Children’s Physical Activity and
Depression: A Meta-analysis
Daphne J. Korczak, MD, MSc, a, b Sheri Madigan, PhD, c Marlena Colasanto, MSca
abstract
CONTEXT: Research regarding the protective effects of early physical activity on depression has yielded conflicting results.
OBJECTIVE: Our objective was to synthesize observational studies examining the association of physical activity in childhood and adolescence with depression.
DATA SOURCES: Studies (from 2005 to 2015) were identified by using a comprehensive search strategy.
STUDY SELECTION: The included studies measured physical activity in childhood or adolescence and examined its association with depression.
DATA EXTRACTION: Data were extracted by 2 independent coders. Estimates were examined by using random-effects meta-analysis.
RESULTS: Fifty independent samples (89 894 participants) were included, and the mean effect size was significant (r = –0.14; 95% confidence interval [CI] = –0.19 to –0.10). Moderator analyses revealed stronger effect sizes in studies with cross-sectional versus longitudinal designs (k = 36, r = –0.17; 95% CI = –0.23 to –0.10 vs k = 14, r = –0.07; 95% CI = –0.10 to –0.04); using depression self-report versus interview (k = 46, r = –0.15; 95% CI = –0.20 to –0.10 vs k = 4, r = –0.05; 95% CI = –0.09 to –0.01); using validated versus nonvalidated physical activity measures (k = 29, r = –0.18; 95% CI = –0.26 to –0.09 vs k = 21, r = –0.08; 95% CI = –0.11 to –0.05); and using measures of frequency and intensity of physical activity versus intensity alone (k = 27, r = –0.17; 95% CI = –0.25 to –0.09 vs k = 7, r = –0.05; 95% CI = –0.09 to –0.01).
LIMITATIONS: Limitations included a lack of standardized measures of physical activity; use of self-report of depression in majority of studies; and a small number of longitudinal studies.
CONCLUSIONS: Physical activity is associated with decreased concurrent depressive symptoms; the association with future depressive symptoms is weak.
aDepartment of Psychiatry, Hospital for Sick Children, Toronto, Ontario, Canada; bDepartment of Psychiatry, Faculty of Medicine, University of Toronto, Toronto, Ontario, Canada; and cDepartment of Psychology, Aberta Children's Research Institute, Calgary, Alberta, Canada
Dr Korczak conceptualized and designed the study, assisted in data collection, and drafted the initial manuscript; Dr Madigan assisted in data collection, carried out the initial analyses, contributed to, and reviewed and revised the manuscript; Ms Colasanto coordinated and assisted in data collection and contributed to and critically reviewed the manuscript; and all authors approved the fi nal manuscript as submitted.
DOI: 10.1542/peds.2016-2266 Accepted for publication Jan 6, 2017
Address correspondence to Daphne J. Korczak, MD, MSc, Department of Psychiatry, The Hospital for Sick Children, 555 University Ave, Toronto, ON M5G1X8, Canada. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Research interest in the health and psychological benefits of exercise has grown exponentially over recent years. Evidence suggests that physical activity may ameliorate depressive symptoms, supporting the use of exercise as part of a comprehensive treatment plan for major depressive disorder (MDD). 1, 2
The reverse association has also been demonstrated: decreased physical activity (PA), as well as increased sedentary behaviors, confers vulnerability for developing depressive symptoms. 3–5 To date,
studies have investigated whether increased PA may also protect individuals against the development of MDD, and findings from
observational studies are promising. 3, 6–8 However, the age
range of participants in these studies has been wide, research has been conducted principally in adult populations, and results have been conflicting.9–11 Thus, using the
current state of the literature for the purpose of clinical decision-making is challenging. A meta-analysis is warranted to resolve discrepancies in the literature and to examine the suggestion that the largest magnitude of protective effect may be found at younger ages, 12 which would in
turn provide support for a potential preventative role of physical activity in the development of depression.
Two recent systematic reviews 13, 14
have reported that increased PA is associated with fewer depressive symptoms. However, only 1 review focused on the child and adolescent age group, 13 and neither review
conducted a meta-analytic synthesis of the data, which can provide a powerful estimate of the mean effect size across studies. Compared with adult participants, in which the investigation of risk factors is confounded by years of the allostatic load of depression (exposure to depressive symptoms and their associated physiologic strain) 15
and comorbid cardiometabolic
disease, 16 studies of children and
adolescents enable the examination of the relationship between PA and depressive symptoms at their most nascent. To our knowledge, this is the first study to conduct a meta-analytic review of the protective effect of PA on depression and, as such, is the first to describe the magnitude of this association. Also, previous systematic reviews have not explored the potential moderating role of sex in the association between PA and MDD, although a stronger effect for females has been suggested in several independent studies. 4, 17, 18
Understanding if the association between PA and MDD is sex-specific is relevant for the elucidation of potential underlying mechanisms of association.
The objective of this meta-analysis was to investigate the potential preventative effect of child and adolescent PA on depression. Several variables have been linked to differences in effects size; thus, we will examine whether between-study differences were observed for child age, sex, and social risk. 19–21 We
will also examine if heterogeneity in effect sizes can be explained by variation in study methodology (eg, methods of assessing physical activity and depression), as well as study quality (eg, longitudinal versus cross-sectional). Clarification on the role of these factors for understanding systematic differences in effect sizes are important for the design and implementation of targeted and effective public health prevention programs.
METHODS
Search Strategy
Published studies on PA and depression in children and adolescents were identified by searching Social Sciences Abstracts, International Bibliography of the Social Sciences, Scopus, SportDiscus, CBA Abstracts, Physical Education
Index, Sociological Abstracts, and PsycINFO electronic databases for potential articles through October 2015. The search was limited to English language articles published between 2005 and 2015 using the keywords (“child*, ” or “teen*, ” or “adolesc*, ” or “youth*, ” or “infant, ” or “infancy, ” or “baby, ” or “babies”) AND (“depress*”), AND (“sedentary behavio*” or “recreation” or “physical activity” or “leisure activity” or “exercise” or “fitness” or “sport*”). This search strategy yielded 3147 nonduplicate articles.
Study Inclusion and Exclusion Criteria
Titles and abstracts of the articles were reviewed to identify studies that met the inclusion criteria. Articles selected for the current study were based on the following criteria. (1) Cross-sectional study of PA and depression collected during childhood or adolescence (<18 years). (2) Longitudinal study of PA collected during childhood or adolescence (<18 years); (3) The constructs measured were PA (eg, energy expenditure) and depressive symptoms. Studies that measured broader, nonspecific constructs of either PA (eg, participation in extracurricular activities) or of depression (eg, psychological distress) were excluded. Because numerous standardized, validated and accessible measures of
depression among youth are widely available, studies that assessed the outcome of depression by using a nonvalidated measure were excluded. Only 1 study 22 needed
to be excluded because it assessed depression by using a single self-report item with no demonstrated psychometric properties. In contrast to the depression literature,
examined as a moderator to determine if this measurement characteristic explained between study heterogeneity. (4) The study statistic could be transformed into an effect size (eg, correlations, odds ratios, means/SDs, and/or P values). (5) The full-text article was available and written in English. Studies in which PA was used as an intervention were not included in the current study.
Multiple results often emerge from a single dataset. If the same participants were used across multiple publications, only 1 study was included in the meta-analysis to ensure independence of effect sizes. A protocol was developed so that each sample of participants was only represented once in the meta-analysis. First, if a single dataset presented both cross-sectional and longitudinal analyses, we selected the study with longitudinal data because this study design was underrepresented in our analyses. Second, if multiple publications emerged from a single cross-sectional dataset, we selected the publication with the largest sample size and most comprehensive data extraction information.
Multiple samples or groups often exist within a particular study. For example, some studies present results separately for boys and girls within a sample. In such cases, effects sizes for both these nonoverlapping samples were calculated and entered into the meta-analysis separately.
Data Extraction
All articles that met inclusion criteria were coded by using a standard coding form to collect information on study and sample characteristics. Several moderator variables were collected to explain effect size variability across studies. Moderator variables were divided into categorical moderators (sex, social risk [ie, low income, minority, or involved in child protective
services], PA type, PA validated measure, depression measure type, study design, and country) and continuous moderators (age at PA/depression, time between assessments, and publication year). Some studies reported data stratified by level of PA. In such cases, data for the group with the greatest PA were used in the analysis. This was done to remain consistent with our primary objective. Data extraction was performed by 2 independent coders (DK and MC). Discrepancies were resolved through discussion, and consensus scores were entered into the final dataset.
Data Analysis
Effect sizes were calculated and analyzed by using Comprehensive Meta-Analysis version 3.0
software. 23 Effect sizes were
calculated directly from information provided in each study. When provided, adjusted effect sizes were included. All effect sizes were transformed into correlations for the purpose of reporting mean effect sizes. Pooled effect size estimates were based on random effects model. We assessed for overall heterogeneity of the mean effect size using the
Q statistic and by calculating the
I2 statistic. The Q statistic is a
test of the null hypothesis that all studies share a common effect size, and the I2 statistic examines the proportion of the variation across studies that is due to heterogeneity rather than chance, expressed as a percentage. General guidelines for the interpretation of the I2 are as follows: 25%, 50%, and 75% indicate low, moderate, and high heterogeneity, respectively. 24
Categorical moderator analyses were conducted by using Q statistics, 25, 26 whereas the
significance of each continuous moderator was assessed by using
meta-regressions.27 Finally, we
examined publication bias using funnel plots and Egger’s test.
Study Quality
To assess the quality of studies, a 7-point quality assessment tool was created based on those implemented in previous meta-analyses of observational studies. 28, 29 The tool evaluated
the articles based on the following 7 criteria: (1) having a defined sample, (2) having a representative sample, (3) rater blinding, (4) report of relevant MDD and PA data, (5) adequate sample size, (6) statistical adjustment for covariates, and (7) a validated PA measure. Articles were given a score of 0 (“No”) or 1 (“Yes”) for each of the abovementioned criteria and summed to give a total score out of 7.
RESULTS
Our electronic search of 7 databases yielded 3147 nonduplicate articles. On review of the titles and abstracts, 87 articles met inclusion criteria and full articles were retrieved. A total of 40 studies with 50 independent samples (89 894 participants) met the inclusion criteria and were included in analyses. Figure 1 presents a flowchart of the review process.
Study and Sample Characteristics
Study Characteristics
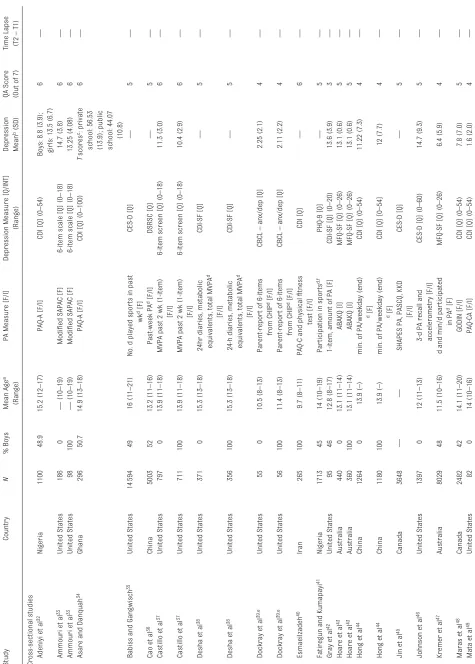
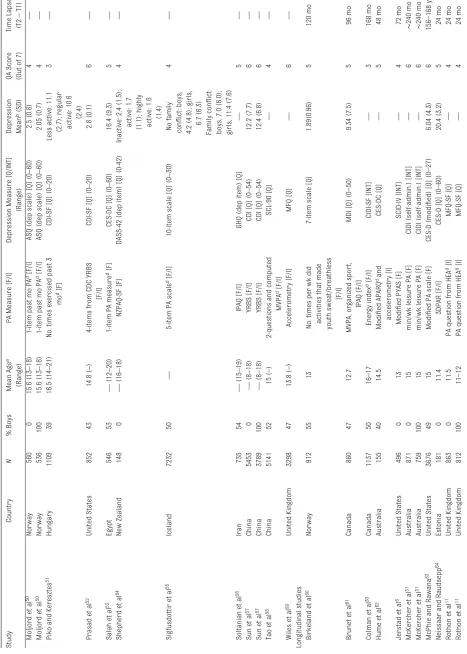
assessment of depression, 4 studies measured depressive symptoms by using interview methodology, whereas 46 studies used self-report questionnaires. The overall burden of depressive symptoms in studies that used a depression self-report measure was low (see Table 1). A clinical diagnosis of MDD was reported at follow-up for the 4 longitudinal samples that measured depressive symptoms by using a standardized interview. An MDD diagnosis was made in 5% to 13% of participants across these studies at follow-up. 6, 30, 31 Although several
studies specifically noted the absence
of antidepressant medication use among participants, the large majority of studies did not include information regarding the use of medications.
Study Quality
Validated measures of PA were used in 19 out of 36 (53%) cross-sectional studies and in 10 out of 14 (71%) longitudinal studies, as indicated in Table 1. The mean study quality score was 4.9 (SD = 0.9) out of 7. For cross-sectional studies, the mean percentage of participants with complete data were 96.6% (range: 68%–100%). For longitudinal studies, the mean
rate of attrition between time points was 13.8% (range: 0.04%–30%). Additional detail regarding individual study- and item-level quality
assessment scoring is summarized in Supplemental Table 6.
Overall Measure of Effect Size
A significant mean effect size for the association between PA and depression was found: (r = –0.14; 95% confidence interval [CI] = –0.19 to –0.10) ( Fig 2), suggesting that children’s PA is negatively associated with depressive symptoms. The funnel plot revealed asymmetry ( Fig 3) and Egger’s test suggested that the asymmetry was significant (P < .01). Using the trim and fill analysis, the adjusted pooled effect size estimate was r = 0.06 (95% CI = –0.11 to –0.01). Statistically significant heterogeneity between the studies was found (Q = 1767.95; P < .0001;
I2 = 95.23) and potential moderator
analyses were explored, including demographic, measurement, and study design factors. The results of all moderator analyses are presented in Tables 2 and 3, and significant moderators are discussed in detail below.
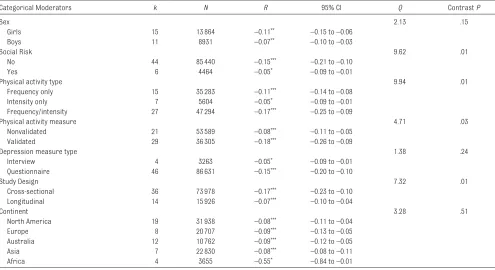
Effect sizes were stronger in samples using cross-sectional designs (k = 36, r = –0.17; 95% CI = –0.23 to –0.10) compared with those using longitudinal designs (k = 14, r = –0.07; 95% CI = –0.10 to –0.04), in which a weak inverse relationship between physical activity and future depressive symptoms was found. Similarly, studies that used interview-based MDD measures demonstrated weaker effect sizes compared with those that used questionnaires (k = 4, r = –0.05; 95% CI = –0.09 to –0.01 vs k = 46, r = –0.15; 95% CI = –0.20 to –0.10). Stronger effect sizes were also observed in samples with no known risks (k = 44; r = –0.15; 95% CI = –0.21 to –0.10) compared with samples with social risk (eg, low income) (k = 6; r = –0.05; 95%
FIGURE 1
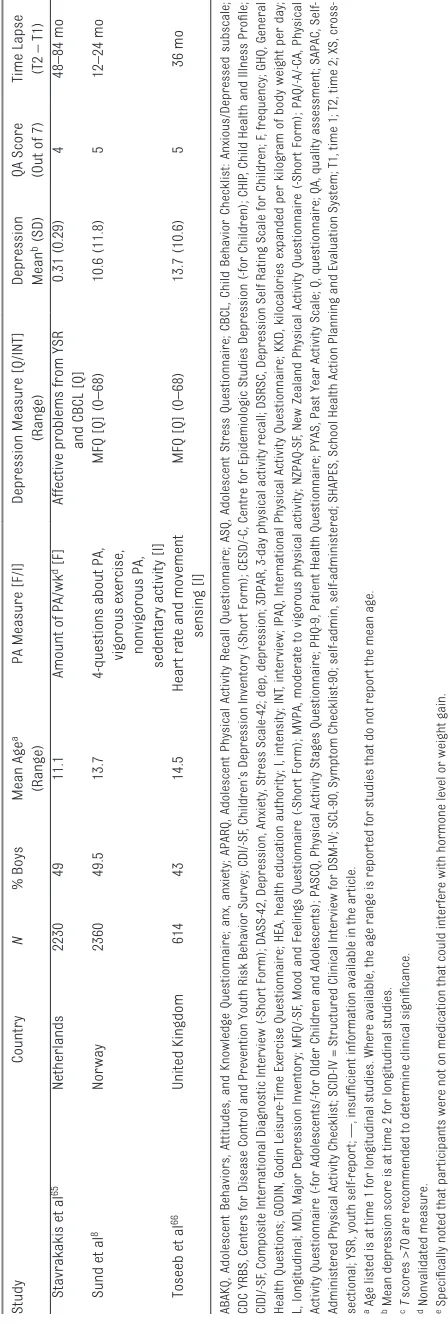
TABLE 1
Independent Samples Included in the Meta-analysis of Physical Activity and Depression
Study Country N % Boys Mean Age a (Range)
PA Measure [F/I]
Depression Measure [Q/INT]
(Range)
Depression Mean
b (SD)
QA Score (Out of 7) Time Lapse (T2 – T1)
Cross-sectional studies Adeniyi et al
32 Nigeria 1100 48.9 15.2 (12–17) PAQ-A [F/I]
CDI [Q] (0–54)
Boys: 8.8 (3.9); girls: 13.5 (6.7)
6—
Ammouri et al
33 United States 186 0 — (10–19) Modifi
ed SAPAC [F]
6-item scale [Q] (0–18)
14.7 (3.8)
6
—
Ammouri et al
33 United States 98 100 — (10–19) Modifi
ed SAPAC [F]
6-item scale [Q] (0–18)
13.25 (4.08)
6
—
Asare and Danquah
34 Ghana 296 50.7 14.9 (13–18) PAQ-A [F/I]
CDI [Q] (0–100)
T
scores
c: private
school: 56.53 (13.9); public school: 44.07
(10.8)
6—
Babiss and Gangwisch
35 United States 14 594 49 16 (11–21)
No. d played spor
ts in past
wk
d [F]
CES-D [Q]
—
5
—
Cao et al
36 China 5003 52 13.2 (11–16) Past-week PA
d [F/I]
DSRSC [Q]
—
5
—
Castillo et al
37
United States
797
0
13.9 (11–18)
MVPA past 2 wk (1-item)
[F/I]
6-item screen [Q] (0–18)
11.3 (3.0)
6
—
Castillo et al
37
United States
711
100
13.9 (11–18)
MVPA past 2 wk (1-item)
[F/I]
6-item screen [Q] (0–18)
10.4 (2.9)
6
—
Desha et al
38
United States
371
0
15.3 (13–18)
24hr diaries, metabolic equivalents, total MVPA
d [F/I] CDI-SF [Q] — 5 —
Desha et al
38
United States
356
100
15.3 (13–18)
24-h diaries, metabolic equivalents, total MVPA
d [F/I] CDI-SF [Q] — 5 —
Dockray et al
39, e United States 55 0 10.5 (8–13) Parent-repor
t of 6-items
from CHIP
d [F/I]
CBCL – anx/dep [Q]
2.25 (2.1)
4
—
Dockray et al
39, e United States 56 100 11.4 (8–13) Parent-repor
t of 6-items
from CHIP
d [F/I]
CBCL – anx/dep [Q]
2.11 (2.2) 4 — Esmaeilzadeh 40 Iran 265 100 9.7 (8–11)
PAQ-C and physical fi
tness test [F/I] CDI [Q] — 6 —
Fatiregun and Kumapayi
41 Nigeria 1713 45 14 (10–19) Par
ticipation in spor
ts d, f PHQ-9 [Q] — 5 —
Gray et al
42
United States
95
46
12.8 (8–17)
1-item, amount of PA [F]
CDI-SF [Q] (0–20)
13.6 (3.9)
3
—
Hoare et al
43 Australia 440 0 13.1 (11–14) ABAKQ [I]
MFQ-SF [Q] (0–26)
13.1 (0.6)
5
—
Hoare et al
43 Australia 360 100 13.1 (11–14) ABAKQ [I]
MFQ-SF [Q] (0–26)
13.1 (0.6)
5
—
Hong et al
44
China
1264
0
13.9 (–)
min. of PA/weekday (end)
d [F]
CDI [Q] (0–54)
11.22 (7.3)
4
—
Hong et al
44
China
1180
100
13.9 (–)
min. of PA/weekday (end)
d [F]
CDI [Q] [0–54]
12 (7.7)
4
—
Jin et al
45
Canada
3648
—
—
SHAPES PA, PASCQ, KKD
[F/I]
CES-D [Q]
—
5
—
Johnson et al
46
United States
1397
0
12 (11–13)
3-d PA recall and accelerometry [F/I]
CES-D [Q] (0–60)
14.7 (9.3)
5
—
Kremer et al
47
Australia
8029
48
11.5 (10–16)
d and min/d par
ticipated
in PA
d [F]
MFQ-SF [Q] (0–26)
6.4 (5.9)
4
—
Maras et al
48 Canada 2482 42 14.1 (11–20) GODIN [F/I]
CDI [Q] (0–54)
7.8 (7.0)
5
—
Mata et al
49 United States 82 0 14 (10–16) PAQ-CA [F/I]
CDI [Q] (0–54)
1.6 (2.0)
4
Study Country N % Boys Mean Age a (Range)
PA Measure [F/I]
Depression Measure [Q/INT]
(Range)
Depression Mean
b (SD)
QA Score (Out of 7) Time Lapse (T2 – T1)
Moljord et al
50 Nor way 560 0 15.6 (13–18)
1-item past mo PA
d [F/I]
ASQ (dep scale) [Q] (0–60)
2.5 (0.8)
4
—
Moljord et al
50 Nor way 536 100 15.6 (13–18)
1-item past mo PA
d [F/I]
ASQ (dep scale) [Q] (0–60)
2.05 (0.7)
4
—
Piko and Keresztes
51
Hungary
1109
39
16.5 (14–21)
No. times exercised past 3
mo
d [F]
CDI-SF [Q] (0–20)
Less active: 11.1 (2.7); regular
active: 10.6
(2.4)
3—
Prasad et al
52
United States
852
43
14.8 (–)
4-items from CDC YRBS
[F/I]
CDI-SF [Q] (0–20)
2.8 (0.1)
6
—
Salah et al
53
Egypt
546
53
— (12–20)
1-item PA measure
d [F]
CES-DC [Q] (0–60)
16.4 (9.3)
5
—
Shepherd et al
54 New Zealand 148 0 — (16–18) NZPAQ-SF [F]
DASS-42 (dep item) [Q] (0-42)
Inactive: 2.4 (1.5);
active: 1.7 (1.1); highly active: 1.6 (1.4)
4—
Sigfusdottir et al
55
Iceland
7232
50
—
5-item PA scale
d [F/I]
10-item scale [Q] (0–30)
No family confl
ict:
boys,
4.2 (4.8); girls,
6.7 (6.3).
Family confl
ict:
boys, 7.0 (6.0); girls, 11.4 (7.6)
4—
Soltanian et al
56 Iran 735 54 — (15–19) IPAQ [F/I]
GHQ (dep item) [Q]
—
5
—
Sun et al
57 China 5453 0 — (8–18) YRBS [F/I]
CDI [Q] (0–54)
12.2 (7.7)
6
—
Sun et al
57 China 3789 100 — (8–18) YRBS [F/I]
CDI [Q] (0–54)
12.4 (6.8)
6
—
Tao et al
58
China
5141
52
15 (–)
2-questions and computed
MVPA
d [F/I]
SCL-90 [Q]
—
4
—
Wiles et al
59 United Kingdom 3298 47 13.8 (–) Accelerometry [F/I] MFQ [Q] — 6 —
Longitudinal studies Birkeland et al
60 Nor way 912 55 13
No. times per wk did activities that made youth sweat/breathless
[F/I]
7-item scale [Q]
1.89(0.96)
5
120 mo
Brunet et al
61 Canada 860 47 12.7 MVPA, or ganized spor t, IPAQ [F/I]
MDI [Q] (0–50)
9.34 (7.5)
5
96 mo
Colman et al
30 Canada 1137 50 16–17 Ener gy index
d [F/I]
CIDI-SF [INT]
—
3
168 mo
Hume et al
62 Australia 155 40 14.5 Modifi ed APARQ
d and
accelerometry [I]
CES-DC [Q]
—
5
48 mo
Jerstad et al
6 United States 496 0 13 Modifi
ed PYAS [F]
SCID-IV [INT]
—
4
72 mo
McKercher et al
31
Australia
871
0
15
min/wk leisure PA [F]
CIDI (self-admin.) [INT]
—
6
∼
240 mo
McKercher et al
31
Australia
759
100
15
min/wk leisure PA [F]
CIDI (self-admin.) [INT]
—
6
∼
240 mo
McPhie and Rawana
63 United States 3676 49 15 Modifi
ed PA scale [F]
CES-D (modifi
ed) [Q] (0–27)
6.04 (4.3)
6
156–168 y
Neissaar and Raudsepp
64 Estonia 181 0 11.4 3DPAR [F/I]
CES-D [Q] (0–60)
20.4 (3.2)
5
24 mo
Rothon et al
11
United Kingdom
863
0
11.5
PA question from HEA
d [I]
MFQ-SF [Q]
—
4
24 mo
Rothon et al
11
United Kingdom
812
100
11–12
PA question from HEA
d [I]
CI = –0.09 to –0.01). Effect sizes were stronger in samples examining a combination of PA frequency and intensity (k = 27; r = –0.17; 95% CI = –0.25 to –0.09) compared with intensity alone (k = 7; r = –0.05; 95% CI = –0.09 to –0.01). Finally, stronger effect sizes were found in studies that used validated (k = 29,
r = –0.18; 95% CI = –0.26 to –0.09) versus nonvalidated PA measures (k = 21, r = –0.08; 95% CI = –0.11 to –0.05).
Longitudinal Studies
Because there were significant differences in effect sizes between cross-sectional and longitudinal studies, and because longitudinal associations may provide insight into the directionality of associations, we performed a set of subanalyses with longitudinal studies only to more explicitly examine the magnitude of the association, as well as the between-study variability, for studies assessing a baseline metric of physical activity and its association with later depressive symptoms. There were 14 studies involving 15 926 participants that reported on longitudinal associations between PA and depression. Five studies 6, 8, 30, 64, 66 reported on
depression-related covariates, including baseline depressive symptoms, number of weeks depressed during the preceding year, body dissatisfaction, social support, self-efficacy, history of childhood trauma or stressful life events, and medication status ( Table 1).
The mean effect size for the
longitudinal association between PA and depression was r = –0.07 (95% CI = –0.10 to –0.04). Statistically significant heterogeneity between studies was found (Q = 59.25;
P < .0001; I2 = 77.52) and potential moderator analyses were explored ( Tables 4 and 5). However, because
Study
Country
N
% Boys
Mean Age
a
(Range)
PA Measure [F/I]
Depression Measure [Q/INT]
(Range)
Depression Mean
b (SD)
QA Score (Out of 7) Time Lapse (T2 – T1)
Stavrakakis et al
65
Netherlands
2230
49
11.1
Amount of PA/wk
d [F]
Affective problems from YSR
and CBCL [Q]
0.31 (0.29)
4
48–84 mo
Sund et al
8
Nor
way
2360
49.5
13.7
4-questions about PA,
vigorous exercise, nonvigorous PA, sedentary activity [I]
MFQ [Q] (0–68)
10.6 (11.8)
5
12–24 mo
Toseeb et al
66
United Kingdom
614
43
14.5
Hear
t rate and movement
sensing [I]
MFQ [Q] (0–68)
13.7 (10.6)
5
36 mo
ABAKQ, Adolescent Behaviors, Attitudes, and Knowledge Questionnaire; anx, anxiety; APARQ, Adolescent Physical Activity Recall Q
uestionnaire; ASQ, Adolescent Stress Questionnaire; CBCL, Child Behavior Checklist: Anxious/Depressed subscale;
CDC YRBS, Centers for Disease Control and Prevention Youth Risk Behavior Sur
vey; CDI/-SF
, Children’s Depression Inventory (-Sho
rt Form); CESD/-C, Centre for Epidemiologic Studies Depression (-for Children); CHIP
, Child Health and Illness Profi
le;
CIDI/-SF
, Composite International Diagnostic Inter
view (-Shor
t Form); DASS-42, Depression, Anxiety, Stress Scale-42; dep, depre
ssion; 3DPAR, 3-day physical activity recall; DSRSC, Depression Self Rating Scale for Children; F
, frequency; GHQ, General
Health Questions; GODIN, Godin Leisure-Time Exercise Questionnaire; HEA, health education authority; I, intensity; INT
, inter
vi
ew; IPAQ, International Physical Activity Questionnaire; KKD, kilocalories expanded per kilogram of body weight per day;
L, longitudinal; MDI, Major Depression Inventory; MFQ/-SF
, Mood and Feelings Questionnaire (-Shor
t Form); MVPA, moderate to vig
orous physical activity; NZPAQ-SF
, New Zealand Physical Activity Questionnaire (-Shor
t Form); PAQ/-A/-CA, Physical
Activity Questionnaire (-for Adolescents/-for Older Children and Adolescents); PASCQ, Physical Activity Stages Questionnaire; P
HQ-9, Patient Health Questionnaire; PYAS, Past Year Activity Scale; Q, questionnaire; QA, quality assessment; SAPAC,
Self-Administered Physical Activity Checklist; SCID-IV = Structured Clinical Inter
view for DSM-IV
; SCL-90, Symptom Checklist-90; sel
f-admin, self-administered; SHAPES, School Health Action Planning and Evaluation System; T1, time 1; T2, time 2; XS,
cross-sectional; YSR, youth self-repor
t; —, insuffi
cient information available in the ar
ticle.
a Age listed is at time 1 for longitudinal studies. Where available, the age range is repor
ted for studies that do not repor
t th
e mean age.
b Mean depression score is at time 2 for longitudinal studies. cT
scores >70 are recommended to determine clinical signifi
cance.
d Nonvalidated measure. e Specifi
cally noted that par
ticipants were not on medication that could interfere with hormone level or weight gain.
f Not specifi
ed; asked about par
ticipation in spor
ting activities.
TABLE 1
the number of studies for several subgroups was small (eg, there were only 2 studies with social risk), the results of these moderator analyses should be interpreted with caution ( Table 5).
DISCUSSION
This systematic review and meta-analysis of 50 samples involving 89 894 participants found that a greater PA level was associated
with fewer depressive symptoms, although not with decreased diagnoses of MDD. This association was stronger for cross-sectional studies than for longitudinal studies, in which the mean effect size was
FIGURE 2
significant, but weak. The nature of the PA was also associated with the presence of depressive symptoms, in that PA of increased frequency and intensity was more strongly associated with decreased depressive symptoms compared with PA that was defined by intensity of activity alone.
Significant effect sizes were observed for studies that examined depressive symptomatology by using questionnaire measures and were considerably stronger than those of studies assessing MDD by using interview measures. Indeed, the majority of studies in this meta-analysis employed self-report inventories to assess depressive symptoms (n = 46) rather than diagnostic interviews (n = 4), which are considered to be the gold-standard measure for MDD. Self-report measures are frequently used in research studies due to their ease of administration, low cost,
minimal time requirement, and low patient response burden. These measures are useful screening tools; however, self-report instruments are limited by their inability to
confirm the presence or absence of an MDD diagnosis. That increased PA was more highly associated with decreased depressive symptoms in this meta-analysis, as compared
FIGURE 3
Funnel plot of the meta-analysis of included studies. The y-axis on the funnel plot represents the SE, and the x-axis is the effect size. Observed studies are indicated by open circles. The white diamond represents the observed mean effect size, and the black diamond represents the adjusted mean effect size.
TABLE 2 Examination of Potential Effect Modifi ers in the Association of Physical Activity and Depression: Categorical Variables
Categorical Moderators k N R 95% CI Q Contrast P
Sex 2.13 .15
Girls 15 13 864 –0.11** –0.15 to –0.06
Boys 11 8931 –0.07** –0.10 to –0.03
Social Risk 9.62 .01
No 44 85 440 –0.15*** –0.21 to –0.10
Yes 6 4464 –0.05* –0.09 to –0.01
Physical activity type 9.94 .01
Frequency only 15 35 283 –0.11*** –0.14 to –0.08
Intensity only 7 5604 –0.05* –0.09 to –0.01
Frequency/intensity 27 47 294 –0.17*** –0.25 to –0.09
Physical activity measure 4.71 .03
Nonvalidated 21 53 589 –0.08*** –0.11 to –0.05
Validated 29 36 305 –0.18*** –0.26 to –0.09
Depression measure type 1.38 .24
Interview 4 3263 –0.05* –0.09 to –0.01
Questionnaire 46 86 631 –0.15*** –0.20 to –0.10
Study Design 7.32 .01
Cross-sectional 36 73 978 –0.17*** –0.23 to –0.10
Longitudinal 14 15 926 –0.07*** –0.10 to –0.04
Continent 3.28 .51
North America 19 31 938 –0.08*** –0.11 to –0.04
Europe 8 20 707 –0.09*** –0.13 to –0.05
Australia 12 10 762 –0.09*** –0.12 to –0.05
Asia 7 22 830 –0.08*** –0.08 to –0.11
Africa 4 3655 –0.55* –0.84 to –0.01
with an MDD diagnosis, is a critical finding. This finding suggests that individuals who are at risk for more severe, syndromal-level symptom burden, impairment, and associated poor health outcomes may not respond to the potential preventative effects of PA. Although it is possible that these results may also reflect the relative methodological limitations associated with the examination of a dichotomous versus a continuous variable, our findings are consistent with previous data reporting that MDD severity is distinguished from subsyndromal depressive symptoms
by its decreased sensitivity to prevention strategies, greater association with cardiovascular risk factors and health outcomes, and greater treatment resistance. 67 –70
Increased PA was more strongly associated with decreased depressive symptoms in cross-sectional studies compared with longitudinal studies, where the effect size was small. Cross-sectional studies are limited in their ability to probe causality, because the temporal relationship between variables cannot be determined. Thus, it is possible
that the cross-sectional studies included in this meta-analysis are actually indicative of the reverse association of PA and depression: that children and adolescents with increased depressive symptoms are less likely to participate in PA. Indeed, amotivation, pessimism, and anhedonia associated with the depressed state have been reported to lead to decreased PA among adult populations. 71 In contrast,
longitudinal studies provide insight into the direction of the association and, in the present meta-analysis, demonstrated a weak inverse TABLE 3 Examination of Potential Effect Modifi ers in the Association of Physical Activity and Depression: Continuous Variables
Continuous Moderators k N Slope SE z Score P
Age at PA assessment 50 89 894 –0.009 0.014 −0.65 .52
Age at depression assessment 50 89 894 0.005 0.005 1.03 .30
Time between assessments 50 89 894 0.008 0.003 1.46 .15
Publication year 50 89 894 0.002 0.009 0.17 .87
TABLE 4 Examination of Potential Categorical Effect Modifi ers in Studies With Longitudinal Associations Between Physical Activity and Depression
Categorical Moderators k N R 95% CI Q Contrast P
Sex 1.16 .28
Girls 4 812 –0.10* –0.20 to –0.00
Boys 2 2411 –0.03 –0.11 to –0.04
Social Risk 12.13 .0001
No 12 14 251 –0.09*** –0.12 to –0.05
Yes 2 1675 –0.01 –0.03 to 0.01
Physical activity type 2.44 .30
Frequency only 5 8032 –0.06** –0.08 to –0.03
Intensity only 5 3090 –0.04+ –0.09 to 0.01
Frequency/intensity 4 4804 –0.14* –0.25 to –0.02
Physical activity measure 11.66 .01
Nonvalidated 4 5042 –0.01+ –0.03 to 0.00
Validated 10 10 884 –0.10*** –0.14 to –0.05
Depression measure type 1.12 .29
Interview 4 3263 –0.05* –0.09 to –0.01
Questionnaire 10 12 663 –0.08*** –0.12 to –0.04
Continent 1.31 .52
North America 4 6169 –0.06*** –0.08 to –0.03
Europe 7 7972 –0.09** –0.15 to –0.04
Australia 3 1785 –0.05* –0.10 to –0.01
+ P < .10. * P < .05. ** P < .01. *** P < .001.
TABLE 5 Examination of Continuous Moderators in Studies With Longitudinal Associations Between Physical Activity and Depression
Continuous Moderators k N Slope SE z Score P
Age at physical activity 14 15 926 0.004 0.009 0.45 .66
Age at depression 14 15 926 0.001 0.002 0.47 .64
Time between assessments 14 15 926 0.001 0.003 0.45 .65
relationship between PA and future depressive symptoms measured 2 to 17 years later, suggesting that PA has a weak but positive association with future mood.
Studies that included a measure of both increased PA frequency and intensity demonstrated stronger associations with depressive symptoms than those that used measures of intensity alone. This finding is consistent with other systematic reviews examining the role of PA as an intervention for depressed adults. 1 Currently, some
clinical guidelines recommend the inclusion of 45 minutes of moderately intense exercise at least 3 days per week in the treatment of MDD among adults. 72
In contrast, guidelines for general health promotion by the Canadian Pediatric Society 73 and American
Academy of Pediatrics 74 recommend
that children and adolescents get at least 60 minutes of moderate to vigorous PA daily to maintain general health. As such, the findings from the current study support the inclusion of both the PA frequency and intensity components in the Canadian Pediatric Society and American Academy of Pediatrics recommendations with respect to the benefit to depressed mood. Many hypotheses regarding the mechanism by which PA may lead to improved mood have been theorized, including via antiinflammatory effects, increased growth factors leading to neural plasticity, neuroendocrine effects on the hypothalamic-pituitary-adrenal axis and insulin sensitivity, and improvements in
self-efficacy.75–77 However, neither
the pathophysiological pathways themselves nor whether they are specific to mood state are known. These factors are important for determining rational prevention versus treatment strategies, gaining insight into the etiology of depression, and for research into
novel treatments for depression for medically ill populations and those unable to participate in PA.
Studies that examined the association of PA with depression in samples of higher social risk (eg, low income, minority, or involved in child protective services) reported weaker effect sizes than those of lower-risk groups. Socioeconomic status and its associated risk factors (eg, disadvantaged neighborhoods) explain a significant proportion of the variance in childhood psychopathology, including depression. 78 Because children
in high–social risk environments may be exposed to many more risk factors for depression, including lower socioeconomic status, 79 increased PA may have
relatively less influence with respect to the proportion of the variance in depression it explains when compared with children of lower social risk. 80 Also, because
measures of depression and PA have traditionally been developed in samples of low social risk, they may be less well calibrated to capture the variation in depression or PA seen in high–social risk children. 81, 82 These results should
be interpreted with caution, however, because few studies have examined the association of PA with depression in high–social risk samples. Given the increased prevalence of both depression and obesity in populations of high social risk, however, additional research examining potential targets for prevention among this vulnerable group of children is needed.
As the first study to conduct a meta-analytic review of the potential protective association of childhood PA with depression, this study has many strengths, including the analysis of a large number of studies to increase the precision of effect size estimates, subanalysis of cross-sectional versus longitudinal associations, and examination
of PA frequency and intensity as potentially contributing effect modifiers. However, our findings must be interpreted within the context of the limitations of this study. The measurement of PA in the majority of studies relied on self-report measures of frequency, intensity, and type of activity, which were not correlated with objective measures of activity (eg, accelerometry). This also reflects a limitation of the PA literature more broadly, in that the use of standardized instruments that have demonstrated reliability and validity was not consistent across studies. The current meta-analysis demonstrated that studies with validated measures of PA had stronger effect sizes than those that used nonvalidated measures. Thus, future PA research should focus on the methodology for PA measurement in children and adolescents to increase confidence in the study results. In addition, the majority of the literature relies on the self-report of depressive symptoms, with few studies able to confirm a diagnosis of depression, leading to wide precision estimates of the magnitude of the effect of PA on clinical depression. Finally, we only included studies that were published in English, and this inclusion criterion may limit the generalizability of our findings to predominantly English-speaking countries.
CONCLUSIONS
depressive symptoms; and (3) depression measure, with a stronger protective effect of increased PA for depressive symptoms than for a clinical diagnosis of MDD. Taken together, this study suggests that PA in childhood and adolescence is associated with improved concurrent symptoms of depression, particularly when undertaken regularly and with vigor, and has weak but significant
effects on future depressive symptoms. Future research is needed to advance the knowledge of PA measurement, elucidate the mechanism of association between PA and depression, and examine the longitudinal relationships between PA, depression, and health outcomes to determine the critical periods in which preventative efforts may be most effective.
ACKNOWLEDGMENT
We thank Ms Qi Fang (University of Toronto) for assistance in the literature search.
ABBREVIATIONS
CI: confidence interval
MDD: major depressive disorder PA: physical activity
Copyright © 2017 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no fi nancial relationships relevant to this article to disclose.
FUNDING: Research support was provided to Dr Madigan by the Alberta Children’s Hospital Foundation and the Canada Research Chairs program. POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential confl icts of interest to disclose.
REFERENCES
1. Cooney GM, Dwan K, Greig CA, et al. Exercise for depression. Cochrane Database Syst Rev. 2013;(9):CD004366 2. Nyström MB, Neely G, Hassmén P,
Carlbring P. Treating major depression with physical activity: a systematic overview with recommendations. Cogn Behav Ther. 2015;44(4):341–352 3. Åberg MA, Waern M, Nyberg J, et al.
Cardiovascular fi tness in males at age 18 and risk of serious depression in adulthood: Swedish prospective population-based study. Br J Psychiatry. 2012;201(5):352–359 4. Carroll DD, Blanck HM, Serdula MK,
Brown DR. Obesity, physical activity, and depressive symptoms in a cohort of adults aged 51 to 61. J Aging Health. 2010;22(3):384–398
5. Hamer M, Molloy GJ, de Oliveira C, Demakakos P. Leisure time physical activity, risk of depressive symptoms, and infl ammatory mediators: the English Longitudinal Study of Ageing. Psychoneuroendocrinology. 2009;34(7):1050–1055
6. Jerstad SJ, Boutelle KN, Ness KK, Stice E. Prospective reciprocal relations between physical activity and depression in female adolescents. J Consult Clin Psychol. 2010;78(2):268–272
7. Strawbridge WJ, Deleger S, Roberts RE, Kaplan GA. Physical activity reduces
the risk of subsequent depression for older adults. Am J Epidemiol. 2002;156(4):328–334
8. Sund AM, Larsson B, Wichstrøm L. Role of physical and sedentary activities in the development of depressive symptoms in early adolescence.
Soc Psychiatry Psychiatr Epidemiol. 2011;46(5):431–441
9. Cooper-Patrick L, Ford DE, Mead LA, Chang PP, Klag MJ. Exercise and depression in midlife: a
prospective study. Am J Public Health. 1997;87(4):670–673
10. Kritz-Silverstein D, Barrett-Connor E, Corbeau C. Cross-sectional and prospective study of exercise and depressed mood in the elderly: the Rancho Bernardo study. Am J Epidemiol. 2001;153(6):596–603 11. Rothon C, Edwards P, Bhui K, Viner
RM, Taylor S, Stansfeld SA. Physical activity and depressive symptoms in adolescents: a prospective study.
BMC Med. 2010;8:32
12. Pinto Pereira SM, Geoffroy MC, Power C. Depressive symptoms and physical activity during 3 decades in adult life: bidirectional associations in a prospective cohort study. JAMA Psychiatry. 2014;71(12):1373–1380 13. Bursnall P. The relationship between
physical activity and depressive symptoms in adolescents: a systematic
review. Worldviews Evid Based Nurs. 2014;11(6):376–382 14. Mammen G, Faulkner G. Physical
activity and the prevention of depression: a systematic review of prospective studies. Am J Prev Med. 2013;45(5):649–657
15. Kobrosly RW, van Wijngaarden E, Seplaki CL, Cory-Slechta DA, Moynihan J. Depressive symptoms are associated with allostatic load among community-dwelling older adults.
Physiol Behav. 2014;123:223–230 16. Vaccarino V, McClure C, Johnson
BD, et al. Depression, the metabolic syndrome and cardiovascular risk.
Psychosom Med. 2008;70(1):40–48 17. Mikkelsen SS, Tolstrup JS, Flachs EM,
Mortensen EL, Schnohr P, Flensborg-Madsen T. A cohort study of leisure time physical activity and depression.
Prev Med. 2010;51(6):471–475 18. Wang F, DesMeules M, Luo W, Dai S,
Lagace C, Morrison H. Leisure-time physical activity and marital status in relation to depression between men and women: A prospective study.
Health Psychol. 2011;30(2):204–211 19. Matsudo VK, Ferrari GL, Araújo TL,
20. Ritterman Weintraub ML, Fernald LC, Goodman E, Guendelman S, Adler NE. Obesity-related behaviors among poor adolescents and young adults: is social position associated with risk behaviors? Front Public Health. 2015;3:224
21. Villagran Perez S, Novalbos-Ruiz JP, Rodriguez-Martin A, Martinez-Nieto M, Lechuga-Sancho AM. Implications of family socioeconomic level on risk behaviors in child-youth obesity. Nutr Hosp. 2013;28(6):1951–1960
22. Eassa S, Hagag SA, Seliem HAEW, Amar HA. Assessment of sport practice among adolescent school students and its effect on perceived health in Sharkia Governorate–Egypt. J Am Sci. 2011;7(3):544–551
23. Borenstein M, Hedges LV, Higgins JP, Rothstein HR. Comprehensive Meta-analysis [computer program]. Version 3. Englewood, NJ: Biostat; 2014
24. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring
inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560
25. Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta-Analysis. West Sussex, United Kingdom: John Wiley & Sons; 2009
26. Rosenthal R. Writing meta-analytic reviews. Psychol Bull. 1995;118(2):183–192
27. Thompson SG, Higgins JPT. How should meta-regression analyses be undertaken and interpreted? Stat Med. 2002;21(11):1559–1573
28. Sanderson S, Tatt ID, Higgins JP. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: a systematic review and annotated bibliography. Int
J Epidemiol. 2007;36(3):666–676 29. Tsang TW, Lucas BR, Carmichael
Olson H, Pinto RZ, Elliott EJ. Prenatal alcohol exposure, FASD, and child behavior: a meta-analysis. Pediatrics. 2016;137(3):e20152542
30. Colman I, Zeng Y, McMartin SE, et al. Protective factors against depression during the transition from adolescence to adulthood: fi ndings from a
national Canadian cohort. Prev Med. 2014;65:28–32
31. McKercher C, Sanderson K, Schmidt MD, et al. Physical activity patterns and risk of depression in young adulthood: a 20-year cohort study since childhood.
Soc Psychiatry Psychiatr Epidemiol. 2014;49(11):1823–1834
32. Adeniyi AF, Okafor NC, Adeniyi CY. Depression and physical activity in a sample of Nigerian adolescents: levels, relationships and predictors.
Child Adolesc Psychiatry Ment Health. 2011;5:16
33. Ammouri AA, Kaur H, Neuberger GB, Gajewski B, Choi WS. Correlates of exercise participation in adolescents.
Public Health Nurs. 2007;24(2):111–120 34. Asare M, Danquah SA. The relationship between physical activity, sedentary behaviour and mental health in Ghanaian adolescents. Child Adolesc Psychiatry Ment Health. 2015;9:11 35. Babiss LA, Gangwisch JE. Sports
participation as a protective factor against depression and suicidal ideation in adolescents as mediated by self-esteem and social support. J Dev Behav Pediatr. 2009;30(5):376–384 36. Cao H, Qian Q, Weng T, et al. Screen
time, physical activity and mental health among urban adolescents in China. Prev Med. 2011;53(4–5):316–320 37. Castillo F, Francis L, Wylie-Rosett
J, Isasi CR. Depressive symptoms are associated with excess weight and unhealthier lifestyle behaviors in urban adolescents. Child Obes. 2014;10(5):400–407
38. Desha LN, Ziviani JM, Nicholson JM, Martin G, Darnell RE. Physical activity and depressive symptoms in American adolescents. J Sport Exerc Psychol. 2007;29(4):534–543
39. Dockray S, Susman EJ, Dorn LD. Depression, cortisol reactivity, and obesity in childhood and adolescence.
J Adolesc Health. 2009;45(4):344–350 40. Esmaeilzadeh S. Relationship between
depressive symptoms with physical activity and physical fi tness among children. Mental Health & Prevention. 2014;2(1–2):11–17
41. Fatiregun AA, Kumapayi TE. Prevalence and correlates of depressive symptoms among in-school adolescents in a rural district
in southwest Nigeria. J Adolesc. 2014;37(2):197–203
42. Gray WN, Janicke DM, Ingerski LM, Silverstein JH. The impact of peer victimization, parent distress and child depression on barrier formation and physical activity in overweight youth.
J Dev Behav Pediatr. 2008;29(1):26–33 43. Hoare E, Millar L, Fuller-Tyszkiewicz M,
et al. Associations between obesogenic risk and depressive symptomatology in Australian adolescents: a cross-sectional study. J Epidemiol Community Health. 2014;68(8):767–772 44. Hong X, Li J, Xu F, et al. Physical
activity inversely associated with the presence of depression among urban adolescents in regional China. BMC Public Health. 2009;9:148
45. Jin S, Muhajarine N, Cushon J, Lim HJ. Factors associated with childhood depression in Saskatoon students: a multilevel analysis. Can J Commun Ment Health. 2013;32(1):29–42 46. Johnson CC, Murray DM, Elder JP, et
al. Depressive symptoms and physical activity in adolescent girls. Med Sci Sports Exerc. 2008;40(5):818–826 47. Kremer P, Elshaug C, Leslie E,
Toumbourou JW, Patton GC, Williams J. Physical activity, leisure-time screen use and depression among children and young adolescents. J Sci Med Sport. 2014;17(2):183–187 48. Maras D, Flament MF, Murray M, et
al. Screen time is associated with depression and anxiety in Canadian youth. Prev Med. 2015;73:133–138 49. Mata J, Thompson RJ, Gotlib IH. BDNF
genotype moderates the relation between physical activity and depressive symptoms. Health Psychol. 2010;29(2):130–133
50. Moljord IEO, Moksnes UK, Espnes GA, Hjemdal O, Eriksen L. Physical activity, resilience, and depressive symptoms in adolescence. Ment Health Phys Act. 2014;7(2):79–85
51. Piko BF, Keresztes N. Physical activity, psychosocial health, and life goals among youth. J Community Health. 2006;31(2):136–145
adolescents. N Am J Psychol. 2009;11(1):173–188
53. Salah EM, Yamamah GA, Megahed HS, Salem SE, El-din S, Khalifa AG. Screening for depressive symptoms and their associated risk factors in adolescent students in South Sinai, Egypt. Life Sci J. 2013;10(3):433–443 54. Shepherd D, Krägeloh C, Ryan C,
Schofi eld G. Psychological well-being, self-reported physical activity levels, and attitudes to physical activity in a sample of New Zealand adolescent females.
Psychology (Irvine). 2012;3(6):447–453 55. Sigfusdottir ID, Asgeirsdottir BB,
Sigurdsson JF, Gudjonsson GH. Physical activity buffers the effects of family confl ict on depressed mood: a study on adolescent girls and boys. J Adolesc. 2011;34(5):895–902
56. Soltanian AR, Nabipour I, Akhondzadeh S, et al. Association between physical activity and mental health among high-school adolescents in Boushehr province: A population based study.
Iran J Psychiatry. 2011;6(3):112–116 57. Sun Y, An J, Wang X, Zu P, Tao FB.
Gender- and puberty-dependent association between physical activity and depressive symptoms: national survey among Chinese adolescents. J Phys Act Health. 2014;11(7):1430–1437 58. Tao FB, Xu ML, Kim SD, Sun Y, Su PY,
Huang K. Physical activity might not be the protective factor for health risk behaviours and psychopathological symptoms in adolescents. J Paediatr Child Health. 2007;43(11):762–767 59. Wiles NJ, Haase AM, Lawlor DA, Ness
A, Lewis G. Physical activity and depression in adolescents: cross-sectional fi ndings from the ALSPAC cohort. Soc Psychiatry Psychiatr Epidemiol. 2012;47(7):1023–1033 60. Birkeland MS, Torsheim TR, Wold B. A
longitudinal study of the relationship between leisure-time physical activity and depressed mood among adolescents. Psychol Sport Exerc. 2009;10(1):25–34
61. Brunet J, Sabiston CM, Chaiton M, et al. The association between past and current physical activity and depressive symptoms in young adults: a 10-year prospective study. Ann Epidemiol. 2013;23(1):25–30
62. Hume C, Timperio A, Veitch J, Salmon J, Crawford D, Ball K. Physical activity, sedentary behavior, and depressive symptoms among adolescents. J Phys Act Health. 2011;8(2):152–156 63. McPhie ML, Rawana JS. The effect
of physical activity on depression in adolescence and emerging adulthood: a growth-curve analysis. J Adolesc. 2015;40:83–92
64. Neissaar I, Raudsepp L. Changes in physical activity, self-effi cacy and depressive symptoms in adolescent girls. Pediatr Exerc Sci. 2011;23(3):331–343
65. Stavrakakis N, de Jonge P, Ormel J, Oldehinkel AJ. Bidirectional prospective associations between physical activity and depressive symptoms. The TRAILS Study. J Adolesc Health. 2012;50(5):503–508
66. Toseeb U, Brage S, Corder K, et al. Exercise and depressive symptoms in adolescents: a longitudinal cohort study.
JAMA Pediatr. 2014;168(12):1093–1100 67. Almas A, Forsell Y, Iqbal R, Janszky
I, Moller J. Severity of depression, anxious distress and the risk of cardiovascular disease in a Swedish population-based cohort. PLoS One. 2015;10(10):e0140742
68. Balestri M, Calati R, Souery D, et al. Socio-demographic and clinical predictors of treatment resistant depression: a prospective European multicenter study. J Affect Disord. 2016;189:224–232
69. Lasserre AM, Marti-Soler H, Strippoli MP, et al. Clinical and course characteristics of depression and all-cause mortality: a prospective population-based study. J Affect Disord. 2016;189:17–24
70. Trivedi MH, Morris DW, Wisniewski SR, et al. Increase in work
productivity of depressed individuals with improvement in depressive symptom severity. Am J Psychiatry. 2013;170(6):633–641
71. Roshanaei-Moghaddam B, Katon WJ, Russo J. The longitudinal effects of depression on physical activity. Gen Hosp Psychiatry. 2009;31(4):306–315 72. National Collaborating Centre for
Mental Health. The Treatment and Management of Depression in Adults
(Updated Edition): National Clinical Practice Guideline 90. London, United Kingdom: National Institute for Health & Clinical Excellence; 2010
73. Canadian Paediatric Society & Healthy Active Living Committee. Healthy active living for children and youth. Paediatr Child Health. 2002;7(5):339–358 74. Council on Sports Medicine and Fitness;
Council on School Health. Active healthy living: prevention of childhood obesity through increased physical activity.
Pediatrics. 2006;117(5):1834–1842 75. Cotman CW, Berchtold NC, Christie
LA. Exercise builds brain health: key roles of growth factor cascades and infl ammation. Trends Neurosci. 2007;30(9):464–472
76. Silverman MN, Deuster PA. Biological mechanisms underlying the role of physical fi tness in health and resilience. Interface Focus. 2014;4(5):20140040
77. Tsatsoulis A, Fountoulakis S. The protective role of exercise on stress system dysregulation and comorbidities. Ann N Y Acad Sci. 2006;1083:196–213
78. Zahn-Waxler C, Shirtcliff EA, Marceau K. Disorders of childhood and adolescence: gender and psychopathology. Annu Rev Clin Psychol. 2008;4:275–303 79. Colman I, Jones PB, Kuh D, et al.
Early development, stress and depression across the life course: pathways to depression in a national British birth cohort. Psychol Med. 2014;44(13):2845–2854
80. Madigan S, Brumariu LE, Villani V, Atkinson L, Lyons-Ruth K. Representational and questionnaire measures of attachment: A meta-analysis of relations to child internalizing and externalizing problems. Psychol Bull. 2016;142(4):367–399
81. Brooks SJ, Kutcher S. Diagnosis and measurement of adolescent depression: a review of commonly utilized instruments. J Child Adolesc Psychopharmacol. 2001;11(4):341–376 82. Ekelund U, Tomkinson G, Armstrong N.
DOI: 10.1542/peds.2016-2266 originally published online March 17, 2017;
2017;139;
Pediatrics
Daphne J. Korczak, Sheri Madigan and Marlena Colasanto
Children's Physical Activity and Depression: A Meta-analysis
Services
Updated Information &
http://pediatrics.aappublications.org/content/139/4/e20162266 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/139/4/e20162266#BIBL This article cites 79 articles, 7 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/public_health_sub Public Health
y_sub
http://www.aappublications.org/cgi/collection/psychiatry_psycholog Psychiatry/Psychology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2016-2266 originally published online March 17, 2017;
2017;139;
Pediatrics
Daphne J. Korczak, Sheri Madigan and Marlena Colasanto
Children's Physical Activity and Depression: A Meta-analysis
http://pediatrics.aappublications.org/content/139/4/e20162266
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2017/03/15/peds.2016-2266.DCSupplemental Data Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.