60
50
40
30
20
I0 ABSTRACT. Purulent conjunctivitisassociatedwith oti
tis media was studied in 124patients in a private practice over a period of one year. Of the 132 patients seen with
purulent conjunctivitis, 96 (73%) concurrently had otitis
media. In 28 (47%) of 60 families with more than one child, siblings of the index cases had either purulent conjunctivitis or otitis media, or both, simultaneously or within one month. During the study period, conjunctival cultures were obtained from 75 patients with purulent conjunctivitis-otitis media and patients with purulent conjunctivitis whose siblings had purulent conjunctivitis
otitis media or otitis media. Haemophilus influenzae was
isolated from 55 (73%). Thirty-one of the patients had nasal cultures done simultaneously with conjunctival cul tures. An identical pathogen was isolated from 27 (87%) patients, Pediatrics 69:695—698,1982;purulent conjunc tivitis, otitis media, Haemophilus influenzae infections.
Although purulent conjunctivitis and otitis media frequently occur together in what appears as one
disease, they are generally considered as two en tirely different diseases. In a review of the literature, only in two series―2 was it noted that purulent
conjunctivitis accompanied otitis media.
The purpose of this study is to determine fre quency and perhaps etiology of the disease.
PATIENTS,METHODS,ANDMATERIALS
Between March, i980, and March 4, i98i, 112 patients representing 98 families from the author's
private practice were selected for the study by the
following criteria: (1) all patients who had purulent conjunctivitis concomitant with otitis media
(PCOM); (2) all patients who either had otitis media (OM) or purulent conjunctivitis (PC) and whose sibling(s) or close playmate(s) had PCOM simulta
neously or within one month; (3) all patients who
Received for publication April 27, 1981; accepted July 22, 1981. Reprint requests to (F.F.B.) Fairview Hospital Physicians' Cen
ter, 18099 Loraine Aye, Cleveland, OH 44111.
PEDIATRICS (ISSN 0031 4005). Copyright © 1982 by the
American Academy of Pediatrics.
had OM and whose sibling(s) had PC, either simul
taneously or within one month. Sixty-four (57%) of
the patients were male and 58 (43%) were female.
Their ages ranged from 2½months to 7 years.
All patients who had purulent discharge from the
eyes underwent a general physical examination.
Diagnosis of otitis media was made on the basis of bulging, erythema, opacity, and reduced mobility of the tympanic membranes.―35
Cultures were taken from the lower palpebral conjunctivae with cotton-tipped applicators, were
immediately inoculated on chocolate- and sheep
blood agar plates. Chocolate-agar plates were in cubated in carbon dioxide atmosphere to facilitate growth of Haemophilus influenzae, whereas blood agar plates were incubated in room air. Bacteria were identified on the basis of growth characteris
0-12m
@ 2 3 4 5 6 7 8 9 0
AGE -Years
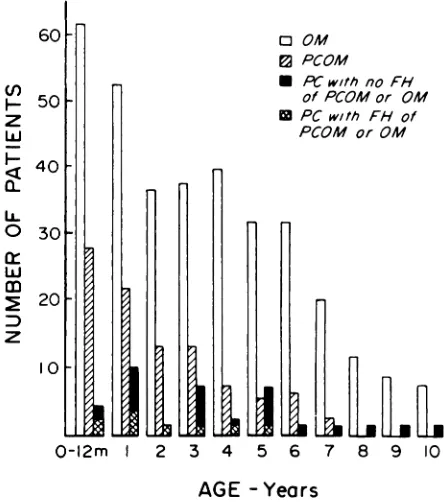
Fig I . Distribution by age of 96 patients with purulent conjunctivitis-otitis media (PCOM), 346 patients with . otitis media (OM), and 36 patients with purulent con
junctivitis (PC). FM, Family history. 0 OM
@ PCOM
S PCwithnoFH
of PCOM or GM
@ PC with PH of
PCOM or GM
(I)
I-z
Lu
I—
U-0
Lu
z
PEDIATRICS Vol. 69 No. 6 June 1982 695
Conjunctivitis-Otitis Syndrome
Frank Franjo Bodor, MD
From the Fairview Hospital Physicians
@ Center, Cleveland
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news
Family Date Name Age Diagnosis Conjunctival Culture NasalCulture
1 3/05W.B.4moPCOMb3/08W.L.10 yr 7 moPCOMb23/04C.R.3
yrPCOMu3/18C.M.7moOMu33/14N.K.2
yr 6 moPCOMu3/29N.B.8
moPCOMb44/25B.R.2
yr 9 moPCOMu4/25B.M.10
moPCOMuHi 3+; Staphylococcus
aureus54/21F.M.1
yr 2 moPCOMu4/25F.D.9
moPCOMuHi 3+Hi
3+64/22P.J.3
yr 7 moPCOMb4/22P.M.1
yr 8 moPCOMbHi 3+74/21B.E.6
moPCOMuHi 3+t5/09B.S.4
yr 5 moPCOMuHiB 3+84/18M.T.3yr3moPC5/24M.M.1
yrPCOMbHi 1+Hi
3+94/30U.M.3
yr 10 moPCOMuHi 3+5/05U.M.11
moPC105/175.5.3
yr 1 moPCOMu5/28S.P.6
yr 7 moPCOMuHi 1+5/21S.L.4
yr 9 moPCOMuHi
2+1
14/28D.C.1 yr 6 moPCOMuPneumococci
3+4/29D.K.4yrOMu125/21M.J.2
yr 3 moPCOMbHi 3+5/25MM.3
yrOMuHi 3+135/24C.J.6
yr 9 moPCOMb5/24C.M.3yrPCOMb147/28W.N.2
yr 7 moPCOMuHi 3+8/11W.J.1
yr 5 moPCHi 3+158/15R.D.7
yrPCOMuStaphylococcus albus8/15R.C.4
yrPCOMuNo growth169/08L.M.6
yrPCOMu10/10L.J.2
yrPCOMu179/09G.M.4yrPCOMu9/19G.M.1
yr 5 moPCOMu189/17D.C.6
yrPCOMuStaphylococcus albus
1+9/30C.B.7
yrPCOMb1910/06B.G.3yr6moPCOMb10/08B.S.1 yr 3 moPCOMu2011/24K.K.1
yr 7 moPCOMbHiB 3+HiB
3+11/24K.D.1
yr 7 mo0MbHiB 3+HiB
3+11/24K.J.3
yr 6 mo0MbHiB 3+HiB
3+2111/29P.M.3
yr 6 moPCOMuHi 3+Hi
2+12/10P.K.6
yrOMuNo growthNF2212/12C.A.2
yr 6 moPCOMbHiB 3+HiB 1+
NF12/14C.M.9
moOMuNo growthHiB
3+2312/01G.A.4
mo0MbNF12/15G.M.4
yrPCOMbHi 3+
TABLE I . Familieswith MoreThan OneChildwith PCOM or OneChildwith PCOM andOther(s)HavingOM or
PC
C Abbreviations used are: PCOM, purulent conjunctivitis-otitis media; OM, otitis media; PC, purulent conjunctivitis;
Hi, Haemophilus influenzae', HiB, H. influenzae type B; 1+, few colonies; 2+, moderate growth; 3+, heavygrowth; u, unilateral; b, bilateral; NF, normal flora.
t Not typed.
PCOM was observed in 96 patients from 70 fam ilies. Nine of these patients had two episodes of PCOM. Their age distribution is shown in Fig 1. tics, colonial morphology, and microscopic exami- RESULTS
nation of Gram stains. H influenzae were typed with type B antiserum. Streptococcus pneumoniae
were identified by morphology of the colonies, Gram stains, and the bile solubiity test.
696 CONJUNCTIVITIS-OTITIS SYNDROME
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news
TABLE 2. ConjunctivalCultureson 75 Patientsw
Purulent Conjunctivitis-Otitis Media (PCOM) and Patients with Purulent Conjunctivitis (PC)ith
29Bacterial
Agent PCOM
PCHaemophilus
influenzae 49
14(nontypable)H
influenzae type B 6
1Streptococcus pneumoniae 3 2Neisseria catarrhalis 1Staphylococcus aureus 1)Staphylococcus albus 11 1Nogrowth 4 8
In 28 (49%) of the 57 families with more than one child in the family more than one child was affected
either simultaneously or within one month with
PCOM or its components. The incidence of families with more than one child with PCOM, PC, or OM simultaneously or within one month is as follows: PCOM-PCOM, 11 families; PCOM-PC, 4 families; PCOM-OM, 8 families; PC-OM, 5 families.
In one family three siblings had PCOM, whereas their mother had PC. Three other mothers had PC simultaneously with their children's PCOM. In two families with two children each, the mothers took turns babysitting for each other's children. The children played together and when one developed PC, a child from the other family developed PCOM 12 days later, followed by PCOM and PC in the other two children after intervals of five and 19 days, respectively. This is shown in Table 1 (fami lies 8 and 9).
CLINICAL OBSERVATIONS
In most of the patients the illness started with low-grade to moderate fever, mucopurulent rhinor rhea, and cough, which was often described as harsh. Pain in the eye and purulent discharge from them usually started three or four days later. The conjunctivae were injected and tearing occurred, sometimes so profusely that the skin in the infraor bital area became irritated if the process lasted several days. Upon awakening, the eyelashes were adherent and covered with crusty material. Earache usually started on the same day as the eye symp toms, or one to three days later, seldom before. However, ear pain was absent in 60% of the patients in this study. Of the patients who were brought to the office 31% came only because of the eye symp toms. Three patients in this study, all of whom had symptoms of PC and mucopurulent rhinorrhea,
were examined before the symptoms and physical
signs of OM developed. All of them had nasal and conjunctival cultures done and were treated with sulfacetamide sodium 10% ophthalmic drops. They
were observed daily, and by the third day all of
them had evidence of OM; in one patient unilateral PC became bilateral. One patient with PCOM had phlyctenular nodules in both eyes. Submandibular lymph nodes were slightly enlarged and tender in some of the patients.
Bacteriologic findings are listed in Table 2. H
influenzae was isolated from 55 (73%) of the total
75 conjunctival cultures done on patients with PCOM. Six of the total 18 cultures that were typed
were type B. Thirty-one of the patients had nasal
cultures done simultaneously with conjunctival cul tures and 27 (87%) of them had identical microor
ganisms. Although pathogens from the conjuncti vae grew almost in a pure culture in 56 (93%) of 60 cultures, it was mixed with saprophytic nasal flora in many of the nasal cultures, making it difficult to identify the pathogen in these nasal cultures. In six of the families, identical pathogens were isolated from siblings as shown in Table 1.
One patient had a heavy growth of H influenzae from the conjunctiva and a heavy growth of both H
influenzae and Spneumoniae from the nasal swab.
Another patient had no growth from the conjunc tivae, and a heavy growth of H influenzae from the nasal culture. One patient with PCOM, whose otitis media failed to resolve after a ten-day course of amoxicillin, underwent middle ear aspiration and the exudate was cultured. H influenzae was iso lated. A conjunctival culture was not done for this patient. The diagnosis of otitis media was given to two children on the same day that a diagnosis of PCOM was given to their sibling. A heavy growth of H influenzae type B was isolated from conjunc tival as well as nasal cultures that were done si multaneously in all three patients (Table 1, family 20).
In Fig 2 are shown seasonal variations in mci dence of PCOM, OM, and PC. There were great variations between cold and warm seasons in num bers of cases of OM, but this was not the case with occurrence of PCOM.
DISCUSSION
A high incidence of otitis media in patients who had purulent discharge from the eyes was found in this study. Based on the data and clinical observa tion of this study and previous studies finding high correlations of nasopharyngeal cultures with cul tures of middle ear exudates,3'4 it appears that this high incidence is not merely a coincidental occur rence. Furthermore, 73% of H influenzae isolated from conjunctival cultures in this study is a rate quite similar to the 72% rate of isolation of H influenzae reported by Coffey' from middle ear
ARTICLES 697
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news
obstruction. From this inflamniatory process, exu date with bacteria is being formed, which on the
side of the tubes is pushed upward into the tubes.
This then causes propagation of the process toward the middle ears and the lacrimal ducts, and, perhaps
into the paranasal sinuses.6
Epidemiologic observations indicate that PCOM
is largely a disease of infants and small children
(Fig 1), more so than otitis media unassociated with purulent conjunctivitis. Of the patients with PCOM
50%werelessthan 2 yearsof age.In the groupof
patients with OM, only 30% were less than 2 years of age.ACKNOWLEDGMENTS
I thank Richard E. Behrman, MD, Alfred Heggie, MD, Bernard L. Kasten, MD, and Paul A. Shurin, MD, for reviewing the manuscript and for their helpful sugges tions, and Isabella Barna, Sandra Cipiti, and Linda Bar
biaux of Fairview General Hospital Laboratory, Section of Microbiology, for technical assistance.
REFERENCES
1. Coffey JD: Otitis media in the practice of pediatrics. Pedi
atrics 38:25, 1966
2. Gigliotti F, Williams WT, Hayden FG, et al: Etiology of acute conjunctivitis in children. J Pediatr 98:531, 1981 3. Howie VM, Ploussard JH, Lester RL Jr: Otitis media: A
clinical and bacteriological correlation. Pediatrics 45:29,
1970
4. Schwartz H, Rodriguez WJ, Mann R, et al: The nasopharyn
geal culture in acute otitits media—a reappraisal of its use fulness. JAMA 241:2170, 1979
5. Bluestone CD, Shurin PA: Middle ear disease in children: Pathogenesis, diagnosis, and management. Pediatr Clin
North Am 21:379,1974
6. Nelson JD, McCracken GH Jr: Maxillary sinusitis in chil
dren. Pediatr Infect Dis, November 1980 60
50
40
30
20
I0
0 GM
@ PCOM
. PCwithnoFH
of PCOM or GM
@ PC with F/-f of
PCOM or GM
M A M J J A S 0 N D J F
MONTH
Fig 2. Seasonaldistribution of purulent conjunctivitis otitis media (PCOM), otitis media (OM), and purulent conjunctivitis (PC). FH, Family history.
exudates of 18 patients who had purulent discharge
from the eyes. This pattern strongly suggests a common etiology. A high attack rate among siblings and close playmates suggest that the infection is
primary, rather than secondary to a viral infection
or allergic disease causing Eustachian tube dysfunc tion. Perhaps the disease, PCOM syndrome, which
is most often caused by H influenzae, starts out as
a primary rhinitis, which because of the edema of
the ostia of the Eustachian tubes, lacrimonasal
ducts, and perhaps paranasal sinuses, causes their
(1)
z
Lu
I-
U-0
Lu
:D
z
698
CONJUNCTIVITIS-OTITIS
SYNDROME
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news
1982;69;695
Pediatrics
Frank Franjo Bodor
Conjunctivitis-Otitis Syndrome
Services
Updated Information &
http://pediatrics.aappublications.org/content/69/6/695
including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or in its
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news
1982;69;695
Pediatrics
Frank Franjo Bodor
Conjunctivitis-Otitis Syndrome
http://pediatrics.aappublications.org/content/69/6/695
the World Wide Web at:
The online version of this article, along with updated information and services, is located on
American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 1982 by the been published continuously since 1948. Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
at Viet Nam:AAP Sponsored on September 7, 2020
www.aappublications.org/news