eye Exam, Child Includes both new vs. established patients. Typically, school eye exams.
A-Scan A preoperative exam prior to cataract surgery.
Table 1
Results
Patient flow analysis is a simple improvement tool to identify patient flow patterns. This can be very useful in resource-limited settings such as a small private outpatient clinic. Flow mapping provides a qualitative perspective, and cycle time measurement provides quantitative data on time throughout the patient’s visit. Patient flow mapping involves when a patient walks into the office and detailing each particular step throughout the entire visit. Figure 1 shows a good representation of day-to-day routine. Cycle time measurements build on flow mapping and involve the time associated with the patient visit. Total cycle time is defined as the number of minutes between when a patient arrives at the practice and when he or she leaves.
Figure 1
Figure 2 displays the baseline characteristics of the study sample. There were a total of 823 appointments in a three-month period. The majority were Established appointments (61%) & New Patient (19%) exams, followed by diagnostic testing (4%), Children exams
(3%), Follow up (3%), and Glaucoma interim (3%). The remaining types were below 3% of total appointment types.
Figure 2
Figure 3 shows the average appointment duration based on type. Disability exams (112 minutes) consume the most time on average compared to other appointment types. Glasses purchase (13) and Contact fittings take the least amount of time.
Figure 3
AP P OIN T ME N T T Y P E COU N T ME AN ME D IAN MOD E R AN GE
Follow-Up 28 43 41 33 94
Eye Exam, NP 154 90 89 89 154
Eye Exam, Est. 501 75 74 70 187
Diagnostic Testing 29 46 33 89 106
Eye Exam, Disability 19 112 115 N/A 93
Eye Exam, Glaucoma Interim 22 72 66 69 133
Eye Exam, Diabetic 7 93 99 N/A 59
Contact Lens Fitting 19 41 34 16 104
Glasses Problem 15 61 55 33 120
Contact Final Fit 5 48 28 N/A 141
Glasses Purchase 1 13 13 N/A 0
Eye Exam, Child 21 99 105 105 117
A-SCAN 1 72 72 N/A 0
Figure 4
Median and mean duration times were calculated for each appointment type in figure 4. The most standard appointment type is a diabetic exam, which averages at 93 minutes per exam and has the lowest range of varying times. Established exam tend to vary the most with a range of 154 and an average of 90 minutes.
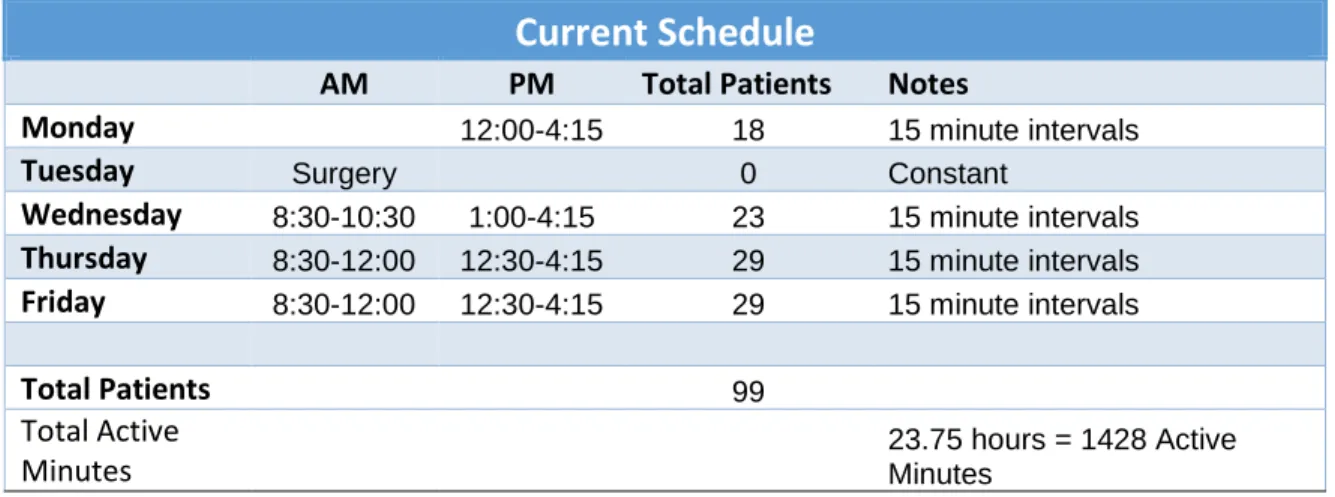
Figure 5 shows a normal workweek schedule. The goal of each week is to schedule between 90-99 patient appointments. There are 1,428 active minutes per week with minutes varying depending on end of day appointments or procedures.
Current Schedule
AM PM Total Patients Notes
Monday 12:00-4:15 18 15 minute intervals
Tuesday Surgery 0 Constant
Wednesday 8:30-10:30 1:00-4:15 23 15 minute intervals
Thursday 8:30-12:00 12:30-4:15 29 15 minute intervals
Friday 8:30-12:00 12:30-4:15 29 15 minute intervals
Total Patients 99 Total Active
Minutes 23.75 hours = 1428 Active Minutes
Figure 5
According to figure 3, the total weighted average per appointment is 77 minutes. New patient, children, disability and diabetic exams tend to exceed the total weighted average. To schedule efficiently, we as a practice should increase the appointment slot for these patients. Instead of 15-minute slots, increase these patients to 30-minute slots each time.
Figure 6
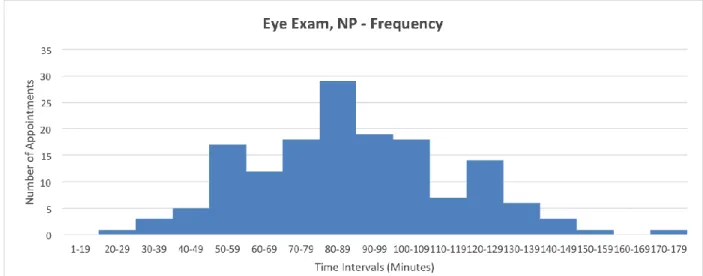
Figure 6-8 are histograms of the grouped frequency distribution show in figure 2. New patient and established exams vary the most among the appointment types. Figure 8 shows the frequency of contact fittings. These appointments are the most constant but also varies the third most behind established and new patient exams.
Figure 8
Discussion
Healthcare facilities face the challenge of providing high-quality care while struggling with large patient volumes and process inefficiencies. Optimizing a patient schedule is trade-off between patient wait, clinical idle time and running over the schedule at the end of the day. We have identified potential problems that can be changed to improve patient appointment time. By minimizing undue waiting and ensuring timely transition among staff, practices can make patients feel well cared for and maximize daily patient load. By studying patient flow, providers are able to increase efficiency and uncover hidden capacity and as a result, improve patients’ overall happiness and health while increasing revenue.
The Affordable Care Act reduced the uninsured rate for low-income groups and people of color. The ACA significantly increased coverage options for low and moderate-income populations. Under the ACA, Medicaid coverage is extended to low-income adults with incomes up to 138% of the federal poverty level in the 32 states that have implemented the Medicaid expansion to date and tax credits are available to middle income individuals who purchased insurance. Since these coverage provisions took effect in 2014, uninsured
rates for the nonelderly population have decreased, falling from 17% in 2013 to 11% in 2015.21 Access to care has increased but the capacity of the practice has not.
Recommendations
Based on the data collected, limiting the number of appointment types can and will benefit the patient duration time. The practice must limit disabilities to two per day, once in the morning and one in the afternoon. Children exams should be conducted in the earliest time slots. New patient exams should not be scheduled consecutively.
Limitations
This study did not address the issue of physician productivity. Human error is another limitation that cannot be explained when marking patients in and out of the clinic.
Citations
1. National Eye Institute. U.S. Latinos have high rates of developing vision loss and certain eye conditions. May 1, 2010. http://www.nei.nih.gov/news/pressreleases/050110.asp Accessed August 3, 2016.
2. The Eye Diseases Prevalence Research Group. Prevalence of open-angle glaucoma among adults in the United States. Arch Ophthalmol.2004;122:532-538.
http://archopht.jamanetwork.com/article.aspx?articleid=416231 Accessed August 3, 2016. 3. Anderson RT, Camacho FT, Balkrishnan R. Willing to wait?: The influence of patient wait time
on satisfaction with primary care. BMC Health Services Research. 2007;7:31. doi:10.1186/1472-6963-7-31.
4. Harnett MJP, Correll DJ, Hurwitz S, Bader AM, Hepner DL.. Improving efficiency and patient satisfaction in a tertiary teaching hospital preoperative clinic. Anesthesiology. 2010;112(1): 66– 72. . 10.1097/ALN.0b013e3181c617cb
5. Burt T. Reinventing the patient experience. Satisfying customers can lead to continuous growth. Healthc exec. 2006;21:8–12.
6. Reeves J, Binder J, Gnida JC. More is not necessarily better. Mark Health Serv 2008;28:24–29. 7. Stelfox HT, Gandhi TK, Orav EJ, Gustafson ML. The relation of patient satisfaction with
complaints against physi- cians and malpractice lawsuits. Am j med. 2005;118: 1126–1133. 8. TrentmanTL,CornidezEG,WilshusenLL,etal.Patientsatisfactionin an academic chronic pain clinic.
Pain Pract. 2012;13(5):372–379.
9. Crow R, Gage H, Hampson S, Hart J, Kimber A (2002) The measurement of satisfaction with healthcare: Implications for practice from a systematic review of the literature. Health Technol Assess 6(32): 1–244 [PubMed]
10. Bartlett EE, Grayson M, Barker R, Levine DM, Golden A, et al. (1984) The effects of physician communications skills on patient satisfaction; recall, and adherence. J Chronic Dis 37(9–10): 755–64 [PubMed]
11. Hazzard A, Hutchinson SJ, Krawiecki N (1990) Factors related to adherence to medication regimens in pediatric seizure patients. J Pediatr Psychol 15(4): 543–55 [PubMed]
12. Roberts KJ (2002) Physician-patient relationships, patient satisfaction, and antiretroviral medication adherence among HIV-infected adults attending a public health clinic. AIDS Patient Care STDS 16(1): 43–50 [PubMed]
13. Schneider J, Kaplan SH, Greenfield S, Li W, Wilson IB (2004) Better physician-patient relationships are associated with higher reported adherence to antiretroviral therapy in patients with HIV infection. J Gen Intern Med 19(11): 1096–103 [PMC free article] [PubMed]
14. Barbosa CD, Balp MM, Kulich K, Germain N, Rofail D (2012) A literature review to explore the link between treatment satisfaction and adherence, compliance, and persistence. Patient Prefer Adherence 6: 39–48 [PMC free article] [PubMed]
adherence on CD4 cell count responses among HIV-infected patients. J Acquir Immune Defic Syndr 35(3): 261–8 [PubMed]
16. Li JZ, Paredes R, Ribaudo HJ, Svarovskaia ES, Kozal MJ, et al. (2012) Relationship between minority nonnucleoside reverse transcriptase inhibitor resistance mutations, adherence, and the risk of virologic failure. AIDS 26(2): 185–92 [PMC free article] [PubMed]
17. Marquis MS, Davies AR, Ware JE (1983) Patient satisfaction and change in medical care provider: A longitudinal study. Med Care 21(8): 821–9 [PubMed]
18. Safran DG, Montgomery JE, Chang H, Murphy J, Rogers WH (2001) Switching doctors: Predictors of voluntary disenrollment from a primary physician’s practice. J Fam Pract 50(2): 130–6 [PubMed]
19. Jha AK, Orav EJ, Zheng J, Epstein AM (2008) Patients’ perception of hospital care in the United States. N Engl J Med 359(18): 1921–31 [PubMed]
20. Boulding W, Glickman SW, Manary MP, Schulman KA, Staelin R (2011) Relationship between patient satisfaction with inpatient care and hospital readmission within 30 days. Am J Manag Care 17(1): 41–8 [PubMed]
21. Robin Cohen, Michael Martinez, and Emily Zammitti, Health Insurance Coverage: Early Release
of Estimates from the National Health Interview Survey, 2015, (Hyattsville, MD: National Center