Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6593
Volume||5||Issue||06||June-2017||Pages-6593-6605||ISSN(e):2321-7545 Website: http://ijsae.in
Index Copernicus Value- 56.65 DOI: http://dx.doi.org/10.18535/ijsre/v5i06.14
Effectiveness of Skill Training Programme on Knowledge and Practice of ANM(R)s
regarding IUCD services in selected subcentres of Birbhum District, West Bengal.
Authors:
Anita Bag1, Prof. Smritikana Mani2, Ananya Bhakta3
1
M.Sc. Nursing (Obstetrical and gynaecological nursing) Clinical Instructor, Govt. College of Nursing, Burdwan Medical College & Hospital, The West Bengal University of Health Sciences.
2
R.N.R.M, M Phil Nursing,M.Sc. Nursing (Obstetrics and gynaecological nursing) Principal, College of Nursing, Medical College and Hospital, Kolkata-73. The West Bengal University of Health Sciences.
3
M.Sc. Nursing (Community health nursing speciality),UG Gold medalist, College of Nursing, Medical College and Hospital, Kolkata-73, The West Bengal University of Health Sciences.
Email- [email protected], [email protected], [email protected]
ABSTRACT
Introduction: The population is not static, but is always in a dynamic state. The current approach in family planning is to offer high quality contraceptive services among eligible clients on a voluntary basis. Another important component of the programme is to promote adequate spacing of births. To challenge with the risks e.i.- population growth, high level of MMR and high level of IMR intrauterine contraceptive method is a backbone of the family planning programmes. Worldwide the Intrauterine Contraceptive Device (IUCD) is one of the most commonly used reversible methods of contraception among woman of reproductive age which is needed for population stabilization.
Objectives: To find out the effectiveness of skill training programme on knowledge and practice of ANM(R)s regarding IUCD services in selected subcentres of Birbhum District, West Bengal.
Materials & method: A quasi-experimental research approach and Pretest Posttest control group design was used for the study. Conceptual framework adopted for the study was based on general system model. Purposive sampling followed by simple random technique was used to select 40 ANM(R)s from two BPHCs namely Nanoor BPHC and Labhpur BPHC. A content was developed for the skill training programme and skill training was provided by using an anatomical model through simulation technique. A structured questionnaire to collect demographic variables, a knowledge questionnaire to assess knowledge, an observation checklist to observe practice and an opinionnaire to determine the opinion of ANM(R)s regarding skill training programme were developed.
Results: The findings of the study revealed that there was significant difference between pretest and posttest knowledge scores {‘t’(19) = 15.42, p<0.05} and practice scores {‘t’ (19) = 41.31, p<0.05} of experimental group. The study also revealed that there was significance difference between posttest knowledge scores {‘t’ (39) = 9.73, p<0.05} and practice scores {‘t’ (39) = 39.2, p<0.05} of experimental and control group. Conclusion: Therefore the study concluded that skill training programme was effective in increasing the knowledge and practice of ANM(R)s regarding IUCD services and thus had implications in the field of nursing practice, nursing education, nursing administration and nursing research.
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6594
INTRODUCTION:
The population is not static, but is always in a dynamic state. The factors involved in population dynamics are death, birth and migration. The world population was only 250 millions at the beginning of the Christian era, nearly 2000 years ago1. But gradually the population increased and in the last 10 years world population has increased very rapidly.
Earlier in the last century the rate of world population increase was about 10 million per year, but now the rate of population increase in the world is 100 million per year. If this increase rate continues then the projected population of 2025 is 8000million or 8 billion2.
The current approach in family planning is to offer high quality contraceptive services among eligible clients on a voluntary basis. Another important component of the programme is to promote adequate spacing of births. The principal objective of the national population policy 2000 is addressing the unmet need for contraception to bring down the Net Fertility Rate to 1 so as to achieve the long term goal of population stabilization by 20453.
To challenge with the risks e.i.- population growth, high level of MMR and high level of IMR intrauterine contraceptive method is a backbone of the family planning programmes. Worldwide the Intrauterine Contraceptive Device (IUCD) is one of the most commonly used reversible methods of contraception among woman of reproductive age which is needed for population stabilization and spacing between children. Results of recent studies have shown that IUCDs provide very effective, safe, short term as well as long term protection against pregnancy and the health risks associated with the method are negligible too. IUCD is a best spacing method as well as it is an effective reversible method. Its failure rate is only 0.8% in the first year of use. Use of IUCD is inexpensive to the community people as CuT380A is distributed free of cost through Government channel3.
In India only 1.8% of married women of reproductive age use IUCDs (Figure-3). Despite the fact that the Government offers IUCD services free of cost, it still remains largely underutilized in India3.
Figure 1: Showing IUCD usage in India VS other methods Source: The third National Family Health Survey; 2005-2006.
A study was conducted at Ghana in 2008 by Ghana Demographic Health Survey. Before this study, they found that 25% of married women of the age group of 15-49 used contraceptive method, but only 4% used long acting method like IUCD (0.9%), female sterilization (1.9) and implant (1%). The study used a pre- and post-test quasi-experimental design with two intervention groups and one comparison group. There were two interventions in the study. The interventions were: 1) training of Community Health Officers (CHOs) and community volunteers in conducting educational activities focused on creating awareness of IUCD and interest in IUCD; and 2) improving the CHO’s IUCD insertion and removal skills. Data were collected by household survey for both assessments4.
ANM(R)s are working in community, directly with the grassroots. They are the first person who will guide the eligible couples about contraception. They are the core person who will provide IUCD services directly
0.00% 10.00% 20.00% 30.00% 40.00%
1.80% 3.10% 5.30%
37.30%
1%
Contraceptive methods
P
er
ce
nt
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6595 to the eligible couples. So it is essential to provide up-to-date information and knowledge to make them skilled regarding counselling, medical eligibility criteria, client assessment, IUCD insertion, IUCD removal, infection prevention, follow up and management of potential problems.
The investigator during working in public health as a BPHN, observed that the knowledge and skill of ANM(R)s regarding IUCD were very poor. Not practicing counselling before and after insertion of IUCD was a major cause of high rate of removal. Poor knowledge and skill on medical eligibility criteria resulted in high rate of complications among the women receiving IUCD. The wrong method of ANM(R)s in insertion and removal of IUCD was the cause of infection, expulsion, perforation, contraception failure etc. Not using sound to measure uterine length resulted in high expulsion rate and perforation. Not cleaning of the cervix and vaginal wall before insertion of the IUCD was the cause of high rate of infection. Not loading the IUCD within the sterile package resulted in a high rate of infection. Not using withdrawal technique in releasing the IUCD into the uterus, rather pushing the plunger rod to release IUCD in the uterus would result in perforation. So the investigator was interested from her clinical field to conduct the present study and to find out the effectiveness of skill training programme on knowledge and practice of ANM(R)s regarding IUCD services assuming that the skill training programme would increase the knowledge and skill of ANM(R)s which would be resulted in providing quality services and ultimately in population stabilization.
OBJECTIVES OF THE STUDY:
To assess the knowledge of ANM(R)s on IUCD services before and after introduction of skill training programme of both the experimental and control group.
To assess the practice of ANM(R)s on IUCD services before and after introduction of skill training programme of both the experimental and control group.
To find out the relationship between post-test knowledge and practice on IUCD services of experimental group.
To find out association between post test knowledge and practice with selected demographic variables in experimental group.
To determine the opinion of ANM(R)s regarding skill training programme.
METHODOLOGY:
The research approach used for the present study was quasiexperimental. The pre-test post-test control group design was used in the present study.
E K1 P1 X K2P2
C K 3P3 _ K 4P4
Symbolic presentation of research design E- Experimental group
C- Control group
K1-pretest of experimental group on knowledge
P1- pretest of experimental group on practice
K2- posttest of experimental group on knowledge
P2 - posttest of experimental group on practice
K3 – pretest of control group on knowledge
P3 – pretest of control group on practice
K4 – post test of control group on knowledge
P4 – post test of control group on practice
X – Skill training on knowledge and practice using anatomical model.
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6596 followed by simple random technique as a study subject from the above selected settings. The data collection tool consists into three parts. Knowledge questionnaire, observation checklist and structured opinionaire. In the structured knowledge questionnaire it contains 5 items for collecting demographic data and 25 items for assessing the knowledge of ANM(R) regarding IUCD Services. Observation Checklist comprised of 6 areas, those are pre insertion, insertion, insertion, pre-removal, removal and post-removal areas. The pre-insertion area was consisted of six items, insertion area was consisted of 34 items, post-insertion area was consisted of 16 items, pre-removal area was consisted of 2 items, removal area was consisted of 17 items and post-removal area was consisted of 5 items. Validity of the toll was done and reliability was calculated. The reliability of the tool were1, 0.84 and 0.97 respectively. The data was collected from the study subject by maintaining confidentiality and by taking informed conscent. The Opinionnaire consisted of ten statements on opinion regarding the skill training programme. There were seven positive statements and three negative statements. There were three columns against the statements namely, ‘agree, partially agree and disagree’.
RESULTS:
The majority (77.5%) of ANM(R)s are in the age group of 31 to 40 years. In the control group majority (55%) of ANM(R)s belong to age group of 31-40 years whereas (100%) of experimental group belong to this as group. In respect of religion majority (75%) of the ANM(R)s were Hindu. In the control group most (80%) of the ANM(R)s were Hindu and in the experimental group (70%) of them were Hindu.All the ANM(R)s were married. Most of the ANM(R)s (90%) of control group had 7-12 months of experience in their service as well as most of the ANM(R)s (85%) in experimental group had 7-12 months of experience in service.
Maximum ANM(R)s (45%) had secondary education. N=40
Figure 2: Bar diagram showing area wise mean percentage of post-test knowledge score of control group and experimental group.
0.00% 20.00% 40.00% 60.00% 80.00% 100.00%
54.29% 60% 60%
35%
60% 55%
32% 45%
35% 90% 95% 95%
77.50% 95%
90%
79% 75% 85%
Control group Experimental group
m
e
an
p
e
rce
n
ta
ge
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6597 Figure 2 reveals that the mean percentage post-test knowledge score of experimental group is higher than the mean percentage post-test knowledge score of control group in each area. In the area of description of IUCD the mean percentage post-test knowledge score was 90% whereas in control group it was 54.29%, in the area of counselling it was 95% in experimental group and 60% in control group, in the area of medical eligibility criteria it was 95% in experimental group and 60% in control group, in the area of client assessment it was 77.5% in experimental group and 35% in control group, in the area of IUCD insertion it was 95% in experimental group and 60% in control group, in the area of IUCD removal it was 90% in experimental group and 60% in control group,in the area of infection prevention it was 79% in experimental group and 32% in control group, in the of follow up it was 75% in experimental group and 45% in control group and in the area of management of potential problems the mean percentage post-test knowledge score was 85% in experimental group and 35% in control group.
N=40
Figure 3: Frequency polygon showing the distribution of posttest knowledge scores between experimental and control group.
The frequency polygon in figure 3 indicates the distribution of post-test knowledge score on IUCD services among experimental and control group with the depiction of mean and median. The frequency polygon of post-test knowledge scores of experimental group ranges from 15 to 25with the mean 21.6 and median 22.25 and the maximum frequency 8 lies in the class interval 22 to 24, whereas the frequency polygon of posttest knowledge scores of control group ranges from 5 to 17with the mean 11.85 and the median 11.5 and the maximum frequency 9 lies in the class interval 10 to 12. The maximum scores of experimental group lies in the right side of the control group indicating that the scores of experimental group increased.
n=20
0 1 2 3 4 5 6 7 8 9 10
1-3 4-6 7-9 10-12 13-15 16-18 19-21 22-24 25-27 28-30
Fr
e
q
u
e
n
cy
Knowledge Score of ANM(R)s
control group
experimental group
control group mean-11.85 median-11.5 experimental group mean-21.6 median-22.25
mean
median
0% 20% 40% 60% 80% 100% 120%
C
u
m
m
u
la
ti
ve
f
re
q
u
e
n
cy
p
e
rcent
ag
e
Knowledge Score
Pretest Posttest
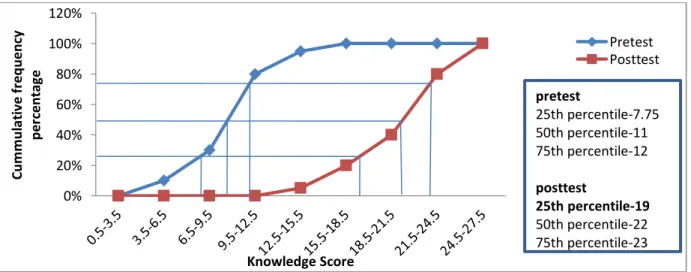
pretest
25th percentile-7.75 50th percentile-11 75th percentile-12
posttest
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6598
Figure 4: Ogive showing the distribution of pretest and post test knowledge score of experimental group. The ogive in figure 4 shows that the post-test knowledge scores of experimental group lies to the right of the pretest knowledge scores of experimental group indicating that the scores of posttest were increased.
Table 1: ‘t’ value showing difference of pretest knowledge of experimental and control group. N=40
Group Mean Mean
difference
SDD SEMD ‘t’ value
Experimental 10.5
0.4 3.19 1.02 0.392
Control 10.9
‘t’ (df38) = 2.02, P< 0.05.
Data given in table 1 depict that the obtained mean difference in the pretest knowledge score of experimental and control group was not found to be statistically significant as evident from calculated ‘t’ value 0.392 for df38 at 0.05 level of significance.
Table-2: ‘t’ value showing difference of post test knowledge of experimental and control group N=40
Group Mean Mean
difference
SDD SEMD ‘t’ value
Experimental 21.6
9.75 3.13 1.0016 9.73*
Control 11.85
‘t’ (df38) = 2.02, P< 0.05. *
Data given in table2 show that the obtained mean difference in the posttest knowledge score between control and experimental group of ANM(R)s is found to be statistically significant as evident from calculated ‘t’ value 9.73 for df38 at 0.05 level of significance.
Table 3:‘t’ value showing difference of pre test and post-test knowledge of experimental group n=20
Group Mean Mean
difference
SDD SEMD ‘t’ value
Pretest 10.5
11.1 3.223 0.72 15.42*
posttest 21.6
‘t’ (df19) = 2.09, P< 0.05. **
Data given in table 3 show that the obtained mean difference in pretest and posttest knowledge score of experimental group is found to be statistically significant as evident from calculated ‘t’ value 15.42 for df19
at 0.05 level of significance.
Table 4:‘t’ value showing difference of pre test and post-test knowledge of control group n=20
Group Mean Mean
difference
SDD SEMD ‘t’ value
Pretest 10.9
0.95 2.35 0.503 1.9
Posttest 11.85
‘t’ (df19) = 2.09, P< 0.05.
Data given in table 4 show that the obtained mean difference in pretest and posttest knowledge scores of control group was not found to be statistically significant as evident from calculated‘t’ value1.9 for df19 at
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6599 N=40
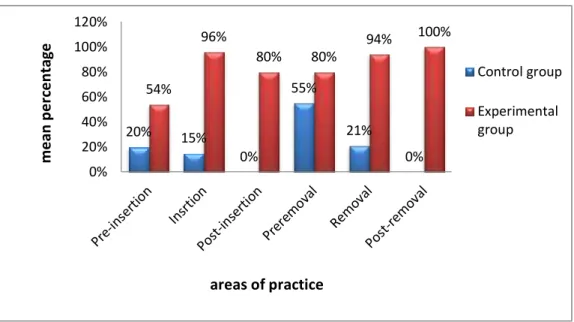
Figure 5: Bar diagram showing the area wise mean percentage of post test practice score in experimental and control group.
Data presented in figure 5 reveals that the mean percentage post-test practice score of experimental group was higher than the mean percentage post-test practice score of control group in each area. The mean percentage posttest practice score in preinsertion area was 54% in experimental group whereas it was 20% in control group. In insertion area it was 96% in experimental group whereas it was only 15% in control group. In post insertion area the mean posttest practice score was 80% in experimental group and 0% in control group, in preremoval area it was 80% in experimental group and 55% in control group, in removal area it was 94% in experimental group and 21% in control group and in the post removal area it was 100% in experimental group and 0% in control group. So the skill training programme was effective to improve practice of ANM(R)s on IUCD services.
N=40
Figure 6: Frequency polygon showing the distribution of posttest practice scores between experimental and control group.
Data presented in figure 6 depict that. the frequency polygon of posttest practice scores of experimental group ranges from 60 to 80 with the mean 71.25 and median 71 and the maximum frequency 6 lies in the class interval 66 to 70 and 71 to 75, whereas the frequency polygon of posttest practice scores of control group ranges from 7 to 18 with the mean 11.6 and the median 11 and the maximum frequency 9 lies in the class interval 6 to 10.The figure also depicts that in control group mean lies to the right of the median, so distribution is positively skewed and the skewness (0.563) is negligible indicating the scores are normally distributed. 0 1 2 3 4 5 6 7 8 9 10 1 --5 6 --1 0 1 1 --1 5 1 6 --2 0 2 1 --2 5 2 6 --3 0 31 --3 5 3 6 --4 0 4 1 --4 5 4 6 --5 0 51 --5 5 5 6 --6 0 6 1 --6 5 6 6 --7 0 7 1 --7 5 7 6 --8 0 8 1 --8 5 control group experimental group fr e q u e n cy
practice score of ANM(R)s
control group mean=11.6 median=11 experimental group mean=71.25 median=71 mean median
20% 15%
0% 55% 21% 0% 54% 96%
80% 80%
94% 100%
0% 20% 40% 60% 80% 100% 120% Control group Experimental group
areas of practice
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6600 n=20
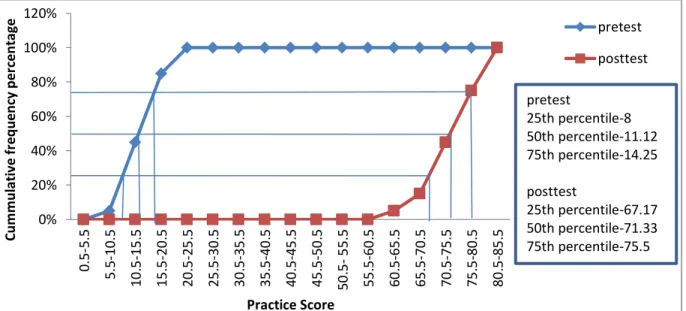
Figure 7: Ogive showing cumulative frequency percentage of pretest and posttest practice score of experimental group.
The ogive in figure 7 shows that the post-test practice scores of experimental group lies to the right of the pretest practice scores of experimental group indicating posttest practice scores were increased than pretest practice scores.
Table 5:‘t’ value showing difference of pre-test practice score of control group and experimental group. N=40
Group Mean Mean difference SDD SEMD ‘t’ value
Experimental 11.35
0.25 3.53 1.1296 0.22
Control 11.1
‘t’ (df38) = 2.02, P< 0.05.
Data given in table 5 show that the obtained mean difference in the pre-test practe score of experimental and control group was not found to be statistically significant as evident from calculated ‘t’ value 0.22 for df38 at
0.05 level of significance.
Table 6:‘t’ value showing difference of post test practice score of experimental and control group N=40
Group Mean Mean
difference
SDD SEMD ‘t’ value
Experimental 71.25
59.6 4.75 1.25 39.02**
Control 11.65
‘t’ (df38) = 2.02, P< 0.05. ** highly significant
Data given in table 6 show that the obtained mean difference in the posttest practice score between control and experimental group of ANM(R)s is found to be statistically significant as evident from calculated ‘t’ value 39.02 for df38 at 0.05 level of significance.
Table 7: ‘t’ value showing of difference of pretest and post test practice of experimental group n=20
Group Mean Mean difference SDD SEMD ‘t’ value
Pretest 11.35
59.9 6.49 1.45 41.31**
Posttest 71.25
‘t’ (df19) = 2.09, P< 0.05. ** Highly significant.
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6601 Data given in table 7 show that the obtained mean difference in the pretest and posttest practice score of experimental group was found to be statistically significant as evident from calculated ‘t’ value 41.31 for df19 at 0.05 level of significance.
Table 8: ‘t’ value showing difference of pre-test and post test practice of control group n=20
Group Mean Mean
difference
SDD SEMD ‘t’ value
Pretest 11.1
0.55 1.57 0.35 1.57
Posttest 11.65
‘t’ (df19) = 2.09, P< 0.05.
Data given in table 8 show that the The obtained mean difference in the pretest and posttest practice score of control group was not found to be statistically significant as evident from calculated‘t’ value 1.57 for df19 at
0.05 level of significance.
Table 9: Coefficient correlation between posttest knowledge and practice of experimental group. n=20
Score Mean Coefficient correlation
Posttest knowledge 21.6
0.3
Posttest practice 71.25
‘r’ df18= 0.44, P<0.05.
Data present in table 9 depict that the mean posttest knowledge was 21.6 and the mean posttest practice was 71.25. Coefficient co-rrelation was calculated and it was 0.3. The calculated r value of is 0.3 for df18 at 0.05
level of significance.
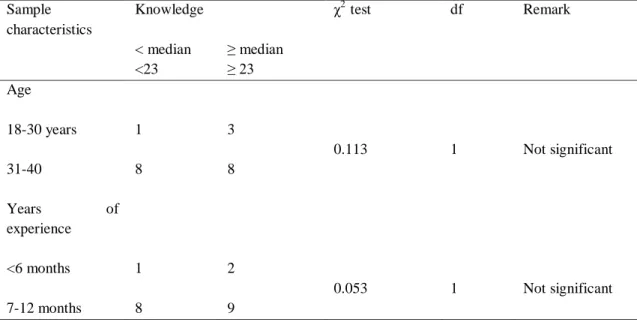
Table 10: χ2 value between posttest knowledge level of experimental groups and demographic variables. N=20
Sample characteristics
Knowledge χ2 test df Remark
< median <23
≥ median ≥ 23 Age
18-30 years 1 3
0.113 1 Not significant
31-40 8 8
Years of
experience
<6 months 1 2
0.053 1 Not significant
7-12 months 8 9
χ2
df1 =3.841, p<0.05.
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6602
Table 11: χ2 value between posttest practice level of experimental groups and demographic variables N=20
Sample characteristics
Knowledge χ2 test df Remark
< median <71
≥ median ≥ 71 Age
18-30 years 1 3
0.113 1 Not significant
31-40 8 8
Years of
experience
<6 months 1 2
0.053 1 Not significant
7-12 months 8 9
χ2
df1 =3.841, p<0.05.
Data presented in table 11 depict that there was no significant association present between post test knowledge with demographic variables.
N=40
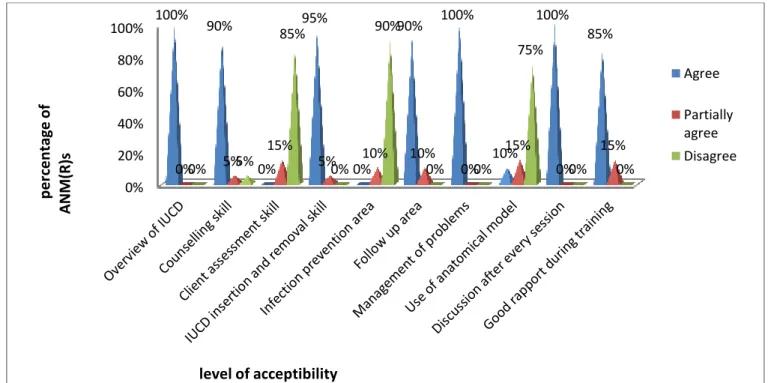
Figure 8: Bar diagram showing percentage of agree, partially agree and disagree of the statements of opinionnaire regarding skill training programme on IUCD services.
DISCUSSION:
The present study was consistent with the study conducted on repositioning IUCD in public health programme in India. One objective of the study was to enhance the acceptability of the IUCD among providers. It was a pre test post test experimental design with no control group. The study clearly shows that the training helped in improving both technical and counseling skills of the workers and it was reflected in significant improvements in the quality of the services provided by the workers5.
The result of present study also revealed that the training helped in enhancing skill of ANM(R)s regarding IUCD services on counselling, medical eligibility criteria, client assessment, infection prevention, follow up
0% 20% 40% 60% 80%
100% 100% 90%
0%
95%
0%
90% 100%
10%
100% 85%
0% 5%
15%
5% 10% 10% 0%
15% 0%
15%
0% 5%
85%
0%
90%
0% 0%
75%
0% 0%
Agree
Partially agree Disagree
p
e
rce
n
ta
ge
o
f
A
N
M
(R)
s
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6603 and management of potential problems as it was evidentfrom ‘t’ value (41.31) at df(19) at 0.05 level of
significance.
The study was consistent with the study conducted at Honduras (2001) on Expansion of the Role of Nurse Auxiliaries in the Delivery of Reproductive Health Services. Nurse auxiliaries who work at the rural health centres of the Honduran Ministry of Health (MOH) are frequently the only source of reproductive health services in the communities they serve. In order to increase access to long-term family planning methods a study was conducted by Honduran MOH. The MOH and the Population Council conducted a study to see if nurse auxiliaries could provide good quality IUCD without health risks for their clients. The study findings concluded that knowledge and skill of auxiliaries were increased adequately, so they could provide these services after proper training6.
Results of the present study also revealed that knowledge and skill of auxiliaries could be increased adequately by providing training as evdent by ‘t’ value of pretest posttest knowledge score (15.42) at df(19) at
0.05 level of significance and ‘t’ value of pretest posttest practice score (41.31) at df(19) at 0.05 level of
significance.
The present study was consistent with the study conducted by Limpaphayom K, Ajello C, Reinprayoon D, Lumbiganon P, Gaffikin L. on effectiveness of model-based training in accelerating IUD skill acquisition. Comparison of a competency-based IUD insertion training approach and the traditional training model indicated that the alternative approach is both feasible and cost-effective for developing country settings. There were control group and experimental group. In experimental group training was given by using an anatomical model and in control group without an anatomical model by using traditional approach. It was found that both the total cost and cost per competent learner were significantly higher in the traditional group due to the longer training period. The study observed that without compromising the quality of client care, the alternative training approach significantly decreases the time midwives must spend away from clinics for training, the number of clients needed for clinical practice, and training costs7.
In the present study training was given by using an anatomical model and the skill training programme was highly effective to increase knowledge and skill of ANM(R)s regarding IUCD in a short time and low cost. The model based training increased both the knowledge and skill of ANM(R)s as evident by ‘t’ value of pretest posttest knowledge score (15.42) at df(19) at 0.05 level of significance and ‘t’ value of pretest posttest
practice score (41.31) at df(19) at 0.05 level of significance. So the present study can concluded that model
based training could be effective to increase knowledge and practice of ANM(R)s on IUCD and they could be able to provide quality client care.
The present study was inconsistent with the study conducted by David Hubacher, Rosa Vilchez, Rebecca Gmach, Carlos Jarqui, Jose Medra, Auxiliadora Gadea, Tom Grey on The impact of clinician education on IUCD uptake, knowledge and attitudes: results of a randomized trial in 2006. Many ministries of health worldwide would like to increase use of the intrauterine device (IUCD) since it is very safe, effective and inexpensive to provide. A randomized trial was conducted among 40 clinics in Nicaragua to test the impact of medical education on both IUCD uptake and on provider knowledge/attitude toward the method. Two types of interventions were used: face-to-face medical training/education of providers and/or provision of an IUCD checklist to help clinicians assess the medical eligibility of clients. The interventions had no impact on uptake of the IUCD or on provider knowledge/attitude8.
Result of the present study concluded that training had impact on provider knowledge. The knowledge of providers increased as evident by t value of pretest and posttest knowledge score (15.42) at df(19) at 0.05
level of significance.
CONCLUSION
The following conclusions were drawn on the basis of findings:
Anita Bag et al IJSRE Volume 05 Issue 06 June 2017 Page 6604 The content was helpful to increase knowledge.
The observation checklist was accepted by the participants and it was helpful to increase skill in IUCD services which was observed by simulation technique.
The skill training programme was effective to increase knowledge and practice of ANM(R)s on IUCD services.
For skill training programme the simulation tecnnique, that is use of an anatomical model was useful to imcrease knowledge and skill.
Limitations
The limitations of the study were
Since the sample was limited to only ANM(R)s of two BPHCs, generalization of the findings is limited. The practice was introduced and observed by simulation technique with an anatomical model not on real sample.
Recommendations
The study can be replicated on a large samples for generalizations.
A similar study may be conducted in other areas like newborn resuscitation, neonatal assessment, post natal check up, intranatal care, waste management in labour room etc.
The study can be conducted on real cases.
An evaluative study on the services of ANM(R)s on IUCD insertion after receiving training can be conducted.
This study also can be conducted on staff nurses working at family planning units.
A descriptive study can be conducted to find out the factors for underutilization of IUCD.
A survey study can be conducted to identify the myths and misconception regarding IUCD in a community. A comparative study can be conducted to find out the effectiveness with model based training and training in real cases.
Based on findings of the present study a project can be initiated by the Government of India on IUCD training of the ANM(R)s, GNM, B.Sc.Nursing and also in M.SC. Nursing curriculum
Evaluation of existing practical components of ANM(R)s on IUCD can be done with a view to bring about innovative changes in the curriculum.
REFERENCES:
1. Park K. Text Book of Preventive and Social Medicine. 20th ed. Jabalpur: M/s Banarsidas Bhanot; 2009.
2. Dutta DC. Text Book of Obstetrics. 6th ed. Calcutta: New Central Book Agency(P) LTD; 2004. 3. IUCD Reference Manual for Medical Officers. New Delhi: Family Planning Division, Ministry of
Health and Family welfare, Government of India; 2007.
4. Ivy Osei, Gertrude Voetagbe, Moses Aikins, John Gyapong, Philomena Nyarko, Harriet Birungi et al. September 2008. http://pdf.usaid.gov/pdf_docs/PNADN581.pdf.
5. Repositioning of IUD in Public Health Program in India [internet]. 2008. Repositioning IUCD in the Family Welfare Programme. New Delhi: Family Planning Division, Ministry of Health and Family welfare, Government of India; 2008Available from:
http://www.k4health.org/system/files/modelworks.pdf.
6. Expansion of the Role of Nurse Auxiliaries in the Delivery of Reproductive Health Services in Honduras. [internet]. 2001. Available from: http://www.k4health.org/toolkits/iud/expansion-role-nurse-auxiliaries-delivery-reproductive-health-services-honduras.