Not Only a Matter of Epilepsy: Early Problems of Cognition and Behavior
in Children With “Epilepsy Only”—A Prospective, Longitudinal,
Controlled Study Starting at Diagnosis
Kim J. Oostrom, PhD*; Anneke Smeets-Schouten, PhD‡; Cas L. J. J. Kruitwagen, MSc§;
A. C. Boudewyn Peters, MD, PhD储; and Aagje Jennekens-Schinkel, PhD*; for the Dutch Study Group of Epilepsy in Childhood (DuSECh)
ABSTRACT. Objective. To understand early educa-tional and behavioral predicament in childhood “epi-lepsy only.”
Methods. A multicenter, prospective, longitudinal study was conducted of 51 outpatient schoolchildren with newly diagnosed idiopathic or cryptogenic epilepsy and 48 sex-matched classmate control subjects. All chil-dren underwent neuropsychological assessment 3 times within the first year after diagnosis; parents and teachers completed behavior questionnaires, and patients’ par-ents were interviewed to inventory contextual adversity. Principal components analysis of cognition and behavior disclosed 6 major components that were related with the interview data (repeated measures analysis of variance). Results. Despite similar intelligence and educational background, significantly more patients (51%) than con-trol subjects (27%) required special educational assis-tance. Patients obtained worse scores across components of cognition and behavior. Parents and teachers per-ceived patients to have more behavioral problems. Dif-ferences between groups existed at pretreatment base-line. Over time, notwithstanding stable percentages of poor scores in both groups, nonpersistence of poor scores was impressive (each time other children scored poorly in other domains). Rather than epilepsy characteristics, contextual adversities were significant risk factors.
Conclusion. Already in the earliest stage of the ill-ness, children with epilepsy are liable to vicissitudes in cognitive and behavioral functioning. Contextual vari-ables are all-important. Pediatrics 2003;112:1338 –1344; adversity, behavior, context, cryptogenic, epilepsy, idio-pathic, predicament, school.
ABBREVIATIONS. SEA, special educational assistance; DuSECh, Dutch Study of Epilepsy in Childhood; AED, antiepileptic drug; SE, size of effect.
H
aving epilepsy is more than suffering from a purely medical condition. Even when the medical prognosis is favorable, as in “epi-lepsy only,”1the patient may still experiencepsycho-social adversity years after the diagnosis. Children with “epilepsy only” have idiopathic or cryptogenic (according to the International League Against Epi-lepsy,2 presumed to be symptomatic but no cause
could be identified, by magnetic resonance imaging, history, or otherwise) epilepsy; receive mainstream education; visit the pediatrician or (child) neurolo-gist only on an outpatient basis; and are hardly, if at all, restricted in daily life activities. Having followed children with “epilepsy only” well into adulthood, Sillanpa¨a¨ et al3 reported even among patients who
had been seizure-free for years an unduly large num-ber of people with only primary education. Presum-ably related with this was the excessively frequent occurrence of unemployment and low-prestige pro-fessions among adults who had at one time had idiopathic or cryptogenic epilepsy. Similar findings were reported in Great Britain4 and the United
States.5All 3 of these large-scale studies were unable
to identify causative factors. One of the questions that needs to be addressed is when educational and psychosocial deprivation starts to develop.
To contribute to an explanation, we focused on the earliest stage of the disease. Starting immediately after diagnosis and 3 and 12 months thereafter, we thoroughly studied cognition and behavior of chil-dren with “epilepsy only.” The controlled study fo-cused on 2 levels: 1) the factual level of whether children required special educational assistance (SEA) and 2) the possibly explanatory level of illness variables, cognitive and/or behavioral deviations, and contextual adversity. The queries were as fol-lows: 1) Do children with “epilepsy only” and healthy classmate control children differ with respect to educational hard facts, ie, repeating years at school and requiring SEA? 2) Can the groups be distinguished with respect to measures of cognition and/or behavior? 3) What proportion of the children obtain abnormally poor scores, and in which do-mains of cognition and behavior do they do so? 4) Which epilepsy variables or contextual variables are associated with eventual differences?
This study is a part of the neuropsychological branch of the multicenter Dutch Study of Epilepsy in
From the *Division of Neuropsychology and㛳Department of Child Neurol-ogy, Wilhelmina Children’s Hospital, University Medical Center, Center for Biostatistics, Utrecht, The Netherlands; §Center for Biostatistics, Utrecht University, Utrecht, The Netherlands; and ‡Division of Clinical Psychology, Medical Spectrum Twente, Enschede, The Netherlands.
Received for publication Nov 21, 2002; accepted Feb 18, 2003.
Reprint requests to (K.J.O.) Department of Child Neurology, Division of Neuropsychology (KG 01.327.1), University Medical Center, Wilhelmina Children’s Hospital, PO Box 85090, 3508 AB Utrecht, The Netherlands. E-mail: [email protected]
Childhood (DuSECh),6a group of closely
collaborat-ing Dutch (child) neurologists. It was approved by the ethics and research committees of the participat-ing hospitals.
METHODS Subjects
From January 1997 to November 1998, 69 patients were included in the study. Inclusion criteria were having had at least 2 unprovoked nonfebrile seizures with a time interval of at most 12 months, idio-pathic or cryptogenic cause,7age between 5 and 16 years, and
atten-dance of a mainstream school. Exclusion criteria were having any associated neurologic disorder (identified by history, physical exam-ination, or neuroimaging), having received a diagnosis of having another chronic illness, or previous use of antiepileptic drugs (AEDs). For the purpose of the present study, data obtained from the 15 children who were younger than 7 years were omitted because the Dutch education system is organized in such a way that a majority of children under this age have not yet received formal education on academic skills such as reading, writing to dictation, and arithmetic. After follow-up, it was decided that 3 children with unclassifiable epilepsy had to be removed from the analyses because they had nonepileptic, psychogenic seizures. This decision was based on re-peated electroencephalogram investigations, some with simulta-neous video registration of behavior. We therefore report on 51 patients (Table 1).
Every child with epilepsy or her or his parents asked a healthy classmate to participate. The healthy control children, matched to the children with epilepsy for age, sex, and educational level, provided the data to control for effects of retesting and of normal development. Three of the 51 children with epilepsy could not find a suitable classmate in time. There was no sample attrition.
Design
The study was prospective, longitudinal, and controlled. Con-secutive inclusion of subjects reduced the chance of sampling bias. Because of the requirement of assessing patients within 48 hours after diagnosis in a standard examination setup, a van was con-verted into a neuropsychological laboratory with 2 examination rooms. Differences in fatigue resulting from differing traveling times to 1 central assessment center were prevented as each child with epilepsy and his or her control child were examined on the compound of the hospital where the child with epilepsy was treated. At diagnosis, indicators of epilepsy were recorded by the children’s neurologists, according to standard protocol, formu-lated by the DuSECh6(Table 2).
Teachers provided protocoled information on the children’s school careers. At the first assessment, a well-trained psychologist held a semistructured interview with the patients’ parents,10
fo-cusing on their and their child’s adaptation to the onset of epilepsy and on previous adversities not intrinsically related to epilepsy (Table 2).
The children were assessed shortly (within 48 hours) after having received the diagnosis and before they started AED treat-ment (if necessary). All children were reassessed 3 and 12 months after the first assessment. The comprehensive neuropsychological assessment covered major domains of cognition, academic skills, and mental and motor speed (Table 2). As many available tools in child neuropsychology are downward extensions of adult psycho-logical tests that are not suitable for children, existing tests were adapted and some new tasks were developed, addressing learning and memory (Word Span and Location Learning12), several
as-pects of attention (Balloon Piercing13), and behavior regulation
(Color Trails13). At every assessment, parents and teachers
com-pleted behavior checklists (Table 2). The ratings were corrected for epilepsy-related ambiguity.15,16
Data Management and Statistical Analysis
Analyses were conducted with SPSS 10.0. The data set was completed by imputing missing data (391 of 5252 [7.4%]) by means of regression scores from a missing value analysis.17
Prin-cipal component analysis with Varimax rotation was used for data reduction.18 Principal component analysis is a statistical
proce-dure to transform dependent variables into a new set of linear variables in such a way that a maximum of variance is extracted from the data set. The resulting linear combinations of cohering variables are called components. According to the criterion of Kaiser,19only components with eigenvalues⬎1 were retained. A
solution of 6 normally distributed (Kolmogorov-Smirnov One-Sample Tests) components emerged. The cumulative percentage of explained variance was 70.4. Variables with weightsⱖ0.4 and
ⱕ⫺0.4 were considered to contribute saliently to a component (Table 3).18The components could be adequately characterized by
the labels Attention, Reaction Times, Intelligence including Arith-metic, Academic Skills, Location Learning, and Behavior. “Per-centage of calculation errors” weighed in the component Aca-demic Skills (0.282) but fulfilled the criterion for salience of the component Intelligence.
The 6 components were used as dependent variables in re-peated measures analysis of variance with “time after diagnosis” as the within-subject factor. For multiple comparisons, the Bon-ferroni correction was applied. When relevant (4 of 6 compo-nents), age was a co-variable. Transversal nominal data were studied using Fisher exact test. Longitudinal nominal data were studied using log linear analysis.
Statistical tests were 2-sided, with a 5% significance level. ForP
values between .05 and .10, a tendency to statistical significance was presumed and reported.
As individual differences were to be expected, in the
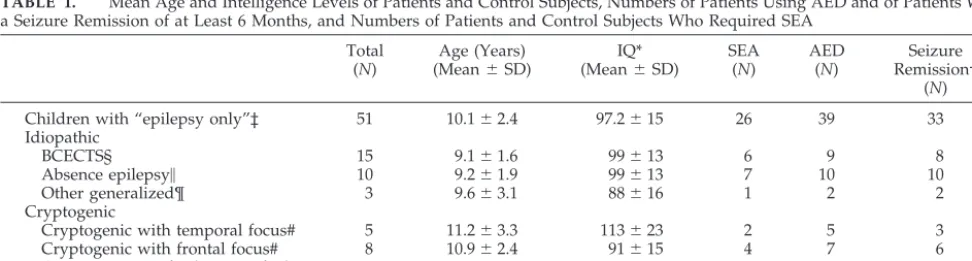
case-by-TABLE 1. Mean Age and Intelligence Levels of Patients and Control Subjects, Numbers of Patients Using AED and of Patients With a Seizure Remission of at Least 6 Months, and Numbers of Patients and Control Subjects Who Required SEA
Total (N)
Age (Years) (Mean⫾SD)
IQ* (Mean⫾SD)
SEA (N)
AED (N)
Seizure Remission†
(N)
Children with “epilepsy only”‡ 51 10.1⫾2.4 97.2⫾15 26 39 33
Idiopathic
BCECTS§ 15 9.1⫾1.6 99⫾13 6 9 8
Absence epilepsy㛳 10 9.2⫾1.9 99⫾13 7 10 10
Other generalized¶ 3 9.6⫾3.1 88⫾16 1 2 2
Cryptogenic
Cryptogenic with temporal focus# 5 11.2⫾3.3 113⫾23 2 5 3
Cryptogenic with frontal focus# 8 10.9⫾2.4 91⫾15 4 7 6
Cryptogenic not further specified# 10 11.1⫾2.7 93⫾14 6 6 4
Classmates (age- and sex-matched) 48 9.9⫾2.5 101⫾15 13 — —
BCECTS indicates benign childhood epilepsy with centro-temporal spikes.
*⬍11 years: Coloured Progressive Matrices8;ⱖ11 years: Standard Progressive Matrices.9
†ⱖ6 months, at 1 year after diagnosis.
‡ Epilepsy classification according to the Commission on Classification and Terminology of the International League Against Epilepsy.7
§ 1.1.a ILAE.
㛳Childhood or juvenile absence epilepsy (2.1.e and 2.1.d ILAE). ¶ Juvenile myoclonic epilepsy (n⫽3; 2.1.f ILAE).
case investigation the criterion for “abnormally poor score” was set on 2 standard deviations worse than the mean component score in the control sample. When an abnormally poor score in a specific component persisted throughout 3 assessments, it was qualified as a “deficit.”
RESULTS School Career
At study entrance, 24% (n⫽12) of the patients had at some time repeated a year at school, more than usual in The Netherlands (11%)20 but not significantly more
than in the control subjects (n⫽10) who were matched for age and sex. Moreover, SEA was required for sig-nificantly more children with epilepsy (n ⫽ 26; 51%) than healthy control subjects (n⫽13; 27%;24.15, df1,
Pⱕ .05). This difference between patients and control subjects did not statistically significantly change over the year after diagnosis.
SEA
Children (patients and control subjects taken to-gether) who required SEA had worse scores in all components of cognition but not in the component Behavior than children who did not require SEA. Sizes of subsamples were too small for reliable
sta-tistical analysis, yet comparison of the 4 groups (pa-tients requiring SEA, pa(pa-tients not requiring SEA, control subjects requiring SEA, and control subjects not requiring SEA) suggested differences. Within pa-tients, the difference between those who required SEA (n ⫽ 26) and those who did not require SEA (n⫽25) pertained to all components of cognition as well as to the component Behavior. Within the con-trol group, the difference between those who re-quired SEA (n ⫽13) and those who did not require SEA (n ⫽ 35) was limited to the component Aca-demic Skills (size of effect [SE]: 13.8, to the advantage of those not requiring SEA).
Components of Cognition and Behavior
Differences Between Patients and Control Subjects
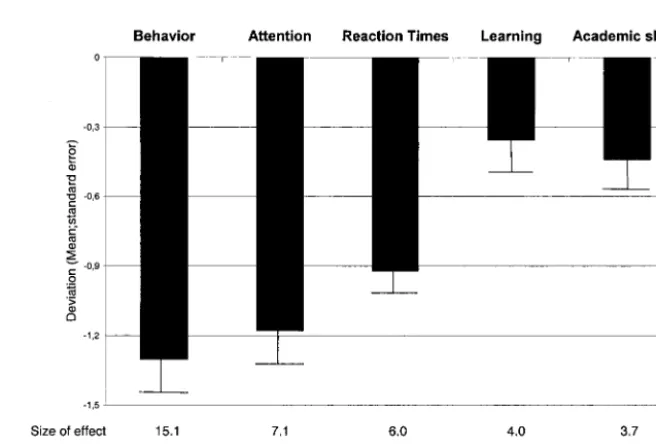
Children with epilepsy obtained statistically sig-nificantly worse scores than control subjects in the components Behavior, Attention, Reaction Times, and Location Learning and tended to score worse in Academic Skills (Fig 1). The differences between pa-tients and control subjects could not be ascribed to any of the epilepsy characteristics.
TABLE 2. Independent and Dependent Variables Independent variables and their classification 1. Epilepsy features
Cause: idiopathic/cryptogenic2,7
Seizure type: primary or secondary generalized tonic-clonic/partial/absence seizure AED: yes/no
Seizure remission ofⱖ6 mo, at 1 year after diagnosis: yes/no 2. School career
Having repeated a year: yes/no Having required SEA: yes/no
3. Reaction to the onset of epilepsy, perceived by parent10
Parenting in the context of adversity caused by epilepsy onset: discontinuity/continuity of habitual parenting
Child’s reaction to the adversity caused by onset of epilepsy: maladaptive/adaptive 4. Previous adversities not intrinsically related to epilepsy, perceived by parent10
Family problems, eg, marital distress, divorce, psychopathology in another family member: present/not present
Long-standing behavior problems, ie, difficult behavior, dating from before onset of epilepsy: present/not present
Long-standing problems in academic skill acquisition, dating from before the onset of epilepsy: present/not present
Neuropsychological battery, screening academic skills, and behavior questionnaires 1. General cognition
Coloured Progressive Matrices,8computerized (children⬍11 yr)
Standard Progressive Matrices,9computerized (children agedⱖ11 yr)
Vocabulary (Wechsler Intelligence Scale for Children–Revised, Dutch edition11
2. Memory and learning
Word span: repetition of nouns with imaginable theme12
Location Learning: learning locations (4⫻4 matrix) of visually presented images of objects12
3. Sustained attention
Balloon Piercing: Target and distracter balloons (ratio 94/281) entering, wandering over and leaving a screen have to be discriminated as quickly and accurately as possible13
4. Behavior regulation
Color Trails–computerized adaptation Color Trails14
5. Reaction Times (RT) 6. Motor speed
Tapping (dominant hand)
7. Academic skills (adapted to the child’s educational level) Reading
Writing to dictation Arithmetic
8. Parents’ and teachers’ ratings of behavior
Child Behavior Checklist, Dutch version, adapted scoring15
Differences Within the Group of Patients Epilepsy features
None of the epilepsy features explained any dif-ferences among patients.
School career
Patients who required SEA obtained worse scores on the components Attention (SE: 17.4), Academic Skills (SE: 9.1), and Reaction Times (SE: 8.5) than patients who did not require SEA.
Reactions to the onset of epilepsy. Patients with par-ents who had had difficulty continuing their habitual parenting style once epilepsy had set in obtained worse scores in Reaction Times (SE: 4.9), Location Learning (SE: 4.5), and Attention (SE: 4.5) and tended to obtain worse scores in Academic Skills (SE: 3.2) than patients with parents who adapted well to the adversity of epilepsy onset. Patients who, them-selves, did not adequately react to the diagnosis
ob-Fig 1. Differences at first assessment between children with “epilepsy only” and control subjects, expressed as deviations from means obtained in controls (zscore*⫽0), shown for ev-ery component.
TABLE 3. Significant Weights in the 6 Components Yielded by the Principle Component Analysis Varimax Solution for 21 Variables With Respect to Cognition, Speed, Academic Skills, and Behavior; Eigenvalues and the Percentage of Variance Explained by Each Component
Components
Attention Reaction Times
Intelligence and Arithmetic
Academic Skills
Location Learning
Behavior
RT: disjunctive decision time 0.828
RT: simple decision time 0.804
Word Span backward ⫺0.704
Word Span forward ⫺0.691
Color Trails part 2: execution time 0.599 0.421
Tapping: number of taps ⫺0.586 ⫺0.508
Color Trails part 1: execution time 0.539 0.474
RT: disjunctive motor time 0.858
RT: simple motor time 0.788
Balloon piercing: execution time 0.552
Coloured/Progressive matrices: IQ 0.824
WISC-R/WPPSI: Vocabulary 0.794
Arithmetic: errors (%) ⫺0.400 ⫺0.563
Reading aloud: errors (%) 0.779
Writing to dictation
Skill errors (%) 0.760
Slips of the pen (%) 0.643
Location Learning:
Total immediate recall 0.819
Proactive interference 0.786
Response time ⫺0.667
Child Behavior Checklist:
Total problems score 0.844
Teacher’s Report Form:
Total problems score 0.759
Eigenvalues 7.22 2.94 1.88 1.35 1.25 1.03
Percentage of explained variance 32.83 13.37 8.55 6.14 5.70 4.70
tained worse scores in Behavior than patients who adapted well to the onset of epilepsy (SE: 4.4).
Previous adversities not intrinsically related to epi-lepsy. Comparing patients whose parents reported previous adversities to patients without a history of difficulties led to the following findings: Patients with family problems obtained worse scores in Be-havior (SE: 7.5) and Location Learning (SE: 4.5) than patients from happy families. Patients with preexist-ing problems of academic acquisition obtained worse scores in Academic Skills (SE: 5.6), and tended to obtain worse scores in Intelligence and Arithmetic (SE: 3.8) and in Attention (SE: 2.9) than children who progressed normally at school. Patients who had behavioral problems that antedated the first signs and symptoms of epilepsy tended to obtain worse scores in Location Learning (SE: 3.3) and Behavior
(SE: 3.0) than children without a history of behavior problems.
Time Effects
Changes over the year after diagnosis were found within the group of patients only: a decline in Aca-demic Skills was found in the group of patients whose parents had complained of problems in aca-demic skill acquisition, dating from before the onset of epilepsy (SE: 4.4), and in the small group of pa-tients who required SEA.
Case-by-Case Analysis
Summated over the year, more patients (n ⫽ 23; 45%) than control subjects (n⫽11; 23%) had at least 1 abnormally poor score (likelihood ratio27.25,Pⱕ
.01). The proportions of patients and control subjects
with abnormally poor scores remained stable over time, but the children of whom this proportion was composed changed (Fig 2).
Abnormally poor scores occurred in 1 or a few components rather than in all at the same time. The component Behavior drew more children with ab-normally poor scores (14 with epilepsy, 4 control subjects) than any of the other components (likeli-hood ratio 2 20.73, P ⱕ .00). In the component
Behavior, 5 patients qualified for a “deficit,” and in the component Reaction Times, 1 other patient did so. One control child had a deficit in both Attention and Academic Skills. Another control child had a deficit in Location Learning.
DISCUSSION
The major findings of the present study focusing on early features of the educational and behavioral predicament in childhood “epilepsy only” are 3-fold: First, the school career of children with newly diag-nosed “epilepsy only” is already at risk in the very earliest stages of the disease. Notwithstanding aver-age intelligence levels, half of the school children aged 7 years and older needed SEA. Second, as a group, children with “epilepsy only” obtained worse scores in principal components of cognition and be-havior than healthy age- and sex-matched control subjects. As the latter were classmates of the children with epilepsy, an explanation by differences in edu-cational background was ruled out. Third, psycho-social context rather than characteristics of the epi-lepsy were related to the patients’ performances on measures of cognition and behavior. These are find-ings that need understanding, for, if not remedied, these early educational and behavioral predicaments may end in psychosocial and vocational burden in adulthood.3,4
To estimate the clinical significance of group find-ings, we looked at the performance of patients and control children individually. On the basis of as-sumptions in clinical practice, we considered scores worse than the cutoff of 2 standard deviations from the mean score in the control sample to be clinically relevant. This classified 45% of the children with epilepsy, compared with 23% of the healthy children, in the range of clinically relevant problems of cogni-tion and behavior. However, as illustrated by the scattering in Fig 2, clinically relevant poor cognitive performances are persistent in only 1 patient (patient 1, in the component Reaction times) and in 2 control subjects (child 1, in the components Attention and Academic Skills; child 2 in the component Location Learning). The Behavior component, assessed by means of ratings by parents and teachers, yielded the largest difference between the groups. No fewer than 5 patients (10%) were qualified as having a (persis-tent) behavior “deficit,” whereas none of the control children was qualified as such.
Among children with “epilepsy only,” cause, lepsy syndrome, use of AED, and course of the epi-lepsy in the first year after diagnosis were not sig-nificantly related to the cognitive or behavioral findings. Contextual variables (listed in Table 2), however, had significant effects on cognition and
behavior. Most consistent, having parents who are thrown off balance in the time preceding the diag-nosis and who fail to continue their habitual parent-ing affected the patients’ cognitive and behavioral functioning. However, belonging to a troubled fam-ily or having preexisting problems of behavior and of acquiring academic skills was also associated with scoring poorly at tests that assess reaction times, location learning, and attention. Also, children who could not adaptively integrate the adversity of epi-lepsy onset obtained worse scores in behavior. This is of particular relevance. We reported previously that healthy children and patients alike perceive epilepsy as different from other illnesses in the sense that epilepsy provokes more shame than other illnesses.21
Current views on risk factors for psychopathology hold that recurrently experiencing negative emotions induces a proneness to those emotions and that this proneness distorts cognition and biases action and perception. For shame, it has been demonstrated that shame-proneness is a potent predictor of depression later in life.22The main message of the present study
is that already at diagnosis, children who do not adaptively react to the adversity of epilepsy have an increased risk of negative reactions.
The present study clearly shows that cognitive and behavioral sequelae arise from multiconditional vul-nerability rather than from strictly medical aspects of epilepsy and that these problems already become apparent at the very earliest stages of “epilepsy only.” As problems of cognition and behavior may have far-reaching consequences, physicians should be attentive not only to the child’s school history and/or behavioral problems but also to the child’s and parents’ upset as a result of the epilepsy. In case of complaints, help should be called in without de-lay.
ACKNOWLEDGMENTS
The study was funded by the National Epilepsy Foundation (grant 97-04), the JANIVO Foundation, and Peugeot Holland NV. Participants in DuSECh: W.F.M. Arts, J.H. Begeer, O.F. Brou-wer, C.A. van Donselaar, A.T. Geerts, E.A.J. Peeters, H. Stroink, G. Hageman, R. ten Houten, A.C.B. Peters, J.F. de Rijk-van Andel, L.M.E. Smit, and M.J. Wennekes.
We thank all of the patients, classmates, parents, and teachers who took part in the study. We thank Professor F.G.I. Jennekens for critical comment on the article and Marguerite Schinkel, BA, for language editing.
REFERENCES
1. Sillanpa¨a¨ M. Epilepsy in children: prevalence, disability, and handicap.
Epilepsia. 1992;33:444 – 449
2. Engel J Jr. A proposed diagnostic scheme for people with epileptic seizures and with epilepsy: report of the ILAE task force on classifica-tion and terminology.Epilepsia.2000;42:1– 8
3. Sillanpa¨a¨ M, Jalava M, Kaleva O, Shinnar S. Long-term prognosis of seizures with onset in childhood.N Engl J Med. 1998;338:1715–1722 4. Morgan CLI, Ahmed Z, Kerr MP. Social deprivation and prevalence of
epilepsy and associated health usage.J Neurol Neurosurg Psychiatry. 2000;69:13–17
5. Preter M. Social deprivation and prevalence of epilepsy and associated health usage.J Neurol Neurosurg Psychiatry. 2000;69:837
6. Arts WFM, Geerts AT, Brouwer OF, Peters ACB, Stroink H, van Don-selaar CA. The early prognosis of epilepsy in childhood: The prediction of a poor outcome. The Dutch Study of Epilepsy in Childhood.Epilepsia.
1999;40:726 –734
Classi-fication and Terminology. Proposal for revised classiClassi-fication of epilep-sies and epileptic syndromes.Epilepsia. 1989;30:389 –399
8. Raven JC, Court JH, Raven J.Coloured Progressive Matrices (1990 edition). Oxford, UK: Oxford Psychologists Press; 1990
9. Raven JC, Court JH, Raven J.Standard Progressive Matrices (1992 edition). Oxford, UK: Oxford Psychologists Press; 1992
10. Oostrom KJ, Schouten A, Kruitwagen CLJJ, Peters ACB, Jennekens-Schinkel A. Parental perceptions of adversity introduced by upheaval and uncertainty at the onset of childhood epilepsy.Epilepsia. 2002;42: 1452–1460
11. Bruyn EEJ de, Steene G van der, Haassen PP van.Wechsler Intelligence Scale for Children–Revised. Nederlandse Uitgave. Lisse: Swets & Zeitlinger; 1986
12. Schouten A, Oostrom KJ, Pestman WR, Peters ACB, Jennekens-Schinkel A. Learning and memory of schoolchildren with epilepsy. A prospec-tive controlled longitudinal study. Dev Med Child Neurol.2002;44: 803– 811
13. Oostrom KJ, Schouten A, Kruitwagen CLJJ, Peters ACB, Jennekens-Schinkel A. Attention deficits are not characteristic of schoolchildren with newly diagnosed idiopathic or cryptogenic epilepsy. Epilepsia.
2002;43:301–310
14. Maj M, D’Elia L, Satz P, et al. Evaluation of two new neuropsychological tests designed to minimize cultural bias in the assessment of HIV-1
seropositive persons: a WHO Study. Arch Clin Neuropsychol.1993;8: 123–135
15. Oostrom KJ, Schouten A, Peters ACB, Jennekens-Schinkel A. Epilepsy-related ambiguity in rating the child behavior checklist and the teach-er’s report form.Epileptic Disord. 2001;3:39 – 45
16. Perrin EC, Stein REK, Drotar D. Cautions in using the Child Behavior Checklist/4 –18.J Pediatr Psychol. 1991;16:411– 421
17. Little RJA, Rubin DB.Statistical Analysis With Missing Data.New York, NY: Wiley; 1987
18. Stevens J. Exploratory and confirmatory factor analysis. In: Stevens J, ed.Applied Multivariate Statistics for the Social Sciences.Mahwah, NJ: Lawrence Erlbaum Associates; 1996:362– 428
19. Kaiser HF. The application of electronic computers to factor analysis.
Educ Psychol Measures. 1960;20:141–151
20. van de Grift W. Hoe kan ik de opbrengst van mijn school bepalen? [English translation: How to assess the output of my school?]School Manag.2000;13:12–22
21. Oostrom KJ, Schouten A, Peters ACB, Jennekens-Schinkel A. Negative emotions in children with newly diagnosed epilepsy.Epilepsia. 2000;41: 326 –331
22. Tangney JP, Burggraf SA, Wagner PE. Shame-proneness, guilt-proneness, and psychological symptoms. In: Tangney JP, Fischer KW, eds.Self Conscious Emotions: The Psychology of Shame, Guilt, Embarrass-ment and Pride.New York, NY: The Guilford Press; 1995:175–197
COLLEGES CAUGHT IN A VISE
“What percentage of the university’s operating costs do you guess are covered by public funds? Almost always, the answer is something on the order of 75%. When I say, no, the figure is just 25% and heading downward—and add that in some states the figure has dipped below 10%—the reaction is usually equal parts surprise and dismay. . . . What percentage of the cost to educate a student do you guess is covered by tuition? . . . If you include not just classroom education but the cost of everything that must be in place for that education to occur—a library, laboratories, computer centers, building maintenance, utilities, safety patrols and more—tuition covers only 26%. ‘You’re telling me that state funds are being withdrawn at the same time expenses are exceeding tuition by a factor of three to one. How can you stay in business?”
Fish S. Colleges caught in a vice.New York Times. September 18, 2003
2003;112;1338
Pediatrics
Peters and Aagje Jennekens-Schinkel
Kim J. Oostrom, Anneke Smeets-Schouten, Cas L. J. J. Kruitwagen, A. C. Boudewyn
Starting at Diagnosis
A Prospective, Longitudinal, Controlled Study
−−
Children With ''Epilepsy Only''
Not Only a Matter of Epilepsy: Early Problems of Cognition and Behavior in
Services
Updated Information &
http://pediatrics.aappublications.org/content/112/6/1338
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/112/6/1338#BIBL
This article cites 16 articles, 2 of which you can access for free at:
Subspecialty Collections
rning_disorders_sub
http://www.aappublications.org/cgi/collection/cognition:language:lea Cognition/Language/Learning Disorders
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
2003;112;1338
Pediatrics
Peters and Aagje Jennekens-Schinkel
Kim J. Oostrom, Anneke Smeets-Schouten, Cas L. J. J. Kruitwagen, A. C. Boudewyn
Starting at Diagnosis
A Prospective, Longitudinal, Controlled Study
−−
Children With ''Epilepsy Only''
Not Only a Matter of Epilepsy: Early Problems of Cognition and Behavior in
http://pediatrics.aappublications.org/content/112/6/1338
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.