Preschool Vision Screening: Summary of a Task Force Report
E. Eugenie Hartmann, PhD*‡; Velma Dobson, PhD§; Louise Hainline, PhD储; Wendy Marsh-Tootle, OD, MS¶; Graham E. Quinn, MD#; Mark S. Ruttum, MD**;
Paulette P. Schmidt, OD, MS‡‡; and Kurt Simons, PhD§§, on Behalf of the Maternal and Child Health Bureau and the National Eye Institute Task Force on Vision Screening in the Preschool Child
V
ision screening to detect eye problems inschool-aged children dates back at least a cen-tury.1Calls to screen specifically for amblyo-pia, generally defined as monocular decreased acu-ity, began appearing by the 1950s.2However, it was not until the 1960s, when animal research indicated that cortical plasticity was limited to a period early in life, that emphasis was placed on vision screening in the preschool years. Since that time, a variety of preschool screening programs have been adopted in various countries,3ranging from the systematic and thorough efforts of Scandinavian countries that eval-uate screening methods and outcome from infancy through preschool ages,3,4to the diversity of screen-ing standards (Table 1) and screenscreen-ing programs found in different jurisdictions across the United States.5,6
Recommendations for health-related screening programs, developed by the World Health Organi-zation,7 require that a disorder suitable for mass screening should have a high prevalence in the pop-ulation, should result in significant impairment to the individual, and should be treatable at the time of its detection. Although the Scandinavian experience and other data make clear the effectiveness of pre-school screening in reducing visual morbidity from amblyopia,8 –10fundamental questions remain about specific issues, ranging from screening methodology to quantitative measures of both efficacy and cost-effectiveness of such screening. These questions were recently brought to focus by a report from the United Kingdom questioning the utility of preschool vision screening.11–13Although both the data interpretation and conclusions of this report have been
ques-tioned,14 –23 it has given impetus to a reexamination of the why and how of preschool vision screening.
Recognizing the growing list of questions about preschool vision screening and the lack of consis-tency in preschool vision screening recommenda-tions and programs in the United States, Congress urged the Maternal and Child Health Bureau in the Health Resources and Services Administration to consult with the National Eye Institute of the Na-tional Institutes of Health, Department of Health and Human Services, and various national and state agencies, to review both research and policy issues involved in vision screening in preschool-aged chil-dren. The specific request was to determine “useful screens to efficiently detect amblyopia risk factors and other significant problems” and “to provide and evaluate the practicality and effectiveness of ocular screening services for young children, including pho-toscreening technology.” As a result of this recom-mendation, an expert panel convened in September 1998, and a report from this panel was released in May 1999.24
There were 2 major outcomes of the expert panel’s deliberations.
OUTCOME 1
Lack of Data on Validity and Effectiveness of Current Screening Methodologies and Programs
The panel expressed concern about the lack of scientific data addressing the validity of currently available screening methodologies, the effectiveness of the programs that are being used to implement these methodologies, and the adequacy of follow-up and treatment of children identified by screening programs. Members acknowledged an urgent need for large-scale, generalizable studies aimed at an-swering basic questions about the reliability and va-lidity of commonly used screening methods, as well as new technologies, such as photoscreening. The panel also emphasized the importance of monitoring both the costs and benefits of a screening program, compared with the cost of leaving visual impair-ments undetected, and recommended that research be conducted to provide objective data on the func-tional implications of amblyopia.
One of the forces driving the convening of the expert panel was the increasing availability and im-plementation of photoscreening in preschool set-tings. Photoscreening, in principal, represents one of
From the *Department of Psychology, Hunter College of the City University of New York, New York, New York; ‡Glaucoma Associates of New York, The New York Eye and Ear Infirmary, New York, New York; §Departments of Ophthalmology and Psychology, University of Arizona, Tucson, Ari-zona;储Department of Psychology, Brooklyn College of the City University of New York, Brooklyn, New York; ¶School of Optometry, University of Alabama, Birmingham, Alabama; #Division of Ophthalmology, The Chil-dren’s Hospital of Philadelphia, Philadelphia, Pennsylvania; **Eye Institute, Medical College of Wisconsin, Milwaukee, Wisconsin; ‡‡College of Optom-etry, The Ohio State University, Columbus, Ohio; and §§Krieger Children’s Eye Center, Wilmer Eye Institute, Johns Hopkins Hospital, Baltimore, Mary-land.
Received for publication Sep 10, 1999; accepted Apr 3, 2000.
Reprint requests to (J.A.S.) Research and Public Policy, Prevent Blindness America, 500 E Remington Rd, Schaumburg, IL 60173. E-mail: [email protected]
the most dramatic developments in the history of preschool vision screening.8 This technique can be applied in early infancy and opens up the possibility of detecting risk factors in a “latent” period before the onset of amblyopia itself. Photoscreening has several advantages over conventional screening tech-niques. Most notably, it is easier to use with these often difficult-to-test individuals than typical recog-nition acuity tests and the resulting photographs (or video images) can provide a quantifiable objective measure. Nonetheless, current photoscreening tech-nologies typically require some degree of interpreta-tion of the results by the examiner. Furthermore, photoscreeners measure amblyopia risk factors not amblyopia itself and, therefore, the efficacy of detect-ing amblyopiogenic risk factors before the onset of amblyopia must be compared with that of more tra-ditional vision screening programs designed to de-tect amblyopia once it has developed.25,26
Current research indicates that caution should be applied in the use of photoscreening devices in pre-school vision screening. Adequate validation studies are lacking for most devices in this rapidly evolving field, and studies comparing the merits of different instrument designs are almost completely absent. Research using novel technology requires represen-tative screening populations, real-world screening settings, and masked clinical gold standard compar-ison examinations. Compounding the problem of evaluation of new devices is the basic science ques-tion of just which amblyopiogenic condiques-tions a pho-toscreener should be detecting. Conditions such as esotropia and media opacification are well-estab-lished as risk factors for amblyopia, but the type and extent of refractive error that actually produce am-blyopia and the importance of the age of appearance of such risk factors are not adequately specified by current research.8,27,28 Furthermore, although the
TABLE 1. Current Recommendations for Preschool Vision Screening Programs
Organization Age
(Years)
Vision Disorders Method (Any of the Following)
American Academy of Pediatrics33 American Academy of
Ophthalmology34
American Association of Pediatric Ophthalmology and
Strabismus35
3–5 1) Amblyopia
2) Strabismus (ocular misalignment)
1) Snellen letters, Snellen numbers, Tumbling E, HOTV, Picture tests, Allen figures, Lea test (all 3 m)
2) Unilateral cover test (at 3 m) or Random Dot E stereotest (at 40 cm)
American Optometric Association36
2–6 1) Amblyopia 2) High refractive
error
3) Ocular
misalignment/strabismus
4) Color vision deficiencies
1) Monocular visual acuity 2) Patient history, Bru¨ckner test,
Monocular visual acuity, Plus lens test
3) Patient history, observation, Bru¨ckner test, Hirschberg, cover test
4) Ishihara plates or equivalent
Prevent Blindness America37 3–4 1) Eye health 1) Observation/questions 2) Reduced visual
acuity
2) Early Treatment for Diabetic Retinopathy Study letters, HOTV letters, Lea chart, Tumbling E (all charts at 3 m) 3) Reduced stereopsis 3) Random Dot E Stereotest 4) Other (unspecified) 4) Optional tests include: cover
test, corneal reflection test, plus lens tests; they are not recommended. State recommendations may vary
Head Start Program38 3 1) Reduced visual acuity
1) Tumbling E (at 3 m)
2) Strabismus 2) Cover test/Hirschberg test US Public Health Service39 3–4 Amblyopia and
strabismus
Stereotesting, such as Random Dot E stereotest, visual acuity testing, Snellen letters, Snellen numbers, Tumbling E, HOTV, Allen figures, Lea test (all above tests listed in order of decreasing cognitive ability; use test with highest level of which child is capable)
Maternal and Child Health Bureau40
3–5 Reduced visual acuity Ocular misalignment
American Academy of Pediatrics/ American Academy of
correction of refractive error poses no risk to an adult, question has been raised as to whether it may interfere with the normalization of refractive errors, known as emmetropization, that occurs in infants and young children.8,28 –30
OUTCOME 2 Interim Screening Recommendations
The panel concluded its work by confronting the question of what recommendations should be made for preschool screening at the present time, before the research outlined above has been completed. Al-though a variety of recommendations have been published by various organizations5,24(Table 1), the panel believed that the recommendations are incon-sistent and, therefore, confusing. In particular, as shown in Table 1, different tests are recommended by different agencies with little guidance for the selection and implementation of the test.31The panel, therefore, constructed a set of interim
recommenda-tions to detect amblyopia and amblyopiogenic fac-tors using assessment of visual acuity and stereopsis (Table 2). The recommendations are more explicit with regard to the specific tests and methodology to be used than are previous such recommendations, to assist personnel responsible for undertaking screen-ing. However, it should be emphasized that these recommendations are conditional and not based on adequate validation data, since such data are not yet available.
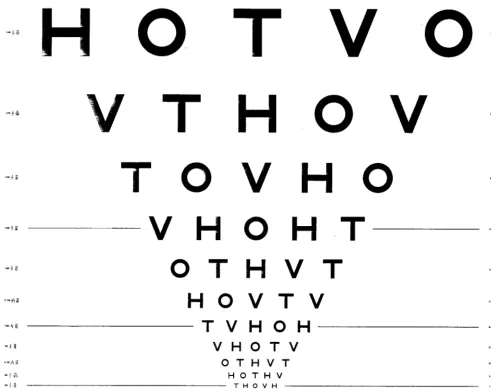
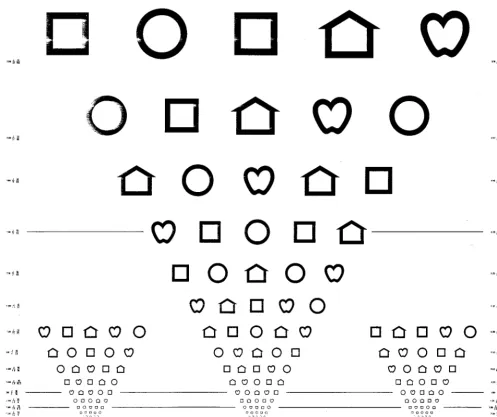
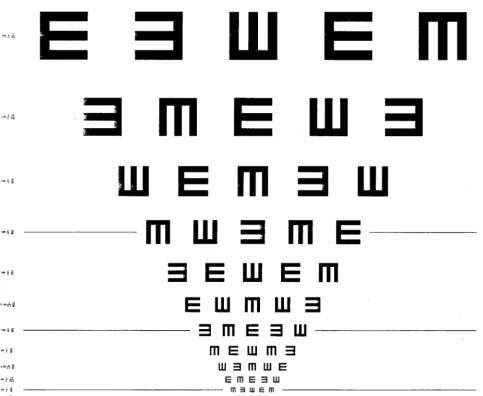
The recommendations are intended for use with 3-and 4-year-old children, since fewer than one half of 3-year-olds are screened in pediatric practices with cur-rent methods.32The most direct way to detect ambly-opia (monocular decreased vision) is to assess monoc-ular visual acuity. For visual acuity assessment, the tests recommended are HOTV, Lea symbols, or tum-bling E charts, because they allow screening of younger children (see Fig 1). Isolated optotypes with surround bars are also acceptable (see Fig 2). In addition, a testing
TABLE 2. Recommendations for Vision Screening Age Range: 36 to 59 Months Function to be
Evaluated
Type of Test Specific Test Recommended Testing Procedures
Passing Criteria
Monocular distance acuity
1) Linear acuity 2) Isolated optotypes
with surround bars NB: isolated optotypes without surround bars should not be used: they overestimate acuity in individuals with amblyopia.
1) HOTV, Lea symbols, Tumbling E 2) HOTV cards
with surround bars
Test distance⫽10 ft (3 m) Pretest (performed binocularly)
Test child’s ability to perform test by having child identify or match each of the 4 optotypes on a line that is expected to be
suprathreshold (20/100 or greater). Child must successfully identify each of the 4 optotypes.
Test procedure (performed monocularly)
Test child’s ability to identify or match optotypes on the line used in the pretest. To proceed, child must identify or match 4 of 5 optotypes on the pretest line. Then test child’s ability to identify or match optotypes on the critical line. Repeat test procedure with the other eye.
Child must identify or match 4 of 5 optotypes on the critical line with each eye tested monocularly. Critical lines
20/40 at 36–⬍48 mo 20/30 at 48–59 mo
Stereopsis Random dot stereogram Random Dot E Test distance⫽40 cm (630 arcsec)
All testing, including pretesting, should be performed binocularly with the polarized glasses on. Pretest
Test child’s ability to perform test by having child identify the location of the 3-dimensional E on 4 of 5 trials (E on left or right; above or below).
Test procedure
Test child’s ability to identify the location of the stereo E. Tester should use 5 presentations, varying location in a nonsystematic manner.
Child must locate stereo E on 4 of 5 presentations.*
procedure and passing criteria are specified. Stereopsis testing is included to detect strabismus as an amblyo-piogenic factor. A specific test, the Random Dot E, is recommended (see Fig 3). Again the testing procedure and passing criteria are specified. (Further details of testing procedures can be found in the complete Pro-ceedings from the Panel.24All tests are commercially available.)
THE NEXT STEP
A critical and unique feature of the expert panel and audience convened for these discussions was the wide range of disciplines represented. Researchers studying early visual development, clinicians (pedi-atricians, pediatric ophthalmologists, and optome-trists), various professionals with direct experience in vision screening in the United States and other countries, biostatisticians, epidemiologists, and
health care economists all participated. This wide representation was deliberately chosen to reflect the fact that vision screening is necessarily conducted by a variety of agencies and specialists. One of the major successes of this meeting was the overall agreement among the array of disciplines represented concern-ing the importance of vision screenconcern-ing in preschool children and the need for continuing work in the realms of both application and research.
The review process begun by the expert panel will be continued under a new initiative being sponsored by the Maternal and Child Health Bureau that will be administered by the American Academy of Pediatrics: Project Universal Preschool Vision Screening. The goal of this initiative is to convene a task force that will include State Maternal and Child Health staff, State Children with Special Health Care Needs staff, the Association of Maternal and Child Health Programs
staff, pediatric and family practice professional organi-zations, consumer organizations cognizant of vision screening issues and needs, and vision experts. The mandate of this broad-based, multidisciplinary task force will be: 1) to analyze the expert panel’s recom-mended guidelines (Table 2) for their applicability to State vision screening programs; 2) to develop stan-dardized recommendations that can be implemented at the State level; 3) to address issues of reimbursement to health professionals for screening, thereby providing incentive for wider adoption of vision screening; 4) to analyze the costs of amblyopia treatment, both finan-cial and in terms of sofinan-cial impact on the child and family; and 5) to propose a system to monitor the States’ preschool vision screening efforts. Further en-dorsement of these goals is found in theHealthy People 2010initiative sponsored by the Department of Health
and Human Services.41 Specifically, increasing “the proportion of preschool children aged 5 years and un-der who receive vision screening” has been identified as 1 of the 10 objectives in the area of visual health.
APPENDIX
Maternal and Child Health Bureau and the National Eye Institute Task Force on Vision Screening
E. Eugenie Hartmann, PhD, Chairperson
Steering Committee Members
Velma Dobson, PhD Louise Hainline, PhD
Task Force Members
Steven Archer, MD
Department of Ophthalmology, University of Michigan, Ann Arbor, MI
Sean Donahue, MD, PhD
Department of Ophthalmology and Visual Sciences, Vanderbilt University School of Medicine,
Nashville, TN
Gunilla Haegerstrom-Portnoy, OD, PhD School of Optometry, University of California Berkeley, Berkeley, CA
Richard Harrad, MD, FRCS
Ophthalmology, Bristol Eye Hospital, Bristol, United Kingdom
Emmett Keeler, PhD
RAND Corporation, Santa Monica, CA Alex R. Kemper, MD, MPH
Department of Pediatrics, University of North Carolina, Chapel Hill, NC
Lynne Kiorpes, PhD
Center for Neural Science, New York University, New York, NY
Ruth E. Manny, OD, PhD
College of Optometry, University of Houston, Houston, TX
Suzanne P. McKee, PhD
Smith-Kettlewell Eye Research Institute, San Francisco, CA
Paulette P. Schmidt, OD, MS
College of Optometry, The Ohio State University, Columbus, OH
John A. Shoemaker, Assistant Vice President Prevent Blindness America, Schaumburg, IL Kurt Simons, PhD
Krieger Children’s Eye Center, Wilmer Eye Institute, Johns Hopkins Hospital, Baltimore, MD Davida Y. Teller, PhD
Department of Psychology, University of Washington, Seattle, WA
James Tielsch, PhD
School of Hygiene and Public Health, Johns Hopkins Hospital, Baltimore, MD
Richard C. Wasserman, MD
Department of Pediatrics, University of Vermont, Burlington, VT
ACKNOWLEDGMENT
Figures courtesy of Precision Vision, 944 First St, La Salle, IL 61301, Phone: 815-223-2022, Fax: 815-223-2224, E-mail: precision [email protected]
REFERENCES
1. Appelboom TM. A history of vision screening.J Sch Health. 1985;55: 138 –141
2. Gundersen T. Glaucoma and amblyopia ex anopsia: two preventable forms of blindness.Trans Sec Ophthalmol AMA. 1954:19
3. Lennerstrand G, Jakobsson P, Kvarnstro¨m G. Screening for ocular dys-function in children: approaching a common program.Acta Ophthalmol Scand Suppl. 1995;214:26 –38
4. Lennerstrand G, Rydberg A. Results of treatment of amblyopia with a screening program for early detection.Acta Ophthalmol Scand Suppl. 1996;219:42– 45
5. Schmidt P. Current screening programs. In: Vision Screening in the Preschool Child. Proceedings of a conference held September 10 –11, 1998; Bethesda, MD. Genetic Services Branch, Maternal and Child Health Bureau, Health Resources and Services Administration, US Department of Health and Human Services; 1999
6. Ciner EB, Dobson V, Schmidt PP et al. A survey of vision screening policy of preschool children in the United States. Surv Ophthalmol. 1999;43:445– 457
7. Wilson JMG, Jungner G.Principles and Practice of Screening for Disease. Geneva, Switzerland: World Health Organization; 1968. Public Health Papers 34
8. Simons K. Preschool vision screening: rationale, methodology and out-come.Surv Ophthalmol. 1996;41:3–30
9. Kvarnstro¨m G, Jakobsson P, Lennerstrand G. Screening for visual and ocular disorders in children, evaluation of the system in Sweden.Acta Paediatr. 1998;87:1173–1179
10. Lithander J. Prevalence of amblyopia with anisometropia or strabismus among schoolchildren in the Sultanate of Oman.Acta Ophthalmol Scand. 1998;76:658 – 662
11. Snowdon SK, Stewart-Brown SL.Pre-School Vision Screening: Results of a Systematic Review. York: NHS Centre for Reviews; 1997. Centre for Reviews and Disseminations Report 9
12. Snowdon SK, Stewart-Brown SL. Pre-school vision screening.Health Technol Assess. 1997;1:1–98
13. Stewart-Brown SL, Snowdon SK. Evidence-based dilemmas in pre-school vision screening.Arch Dis Child. 1998;78:406 – 407. Editorial 14. Rahi JS, Dezateux C. The future of preschool vision screening services in
Britain.Br Med J. 1997;315:1247–1248. Editorial
15. Williams C, Harrad RA, Sparrow JM, et al. Future of preschool vision screening: conclusions for or against services are invalid without ap-propriate research evidence.Br Med J. 1998;316:937. Letter
16. Lee J, Adams G, Sloper J, et al. Future of preschool vision screening: cost effectiveness of screening for amblyopia is a public health issue. Br Med J. 1998;316:937–938. Letter
17. Fielder AR. Future of preschool vision screening: review article did not separate review and implementation processes.Br Med J. 1998;316:938. Letter
18. Aylward GW. Future of preschool vision screening: the existence of a service is not evidence of its value.Br Med J. 1998;316:938. Letter 19. Rahi J, Dezateux C. Authors’ reply.Br Med J. 1998;316:937
20. Moseley MJ. Preschool vision screening: a recent report calls for a halt. Br J Ophthalmol. 1998;82:722–723. Editorial
21. Harrad R. Screening program in Britain. In: Vision Screening in the Preschool Child. Proceedings of a conference held September 10 –11, 1998; Bethesda, MD. Genetic Services Branch, Maternal and Child Health Bureau, Health Resources and Services Administration, US Department of Health and Human Services; 1999
22. Harrad RA, McKee SP. Preschool vision screening: results of a system-atic review.Surv Ophthalmol. 1999;43:374 –376
23. Simons K, Preslan M. Natural history of amblyopia untreated owing to lack of compliance.Br J Ophthalmol. 1999;83:582–587
24. Hartmann EE, ed.Vision Screening in the Preschool Child. Proceedings of a conference held September 10 –11, 1998; Bethesda, MD. Genetic Ser-vices Branch, Maternal and Child Health Bureau, Health Resources and Services Administration, US Department of Health and Human Services; 1999
25. Ottar WL, Scott WE, Holgado SI. Photoscreening for amblyogenic fac-tors.J Pediatr Ophthalmol Strabismus. 1995;32:289 –295
26. Tong PY, Enke-Miyazaki E, Bassin RE, et al, and the National Children’s Eye Care Foundation Study Group. Screening for amblyopia in prever-bal children with photoscreening photographs.Ophthalmology. 1998;105: 856 – 863
27. Archer S. Ocular risk factors for amblyopia. In:Vision Screening in the Preschool Child. Proceedings of a conference held September 10 –11, 1998; Bethesda, MD. Genetic Services Branch, Maternal and Child Health Bureau, Health Resources and Services Administration, US Department
Fig 2. A single optotype with surround bars.
of Health and Human Services; 1999
28. Simons K. Vision screening techniques: a survey. In:Vision Screening in the Preschool Child. Proceedings of a conference held September 10 –11, 1998; Bethesda, MD. Genetic Services Branch, Maternal and Child Health Bureau, Health Resources and Services Administration, US De-partment of Health and Human Services; 1999
29. Ruttum M. Ocular risk factors for amblyopia. In:Vision Screening in the Preschool Child. Proceedings of a conference held September 10 –11, 1998; Bethesda, MD. Genetic Services Branch, Maternal and Child Health Bureau, Health Resources and Services Administration, US Department of Health and Human Services; 1999
30. Smith EL, Hung LF. The role of optical defocus in regulating refractive development in infant monkeys.Vision Res. 1999;39:1415–1435 31. Shoemaker J. Practical aspects of children’s vision screening
pro-grams. In: Vision Screening in the Preschool Child. Proceedings of a conference held September 10 –11, 1998; Bethesda, MD. Genetic Services Branch, Maternal and Child Health Bureau, Health Resources and Services Administration, US Department of Health and Human Services; 1999
32. Wasserman RC, Croft CA, Brotherton SE. Preschool vision screening in pediatric practice: a study from the Pediatric Research in Office Settings (PROS) Network. American Academy of Pediatrics.Pediatrics. 1992;89: 834 – 838
33. American Academy of Pediatrics, Committee on Practice and Ambula-tory Medicine, Section on Ophthalmology. Eye examination and vision
screening in infants, children, and young adults. Pediatrics. 1996;98: 153–157
34. American Academy of Ophthalmology.Pediatric Eye Evaluations: Pre-ferred Practice Pattern. San Francisco, CA: American Academy of Ophthalmology; 1997
35. American Association for Pediatric Ophthalmology and Strabismus. Eye care for the children of America.J Pediatr Ophthalmol Strabismus. 1991;28:64 – 67
36. Scheiman MM, Amos CS, Ciner EB, et al. Pediatric Eye and Vision Examinations: Optometric Clinical Practice Guideline. St Louis, MO: Amer-ican Optometric Association: 1994:1– 45
37. Gerali PS, Flom MC, Raab EL.Report of Children’s Vision Screening Task Force. Schaumberg, IL: National Society to Prevent Blindness; 1990 38. US Department of Health and Human Services.Head Start—A Child
Development Program. Washington, DC: US Department of Health and Human Services; 1980. Publication (OHDS) 80-31092
39. US Public Health Service. Vision screening in children.Am Fam Physi-cian. 1994;50:587–590.
40. Green M, ed.Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. Arlington, VA: National Center for Education in Maternal and Child Health; 1994
41. US Department of Health and Human Services.Healthy People 2010: Understanding and Improving Health. Conference ed. Washington DC: US Department of Health and Human Services
ABSTRACT
Shaneyfelt TM, Mayo-Smith MF, Rothwangl J. Are guidelines following guide-lines? The methodological quality of clinical practice guidelines in the peer-reviewed medical literature.JAMA.1999;281:1900 –1905
Context. Practice guidelines play an important role in medicine. Methodolog-ical principles have been formulated to guide their development.
Objective. To determine whether practice guidelines in peer-reviewed medical literature adhered to established methodological standards for practice guidelines. Design. Structured review of guidelines published from 1985 through June 1997 identified by a MEDLINE search.
Main Outcome Measures. Mean number of standards met based on a 25-item instrument and frequency of adherence.
Conclusion. Guidelines published in the peer-reviewed medical literature dur-ing the past decade do not adhere well to established methodological standards. While all areas of guideline development need improvement, greatest improve-ment is needed in the identification, evaluation, and synthesis of the scientific evidence.
DOI: 10.1542/peds.106.5.1105
2000;106;1105
Pediatrics
Vision Screening in the Preschool Child
the Maternal and Child Health Bureau and the National Eye Institute Task Force on
of
Graham E. Quinn, Mark S. Ruttum, Paulette P. Schmidt, Kurt Simons and on behalf
E. Eugenie Hartmann, Velma Dobson, Louise Hainline, Wendy Marsh-Tootle,
Preschool Vision Screening: Summary of a Task Force Report
Services
Updated Information &
http://pediatrics.aappublications.org/content/106/5/1105
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/106/5/1105#BIBL
This article cites 25 articles, 7 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/ophthalmology_sub Ophthalmology
http://www.aappublications.org/cgi/collection/agency_abcs Agency ABC's
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.106.5.1105
2000;106;1105
Pediatrics
Vision Screening in the Preschool Child
the Maternal and Child Health Bureau and the National Eye Institute Task Force on
of
Graham E. Quinn, Mark S. Ruttum, Paulette P. Schmidt, Kurt Simons and on behalf
E. Eugenie Hartmann, Velma Dobson, Louise Hainline, Wendy Marsh-Tootle,
Preschool Vision Screening: Summary of a Task Force Report
http://pediatrics.aappublications.org/content/106/5/1105
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.