The Effects of Induced Hypervigilance in Healthy Subjects Sloan Walters
University of North Carolina at Chapel Hill Spring 2015
A thesis presented to the faculty of The University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the Bachelor of Science degree with Honors in Psychology.
Advisor________________________
Reader________________________
Abstract
Previous studies have both associated hypervigilance with generalized amplified perception and demonstrated that is it possible to induce hypervigilance in healthy participants. However, little research has been done to understand the perceptual changes associated with induced
hypervigilance in healthy participants. This study sought to understand if hypervigilance could be induced in healthy participants using writing and counting tasks. Also, the study explored if participants in this hypervigilant state perceived tactile stimulation differently than control subjects. A total of 48 undergraduates from the PSYC 101 Participant Pool at the University of North Carolina at Chapel Hill participated in the study. Over the course of an hour they
completed writing and counting tasks, as well as a series of questionnaires. Then, ratings of tactile stimuli were used to detect any differences in pain perception in the groups. Comparisons of unpleasantness threshold and pain threshold, as well as intensity and unpleasantness ratings, reveal that there was little statistically significant difference between groups. Additionally, questionnaire data revealed that hypervigilance was not induced in experimental subjects. The results did not support the hypotheses that hypervigilance would be induced or that
Acknowledgements
I am happy to express my most sincere gratitude to my advisor, Dr. Mark Hollins, for affording me the opportunity to extend my education in the most valuable way, through
experience. Further, I offer my appreciation for the opportunity to research a topic of my interest while gaining invaluable research experience and critical thinking skills. Without his support and challenges I would not be the student that I have grown to become.
Further, I would like to extend additional thanks to Dr. Mark Hollins, Dr. Viji Sathy and Page Dobson for participating in my honors committee. I am humbled by the time they sacrificed to both critically read and review my thesis as well as join me for my defense for the sake of my education. Moreover, their insightful critiques and constructive criticisms offered me lessons that could never be learned in a classroom.
To the Somatosensory Lab, especially Dr. Hollins, Page Dobson and Mary Whatley, thank you for allowing me to share in your resources of time and space in order to successfully implement my thesis research. Further, I am grateful for your endless support in its many forms, from advice about statistics, to providing a listening ear practicing presentations as well as conducting participant trials. I would also like to thank the Honors Psychology program, especially Dr. Beth Kurtz-Costes and Dr. Peter Ornstein, your guidance and support were a crucial aspect of this project.
The Effects of Induced Hypervigilance in Healthy Subjects
Pain is a persistent variable of the human experience. Both emotionally and physically, epochs of pain are often among the most defining in a person’s life. The topic of this research is a sort of pain that while life defining, serves little utility. Specifically, this paper speaks about chronic pain and its origins. In order to best grasp the importance of the significance of chronic pain research it is best to understand the utility and nature of normal pain processes. Generally, pain protects the body in two important ways: alerting and reminding. Alerting pain protects animals by offering a warning about ongoing damage, an example of this is when a child places his hand on a stove and immediately withdraws it to prevent tissue damage. Reminding pain exists to ensure that an injured area is favored until it can heal completely. An example of this is the tenderness associated with lacerations. Aside from the function of pain, time is another important dimension of the pain experience. Acute pain is the useful kind of pain just discussed and is almost always capable of being attributed to some direct cause and utility to the body. It is clinically defined as lasting less than one month (Chapman, 1978). Long-term pain, called chronic pain, such as that seen in disorders like fibromyalgia, retains little benefit to the body. This sort of pain is generally defined as pain lasting more than three months. While intermittent, acute pain is healthy and important to the protection of the body, long term pain does not provide any meaningful information about the body’s current state and greatly decreases the quality of life of the person experiencing it.
chronic pain have decreased executive functioning (Nes, Roach, & Segerstrom, 2009). Also, chronic pain sufferers are more likely to suffer from depression and report a decreased quality of life (Allen, Hubbard, & Sullivan, 2005). In addition to effects on the individual, chronic pain is a great obstacle to productivity at a population scale. Chronic pain conditions such as fibromyalgia and migraine disorders have been estimated to cause productivity loss of nearly 13% in US workforce work hours. This brings an annual cost of more than 60 billion dollars to the nation’s government (Allen, Hubbard, & Sullivan, 2005). This problem is a growing epidemic. At the time of their study 29% of participants met the definition for chronic pain; this corresponded with drops of more than 45% in physical health and 23% in mental health (Allen, Hubbard, & Sullivan, 2005).
With concerns at both an individual and societal levels in mind, scientists and patients alike have sought remedies for chronic pain. Generally, these attempts have been met with little success in finding a treatment that effectively reduces chronic pain in the long term. Scientists and health professionals have drawn knowledge and techniques from diverse sources ranging from the most advanced biomedicine to herbal remedies that are thousands of years old (Turk & Monarch, 1996). In spite of this global effort, nothing has been able to alleviate chronic pain permanently. All of these failed approaches have addressed the complicated physiological and biochemical etiologies of chronic pain, but have paid less attention to the cognitive and affective components of chronic pain mechanisms. Moving forward, it is important to combine the
In order to address the psychological components of chronic pain, a psychological model of chronic pain must first be established. The model of chronic pain used in this study ascribes chronic pain in part to a cognitive attribution style in which perception is generally magnified and feedback loops prevent pain from ever being ameliorated. The name used for this
attributional style is called hypervigilance. In this study, an attempt to understand chronic pain is made using hypervigilance as part of a psychological model. The experiments are devised in hopes that the link between hypervigilance and chronic pain can be more firmly established. The hypothesis is that by using manipulations explained later, hypervigilance will be induced in healthy college students. Once this cognitive bias is introduced into the student it is predicted that they will respond to pressure pain in ways more similar to chronic pain patients than controls. Ideally, this line of research could lead to the development of more successful treatments of chronic pain which include a cognitive model that goes beyond chemical
approaches. Perhaps if both the mind and body are considered in the treatment of chronic pain patients a more permanent solution may be found to ending their suffering.
Previous Studies on Hypervigilance
noises, respectively. This line of research eventually culminated into the development of the General Hypervigilance Hypothesis (GHH), (McDermid, Rollman, & McCain 1996). This hypothesis argued that such awareness of distress leads to increased symptom reporting and hypochondriasis.
Yet another line of research, found in a chapter of a book about the psychology of physical symptoms, claimed that the pattern of increased symptom reporting (and therefore the cognitive bias) which is associated with hypervigilance can be induced in healthy participants (Pennebaker, 1982). Attentional manipulations, such as amplifying the sounds of an individual’s breathing as she runs, were able to make participants more aware of their bodies. In this
example, the manipulation changed the subject’s tendency to detect noxious sensations such as cramping (Pennebaker, 1982). However, it is important to note that this study did not appear in a peer reviewed article. Altogether, these studies showed that hypervigilance could be induced and this hypervigilance would lead to a generalized perceptual amplification (Chapman 1978).
The idea that hypervigilance is indicative of a cognitive bias was pursued further with the proposal of the Generalized Hypervigilance Hypothesis (GHH), as mentioned before. According to this more formal theory, hypervigilance is a perceptual habit that involves subjective
amplification of a variety of aversive sensations such as loud noises and annoying stimuli, not just painful ones (McDermid et al., 1996). To gather evidence for this claim, patients with fibromyalgia (a population with significant recorded hypervigilance) were compared to patients with rheumatoid arthritis and healthy controls based on their response to both tactile and auditory stimuli. This was done under the assumption that patients with fibromyalgia patients had
significantly more hypervigilance than arthritis patients who had significantly more
hypervigilant had increased sensitivity to noxious stimuli that are both internal (pain) and external (audio) in nature. Concurrent research showed that the different way in which pain patients respond to pain stimuli is likely attributable to hypervigilance rather than personality factors alone. This solidifies that it was variance in hypervigilance rather than some personality factor that lead to group differences in pain perception (Rollman & Lautenbacher, 1993). These studies provide evidence that cognitive bias changed both the expectation and experience of pain.
Work from the Hollins Lab
In an attempt to gain further insight into the nature of hypervigilance, Hollins and
colleagues (2009) investigated the claims of the GHH over a broad range of stimulus intensities. In this study, fibromyalgia patients and patients with temporomandibular disorders were
compared to healthy controls in a weighted rod task. In this task, a series of different weights were placed on the dorsal side of participants’ forearms in random order. After each weight, the participant rated the intensity and unpleasantness of the weighted rod sensation. Additionally, a similar experiment was conducted using increasingly loud sounds. Perceptual amplification in hypervigilant pain patients was found to occur across a wide range of both tactile and auditory intensities. The interesting result is that the expected amplification effect was not confined to unpleasant stimuli. This challenges the GHH’s assertion that the cognitive bias only involves noxious stimuli. According to these results, hypervigilance seems to be a cognitive pattern that leads to manipulation across modalities and intensities. Leading up to the current study,
Unlike the research previously discussed, the present study is unique in that it focuses on inducing hypervigilance in healthy participants and tests for a resulting amplification of tactile pain perception across a large range of intensities. Similar prior research was limited in that it only analyzed the tendency of people with induced catastrophization to show increases in expected and perceived pain as well as demonstrate an increased incidence of escape behaviors using a cold presser task (Severeijns, van den Hout & Vlaeyen, 2005). This research did not, however, directly measure the amplification of the pain perception itself. According to the logic employed by Severeijns et al. (2005), changing a person’s expectation of pain would change the experience of pain itself. However, this study did not gather conclusive findings, and their data did not support this claim. Though a small amount of catastrophization was induced, the experimental group actually demonstrated less escape behavior. In spite of these results, this study was an important conceptual stepping stone because it was the first to manipulate healthy subjects. With all this knowledge, the stage is set to manipulate subjects in order to induce hypervigilance rather than pain catastrophization.
Another recent study analyzed the relationship between interoceptive sensitivity and pain perception (Pollatos, Füstös, & Critchley, 2012). Similar to hypervigilance, interoceptive
sensitivity is defined as awareness of internal stimuli on a general level, but unlike
pain perception, the research by Pollatos (2012) supports the hypothesis that increased pain reporting can be related to a testable psychological trait such, as believed in the current study. Though there was no experimental manipulation by Pollatos (2012), the study sets this important precedent about attentional qualities and pain perception as measured in a lab environment. As this he demonstrates, enhanced sensitivity to autonomic state is accompanied by an increased likelihood of perceiving pain. It was believed in the design of the current study that this enhancement could be trained via counting task.
Preliminary Research
In a preliminary study conducted in the lab on healthy participants an attempt at inducing hypervigilance was made by asking those in the experimental condition to count three internal stimuli: their blinks, breaths and heartbeats in three separate tasks. This design used the rationale supported in the previous section by Pollatos (2012). Those in the control condition performed temporally equivalent tasks focused on external rather than internal stimuli. These included counting flashes on a computer screen from black to white and beeps through headphones in separate tasks. These induction tasks were followed by a weighted rod task in which a rod with weights of 77-1077g were placed on the dorsal forearm of participants. Eleven weights were used in increments of 100g in the range given; the weights were applied in a different random order for each participant in separate trials. After each trial, the participants were subsequently asked to report on the sensations evoked by these stimuli in terms of unpleasantness and intensity from 0-100. On these scales 0 means no intensity or unpleasantness at all and 100 means the most intense or unpleasant sensation imaginable. The participants also reported a word choice describing the weight as either neutral, unpleasant but not painful, or painful. During the
performed twice. As a manipulation check, participants completed the Five Factor Model Questionnaire for mindfulness (Gill & Hodgkinson, 2007) and the Pennebaker Inventory of Limbic Languidness (Pennebaker, 1982) both before and after the experimental phase.
The manipulation for the preliminary study did not produce a significant difference of the amount of hypervigilance between groups nor did it show group differences in the perceptions of the weighted rod. Groups were only significantly different on scores of mindfulness (t(22) = 1.780 p = .032) while measures of hypervigilance did not arrive at significance (t(22) = 0.786, p = 0.401). Additionally, no results were significant when comparing questionnaire scores on the pre and post-tests. Likely, this is the case because data was collected over the course of an hour and a half and participants could simply remember the answers they originally responded with on all questionnaire measures. While the difference in painfulness ratings between groups
approached significance (t(22) = 1.691, p = .074) there was no evidence that hypervigilance was induced according to the manipulation check, so no causal arguments could be made. The purpose of the current study is to improve upon the design of the preliminary research by more effectively inducing hypervigilance with a writing task. The current design was forged such that it did not rely on a pre/post-test approach to questionnaire testing in hopes to find more
significance.
The Present Study
collecting questionnaire data once, as the last step in a subject’s participation. Also, though the participants in the preliminary study were asked to become more aware of their bodies via the counting tasks, the extent to which this induced hypervigilance was limited. This may be because it was not associated with health concerns (Pennebaker, 1982). Therefore, an additional
manipulation was devised to draw attention to the body in a way that relates more to health and distress in the body. This was manifested in the form of a writing task in which participants wrote for 10 minutes about preparing for flu season. Members of the control condition wrote about the contents of their morning routines. In the flu condition, the prompt included facts and figures about the consequences of the flu and a general description of symptoms. The rationale for this writing prompt task derives from the work of a previous honors student from the Hollins lab, Kara Thio. In her research, Kara Thio (2013) used essay prompts to effectively induce different sorts of positive affect before subjecting participants to a cold presser task to test how pain tolerance was affected.
With these additions it was hoped that a more salient manipulation could be completed and more useful questionnaire data would be collected. The weighted rod task remained the same as before, but was only carried out once.
Methods
Participants
Individuals were recruited from the Introductory Psychology participant pool at the University of North Carolina at Chapel Hill. Students are required to participate in
participants would answer questions about themselves and judge pressure applied to a certain part of the arm. Participation in the study was compensated with 60 minutes toward the experimentation requirement.
Participation in the study was restricted to college students ages 18 to 25. Additional exclusionary criteria included any injury or neurological damage affecting the right forearm, and diagnosis of diabetes. These exclusions were put in place in order to avoid interference with the completion of the pressure task and to avoid distortions in the data of pain perception. It was necessary to have “healthy participants” for the sake of the manipulation of the experiment. Unlike previous research which primarily focused on individuals currently suffering from chronic pain, this study seeks to understand hypervigilance by inducing it; therefore, it was necessary to exclude any participants with interfering conditions. Any students under the instruction of Dr. Mark Hollins, the faculty advisor of the study, were also excluded from participation. The study sample consisted of 48 participants, 30 female and 18 male. Of whom, 23 participated in the control condition and 25 participated in the experimental condition. The average age of participants was 19.5. The sample includes 28 White, 14 Asian, 5 Black and 1 American Indian participant. There was one non-archival (practice) subject that was not considered in data calculations. Subjects provided written informed consent for all procedures. All aspects of the study were approved by the University’s IRB.
Stimuli
to respond to a writing prompt about how they prepare for flu season. Included in the prompt were statistics about the frequency and health outcomes of those with the flu. This prompt was chosen specifically to increase the subject’s cognitions about health concerns in relation to the self. Increased attention toward health-related stimuli, has been documented as a facet of hypervigilance (Pennebaker, 1982). It was believed that by asking the participant to have these thoughts, the magnitude of induced hypervigilance would increase. Individuals in the control condition were asked to respond to a prompt about their morning routines which was similar in length and composition. Both prompts are included in Appendix A.
The counting tasks were different between the experimental and control conditions, just as in the previous study. In the experimental condition, participants were asked to count their blinks, breaths and heartbeats (without palpating to check pulse). Members of the control condition counted visual stimuli created using Discotheek software in place placed the
physiological counting tasks. Discotheek is a program that can command a computer screen to change from white to black at a rate comparable to the rate of breathing, 15 breaths per minute (Holcomb et al., 2005). Auditory stimuli were also counted in the control condition. The two auditory stimuli were created using midi-files. One file contained high-pitched pulses which occurred at a rate comparable to the rate of blinking, 15 blinks per minute (Holcomb et al., 2005). The other file contained low-pitched pulses which occurred at a rate analogous to an average resting heart rate, 65 beats per minute (Holcomb et al., 2005). All pulses and blinks were programed to occur at random intervals to correspond with average rates.
To administer tactile pressure and pain, a weighted vertical rod was used. The rod was designed with a round Delrin tip approximately 5mm2 in diameter which rested on the dorsal
aluminum attached to the top of the rod allowed weights to be added to manipulate total force applied to the forearm. Total, there were 11 applied weights which ranged from 77g to 1077g in 100g intervals. A partition blocked the subject’s view of the simulator and of the stimulated region of the arm. Between trials the rod was moved so that the area did not become tender and bias pain ratings over the course of the many trials.
Procedure & Measures
Upon entrance to the lab, the participants were informed about the nature of the study and gave informed consent. Each subject was then randomly assigned to either the experimental or the control condition. Subsequently, participants completed three blocks of tasks in this order: the writing task, the counting tasks and finally the cutaneous pressure tasks. This was followed by completion of the questionnaire measures. Both the writing task and questionnaires were incorporated into on Qualtrics survey. Upon completion of the experiment, participants were debriefed and granted PSYC 101 experiment participation credit.
The final task to be completed was the cutaneous pressure task. The subject positioned their right forearm in the apparatus, resting it on a small pillow as well as layers of cardboard and cloth to ensure an appropriate height for appropriate contact with the weighted rod. The task consisted of one presentation of each of the 11 weight levels in a different random order for each subject. Each trial began with the lowering of the weighted rod onto the skin, over the course of about 1s. It was left in place for 15s, and then was raised off the skin over the course of an additional second. The subject was then asked to report the sensation produced by the rod on three scales, using verbal report. The first rating was of the intensity of the sensation caused by the stimulus on a 0–100 scale, with 0 representing “no sensation at all” and 100 indicating “the most intense sensation imaginable”. The participant was then asked to classify the stimulus as “painful, unpleasant but not painful, or neutral”. Finally, the subject gave a second numerical rating, this time of the unpleasantness of the sensation, from 0 (“not at all unpleasant”) to 100 (“the most unpleasant sensation imaginable”). The experimenters moved the subject’s forearm slightly between trials, to prevent repeated stimulation of the same site as previously explained.
Finally, subjects completed several psychometric instruments, in order: a Current Pain Questionnaire (Appendix B), the Pennebaker Inventory of Limbic Languidness (PILL)
(Pennebaker, 1982), the Pain Catastrophizing Scale (PCS) (Severeijns et al., 2005), the Speilberger State-Trait Anxiety Inventory (STAI) (Spielberger & Gorsuch 2013), and a
Statistical Analysis
In cases regarding questionnaire measures (PILL, STAI, and PCS) the control and
experimental groups were compared using independent-sample t-tests. This test was also used to compare unpleasantness threshold and pain threshold by experimental group (as well by gender), as defined in the next section. However, an 11 by 2 mixed-model ANOVA was used when ratings in the weighted-rod task were being compared across intensity levels as separated by group. Additionally, correlations (Person’s r) were used to investigate relationships between scores on the questionnaire measures. Also, correlations were used to assess gender as a factor regardless of condition in ratings of pain and unpleasantness ratings as well as in questionnaire scores. Alpha was set to 0.05 for each test. Individual estimates of sensation intensity and unpleasantness were converted into logarithmic form, as is normally done in ratio scaling experiments (Gescheider, 2013).
Results
Questionnaire Measures
were also not significant differences between the groups for current pain t(46) = .467, p = .522, would have allowed for better support of the hypotheses. This is true because it would mean that the groups were similar enough in pain background to be validly compared for responses to induced hypervigilance.
However, this was not possible because the groups were also not significantly different in terms of their PILL scores, t(46) = 1.067, p = 0.292. As recommended by Pennebaker, a person’s score on this instrument was the number of items (such as ‘‘headaches” or ‘‘sweat even in cold weather”) which the participant reported experiencing at least ‘‘every month or so” (Pennebaker, 1982). This means that the double manipulation did not effectively induce hypervigilance in participants in the experimental condition; therefore, no real conclusions about the effects of hypervigilance in healthy subjects can be made. Finally, there was no difference between groups on the PCS either, t(46) = 1.042, p = 0.303, meaning that the manipulations did not change the way that subjects thought about or interacted with their experience of pain. When separating groups by gender, regardless of manipulation, there was only a significant difference between groups for the PILL, t(45.7) = 2.393, p = 0.021 (equal variance not assumed).
Pressure Rod Data
Though analysis of PILL data did not indicate that hypervigilance was induced,
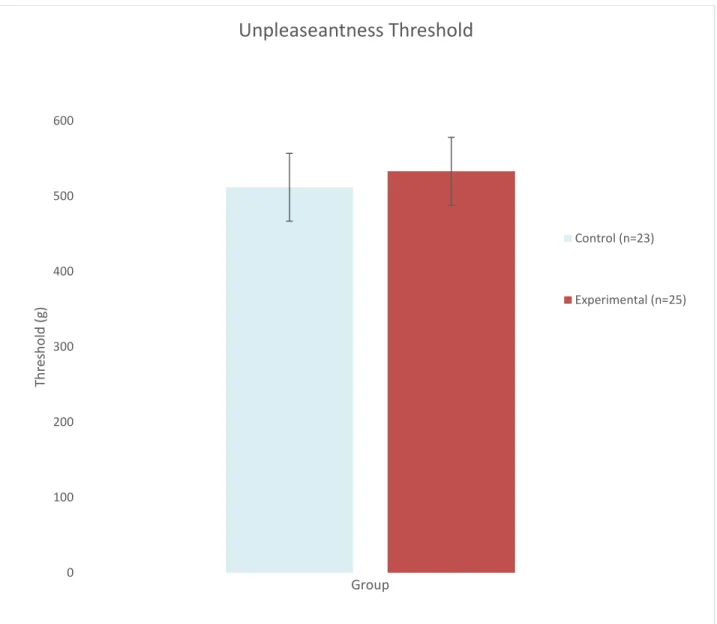
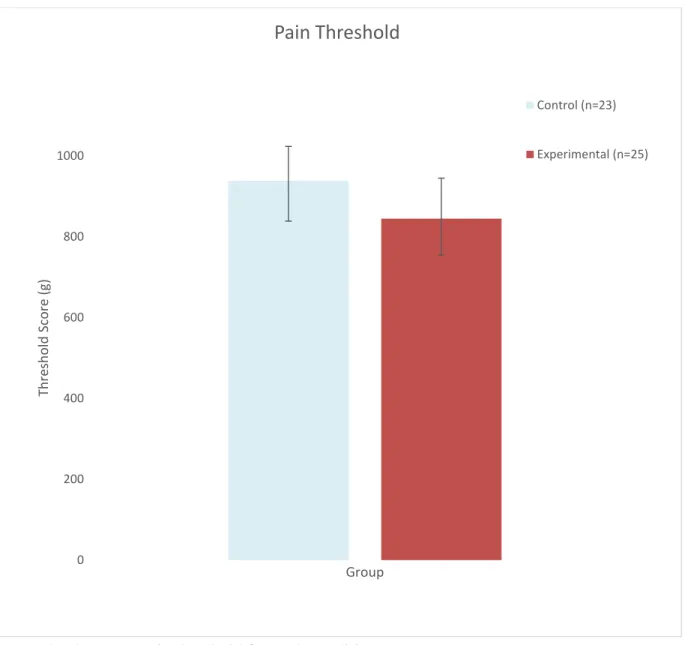
that hypervigilance was not induced and the groups showed no difference in response to the weighted rods. Figure 1 and Figure 2 illustrate the mean unpleasantness threshold and mean pain threshold for each group, respectively. The number of participants who rated specific stimuli as either unpleasant or painful can be found in Figure 3 and Figure 4, respectively. The graphs often overlap, conveying little difference between the two groups. When comparing groups by gender, regardless of condition, there were no significant differences between groups for thresholds of unpleasantness or pain.
Results of the ANOVAs were consistent with the threshold analyses. As expected. the effect of weight was significant, F(11, 36) = 39.44, p < 0.000, meaning that subjects did rate heavier weights as being both more unpleasant and more intense in both conditions. However, the analyses for main effect for group for intensity rating (F(11, 36) = 0.993, p = 0.471) or unpleasantness rating (F(11, 36) = 0.895, p = 0.554) were insignificant. This means that while subjects in both conditions responded to heavier weight with more sensation of intensity and unpleasantness, those in the induced hypervigilance condition did not do so in a way that demonstrates any amplified perception compared to controls. Further, analysis of one-way ANOVAs for pressure stimulus reveal that there was not a significant difference between groups for any of the 11 weight amounts for either intensity rating of unpleasantness rating.
Correlational Analysis
Correlations of questionnaire measure scores with one another as well as with
p = 0.007), but state anxiety was never correlated to PILL scores. As discussed later, this may provide evidence about the nature of the manipulation tasks used. Additionally, in all groups state and trait anxiety were correlated at a p < 0.001 level (r = 0.732 overall), which was
expected. Curiously, it was found that PILL and PCS scores were only significantly correlated in the experimental group (r = 0.473, p = 0.017), but not overall among participants or in the control group. This may make pain catastrophization a confounding variable. However, these results are inconclusive because t-tests revealed no significant differences between groups for any of these measures.
The final correlational result considered, was that both unpleasantness threshold and pain threshold were negatively correlated with PILL scores, PCS scores, trait anxiety and state
anxiety. However, these are only significant in the control condition. Again, because of t-test results these findings help explain expected trends but are not definitive.
Discussion
This study aimed to further establish the link between hypervigilance and chronic pain in hopes that inducing hypervigilance in healthy subject would lead to a demonstration of
perceptual amplification such as found in chronic pain patients. It was predicted that if
reasoning for the failure of the manipulation will be discussed in addition to what adaptations could be made to improve the experiment for the future. It is important to learn from every shortcoming.
It would be easy to make a one-dimensional, sweeping judgment about the insignificance of the data. However, there is no way of truly assessing these hypotheses with the data collected. There is no supporting evidence to claim that hypervigilance was induced because there were no real group differences on the PILL or PCS. Because of this, it cannot be known if the lack of an effect of experimental condition for ratings of intensity and unpleasantness ratings with changing weight was due to the lack of induced hypervigilance or due to a real weakness in the
relationship between levels of hypervigilance and tactile perception which would counter the second hypothesis mentioned. However, a claim can be made about the quality of
hypervigilance. It seems that, unlike interoceptive sensitivity and pain catastrophization, hypervigilance is not easily induced in a lab setting. It is possible that the cognitive and attentional biases associated with hyperviglance build up overtime and are the product of an accumulation of life experiences that cannot be imitated in a lab setting. Further, there has been previous criticism of the PILL as a measure of hypervigilance, as it is singularly a list of
responses regarding the frequency of experiencing symptoms (Van Damme et al., 2009).
odds with the consideration that women were shown to be induced for hypervigilance at rates significantly higher than men.
Correlational analysis also revealed some interesting facets of the data. The first is that trait anxiety and PILL score were correlated regardless of group. This result indicates that the manipulation used did not likely induce anxiety in the participants, but that it is possible that those who are generally more anxious as a trait were more easily induced to have increased hypervigilance. The fact that PCS scores and PILL scores were correlated in the experimental group only may it indicate that the manipulation induced an increase of pain catastrophization which may confound any effects from hypervigilance. The result that questionnaire measures only significantly negatively correlated with unpleasantness and pain threshold in the control group is troubling. This counteracts the hypothesis that the manipulation would decrease thresholds for pain and unpleasantness as compared to the control group. Though it must be established that these correlations have barely reached significance. The correlations between threshold and anxiety/pain catastrophization may also indicate confounding variables.
There were no differences between the groups for pain threshold or unpleasantness threshold. Again, this likely occurred by virtue of the lack of a successful manipulation of induced hypervigilance. It is important to consider that the literature support substantiating that hypervigilance can be induced is imperfect. Pennebaker (1982) was the only source to claim that hypervigilance would be induced, but this experiment was published as a chapter in a book, not a peer reviewed article. Additionally, Pollatos (2012) did successfully manipulate health subjects, but this research was focused on interoceptive sensitivity, which is not the same thing as
log ratings of unpleasantness for the log force of each weight overlap between the groups as weight changes. This is also true for log mean painfulness ratings, as seen in Figure 6. These graphs show that the samples were essentially the same as one another, though those in the experimental group did show slightly higher log mean ratings for intensity.
The manipulation’s inability to attain a difference between the groups on scales of hypervigilance and tactile perception highlight some of the limitations of this study. An important shortcoming is that in the hopes of having a strong double-dose of manipulation by asking experimental subjects to take part in both the writing and counting manipulations there were only two groups. With this design, there was no way to differentiate between how much, if any, hypervigilance was induced by each manipulation on its own. This shortcoming was largely the result of the nature of completing an honors project. There was not sufficient time to collect enough data for four groups of participants, which is what would be needed to make this analysis. A better study would take place over a longer period of time and allow for this sort of statistical analysis.
lead to variance in the results that is attributable to anxiety and fear, but this is what the STAI is for. This test can parse out just how anxious participants were and allow researchers to consider that as a variable to remove from analysis.
There were a considerable amount of subjects in both conditions failed to rate even the most heavy weighted rod task as painful or unpleasant. Moreover, not even a single subject had ratings completely accurate when mapping actual weight to perceived intensity and
unpleasantness. In other words, no subject’s responses for unpleasantness and intensity aligned with the weight numbers in numerical order. Considering these things, it is likely that a better test of tactile perceptual amplification would include more intense (heavier weights) and have intervals greater than 100g so that participants are more likely to accurately differentiate between the weights. Without stimuli that cause mild to moderate pain in each participant, it is not
possible to accurately study the relationship between chronic pain, hypervigilance and perception in healthy people that is the focus of this entire study. Also, there were anchoring effects in how participants rated the sensations. For example, if the first weight in a subject’s random order was 977g (the second heaviest) and they happened to respond with a low intensity, they would never likely rate any stimulus with a high intensity. Conversely, if the first weight experiences was very light, they participants tended to rate the heavier weights as more intense and unpleasant regardless of condition.
References
Allen, H., Hubbard, D., & Sullivan, S. (2005). The burden of pain on employee health and productivity at a major provider of business services. Journal of Occupational and Environmental Medicine, 47(7), 658-670.
Chapman, C. R. (1978). Pain: The perception of noxious events. In R. A. Sternbach (Ed.), The psychology of pain (pp. 169-202). New York: Raven Press.
Gescheider, G. A. (2013). Psychophysics: the fundamentals. Psychology Press.
Gill, C. M., & Hodgkinson, G. P. (2007). Development and validation of the Five Factor Model Questionnaire (FFMQ): An adjectival-based personality inventory for use in
occupational settings. Personnel Psychology, 60(3), 731-766.
Holcomb, J. B., Salinas, J., McManus, J. M., Miller, C. C., Cooke, W. H., & Convertino, V. A. (2005). Manual vital signs reliably predict need for life-saving interventions in trauma patients. Journal of Trauma and Acute Care Surgery,59(4), 821-829.
Hollins, M., Harper, D., Gallagher, S., Owings, E. W., Lim, P. F., Miller, V., Siddiqi, M. Q., & Maixner, W. (2009). Perceived intensity and unpleasantness of cutaneous and auditory stimuli:An evaluation of the generalized hypervigilance hypothesis. Pain, 141, 215-221.
Hollins, M., Harper, D., & Maixner, W. (2009). Response to the letter to the editor by Van Damme and Colleagues. Pain, 144, 343-344.
Nes, L. S., Roach, A. R., & Segerstrom, S. C. (2009). Executive functions, self-regulation, and chronic pain: a review. Annals of Behavioral Medicine,37(2), 173-183.
Pennebaker, J. W. (1982). The Psychology of Physical Symptoms. New York: Springer-Verlag. Chapters 1 and 2, and Appendix B.
Pollatos, O., Füstös, J., & Critchley, H. D. (2012). On the generalised embodiment of pain: How interoceptive sensitivity modulates cutaneous pain perception. Pain, 153, 1680-1686.
Rollman, G. B., & Lautenbacher, S. (1993). Hypervigilance effects in fibromyalgia: Pain experience and pain perception. In H. Værøy & H. Merskey (Eds.), Progress in fibromyalgia and myofascial pain (Vol. 6). Amsterdam: Elsevier.
Severeijns, R., van den Hout, M., & Vlaeyen, J. W. S. (2005). The causal status of pain catastrophizing: an experimental test with healthy participants. European Journal of Pain, 9, 257-265.
Spielberger, C. D., & Gorsuch, R. L. (2013). State-trait Anxiety Inventory for Adults: Instrument (adult Form) and Scoring Guide. Mind Garden.
Thio, Kara (2013). The Effects of Pride and Admiration on Pain. Retrieved from Dissertation and Theses database at the University of North Carolina at Chapel Hill.
Turk, D. C., & Monarch, E. S. (1996). Biopsychosocial perspective on chronic
pain. Psychological approaches to pain management: A practitioner’s handbook, 3-32
Appendix A
Writing Instructions for Each Condition Experimental Condition:
The flu is a contagious respiratory illness caused by influenza viruses that infect the nose, throat, and lungs. The disease is quite contagious and can be spread through the air by coughing or sneezing. It can cause mild to severe illness, and in extreme cases can be fatal. The flu is especially common during the colder months of the year, known as “flu season.” In fact, it is estimated that the virus kills more than 55,000 people annually in the United States, more than any other infectious disease. Fortunately, there are steps most people can take to greatly reduce their chances of contracting the flu, although no one measure provides complete protection. We would like you to think about the things you do on a regular basis to ward off the flu, especially as flu season approaches and throughout the winter months. Some of these things may be actions that you plan, whereas others may be small things that you do without thinking about it.
After you have reflected on this subject, you will be asked to write about it. Please describe your actions as vividly and in as much detail as you can for about 10 minutes. This page contains the text box in which you may write your story. There is no need to worry about spelling or
grammar – we are just interested in finding out more about your actions in everyday life. This writing task is completely confidential; if you mention individuals, feel free to use pseudonyms instead of real names. We are just interested in your narrative, which will be kept for data analysis.
Please write your story in the text box below:
Control Condition:
After you have reflected on this subject, you will be asked to write about it. Please describe your actions as vividly and in as much detail as you can for about 10 minutes. This page contains the text box in which you may write your story. There is no need to worry about spelling or
grammar – we are just interested in finding out more about your actions in everyday life. This writing task is completely confidential; if you mention individuals, feel free to use pseudonyms instead of real names. We are just interested in your narrative, which will be kept for data analysis.
Please write your story in the text box below:
Appendix B
Current Pain Questionnaire
Complete Questions 1-5 with a number on a 0-100 scale:
Over the past two weeks…
1. The average intensity of your pain over the past two weeks _______
2. The average unpleasantness of your pain over the past two weeks _______
3. On average, what percentage of your waking day do you have pain? ______%
4. The intensity of your current pain ______
5. The unpleasantness of your current pain _______
6. What is the location of your current pain (check all that apply):
Head or neck ____ Back ____ Chest ____ Abdomen ____
Left arm ____ Right arm ____
Left hand ____ Right hand ____
Left leg or foot____ Right leg or foot____
7. Do you have chronic pain (pain that has lasted more than 3 months)? ________
If so, please describe. ______________________________________________
Table 1
Mean (and standard deviation) for Hypervigilance, Pain Catastrophizing and State/Trait Anxiety post manipulation
Questionnaire Measure Group
Control Experimental
PILL 16.8 (9.5) 14.1 (7.7)
PCS 24.4 (8.1) 22.4 (4.9)
STAI-S 33.4 (8.9) 32.6 (8.67)
STAI-T 40.56 (12.1) 38.6 (8.8)
Figure 1. The mean unpleasantness threshold for each condition. 0
100 200 300 400 500 600
Th
re
sh
o
ld
(g)
Group
Unpleaseantness Threshold
Control (n=23)
Figure 2. The mean pain threshold for each condition. 0
200 400 600 800 1000
Th
re
sh
o
ld
Score
(g)
Group
Pain Threshold
Control (n=23)
Figure 3. The number of participants in each condition that rated each force as unpleasant. 0
2 4 6 8 10 12 14 16 18
-0.2 0 0.2 0.4 0.6 0.8 1 1.2
N
u
m
b
er
o
f Su
b
jec
ts
Log Force (N)
Unpleasantness Ratings
Experimental (n=25)
Figure 4. The number of participants in each condition that rated each pressure as painful. 0
2 4 6 8 10 12 14 16
-0.2 0 0.2 0.4 0.6 0.8 1 1.2
N
u
m
b
er
o
f Su
b
jec
ts
Log Force (N)
Pain Ratings
Experimenal (n=25)
Figure 5. Mean log intensity as a function of the force exerted on the forearm by the weighted rod.
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8
-0.2 0 0.2 0.4 0.6 0.8 1 1.2
Lo
g Se
n
sat
ion
In
ten
sity
Log Force (N)
Log Mean Intensity vs. Log Force
Experimental (n=25)
Figure 6. Mean log unpleasantness as a function of the force exerted on the forearm by the weighted rod.
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8
-0.2 0 0.2 0.4 0.6 0.8 1 1.2
Lo
g Se
n
sat
ion
U
n
p
le
asan
tn
es
s
Log Force (N)
Log Mean Unpleasantness vs. Log Force
Experimental (n=25)