All authors are associated with Banner Good Samaritan Medical Center, Phoenix, Arizona. Kerry Montefour is the director of the infection control program.
Jeanne Frieden is an infection control practitioner.
Sue Hurst is a critical care clinical nurse specialist in medical-surgical and transplant intensive care units.
Cindy Helmich is the director of nursing for the medical cardiology service and inpatient wound care.
Denielle Headley is the nurse education specialist for the medical-surgical and trans-plant intensive care unit.
Mary Martin is the associate director of the antimicrobial management team. Deborah A. Boyle is the practice outcomes nurse specialist and Magnet coordinator.
A
cinetobacter baumanniiis a troublesome and increasingly problematic healthcareassociated path -ogen, especially in critical care.1-4It may be associated with hospital-acquired infections with consider-able clinical and economic costs. In physiologically compromised patients, morbidity and mortality are common sequelae ofhospital-acquired infections.4-7Hence, multi-ple professional organizations have identified multidrug-resistant
(MDR) pathogens as a critical target that requires intervention (Tables 1 and 2).
Acinetobacter
baumannii
An Emerging
Multidrug-Resistant Pathogen in
Critical Care
Cover
Article
AuthorsKerry Montefour,
RN, BSN, CICJeanne Frieden,
BA, RN, BSN, CICSue Hurst,
RN, MSN, CCRNCindy Helmich,
RN, MBA, CCRNDenielle Headley,
RN, BSNMary Martin,
PharmDDeborah A. Boyle,
RN, MSN, AOCNCorresponding author: Kerry Montefour, RN, BSN, CIC, Banner Good Samaritan Medical Center, 1111 E McDowell Rd, Phoenix, AZ 85006 (e-mail: [email protected]).
To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.
CE
Continuing Education
This article has been designated for CE credit. A closed-book, multiple-choice examination fol-lows this article, which tests your knowledge of the following objectives:
1. Identify factors that contribute to the emergence and significance of Acinetobacter baumanniiin healthcare environments 2. Describe the characteristics of A baumannii
and the associated risk factors for development of A baumannii infections
3. Discuss nursing interventions, infection control measures, and clinical recommendations for prevention and containment of A baumannii
Our experience with managing an outbreak of MDR A baumannii in a medical intensive care unit (ICU) prompted an evidence-based review of the literature, which resulted in few findings. Key elements of outbreak control and nursing care interven-tions associated with this resistant strain had not been identified. In this article, we provide a synthesis of the
moist surfaces.6
A total of 19 strains of A baumanniihave been identified.12 Although inconsequential to hosts with intact immune systems, A bau-mannii infections may be fatal in those with suboptimal immune defenses. The evolution of this infection com-monly occurs in chronically ill patients who have multiple comor-bid conditions, are hospitalized for long periods, have multiple invasive procedures, and are of advanced age. Risk factors encompass those for hospital-acquired MDR infec-tions and ventilator-associated pneumonias (Table 3). The role of A baumanniiin hospital-acquired infections is associated with 3 factors: its diverse reservoir, its association with antimicrobial resistance, and its outbreak potential.
Growth Reservoir
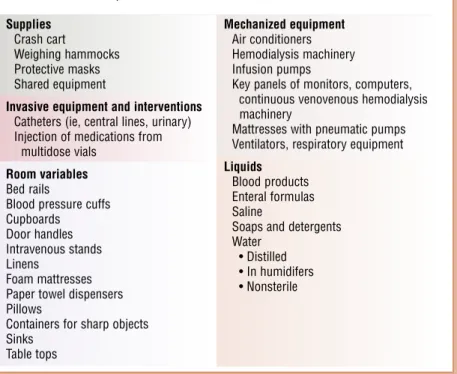
Although risk factors for A bau-manniiinfection have been well described, the reservoirs of this pathogen are poorly understood.6 Acinetobacter baumanniiis nonselec-tive in its habitat (Table 4) and can survive indefinitely. The respiratory tract, blood, pleural fluid, peri-toneum, urinary tract, surgical wounds, central nervous system, skin, and eyes may be sites of infec-tion or colonizainfec-tion.4,6,11
Invasive devices used to facilitate fluid moni-toring, administer medications, and provide lifesaving support may also be sources of colonization. For example, in patients receiving mechanical ventilation, the forma-tion of a biofilm on the surface of the endotracheal tube may be the source of colonization of the lower part of the airway.15
Inert surfaces such as those listed in Table 4 appear to be improbable sources of medical literature on A baumannii, a
chronology of our efforts to control the outbreak, and recommendations for responding to A baumannii infections in ICU settings.
Literature Review
Characteristics of A baumannii and A baumannii Infections
Acinetobacter baumanniiis a non-fermentive, aerobic, opportunistic, gram-negative coccobacillary rod. Morphological findings vary accord-ing to the phase of cell growth and exposure to antimicrobial agents.2,6 Widely distributed in soil and water, A baumanniigrows at various tem-peratures and pH environments and uses a vast variety of substrates for growth.3,11
The indiscriminate nature of this organism and its recent acqui-sition of MDR intensify its emer-gence and significance in healthcare environments.5
Acinetobacter baumanniinormally inhabits skin, mucous membranes, and soil. The organism can survive for long periods on both dry and
Table 1 Actions of professional organizations and recommended interventions for outbreaks of infections caused by multidrug-resistant organisms
Centers for Disease Control and Prevention
• Identified antimicrobial resistance and lack of new drugs coming to market as a major health threat (1997)
• Created a 12-step initiative to increase awareness of resistance and implement strategies to prevent the development of resistance in various populations8 Centers for Disease Control and Prevention and Food and Drug Administration
• Cochaired a 10-agency task force (1999)
• Published A Public Health Action Plan to Combat Antimicrobial Resistance9 Infectious Disease Society of America
• Initiated the program Bad Bugs No Drugs10to enlighten federal policymakers about the inadequacy of the pharmaceutical pipeline in the development of new antimicrobial agents
American Society for Microbiology and the Society for Healthcare Epidemiology of America
• Created the Antimicrobial Resistance Prevention Initiative, a program providing ongoing education exploring epidemiology and molecular mechanisms of resistance Clinical and Laboratory Standards Institute
• Developed standard reference methods for antimicrobial susceptibility tests
Table 2 Centers for Disease Control and Prevention: 12 steps to prevent antimicrobial resistance among hospi-talized adults8
Prevent infection 1. Vaccinate 2. Get catheters out
Diagnose and treat infection effectively 3. Target the pathogen
4. Ask the experts Use antimicrobials wisely
5. Practice antimicrobial control 6. Use local data
7. Treat infection, not contamination 8. Treat infection, not colonization 9. Know when to say no to vancomycin 10. Stop treatment when infection is
cured, unlikely, or undiagnosed Prevent transmission
11. Isolate the pathogen 12. Break the chain of contagion
A baumannii, but culturing of speci-mens obtained from these areas has indicated the prominence of the sur-faces in the evolution of A bauman-nii.18Of note, increased incidence of MDR A baumanniiin military per-sonnel injured in Iraq, Kuwait, and Afghanistan has been reported.19 The majority of the injured had had traumatic injuries in the field. Infec-tion with A baumanniiwas diag-nosed after the personnel were transferred to major military hospi-tals in Western Europe.
Despite the diversity of host sites of A baumannii, inadequate hand hygiene remains a significant factor in the transmission of this pathogen.18 Cross-transmission of MDR A bau-manniioccurs via direct contact from hands (especially in persons with damaged skin from chronic der-matitis) and gloves from healthcare professionals to patients.3,4,6,12,18 Colonization on the skin and con-tamination on glove surfaces may be direct or indirect as the healthcare provider touches the patient and/or
numerous surfaces in providing care.8,10,20-29
Acinetobacter baumannii organisms are readily removed by most hand cleansing agents and by the environmental cleaning done in hospital settings.15,21,22
An Outbreak of MDR
A baumannii
In mid-December of 2005, the microbiology specialist at Banner Good Samaritan Medical Center, Phoenix, Arizona, reported that 5 extremely resistant isolates of A bau-manniihad been cultured during a 2-week period. This number was a dramatic increase. In the previous 6 months, resistant A baumanniihad been isolated from only 11 speci-mens. All of the December isolates were from 5 patients in medical ICUs, and all 5 patients were receiv-ing mechanical ventilation.
Development of Antimicrobial Resistance
Antimicrobial resistance has become a national problem.24-26
An organism is considered resistant when its growth in vitro is not inhib-ited by an antimicrobial agent that has been associated with eradication of the organism in vivo. Causes of resistance vary but are often linked to inappropriate initial antimicrobial therapy,16
including administration of subtherapeutic doses of antimi-crobial agents, drug overuse, abbre-viated or interrupted courses of treatment, and poor tissue penetra-tion by the antimicrobial agent.9,25,28 In A baumannii, antimicrobial resistance probably originated from resistance genes that are transferred between bacterial species.5,30-33
These genes are acquired rapidly and contribute to the development of
Table 3 Risk factors for acquiring Acinetobacter baumannii4-6,13-16 Advanced age
Antimicrobial therapy within past 90 days Use of artificial devices
• Dialysis (chronic) within past 30 days • Mechanical ventilation • Sutures • Catheters •Central venous •Intravenous •Urinary
Evidence of high-frequency antibiotic resistance in the community or hospital Severe immunocompromise due to disease or therapy
Multiple comorbid conditions
Prolonged hospitalization (especially critical care) or residence in an extended care facility
Table 4 Potential hospital environmental sources of Acinetobacter baumaniii 3,4,6,12,17,18
Supplies Crash cart
Weighing hammocks Protective masks Shared equipment
Invasive equipment and interventions Catheters (ie, central lines, urinary) Injection of medications from
multidose vials Room variables Bed rails
Blood pressure cuffs Cupboards Door handles Intravenous stands Linens
Foam mattresses Paper towel dispensers Pillows
Containers for sharp objects Sinks Table tops Mechanized equipment Air conditioners Hemodialysis machinery Infusion pumps
Key panels of monitors, computers, continuous venovenous hemodialysis machinery
Mattresses with pneumatic pumps Ventilators, respiratory equipment Liquids
Blood products Enteral formulas Saline
Soaps and detergents Water
• Distilled • In humidifers • Nonsterile
antimicrobial resistance.5
Some of the genes are inherited, some emerge from random DNA mutations in bacteria, and others are imported from related bacteria33
(Figure 1). Evidence of A baumannii antimicro-bial resistance may be a harbinger, or indication, of transmission of the organism among patients and may be predictive of an impending out-break of A baumanniiinfections.4
Outbreak Potential
The evolution of A baumannii infections and their associated rela-tionship with outbreaks correlate with the virulence of the strain. Inher-ent, unknown mechanisms appear to impede desiccation of this pathogen. Resistant A baumanniioften become apparent as a cluster of infections caused by the bacterium.4
Cases are often aggregated by time and place within settings. An outbreak may
and air conditioner parts despite fil-ters placed at air inlets and outlets. Because of the scope of technological equipment within critical care, this potential source of A baumannii should receive further investigation. Antimicrobial Management
Historically, carbapenems have resulted in the best therapeutic response in infections caused by MDR A baumannii.5,25,36Currently, carbapenems, such as imipenem and meropenem, remain the widely recognized drug of choice for A bau-manniiinfections.5,13,25,38Never theless, susceptibility testing is still required when this pathogen is identified.
During the time of our outbreak, testing resulted in an unprece-dented 38% resistance rate to imipenem (Table 5). Resistance to meropenem for the MDR isolates was close to 100%.
Tests for susceptibility to colistin and tigecycline were also performed. For carbapenem-resistant A bau-mannii, tigecycline and colistimeth -ate are 2 of the most frequently used alternative agents. The Clinical and Laboratory Standards Institute did originate from a single source with widespread environmental contamination or where no reservoir for the contamination can be veri-fied.4,33-37 Most MDR A baumannii outbreaks occur in critical care settings and involve resist-ance to multiple classes of antimicrobial agents.4,18 Poten-tial sources of A baumanniiin the ICU have received close scrutiny. Dust has been identified as a potential vehi-cle. In one investigation,17the out-break strain of A baumannii was recovered from dust within pneu-matic and electronic equipment, in air filters of continuous veno-veno hemodialysis machinery, ventilators,
Figure 1 Bacterial acquisition of resistance genes. Bacteria gain resistance genes by 3 major methods: (a) donor cells transmit whole plasmids containing one or more genes into bacteria, (b) a virus acquires a resistance gene from a bacterium and injects it into a different bacterial cell, and (c) bacteria assimilate gene-bearing components of DNA within their immediate vicinity. Reprinted from Levy,8with permission from Tomo Narashima/Tane+1.LLC.
Resistance gene Plasmid donor Resistance gene Dead bacterium Resistance gene Bacterium infected by a virus Transfer of free DNA Transfer by viral delivery Bacterium receiving resistance genes Plasmid Plasmid transfer a c b
Table 5 Susceptibility of Acinetobacter baumannii isolates to antimicrobials at Banner Good Samaritan Medical Center and in the United States, January 2005-April 2006
Antimicrobial Amikacin Ampicillin/sulbactam Aztreonam Cefepime Ceftazidime Ciprofloxacin Gentamicin Imipenem Levofloxacin Piperacillin/tazobactam Trimethoprim/ sulfamethoxazole Tobramycin
Medical center (18 isolates) 25.5 47.8 0.0 16.3 16.8 15.2 19.6 62.0 16.8 20.2 16.4 23.9 National39(>8000 isolates) 80.4 67.1 6.2 41.8 39.6 42.0 52.3 72.1 Not available 47.0 52.7 70.1 Susceptibility of isolates, %
not well established. Colistin is poorly removed by hemodialysis. Patients with renal impairment require monitoring of renal function, and dose and interval adjustments of the drug are recommended. No commercial method for monitoring the therapeutic level of colistin is available in the United States. Tigecycline Tigecycline, a parenteral broad-spectrum bacteriostatic agent, is approved for treatment of compli-cated skin and skin structure infec-tions and intra-abdominal infecinfec-tions caused by susceptible organisms.39 In one study,38
in susceptibility test-ing, the minimum inhibitory con-centration required to inhibit the growth of 90% of organisms in vitro was 2.0 μg/mL for 739 isolates of Acinetobacter,indicating the poten-tial clinical effectiveness of tigecy-cline. Tigecycline’s mechanism of action involves binding to the 30S ribosomal subunit and blocking protein synthesis.
Tigecycline has a 7 to 9 L/kg vol-ume of distribution and a half-life of approximately 42 hours. A loading dose of 100 mg is recommended, with a maintenance dose of 50 mg every 12 hours. No dose adjustment is required for patients with renal impairment or mild to moderate hepatic impairment. Major side effects include nausea (29.5%), vomit-ing (19.7%), and diarrhea (12.7%).36 Infection Control Measures
Once the cluster of MDR A bau-manniiwas recognized, discussions occurred between personnel in infec-tion control and the nurse managers of the affected ICUs. Contact precau-tions were implemented for the patients who had infections caused not provide interpretation of
“sus-ceptible”, “intermediate,” and “resis-tant” for susceptibility to tigecycline because of a lack of correlating clini-cal data. Without an interpretation, only the size of the area of growth inhibition could be reported. Hence, the interpretation of these findings was left up to individual physicians.
In mid-February 2006, the use of tigecycline E-test strips was imple-mented by our microbiology labora-tory. (E-test strips are impregnated with a predefined antibiotic gradient. They are placed on agar culture plates that have been inoculated with the organism. The goal is to determine the in vitro minimum inhibitory concentration.) Results and inter-pretations of the E-tests were pro-vided to clinicians according to the Food and Drug Administration’s interpretive guidelines to provide more standardized and informa-tional guidance to physicians. Colis-timethate was used clinically because of its proven ability to treat infections caused by MDR A baumanniiand other MDR organisms.38,40
According to The Surveillance Network,37
the susceptibility of A baumanniiisolates to polymyxin B in the United States is 95.4%. During the outbreak, no polymyxin B–resistant organisms were identified. Tigecycline, a new broad-spectrum minocycline deriva-tive, received approval from the Food and Drug Administration in June 2005.39
We subsequently used tigecycline because of the reported in vitro sus-ceptibility of A baumanniito this drug. By the E-test strip method, the susceptibility of MDR A bau-manniiat the medical center Febru-ary through June 2006 was 71%. Susceptibility to tigecycline has
rap-idly declined; only 39% of isolates obtained from July through Decem-ber 2006 were susceptible, and 22% of those obtained from January through June 2007. Of note, this resistance pattern has emerged despite restriction of tigecycline to treatment of MDR organisms that were sensitive only to colistin and tigecycline. The combination of col-istimethate and tigecycline was pre-scribed for many of our patients because the severity of illness, limited susceptibility information, and lack of clinical outcome data for tigecycline. Colistimethate Colistimethate is an antimicrobial produced by Bacillus colistinus. It became commercially available in 1959. Use of this agent has been limited because of its nephrotoxicity and the availability of less toxic agents. It is approved by the Food and Drug Administration for treatment of acute or chronic infections due to susceptible gram-negative bacteria. Colistimethate is hydrolyzed to colistin, also known as polymyxin E. Colistin acts as a cationic detergent to damage the bacterial cell wall, resulting in leak-age of intracellular substances and cell death. Colistin is eliminated via the kidneys and has a half-life of 1.5 to 8 hours.41
The most common dose of colis-timethate is 2.5 mg/kg intravenously every 12 hours for patients with normal renal function. Nephrotoxic, neurotoxic, and pulmonary toxic effects are significant adverse events associated with this drug. Dose and interval adjustments are recom-mended for patients with creatinine clearance less than 75 mL/min. However, dosing modifications for patients with renal impairment are
by MDR A baumannii, as per hospi-tal policy for any patient with an MDR organism. As new patients continued to be identified, it became apparent that contact precautions were not controlling the outbreak. Nursing staff reported that some colleagues, particularly physicians, but also other staff working on and off the units, had not been following strict contact precautions.
Cohorting or keeping patients who have the same illness together, is a strategic intervention to limit outbreaks of infections caused by MDR organisms.42
The patients were moved to a single ICU, and the unit was closed to other patients. Nurs-ing and respiratory staff were dedi-cated to that unit: they did not respond to code calls or assist in other units during their shift. Equip-ment was dedicated to that unit as well (eg, portable x-ray machine). In order to verify that the isolates were related, isolates from 4 patients were sent to the Arizona state laboratory for ribotyping and pulse field gel electrophoresis (PFGE). Results con-firmed that the isolates were identical. Recent reports of PFGE testing to prove clonal spread is useful in determining the appropriate actions to control an outbreak.43
The results of our request for PFGE testing prompted the state health department to investigate the prevalence of MDR A baumannii throughout Phoenix. The investiga-tion indicated some unrecognized endemicity of this organism in the greater Phoenix area. Of the Phoenix isolates tested, 80% were the same type, and a quarter of those had indi-cations of single point mutations, indicating that although the isolates appeared to come from a single
ready for use, were cultured; all were negative for A baumannii. The respiratory therapy department created a spreadsheet to track spe-cific ventilator use on individual patients. Ventilator use did not explain patient transmission.
Transmission via bronchoscopes was also investigated. Cleaning pro-cedures were reviewed. No new technicians were cleaning the bron-choscopes, and all the technicians were well trained and had received updated annual in-service education. The bronchoscopes were tracked, and their use in patients affected by the outbreak was determined. Only 2 bronchoscopes were used on more than a single patient with MDR A baumannii, and in both instances, use of the bronchoscope in patients who became infected with A bau-manniiwas separated by at least a 2-week period, and the instrument was used in between on other patients who did not become infected.
A new procedure for active sur-veillance was initiated. Each time MDR A baumanniiwas isolated from a new patient receiving mechanical ventilation, contact precautions were implemented empirically for all patients in that nursing unit who were receiving mechanical ventila-tion. The use of the precautions was continued until a sputum specimen negative for MDR A baumanniiwas obtained from each patient. Addi-tionally, for any patient admitted from an outside facility who was receiving mechanical ventilation or had a tracheostomy, contact precau-tions were implemented empirically until a sputum specimen negative for A baumanniiwas obtained. This precaution has continued. Cohorting was discontinued on March 1, 2006, source, this organism had been
circu-lating in the area for a while. We investigated environmental sources of contamination at the medical center. It was verified that our hospital disinfectant (a quater-nary ammonium compound) was effective against Acinetobacter. Ran-dom specimens for culturing were taken in patients’ rooms from fre-quently touched surfaces, including beds, bed rails, intravenous pumps, and ventilator faces. Of 13 cultures, 7 were positive for A baumannii.
Extensive education was done with the environmental services staff about the importance of attention to detail in room cleaning. Additional education was done with clinical staff (nurses, physicians, and respi-ratory therapists); data on the posi-tive environmental cultures were used to reinforce the need for strict contact precautions with gowns, hand hygiene, and so on. Later, specimens were obtained from vacant cleaned rooms in the cohort nursing unit and at the nurses’ station (ie, automatic medication-dispensing machines, telephones, and computers). All specimens were negative for A bau-mannii, verifying that the cleaning with our disinfectant was effective.
Of the first 9 cases at the medical center, 6 occurred in patients receiv-ing mechanical ventilation, so atten-tion was focused on the ventilators. It was verified that when mechanical ventilation was discontinued, the circuits on the machine were dis-carded and the outside of the machine was disinfected. The ventilators used on patients who had A baumannii infections were, in addition, sent to the decontamination department for extensive cleaning. Exhalation filters on several random ventilators,
when only 2 patients remained in the unit and no new patients had been identified for 3 weeks.
A second cohort unit was started at the end of May 2006, nearly 3 months after the first cohort unit had closed. Intermittent cases of MDR A baumanniiinfections had been identified, but when 8 patients in different ICUs with such infec-tions were identified during the same time frame, the decision was made to open a cohort unit. After 3 weeks, 3 patients remained, and the unit was opened up to patients who did not have A baumannii infec-tions. The latter patients had to be at low risk for infection: no mechan-ical ventilation, no tracheostomies, and no surgical or open wounds. No new clusters of patients infected with this organism have occurred since that time.
Staffing Impact
Staffing needs of a cohort unit vary from the usual. As might be expected, challenges during the use of a cohort unit included matching the number and types of staff required with available resources. Most of the patients required a 1 to 1 nurse to patient ratio because of the frequency of treatments, tests, and drug ther-apies. As isolation precautions intensified, so did patient acuity. Additionally, with this model of cohorting infectious patients, mem-bers of the nursing staff were required to assume additional responsibili-ties. Of note was their need to coach all healthcare workers, including physicians, who interacted with patients to ensure that proper con-tact precautions were being adhered to during patient contact. The staffing implications also affected respiratory
therapy staff, because they were restricted to the cohort unit for the duration of a shift, and often that ICU did not require a respiratory therapist full time. Staffing these cohort units increased the variance between budgeted and actual costs. Information: Getting Out a Consistent Message
During the cohort experience, we used multiple strategies to quickly bring the most current information about the cohorting procedure to the nursing staff. First, the nursing management and infection control teams made rounds at least daily, and at times more often, to update the staff about the situation and to address questions. These rounds provided a time for day and night nursing staff to speak with infection control staff and to inform manage-rial staff of the nurses’ needs. Second, it was necessary to update all health-care providers around the clock. Because the members of the nursing staff were the liaisons and primary educators for what was transpiring in the units, these personnel needed more resources to provide ongoing, timely, and accurate information to a variety of colleagues involved in the unit’s functioning. As a result, an “Acinetobacterupdate” flyer (Figure 2) was created. The flyer was updated periodically to keep the staff informed of any new issues or pertinent clini-cal changes related to Acinetobacter. In addition, extensive education was done, on a continuing basis, to increase compliance with contact precaution measures.
Staff Responses to the Outbreak At the beginning of the outbreak, a general sense of fear and uncertainty
existed in the unit. Acinetobacter baumanniiwas an unknown organ-ism to the staff, and most of the nurses were unfamiliar with the threat it posed to themselves and their families. The initial days were characterized by questions about what to wear, what not to touch, how often to wash hands, and how long the unit would remain cohorted. One staff nurse said the following:
I remember working on the A baumanniiunit for the first time: gowns, gloves, booties, and isolation signs covered the entire unit. Everyone seemed to have a fear of working here. Some would refuse. Nurses feared for their health and that of their families. Questions and uncertainties filled the day: Should I shower at work? Should I change my scrubs before going home? Will I become infected?
News of the unit’s cohorting sta-tus quickly spread throughout the hospital. The unit became known as the “quarantine” or the “bug unit.” These names created an even deeper sense of isolation for the nursing staff working there. The staff were stigmatized and characterized as being different. Some staff members asked to be transferred. The nurses who remained felt an overwhelming sense of exhaustion as each day the requirement to gown and glove upon entering a patient’s room seemed increasingly burdensome.
As the outbreak continued and core staff began to understand the need and purpose for cohorting, fear dissipated and the staff assumed ownership of this special
population of patients. One nurse remarked as follows:
Core staff became comfort-able with the isolated unit. I remember working on the A baumanniioutbreak unit for 3 months straight. I became an advocate for proper edu-cation to doctors, nurses, and other healthcare providers,
Figure 2 Example of an Acinetobacter update flyer.
Abbreviations: ET, endotracheal tube; ICU, intensive care unit; LTC, long-term care; trach, tracheostomy; vent, mechanical ventilation. Reprinted with permission of Banner Good Samaritan Medical Center, Phoenix, Arizona.
Critical Care Nursing News
AcinetobacterUpdate
March 24, 2006
Due to the newness of this pathogen and the evolving nursing care requirements associated with this patient population, a periodic newsletter will be sent to critical care areas to ensure all staff have access to updated, timely information. This is the second newslet-ter in this series of updates.
Definition:
Acinetobacter baumaniiis a gram-negative bacteria, often found in soil and water and can be isolated readily from many sources in the environment. It can survive for long periods of time in the environment and tolerates both moist and dry conditions. Resistant strains of this bacteria have developed recently throughout the United States and are difficult to treat. In hospitals, Acinetobacter baumannii is most common in ICU and burn patients. It poses very little risk to healthy people.Patients at highest risk are very ill, on ventilators, have open wounds and/or have many invasive devices.
As of March 1st, we are no longer cohorting patients. Strict adherence to Contact Precautions and optimum hand hygiene remain the standard of care. We are continuing to screen all patients being transferred to us from long term care facilities if they are vented, have a trach, or have large or draining wounds. Such patients are placed into Contact Precautions upon admission, and remain so until screening cultures are finalized.
These resistant organisms have been found in many hospitals around our valley. The Arizona Department of Health Services has been collecting isolates from hospitals around Arizona and most have turned out to be identi-cal strains. In the long term, this may be an organism that is here to stay. The most recent nosocomial isolates of resistant Acinetobacter were in sputum specimens from 2 of our patients, both collected on 3/22/06. It had been a month since the last one was identified on 2/26/06.
For patients admitted from LTC with a trach, draining wound, or who are vented:
√Immediately upon Admission, place the patient in Contact Precautions;
√Obtain a culture of the site (i.e., trach, draining wound, or ET tube);
√Notify Infection Control x 34390; may leave a message.
Question of the Week What kind of patient can be paired with an Acinetobacter patient?
Ideally, for a patient in an ICU, a 1:1 assignment is preferred. If that is not possible, the nurse should be assigned to a non-vented/non-trached patient, one who has not had recent surgery, and one with few invasive devices or draining wounds.
Please call ***** (x 34390 or page 555-5555)if you have any concerns and please refer to these evolving updates for continued information.
compiling education posters for display throughout our hospital so that others could understand more about this bacterial outbreak.
The initial struggle evolved into a shared ownership between the critical care nursing staff, infection control specialists, and nursing management. The need to
compre-hensively educate the hospital and public became a joint venture. For example, the routine process of sending a patient for a medical imag-ing procedure became a seemimag-ingly unyielding event because of the increased demands for preparation, planning, transportation, and per-forming the procedure. An added burden was also imposed on staff
who remained in the unit to oversee patient care in the absence of the nurse deemed responsible for care during this time.
Finally, as the decrease in the number of infected patients became obvious, staff realized how the combination of cohorting, effective hand hygiene, and institutional education had worked together to combat the spread of MDR A bau-mannii. Although staff nurses were obviously approaching “burnout”
near the culmination of this experi-ence, the support of nursing man-agement and the infection control specialists sustained the core nursing staff by providing daily effective commun ication and listening to staff members’ concerns about and reac-tions to this intense experience.
Clinical Recommendations
The first and foremost clinical recommendation for preventing out-breaks of MDR A baumannii
infec-tion is early recogniinfec-tion: develop a method to track the incidence and resistance patterns of all Acineto bacter isolates in your critical care areas.4 By the time a patient arrives in the ICU, he or she is often heavily pre-treated and highly compromised and thus vulnerable to a number of potentially fatal sequelae. Patients with known clinical infection most likely represent only a small per-centage of microbial colonization/ contamination, signifying the
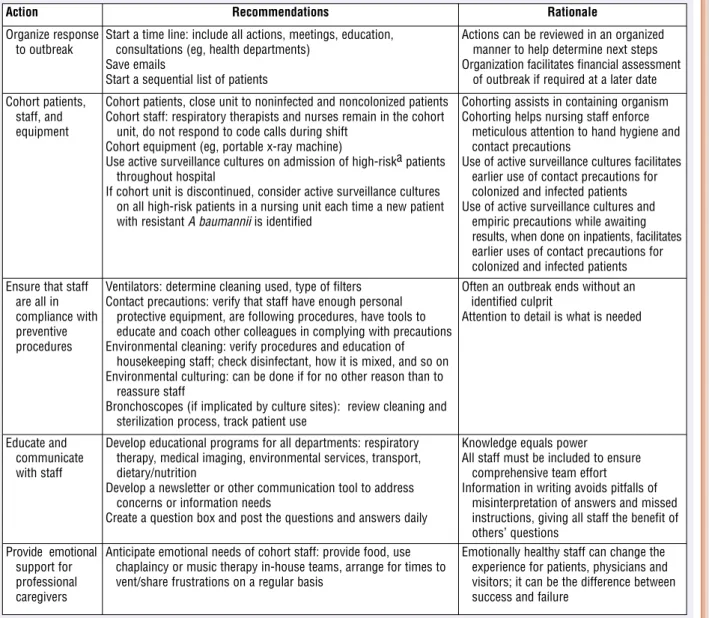
Table 6 Recommendations for control of Acinetobacter baumanii outbreaks
a During the outbreak at Banner Good Samaritan Medical Center, patients from long-term care facilities who were receiving mechanical ventilation or had a tracheotomy and any patient with draining wounds were high risk.
Action Recommendations Rationale
Organize response to outbreak
Start a time line: include all actions, meetings, education, consultations (eg, health departments)
Save emails
Start a sequential list of patients
Actions can be reviewed in an organized manner to help determine next steps Organization facilitates financial assessment
of outbreak if required at a later date Cohort patients,
staff, and equipment
Cohort patients, close unit to noninfected and noncolonized patients Cohort staff: respiratory therapists and nurses remain in the cohort
unit, do not respond to code calls during shift Cohort equipment (eg, portable x-ray machine)
Use active surveillance cultures on admission of high-riska patients throughout hospital
If cohort unit is discontinued, consider active surveillance cultures on all high-risk patients in a nursing unit each time a new patient with resistant A baumanniiis identified
Cohorting assists in containing organism Cohorting helps nursing staff enforce
meticulous attention to hand hygiene and contact precautions
Use of active surveillance cultures facilitates earlier use of contact precautions for colonized and infected patients Use of active surveillance cultures and
empiric precautions while awaiting results, when done on inpatients, facilitates earlier uses of contact precautions for colonized and infected patients Ensure that staff
are all in compliance with preventive procedures
Ventilators: determine cleaning used, type of filters Contact precautions: verify that staff have enough personal
protective equipment, are following procedures, have tools to educate and coach other colleagues in complying with precautions Environmental cleaning: verify procedures and education of
housekeeping staff; check disinfectant, how it is mixed, and so on Environmental culturing: can be done if for no other reason than to
reassure staff
Bronchoscopes (if implicated by culture sites): review cleaning and sterilization process, track patient use
Often an outbreak ends without an identified culprit
Attention to detail is what is needed
Educate and communicate with staff
Develop educational programs for all departments: respiratory therapy, medical imaging, environmental services, transport, dietary/nutrition
Develop a newsletter or other communication tool to address concerns or information needs
Create a question box and post the questions and answers daily
Knowledge equals power
All staff must be included to ensure comprehensive team effort
Information in writing avoids pitfalls of misinterpretation of answers and missed instructions, giving all staff the benefit of others’ questions
Provide emotional support for professional caregivers
Anticipate emotional needs of cohort staff: provide food, use chaplaincy or music therapy in-house teams, arrange for times to vent/share frustrations on a regular basis
Emotionally healthy staff can change the experience for patients, physicians and visitors; it can be the difference between success and failure
“iceberg phenomenon.”6
Prevalence of infection in the setting may be only partially realized.
Our list of recommendations for facilities that must address the man-agement of A baumanniiinfections fall into 5 categories (Table 6). Consideration of Cost
The costs associated with a hospital-acquired infection are sig-nificant.2,44In the United States, an estimated 250000 episodes of hospital-acquired infection occur annually, with a total cost of nearly $5 billion, associated mortality rates of 35%, an extended mean length of hospitalization of 24 days, and added costs exceeding $40000 per survivor.7,10,45The cost of treating resistant hospital-acquired infec-tions is staggering, particularly in critical care.24ICU beds account for 5% to 10% of inpatient beds, yet account for more than 30% of hospi-tal budgets and 8% of healthcare costs45-47(Table 7).
According to one estimate,48the overall cost to contain an outbreak
• Investigation of intervention timing (eg, cohorting patients, staff, equipment) and its impact on the magnitude of the outbreak
Variations in nursing care inter-ventions for ICU patients infected with MDR organisms have not been identified. Frequency of culturing, types of cohorting, communication strategies, prevalence, and intensity of adverse reactions to multiple drug therapies remain unknown. Preventive interventions are difficult to measure, and most researchers did not describe the monitoring of infection control practices.4We make no recommendations about staffing for patients with MDR pathogens; however, high work load can be a contributing factor for the acquisition of antimicrobial-resistant organisms.18
Conclusion
A new class of patient has unin-tentionally evolved in healthcare: the chronically critically ill.22 Increases in the number of such patients will require added nursing resources and expertise. These com-plex patients also require fine-tuned teams with respect for specialty knowledge. In our experience with an outbreak of infections caused by MDR A baumannii, a high-quality team effort was responsible for a timely, interdisciplinary, and ulti-mately successful effort to contain a potentially widespread outbreak. Acknowledgments
We wish to acknowledge significant contributions for this article from Michael A. Saubolle, PhD,Medical Direc-tor, Infectious Disease Division, Laboratory Sciences of Arizona, Banner Health; Adarsh Khalsa, Microbiology Technical Specialist, Banner Health; Mark F. Rudinsky,
MD,Chairman, Infection Control Committee, Banner Good Samaritan Medical Center; and ICU staff and physicians at Banner Good Samaritan Medical Center. Financial Disclosures
None reported. was $220000 per patient. Addi tion
-ally, the hospital may lose more than $2 million in potential revenue because of the loss of nearly 300 hospital-bed days because of room closings. Although our review did not include quantification of cost, we recommend the integration of cost data in future analyses of outbreaks. Quality Improvement and Nursing Research Indices
Although infection is a nurse-sensitive indicator of quality care,45 personnel from numerous health-care disciplines interact with patients in the ICU. In order to improve outcomes in patients with MDR and potentially fatal infec-tions, nurse-promoted multidiscipli-nary inquiries could target the following areas:
• Proactive planning to anticipate the emergence of MDR organisms
• Ongoing collaboration with infection control practitioners regarding trends of outbreaks of infections caused by MDR organ-isms and prevention strategies
• Providing a forum to enhance staff nurses’ criti-cal thinking
•Identifying
the interrelation-ship of host factors (eg, type, number and severity of comorbid condi-tions, age, and effect of antibiotic polypharmacy)
•Staff
com-pliance with stan-dard precaution requirements (ie, hand hygiene, gown use)
Table 7 Costs of an outbreak Direct
• Prolonged length of stay
• Consumption of supplies (eg, personal protective equipment, disposal of supply cart contents after patient is discharged)
• Use of professional services (eg, consultations with physicians, dedicated respiratory personnel)
• Dedicated equipment for the unit (eg, portable electrocardio-graphic and x-ray machines)
• Pay for nursing full-time equivalents
• Laboratory services (eg, additional surveillance cultures, environmental and patient screening, pulse field gel electrophoresis testing)
Indirect
• Onsite time for chaplain, psychologist unit manager, intensive care nurses
• Loss of intensive care unit bed days Outbreak containment
References
1. Chastre J, Trouillet JL. Problem pathogens (Pseudomonas aeruginosaand Acinetobacter).
Semin Respir Infect.2000;15(4):287-298. 2. Wilson SJ, Knipe CJ, Zieger MJ, et al. Direct
costs of multidrug-resistant Acinetobacter baumanniiin the burn unit of a public teach-ing hospital. Am J Infect Control.2004;32(6): 342-344.
3. Simor AE, Lee M, Vearncombe M, et al. An outbreak due to multiresistant Acinetobacter baumanniiin a burn unit: risk factors for acquisition and management. Infect Control Hosp Epidemiol.2002;23(5):261-267. 4. Villegas MV, Hartstein AL. Acinetobacter
outbreaks, 1977-2000. Infect Control Hosp Epidemiol.2003;24:284-295.
5. Fournier PE, Richet H. The epidemiology and control of Acinetobacter baumanniiin health care facilities. Clin Infect Dis. 2006; 42(5):692-699.
6. Bayuga S, Zeana C, Sahni J, Della-Latta P, el-Sadr W, Larson E. Prevalence and antimi-crobial patterns of Acinetobacter baumannii
on hands and nares of hospital personnel and patients: the iceberg phenomenon again.
Heart Lung.2002;31(5):382-390. 7. Brooklyn Antibiotic Resistance Task Force.
The cost of antibiotic resistance: effect of resistance among Staphylococcus aureus,
Klebsiella pneumoniae, Acinetobacter bau-mannii, and Pseudomonas aeruginosaon length of hospital stay. Infect Control Hosp Epidemiol.2002;23(2):106-108.
8. Centers for Disease Control and Prevention. Campaign to Prevent Antimicrobial Resist-ance in Healthcare Settings fact sheet: 12 steps to prevent antimicrobial resistance among hospitalized adults. http://www.cdc .gov/drugresistance/healthcare/ha/12steps _HA.htm. Accessed November 9, 2007. 9. Al Naiemi N, Duim B, Savelkoul PH, et al.
Widespread transfer of resistance genes between bacterial species in an intensive care unit: implications for hospital epidemi-ology.J Clin Microbiol. 2005;43(9):4862-4864.
10. Niederman M. Impact of antibiotic resist-ance on clinical outcomes and cost of care.
Crit Care Med. 2001;29(suppl 4):N114-N120. 11. Gusten WM, Hansen EA, Cunha BA. Acine-tobacter baumanniipseudomeningitis. Heart Lung.2002;31:76-78.
12. Hiong C, Joseph T, Cunha BA. Acinetobacter baumanniiline-associated infection. Heart Lung.2000;29:222-224.
13. American Thoracic Society, Infectious Dis-eases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated and healthcare-associ-ated pneumonia. Am J Respir Crit Care Med.
2005;171(4):388-416.
14. Gales AC, Jones RN, Forward KR, Linares J, Sader HS, Verhoef J. Emerging importance of multidrug-resistant Acinetobacter species and Stenotrophomonas maltophiliaas pathogens in seriously ill patients: geographic patterns, epidemiological features, and trends in the SENTRY Antimicrobial Sur-veillance Program (1997-1999). Clin Infect Dis.2001;32(suppl 2):S104-S113. 15. Lorente C, del Castillo Y, Rello J. Prevention
of infection in the intensive care unit: cur-rent advances and opportunities for the future. Curr Opin Crit Care.2002;8:461-464. 16. Rello J, Diaz E. Acinetobacter baumannii: a
threat for the ICU? Intensive Care Med.2003; 29:350-351.
17. Bernards AT, Harinck HI, Dijkshoorn L, van der Reijden TJ, van den Broek PJ. Per-sistent Acinetobacter baumannii? Look inside your medical equipment. Infect Con-trol Hosp Epidemiol.2004;25(11):1002-1004. 18. Fierobe L, Lucet JC, Decré D, et al. An
out-break of imipenem-resistant Acinetobacter baumanniiin critically ill surgical patients.
Infect Control Hosp Epidemiol.2001;22(1): 35-40.
19. Goldrick BA. Monitoring the health of military personnel. Am J Nurs.2005; 105(2):29-30.
20. D’Agata DM, Thayer V, Schaffner W. An outbreak of Acinetobacter baumannii: the importance of cross-transmission. Infect Control Hosp Epidemiol.2000;21:588-591. 21. Bhalla A, Pultz NJ, Gries DM, et al.
Acquisi-tion of nosocomial pathogens on hands after contact with environmental surfaces near hospitalized patients. Infect Control Hosp Epidemiol.2004;25(2):164-167. 22. Cardoso CL, Pereira H, Zequin JC,
Guilher-metti M. Effectiveness of hand-cleansing agents for removing Acinetobacter bauman-niistrain from contaminated hands. Am J Infect Control.1999;27(4):327-331. 23. Denton M, Wilcox MH, Parnell P, et al.
Role of environmental cleaning in control-ling an outbreak of Acinetobacter baumannii
on a neurosurgical intensive care unit.
Intensive Crit Care Nurs.2005;21(2):94-98. 24. Houghton D. Antimicrobial resistance in the
intensive care unit: understanding the prob-lem. AACN Clin Issues.2002;13:410-420. 25. Todd B. Beyond MRSA: VISA and VRSA:
what will ward off these pathogens in health care facilities? Am J Nurs.2006;106(4):28-30. 26. Romero DV, Treston J, O’Sullivan AL.
Hand-to-hand combat: preventing MRSA.
Nurs Pract.2006;31(3):16-18, 21-25. 27. Dzidic S, Bedekovic V. Horizontal gene
transfer-emerging multidrug resistance in hospital bacteria. Acta Pharmacol Sin.
2003;24(6):519-526.
28. Livermore DM. Bacterial resistance: ori-gins, epidemiology, and impact. Clin Infect Dis. 2003;36(suppl 1):S11-S23. 29. Levy SB. The challenge of antibiotic
resist-ance. Sci Am.1998;278:46-53. 30. Landman D, Quale JM, Mayorga D, et al.
Citywide clonal outbreak of multiresistant
Acinetobacter baumanniiand Pseudomonas aeruginosain Brooklyn, NY: the preantibi-otic era has returned. Arch Intern Med.
2002;162(13):1515-1520.
31. Aygun G, Demirkian O, Utku T, et al. Envi-ronmental contamination during a car-bapenem-resistant Acinetobacter baumannii
outbreak in an intensive care unit. J Hosp Infect.2002;52(4):259-262.
32. Wang SH, Sheng WH, Chang YY, et al. Heathcare-associated outbreak due to pan-drug resistant Acinetobacter baumanniiin a surgical intensive care unit. J Hosp Infect.
2003;53(2):97-102.
33. Mah MW, Memish ZA, Cunningham G. An outbreak of Acinetobacter baumanniiin an intensive care unit associated with tra-cheostomy. Am J Infect Control.
2001;29:284-288.
34. Garnacho-Montero J, Ortiz-Leyba C, Jimenez-Jimenez FJ, et al. Treatment of mul-tidrug-resistant Acinetobacter baumannii
ventilator-associated pneumonia (VAP) with intravenous colistin: a comparison with imipenem-susceptible VAP. Clin Infect Dis.2003;36(9):1111-1118.
35. Colistimethate package insert. Minneapo-lis, MN: Paddock Laboratories; 2005. 36. Tigecycline [package insert]. Philadelphia,
PA: Wyeth Pharmaceuticals Inc; 2007. 37. The Surveillance Network Database—USA.
http://www.focusdx.com/focus/cms/cms .asp?pid=cms_XIKI33Z0G. Accessed December 5, 2007.
38. Garrison M, Neumiller J, Setter S. Tigecy-cline: an investigational glycylcycline antimicrobial with activity against resistant gram-positive organisms. Clin Ther. 2005 ;27:12-22.
39. Institute of Medicine. Antimicrobial Resist-ance: Issues and Options.Washington DC: National Academy Press; 1998. 40. Ling ML, Ang A, Wee M, Wang GC. A
nosocomial outbreak of multiresistant
Acinetobacter baumanniioriginating from an intensive care unit. Infect Control Hosp Epidemiol.2001;22(1):48-49.
41 Lacy CF, Armstrong LL, Goldman MP, Lance LL. Drug Information Handbook: With International Trade Names Index. 15th ed. Hudson, OH: Lexi-Comp; 2007. Lexi-Comp’s Drug Reference Handbooks. 42. Siegel JD, Rhinehart E, Jackson M,
Chiarello L, and the Healthcare Infection Control Practices Advisory Committee. 2007 Guideline for Isolation Precautions: Pre venting Transmission of Infectious Agents in Healthcare Settings 2007. http://www.cdc.gov/ncidod/dhqp /gl_isolation.html. Accessed December 5, 2007.
43. Stephens C, Francis S, Abell V, DiPersio JR, Wells P. Emergence of resistant Acinetobac-ter baumanniiin critically ill patients within an acute care teaching hospital and a long-term acute care hospital. Am J Infect Control.2007:35(4):212-215.
44. Smyrnios NA, Connolly A, Wilson MM, et al. Effects of a multifaceted, multidiscipli-nary, hospital-wide quality improvement program on weaning from mechanical venti-lation. Crit Care Med.2002;30(6):1224-1230. 45. American Nurses Credentialing Center.
Unit-level nurse-sensitive indicators. In:
Magnet Recognition Program: Application Manual.Silver Spring, MD: American Nurses Credentialing Center; 2005:72. 46. Doran DM, Harrison MB, Laschinger HS,
et al. Nursing-sensitive outcomes data col-lection in acute care and long-term care set-tings. Nurs Res.2006;55(2 suppl):S75-S81. 47. Given BA, Sherwood PR. Nursing sensitive
patient outcomes: a white paper. Oncol Nurs Forum. 2005;32(4):773-784. 48. Dollars and nonsense: ICPs battle bugs,
CE Test
Test ID C081: Acinetobacter baumannii:An Emerging Multidrug-Resistant Pathogen in Critical CareLearning objectives: 1. Identify factors that contribute to the emergence and significance of Acinetobacter baumanniiin healthcare environments 2. Describe the characteristics of A baumanniiand the associated risk factors for development of A baumanniiinfections 3. Discuss nursing interventions, infection control measures, and clinical recommendations for prevention and/or containment A baumannii infections
Program evaluation
Yes No Objective 1 was met K K Objective 2 was met K K Objective 3 was met K K Content was relevant to my
nursing practice K K My expectations were met K K This method of CE is effective
for this content K K The level of difficulty of this test was:
Keasy Kmedium Kdifficult To complete this program,
it took me hours/minutes.
Test answers:Mark only one box for your answer to each question. You may photocopy this form.
1. Acinetobacter baumanniiis a normal inhabitant in which area of the body?
a. Gastrointestinal tract b. Plasma
c. Lungs
d. Skin and mucous membranes
2. What is the most significant factor in the transmission of A baumannii? a. Widespread overuse of broad-spectrum antibiotics
b. Direct contact with persons who have contact dermatitis c. Inadequate hand hygiene among healthcare providers d. The organism’s resistance to multiple hand-cleansing agents 3. How many strains of A baumanniihave been identified thus far? a. 19
b. 15 c. 21 d. 14
4. Which of the following drug’s associated nephrotoxicity requires that doses and intervals be adjusted for patients with renal impairment? a. Tigecycline
b. Imipenem c. Colistimethate d. Aztreonam
5. The term “cohorting” refers to which of the following? a. Colonization of A baumanniion the skin of susceptible persons b. Concurrent use of a combination of 1 or more antimicrobial agents c. Implementation of strict contact isolation procedures for patients at high risk for development of multidrug-resistant (MDR) infections
d. Placement of patients who have the same illness together
6. What is the first and foremost recommendation made by the authors for preventing outbreaks of MDR A baumanniiinfections?
a. The use of a multidisciplinary team to establish infection control meas-ures for each healthcare facility
b. Paying attention to the infection rates specific to critical care settings c. Implementation of contact precautions for patients who have infections caused by MDR A baumannii
d. Extensive education for environmental services staff about the importance of attention to detail in room cleaning
7. Acinetobacter baumanniiis what kind of bacteria? a. Gram-negative, coccobacillary rod
b. Gram-positive, opportunistic fungi c. Gram-negative, nonfermentive spirochete d. Gram-positive, anaerobic mycobacteria
8. Which of the following statements about A baumanniiis true? a. The organism cannot survive on moist surfaces for long periods. b. The organism is inconsequential to hosts with intact immune systems. c. Infections caused by this organism are most prevalent in extended-care and rehabilitation settings.
d. Eradication of the organism from hospital surfaces requires specially formulated cleaning solutions and particular cleaning techniques.
9. What is an expected outcome of establishing a cohort/isolation unit? a. Improved productivity of nursing and respiratory therapy staff
b. Increased ease of matching the number and types of staff required with available resources
c. Increased variance between budgeted and actual costs d. Rapid understanding and acceptance of the need for cohorting
10. Successful prevention of the spread of MDR A baumanniiinfections includes which of the following combinations?
a. Improved staffing, cohorting, and enhanced infection control practices b. Increased interdisciplinary involvement, standardized antibiotic therapy, and review of cleaning procedures
c. Contact precautions on all mechanically ventilated patients, tracking of specific ventilator use on individual patients, and additional education with all clinical staff d. Institutional education, effective hand hygiene, and cohorting
11. Which of the following is a recommendation of the Centers for Disease Control and Prevention’s 12 Steps to Prevent Antimicrobial Resistance Among Hospitalized Adults?
a. Begin antimicrobial treatment with multiple agents at first and eliminate as soon as possible when susceptibility results are available.
b. Treat the infection, not colonization of the bacteria. c. Treat the infection according to the most recent national data. d. Use antimicrobial-treated catheters.
12. Risk factors for acquiring A baumanniiinclude which of the following? a. Male sex
b. Fall or winter season c. Depression
d. Mechanical ventilation
13. What is a recommendation to aid in cohorting patients, staff, and equipment? a. Post flyers and informational literature throughout the facility.
b. Ensure proper cleaning of ventilators and bronchoscopes.
c. Require that staff on the cohort unit do not respond to code calls during shifts. d. Sterilize and disinfect all ventilator circuits used on the cohort unit between patients. 14. What is the estimated cost of outbreak containment per patient?
a. $40 000 b. $220 000 c. $510 000 d. $730 000
For faster processing, take this CE test online at http://ccn.aacnjournals.org
(“CE Articles in this issue”) or mail this entire page to:
AACN, 101 Columbia Aliso Viejo, CA 92656.
Test ID: C081 Form expires: February 1, 2010 Contact hours: 1.0 Fee: AACN members, $0; nonmembers, $10 Passing score: 10 correct (71%) Category: A, Synergy CERP A Test writer: Ann Lystrup, RN, BSN, CEN, CFRN, CCRN
9. Ka Kb Kc Kd 8. Ka Kb Kc Kd 7. Ka Kb Kc Kd 6. Ka Kb Kc Kd 5. Ka Kb Kc Kd 4. Ka Kb Kc Kd 3. Ka Kb Kc Kd 2. Ka Kb Kc Kd 1. Ka Kb Kc Kd 11.Ka Kb Kc Kd 14.Ka Kb Kc Kd 12.Ka Kb Kc Kd 13.Ka Kb Kc Kd 10. Ka Kb Kc Kd Name Member # Address
City State ZIP Country Phone E-mail
RN Lic. 1/St RN Lic. 2/St Payment by: KVisa KM/C KAMEX KDiscover KCheck Card # Expiration Date Signature