5.1.7 Identify any physical development limitations (e.g. space) 5.1.8 Determine whether provision of services for families of drug
25
0
0
Full text
(2) 5.1 Assessing development needs and constraints Consider: Understanding the prevailing, and projected, development and delivery needs and constraints for family focussed interventions/services is vital. Not only should it enhance the design of an intervention or service (giving it the best possible chance of meeting its' defined aims, objectives and outcomes), but it is also an important way of achieving best value and, as such, will help secure any necessary funding. However, the assessment process is ideally a 360° exercise and should also include an assessment of known, or likely, constraints.. Suggested Good Practice. = Immediate implementation desirable. Assessing needs. 5.1.1. Avoid making the assumption that the service development needs and constraints of your agency/establishment/service users are identical to those of other agencies/establishments/service users. Though there are bound to be some similarities, circumstances (and, therefore, needs) are rarely identical. Carry out a formal needs assessment exercise to establish actual needs.. 5.1.2. Use anecdotal information (e.g. feedback from prison, treatment and family support service staff) to highlight potential need. 5.1.3. Use findings from formal research/consultation and/or ongoing monitoring and evaluation mechanisms to determine actual need (Feedback relating to current services and possible development needs can be gathered locally via comments and suggestions forms and boxes in: Visitors' Centres; visits waiting rooms; community agencies or, more widely, by including feedback forms in information packs and other resources etc. sent/given to families). 5.1.4. Consider the needs associated with certain issues that may be more prevalent amongst certain groups and/or prison profiles. (See 5.5 - Diversity). 5.1.5. Ensure the diverse needs/circumstances of families in relation to culture, ethnicity, religion, language, age, disability, gender, sexuality and other differences are identified. (See 5.5 - Diversity). 5.1.6. Ensure those taking part in consultation processes are given the opportunity to receive feedback about findings and recommendations. ✓. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✗. 39.
(3) 5.1 Assessing development needs and constraints. Suggested Good Practice. = Immediate implementation desirable. Assessing constraints. 5.1.7. Identify any physical development limitations (e.g. space). 5.1.8. Determine whether provision of services for families of drug users is consistent with your organisational remit/ethos. 5.1.9. Determine whether provision of services for families in their own right is consistent with your organisational remit. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✓. ✗. 40.
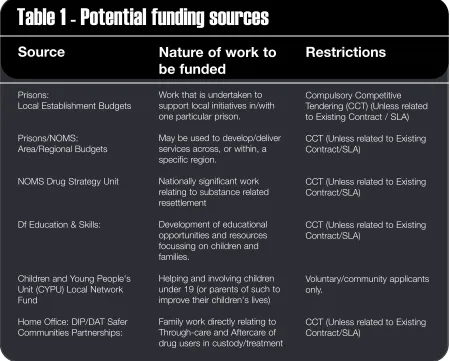
(4) 5.2 Raising funds for family work Consider: Many 'core' activities detailed in this Toolkit should not require additional finance to support them as they will probably involve amendment to existing practice rather than development of completely new work. Where additional funding is required, there are a number of options to explore. A basic overview of these is given at Table 1. Where development is collaborative/in partnership, the most appropriate lead funding applicant depends on who/what the funding is for, and from where it is being sort. (This usually depends on the nature and location of work to be undertaken.) In some cases, funding for individual components of one entire project may need to be sought from different sources. Examples of these are given at Table 2.. Suggested Good Practice. = Immediate implementation desirable. Raising funds for family work. 5.2.1. Use established evidence (Research/Needs Assessment) and current policy to support funding applications.. 5.2.2. Aims and objectives should be Specific Measurable Achievable Realistic and Time bound. (S.M.A.R.T.). 5.2.3. Create a full and realistic Income and Expenditure Budget showing all expected costs and any anticipated/secured sources of income. 5.2.4. Before submitting bids for collaborative work, ensure that all parties have formally agreed the timescales and budgets for work they will be responsible for delivering. 5.2.5. Do not confuse the aim of fundraising activities with those of promotional events. Ensure your budget for costs of holding an activity or event includes everything (from staff time to stationery and phone calls) if you intend/need to make a net profit (i.e. raise funds). 5.2.6. Consider asking prisoners to hold fundraising activities to support the work of family services. 5.2.7. If the member of staff drafting a funding application is inexperienced, consider asking someone with fundraising experience/success to act as a fundraising mentor, or to review the application before it is submitted.. 5.2.8. Consider investing in specialist training for staff required/expected to fulfil a fundraising role - however limited. ✓. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✗. 41.
(5) 5.2 Raising funds for family work. Suggested Good Practice Raising funds for family work. ✓. 5.2.8. Consider investing in specialist training for staff required/expected to fulfil a fundraising role - however limited. 5.2.9. Consider any ethical implications there may be when applying for funds. (e.g. would you want to accept funding from a company that has been connected to bad employment/investment practices in the developing World?). 5.210. Consider holding 'open' events to inform potential funders about your existing work and how any proposed developments would complement it. ✗. Table 1 - Potential funding sources Source. Nature of work to be funded. Restrictions. Prisons: Local Establishment Budgets. Work that is undertaken to support local initiatives in/with one particular prison.. Compulsory Competitive Tendering (CCT) (Unless related to Existing Contract / SLA). Prisons/NOMS: Area/Regional Budgets. May be used to develop/deliver services across, or within, a specific region.. CCT (Unless related to Existing Contract/SLA). NOMS Drug Strategy Unit. Nationally significant work relating to substance related resettlement. CCT (Unless related to Existing Contract/SLA). Df Education & Skills:. Development of educational opportunities and resources focussing on children and families.. CCT (Unless related to Existing Contract/SLA). Children and Young People's Unit (CYPU) Local Network Fund. Helping and involving children under 19 (or parents of such to improve their children's lives). Voluntary/community applicants only.. Home Office: DIP/DAT Safer Communities Partnerships:. Family work directly relating to Through-care and Aftercare of drug users in custody/treatment.. CCT (Unless related to Existing Contract/SLA). Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 42.
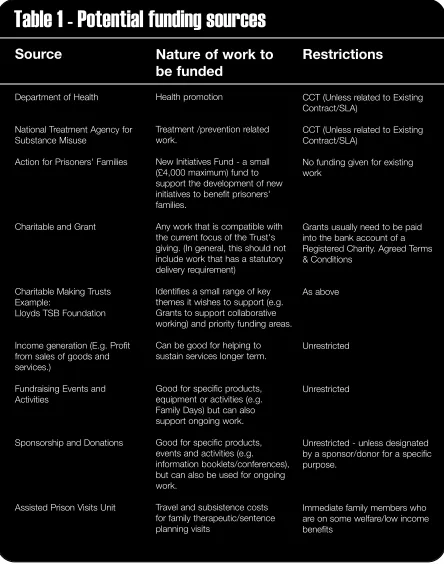
(6) 5.2 Raising funds for family work. Table 1 - Potential funding sources Source. Nature of work to be funded. Restrictions. Department of Health. Health promotion. CCT (Unless related to Existing Contract/SLA). National Treatment Agency for Substance Misuse. Treatment /prevention related work.. CCT (Unless related to Existing Contract/SLA). Action for Prisoners' Families. New Initiatives Fund - a small (£4,000 maximum) fund to support the development of new initiatives to benefit prisoners' families.. No funding given for existing work. Charitable and Grant. Any work that is compatible with the current focus of the Trust's giving. (In general, this should not include work that has a statutory delivery requirement). Grants usually need to be paid into the bank account of a Registered Charity. Agreed Terms & Conditions. Charitable Making Trusts Example: Lloyds TSB Foundation. Identifies a small range of key themes it wishes to support (e.g. Grants to support collaborative working) and priority funding areas.. As above. Income generation (E.g. Profit from sales of goods and services.). Can be good for helping to sustain services longer term.. Unrestricted. Fundraising Events and Activities. Good for specific products, equipment or activities (e.g. Family Days) but can also support ongoing work.. Unrestricted. Sponsorship and Donations. Good for specific products, events and activities (e.g. information booklets/conferences), but can also be used for ongoing work.. Unrestricted - unless designated by a sponsor/donor for a specific purpose.. Assisted Prison Visits Unit. Travel and subsistence costs for family therapeutic/sentence planning visits. Immediate family members who are on some welfare/low income benefits. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 43.
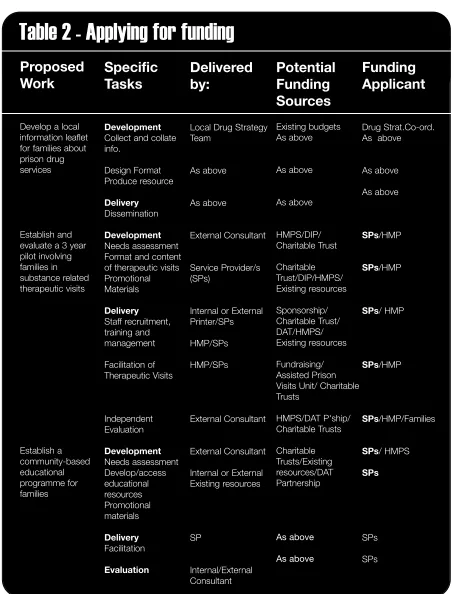
(7) 5.2 Raising funds for family work. Table 2 - Applying for funding Proposed Work. Specific Tasks. Delivered by:. Develop a local information leaflet for families about prison drug services. Development Collect and collate info.. Local Drug Strategy Existing budgets As above Team. Design Format Produce resource. As above. As above. Delivery Dissemination. As above. As above. Potential Funding Sources. Funding Applicant Drug Strat.Co-ord. As above. As above As above. Establish and evaluate a 3 year pilot involving families in substance related therapeutic visits. Establish a community-based educational programme for families. Development External Consultant Needs assessment Format and content of therapeutic visits Service Provider/s Promotional (SPs) Materials. HMPS/DIP/ Charitable Trust. SPs/HMP. Charitable Trust/DIP/HMPS/ Existing resources. SPs/HMP. Delivery Staff recruitment, training and management. Internal or External Printer/SPs. Sponsorship/ Charitable Trust/ DAT/HMPS/ Existing resources. SPs/ HMP. Facilitation of Therapeutic Visits. HMP/SPs. Fundraising/ SPs/HMP Assisted Prison Visits Unit/ Charitable Trusts. Independent Evaluation. External Consultant. HMPS/DAT P'ship/ Charitable Trusts. SPs/HMP/Families. Development Needs assessment Develop/access educational resources Promotional materials. External Consultant. SPs/ HMPS. Internal or External Existing resources. Charitable Trusts/Existing resources/DAT Partnership. Delivery Facilitation. SP. As above. SPs. As above. SPs. Evaluation. Internal/External Consultant. HMP/SPs. SPs. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 44.
(8) 5.3 Commissioning and funding Consider: The acknowledged benefits of supporting families, both in their own right and as part of a user's treatment plan, should not be underestimated. The health, employment, educational, financial and social welfare of individuals and whole families can all be adversely affected by problematic drug use and imprisonment. The commitment of commissioners, and Charitable Trusts, to be both realistic and flexible when funding work with families is vital - not only to reduce the levels of current and future drug use, but to minimise the negative impact of it on others. Useful related documents: We Count Too - Home Office/Adfam/PADA/FAMFED Getting it Right Together - Prison Service/CLINKS. Suggested Good Practice. = Immediate implementation desirable. Commissioning and funding. 5.3.1. Prisons, Drug Action Teams, Primary Care Trusts, Social Services, Crime and Disorder/Safer Communities Partnerships should reference the need for, and provision, of family services in strategic reviews and planning processes. 5.3.2. Only those services that meet established need, and identified gaps, in service provision should be commissioned/funded (Where existing services are insufficiently funded to meet need, or promote services, consider capacity building funding). 5.3.3. Services that are commissioned/funded should be required to demonstrate that they are delivered in accordance with relevant quality standards and legislation and levels of funding should be set to ensure that these can be maintained. 5.3.4. Services to engage and involve families in reducing drug supply, demand and harm should be commissioned/funded to be delivered at appropriate prison or community based sites. 5.3.5. Family focussed services should aim to meet the needs of families in their own right, not only as part of a user's treatment plan. 5.3.6. The range of services commissioned/funded should reflect the diverse needs of families within the locality/region. 5.3.7. Prisons that commission services from volunteer agencies (or individual volunteers) should expect to meet reasonable travel, subsistence and support costs for volunteers. ✓. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✗. 45.
(9) 5.3 Commissioning and funding. Suggested Good Practice Commissioning and funding. 5.3.8. Restrictions on locally based family services should not require that imprisoned drug users are held (or intend to reside) in the same area as family members accessing service. 5.3.9. Consider commissioning/funding/facilitating feasibility studies to explore partnership/joint working potential. ✓. ✗. 5.3.10 Where required funding for a project, or piece of work, cannot be provided by one funding body alone, that body should actively seek to involve other funding partners in joint commissioning/funding arrangements where appropriate. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 46.
(10) 5.4 Joint working Consider: Just as prisons have limited experience in providing services for families (and does not have a specific remit for doing so), many community based families and/or substance related agencies have limited understanding of the issues involved in prison work. It is, therefore, likely that there will be a need for collaborative relationships/partnerships (with agencies who have more relevant experience and/or expertise) to be formed in order to develop and deliver effective services and interventions aimed at involving families. Bringing together the variety of cultures, practices and experiences that exists within the statutory, not-for-profit and commercial sectors can bring significant benefits, when managed well. However, it can also be very challenging and sometimes leads to suspicion, misunderstanding and confusion. This, in turn, can undermine the potential success of any project. It is vital, therefore, to address as many potential areas of conflict or concern during the development phase.. Suggested Good Practice. = Immediate implementation desirable. All services. 5.4.1. Joint Working Agreements (JWAs) or Service Level Agreements (SLAs) should be used to underpin agreed joint working practice and procedure between agencies - whether or not there is a financial relationship.. 5.4.2. JWAs/SLAs should detail each party's responsibility for facilitating/ delivering a service/resource (e.g. office space, equipment and maintenance, independent telephone and building access etc.). 5.4.3. JWAs/SLAs should include details for how the joint working arrangements and relationship will be monitored and reviewed (including review dates). 5.4.4. Before entering into a formal joint working relationship, ensure that there are clear, written, protocols in place for appropriate interagency sharing of information - particularly in relation to sensitive information. (See Appendix 7.3). 5.4.5. Prospective joint working partners should agree a Confidentiality Statement to be included in promotional literature and displayed in appropriate areas, e.g. visits, visitors' centres, service delivery areas.. 5.4.6. Where necessary, community based agencies should amend employment procedures to include the need for all staff working with prisoners' families (or having access to confidential information about them) to be security cleared in the same way - whether they are prison based or not. ✓. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✗. 47.
(11) 5.4 Joint working. Suggested Good Practice All services. 5.4.7. Reciprocal learning opportunities (shadowing/job swaps) should be developed. 5.4.8. Establishments and agencies should create and develop broad focus e-mailing lists (including all departments and agencies working in/with prisons) to promote training events that are appropriate for interagency participation. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✓. ✗. 48.
(12) 5.5 Diversity Consider: Despite natural similarities, there are many differences in personal custom, culture and experience that impact on individual reactions and responses to the drug use and imprisonment of a family member. Whilst some family members accept it as part of their user's (or their own) lifestyle, others feel traumatised by the experience. They can also suffer severe social stigma. Such differences can lead to people feeling they are not eligible to use, or able to find out about, services they need and to which they are entitled.. Family diversity: Below are some examples of diversity issues that should be considered when working to engage and involve family members. Culture, Ethnicity and Language: • Attitudes to, and understanding of, various substances (e.g. is alcohol viewed as more, or less, acceptable/harmful than some illegal substances) can vary significantly • Services and resources may not be culturally sensitive • Shame and stigma about drug use can be stronger in some communities • Major cultural/religious festivals do not necessarily coincide Age: • Significant numbers of young people may have been carers for a drug using parent or sibling • Specialist services and resources will be needed to help children and young people address fears and concerns about drug use • Older people (usually grand-parents) may be more likely to need help preventing/identifying onset of drug use amongst children they are caring for during the imprisonment of an adult 'child' • Elderly carers may have more health problems that limit accessibility Disability/Health: • Diversion of prescribed medication may be an issue • Access to services/events may be problematic for wheelchair, or otherwise mobility impaired, family members • Special equipment might be needed to enable families affected by sensory impairment to be engaged and involved • Procedures are needed for enabling sensitive health information to be shared between prisoners and families Gender: • Men and women tend to respond to different engagement methods, with men more likely prefer factual, information resources and women a more direct interpersonal approach • There may be gender issues may in relation to staffing • Societal/family attitudes often prevail in relation to use of particular substances by gender group (e.g. is it generally viewed as more acceptable for males to use alcohol regularly) • Substance related domestic violence predominantly affects women • Males often find it harder to acknowledge emotional distress. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 49.
(13) 5.5 Diversity Sexuality/Sexual identity: • Families - particularly those of young people in prison - may be impacted by the disclosure of previously unknown sexual identity or sexuality issues • Prisoners and/or families may feel inhibited, or fear discrimination, when disclosing or discussing issues of sexual identity or sexuality in group situations • The high incidence of previous sexual abuse experienced amongst prisoners may impact on the ability of some to form a positive sexual identity. Helping a prisoner to resolve this may result in difficulties within existing relationships. In addition, disclosure of previous sexual abuse involving family members or friends may give rise to child protection issues; family breakdown; violent reaction; self-harm etc.. Prison profile: When considering responses to meet diverse needs, it is also necessary to take account of different profiles within the prison estate. Certain needs will be greater, and services more appropriately delivered, in some prisons and circumstances than in others. Women's Prisons: • Women are more likely to be lone parents • Family members, particularly grandparents, are often caring for prisoners' children - sometimes as a result of imprisonment but also as a result of pre imprisonment parental substance use. (This can result in need for complex family dynamics problems - especially where legal proceedings over custody/residency have ensued - to be addressed) • Families may have more difficulty coming to terms with activities a woman has been involved in (e.g. prostitution to fund substance use) than the substance use itself • Maintaining, rather than detoxifying, a pregnant user can lead to confusion/frustration for families • Mother and Baby Units are also Voluntary Testing Units and, as such, access/residence is limited to those drug users who are a) abstinent or b) using prescribed medication only • Women are often held in prisons far from home and family • Male partners are more likely to be substance users Juvenile Training Centres & YOI: • Many young people have been/are in care and there may be long standing and complex family problems (including Child Protection issues) • There may be more need to work with extended family members, foster carers, Mentors and Social Workers • Use of alcohol, tobacco, cannabis and volatile substances may be more problematic than many Class A drugs • Parents and/or siblings may also be drug users Local Prisons: • Families may be traumatised and/or confused by their experiences/circumstances • Local supply networks are readily accessible and pressure may be exerted on families to access them • Newly imprisoned users may have drug debts that families are expected to pay - sometimes by dealing drugs to prisons Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 50.
(14) 5.5 Diversity Local Prisons (continued): • Families, and their addresses/personal circumstances, may be known to other visitors • Families may discover drug use for the first time when a user is imprisoned • Short sentences/remand may restrict prison based involvement opportunities Rurally Located Prisons: • Families may have significant difficulty travelling to participate in activities High Security Prisons: • There may be less potential for bringing families into the prison for family group-work due to security clearance issues • There may be additional security clearance issues for community staff • Sentences are usually longer and family relationships less sustainable • Long term prisoners may develop drug problems whilst in prison • Family contact and bereavement may be particular issues for prisoners serving long sentences. (They are more often supported by elderly, sometimes infirm, parents) • Prisoners (and visitors) may have more links to organised drug trafficking and/or criminal networks and have lifestyles and/or status they feel a need to maintain through continued criminal activity • Families under pressure may be more vulnerable to serious violence, but less trusting of authority. Useful related reading and documents: PSO 3630 The Race Relations (Amendment) Act 2000 - Commission for Racial Equality Children Acts 1989. Suggested Good Practice. = Immediate implementation desirable. Relationships. 5.5.1. ✓. ✗. Recognise, and value, the nature of different relationships within each family by defining and promoting the term 'FAMILY' as inclusive of all socially significant others, irrespective of birth relationships or legal status. Culture, ethnicity and language 5.5.2. Ensure that staff having contact with families are aware of, and sensitive to, varying family structures/relationships that exist across diverse cultural and ethnic groups. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 51.
(15) 5.5 Diversity. Suggested Good Practice. = Immediate implementation desirable. Culture, ethnicity and language. 5.5.3. Ensure that staff are aware of the attitudes and experiences within different cultures in relation to specific substances - including alcohol. 5.5.4. Ensure that images used in information and promotional materials reflect cultural/ethnic origins of the potential family client group. 5.5.5. Ensure that staff are sensitive to what constitutes appropriate contact between genders within some cultural and religious communities (e.g. some may not feel able to be supported by, or share a group situation with, members of their opposite gender). 5.5.6. Do not schedule family involvement events on dates that coincide with major religious and/or cultural festivals. 5.5.7. Ensure that a culturally appropriate food mix is provided during family involvement events. 5.5.8. Where possible, ensure the staff team reflects the ethnic and cultural balance of the service user group. 5.5.9. Provide general information in other relevant languages (Consult with specialist groups to ensure translation is culturally sensitive). ✓. ✗. 5.5.10 Consider the use of Peer Engagement and Involvement Workers 5.5.11 Where service users do not have English as their first language, no not make assumptions about their ability to read written English just because they speak it. If in doubt, check with them by using a phrase such as: “You speak English very well. Would it be OK for me to send/give you some written information in English, or would you prefer me to let you have/try and find it in (first language)?” 5.5.12 When a service user has a strong accent that you find difficult to understand (especially when they are emotional and may be speaking more quickly than usual), you need to address this. Perhaps you could say: “I need you to speak a little more slowly, please. Would it help if I did too? We have very different accents and I really want us to be sure we understand each other” 5.5.13 Where necessary and appropriate, use (security cleared) translators to enable non-English speaking families to be involved. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 52.
(16) 5.5 Diversity. Suggested Good Practice. = Immediate implementation desirable. Sexual identity and sexuality. ✓. ✗. 5.5.14 Do not make assumptions about the sexuality of family members, or the nature of their relationship with the prisoner or each other 5.5.15 Families (including prisoners) should be made aware that same sex partners have equal opportunities to access services aimed at involving family members in sentence planning and treatment 5.5.16 Ensure, where possible, that issues of family discord in relation to sexual identity/sexuality are addressed 5.5.17 Wherever possible, recruit staff of both genders and assign individual clients in accordance with their identified needs 5.5.18 Wherever possible, encourage positive role modelling by 'out' staff. Age 5.5.19 Provide/develop services and/or resources that are designed to meet the specific needs of children and young people at different developmental stages. (E.g. early years; 5-8, 9-12, 13-16 etc.). Disability/health 5.5.20 Consider offering services designed specifically for young carers 5.5.21 Do not assume that a disability, or serious health problem, is visible. Promote opportunities for family members to disclose relevant information about disability/health issues (e.g. the need to access medication at specific times; use of a hair piece following chemotherapy etc.) and ensure that any such information remains confidential and that identified needs are addressed sensitively 5.5.22 Provide general drug and security information for visitors (including arrangements for authorised use of prescribed and over-the-counter medication on premises) in writing and on audio tape 5.5.23 Conduct searches of disabled visitors and disability aids with sensitivity and, where necessary to preserve dignity, out of sight of other visitors 5.5.24 Ensure that key information is also posted at eye level height (for wheelchair users) and in disabled toilets. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 53.
(17) 5.5 Diversity. Suggested Good Practice. = Immediate implementation desirable. Disability/health. ✓. ✗. 5.5.25 Where they remain unlocked, and accessible for general use, ensure that disabled toilets are regularly inspected.(Less frequent use, and increased space, makes them particularly vulnerable to drug activity as users are/feel less likely to be interrupted) 5.5.26 Ensure that engagement and involvement services are accessible to family members who are mobility impaired 5.5.27 Offer a (security cleared) guide, or escort, for unaccompanied visually or mobility impaired family members visiting your premises 5.5.28 Where appropriate, try to use (security cleared) signers to enable hearing impaired family members to be involved. Literacy 5.5.29 Use stand alone video and/or audio cassettes to engage families and inform them of involvement opportunities 5.5.30 Utilise, or develop, pictorial information and messages for families who may have less well-developed literacy skills. Prison profile 5.5.31 Efforts should be made to engage families and give them access to appropriate involvement opportunities, irrespective of prison profile. (In addition to the more generalised approaches detailed in previous sections/Chapters, the following sections detail examples of the family focussed interventions and services that are particularly appropriate for engaging and involving families within specific types of prison) 5.5.31.1 - Women's Prisons • Family liaison • General drugs information for families including that which is SPECIFIC to female drug users (e.g. pregnancy and detoxification; Child Protection/Custody issues) • Parenting courses covering issues related to drug use and childcare from the point of conception (for Prisoners) • Drug related information and educational opportunities specifically for carers of prisoners' children • Pre release education and family liaison opportunities to identify and address issues relating to post release residency and childcare. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 54.
(18) 5.5 Diversity. Suggested Good Practice. = Immediate implementation desirable. Prison profile. ✓. ✗. 5.5.31.1 - Women's Prisons (continued) • Referral information and support opportunities to assist those families struggling with their feelings about their family member being involved in drug related prostitution 5.5.31.2 - Juvenile Training Centres • Family liaison • Greater emphasis on information about alcohol, tobacco and sexual health • Information for families about drug use and youth culture • Drug prevention/education information for young people (siblings/friends) • Information and support (including referral to specialist support groups) for families affected by Attention Deficit Hyperactivity Disorder (ADHD) • Drug education opportunities for grand/parents, foster carers and Mentors • Family mediation and case conferencing • Whole family drug awareness workshop opportunities (looking at the +/- influence of family culture/attitudes) • Parenting and drug use (parents/carers) • Referral of family members to community based drug services • Involvement of families in drug rehabilitation programmes • Information on YOIs and how to support transitional relapse prevention strategies 5.5.31.3 - Young Offender Institutions • Family liaison • Young parents and drug use education (for Prisoners) • Parenting and drug use (for offenders' parents/carers) • Referral of family members to community based drug services • Drug prevention/education information for young people (siblings/friends) • Information and support (including referral to specialist support groups) for families affected by Attention Deficit Hyperactivity Disorder (ADHD) Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 55.
(19) 5.5 Diversity. Suggested Good Practice. = Immediate implementation desirable. Prison profile. ✓. ✗. 5.5.31.3 - Young Offender Institutions • Drug education opportunities for grand/parents, foster carers and Mentors • Family mediation and case conferencing • Whole family drug awareness workshop opportunities (looking at the +/- influence of family culture/attitudes) • Information for families about drug use and youth culture • Involvement in drug programmes • Information on the adult prison system and how to support transitional relapse prevention strategies 5.5.31.4 - Local and Remand Prisons • Information on harm reduction in the home (especially retrieval and disposal of drugs and/or drug paraphernalia) • Drug services information (in prisons and the community) • Family inclusive Anti bullying strategies • Family liaison 5.5.31.5 - High Security Prisons • Family liaison • Drug awareness/prevention information • Family inclusive Anti bullying strategies • Supporting Relapse Prevention pre de-categorisation 5.5.31.6 - Training Prisons • Involvement of families in drug programmes • Pre-release workshops/information for families • 'Supporting Relapse Prevention' information and education (to include managing transition to open conditions) for families 5.5.31.7 - Open Prisons • 'Pre-release' workshops/information • 'Supporting Relapse Prevention' information and education. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 56.
(20) 5.6 Reducing drug related harm to children Consider: It is estimated that between 250,000 and 350,000 children are affected by the problem drug use in the UK (Hidden Harm - ACMD 2003). This equates to an average of one per problem drug user. Given the high concentration of problem drug users within the prison system, it is likely that significant numbers of children will have been, and continue to be, impacted by problem drug use. This is especially true for those children whose primary carer has a drug problem and who may have been neglected financially, emotionally or physically prior to the user's imprisonment. As a result of the problem drug user's inability to parent responsibly, many children are cared for by members of their extended family. Approximately 5% of those children affected are cared for by Social Services. Some children are born during a mother's imprisonment and may remain with her in custody. However, drug activity in prisons has the potential to affect ALL children visiting prisons. Steps must be taken to identify and address reduce the harm caused to children not only by problem drug use within the family but also by drug activity within prisons.. Useful related reading and documents: • Hidden Harm (ACMD 2003) • Every Child Matters - Changes for children in the criminal justice system • Getting our priorities right: Good Practice Guidance for working with children and families affected by substance misuse (Edinburgh: Scottish Executive 2003) • Children Act (1989) • United Nations Convention on the Rights of the Child • Working Together to Safeguard Children (1999). Suggested Good Practice. = Immediate implementation desirable. Prison visits. 5.6.1. Reduce public health risks to visitors and staff - especially children - by ensuring there are appropriate written protocols and equipment in place for dealing with incidents of spillage and/or drug related finds (including instructions for visitors on how to report them particularly in cloakrooms and baby changing areas - See DT 14) in visitors' centres and visits rooms.. 5.6.2. Ensure that free disposable nappies/wipes are available to visitors in the search areas and visits rooms (where baby milk/food should also be available for purchase) to avoid necessity for visitors to bring them in to the prison, or for visits to be ended unnecessarily early.. 5.6.3. Before being searched, children should be asked if anybody has given them anything to bring into the visit.. ✓. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✗. 57.
(21) 5.6 Reducing drug related harm to children. Suggested Good Practice. = Immediate implementation desirable. Prison visits. 5.6.4. Ensure all staff involved in the searching of children are able to interpret language and/or behaviours exhibited by children and/or carers that may give rise to substance related Child Protection concerns. 5.6.5. Invoke Child Protection procedures when children under 16 years of age are found to have drugs, or other contraband, secreted on them.. 5.6.6. Invoke Child Protection procedures when children under 16 years of age are in the care of an adult engaged in drug supply or under the influence of dugs/alcohol.. 5.6.7. Promote positive parenting information in visitors' centres and prisoner holding areas. 5.6.8. Search staff should wear disposable gloves for all searches, rather than only when searching those visitors who are under suspicion, or whose personal hygiene suggests it is necessary to do so - which may be seen as discriminatory. (Gloves should be changed when they have come into contact with any potentially contaminating substance or at the request of a visitor who is about to be searched). ✓. ✗. Child specific support (including supervised play) 5.6.9. Develop collaborative relationships with specialist agencies (e.g. children and families/substance related/social/security services) to ensure that your services for children are designed and delivered appropriately to take account of drugs. 5.6.10 Ensure all staff involved in the support/supervision of children are: substance aware; able to interpret language and/or behaviours exhibited by children during play that may give rise to substance related Child Protection issues; are fully conversant with information sharing protocols 5.6.11 Carry out pre/post visit session security checks of play areas (including equipment) 5.6.12 Ensure that children's play areas are closely monitored (e.g. by substance aware staff and/or CCTV) 5.6.13 Provide only play equipment that is easily checked for secreted drugs and/or paraphernalia. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 58.
(22) 5.6 Reducing drug related harm to children. Suggested Good Practice. = Immediate implementation desirable. Child specific support (including supervised play). ✓. ✗. 5.6.14 Involve children and young people in development of substance related resources 5.6.15 Provide special family 'bonding' visits for siblings of babies in Mother and Baby Units (to include mother, baby, siblings and community carer/s) 5.6.16 Consider providing therapeutic play/activities/resources for children of drug users: attending prison family involvement events; in community treatment and support settings 5.6.17 Consider establishing a Young Carers support group/service. Prisoners as parents and carers 5.6.18 Recognise and value the different roles that family members have in caring. (Remember that primary carers are not always parents and not always female) 5.6.19 Ensure that pregnant drug users are identified as soon as possible after entry into prison and that they receive appropriate ante natal care (i.e. specific to their needs as drug users and equivalent to that which is available in the community) 5.6.20 Recovering drug users who are resident with their children in Mother and Baby Units should receive specialist parenting support and training aimed at reducing harm to their children 5.6.21 Develop/commission specific substance related modules for parenting courses. (Content should be aimed at imprisoned parents whom: use substances; have children being cared for by substance users; or who have concerns about their children as potential/actual substance users) 5.6.22 Co-ordinate facilitated support groups for imprisoned parents who are concerned about their children using substances. (These should be aimed at helping prisoners address issues, and develop strategies to deal with: communicating with young people about drugs and alcohol; positive role modelling; guilt and anger; disempowerment; blaming/being blamed etc.). Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 59.
(23) 5.6 Reducing drug related harm to children. Suggested Good Practice. = Immediate implementation desirable. Prisoners as parents and carers ✓. ✗. 5.6.23 Ensure that newly received prisoners who were caring for a problem substance user prior to imprisonment are identified and referred for appropriate support 5.6.24 Consider piloting a dedicated Mother and Baby Drug Rehabilitation Unit. Supporting non-imprisoned parents and carers 5.6.25 Ensure that adults escorting children on prison visits are aware of their responsibilities in relation to drugs, or other contraband, found secreted on children they are escorting - whether or not they are normally responsible for the child's day-to-day care. (This can be done using: reminders at booking; notices at the entrance to the prison; and also by verbal reminder to escorts prior to searching of a child under 16 - See DT 13). 5.6.26 Provide benefits and support information specific to the needs of non-parental carers 5.6.27 Provide parenting support and drug service referral for carers who are also drug users 5.6.28 Facilitate/sponsor child-care support, if necessary, to enable carers to participate in family involvement opportunities 5.6.29 Consider establishing a parent support group for families of drug users 5.6.30 Consider establishing a carer support group to address non-parental caring issues (e.g. carer/parent conflict, custody, finance etc.). Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 60.
(24) 5.7 Staff learning and skills Consider: Family work is complex, encompassing as it does such a wide variety of issues. It is not surprising that staff, sometimes, feel overwhelmed with the knowledge and skills they are expected to have at their fingertips. However, acquisition of family focussed knowledge and skills should not be seen as something that is achieved at induction, or during occasional training days/courses. Rather, it should be viewed as something that is ongoing, 'on the job' and needs led. It should comprise a variety of learning opportunities. (E.g. formal classroom based learning; cross project 'shadowing'; and multi-disciplinary training events.). Useful related documents: DANOS (Drug and Alcohol National Occupational Standards). Suggested Good Practice. = Immediate implementation desirable. Staff learning and skills. 5.7.1. Ensure that the content of training delivered is consistent with the needs of the role staff are expected to fulfil. (E.g. All staff coming into contact with families have a need to be drug aware. It is not essential to require that all VC staff have in depth knowledge of the history and long term effects of different drugs, but they do need to know how to manage substance related finds. Skills in assessment service user need in relation to drugs, and making appropriate referrals, is something all VC support staff need). 5.7.2. All staff engaged in drug related family support should be provided with training in: Basic Drug Awareness; Drugs and Families Awareness (including race and culture); Basic Drug Interventions (Prison and Community based); Assessment and Referral; Motivational Interviewing; Raising of Security Information Reports (SIRs). 5.7.3. Ensure that all Visitors' Centre and community based family support staff are aware of, and understand, prison: rules; procedures; treatment and support approaches for prisoners and families experiencing drug related problems (including a working knowledge of appropriate referral procedures including raising family concerns about prisoners thought to be at risk of self-harm/suicide); confidentiality/information sharing protocols. 5.7.4. Ensure all staff coming into contact with families are familiar with Child Protection reporting procedures. ✓. Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). ✗. 61.
(25) 5.7 Staff learning and skills. Suggested Good Practice. = Immediate implementation desirable. Staff learning and skills ✓ 5.7.5. Family support staff (particularly those conducting Home Visits) should receive training that enables them to identify, assess, manage and report substance related activity/risks. 5.7.6. Generic staff should be provided with information and learning opportunities that enable them to make appropriate substance related family referrals. 5.7.7. All prison based staff coming into contact with prisoners and/or families (whether service or civilian) should receive training on: Families and drugs; confidentiality and information sharing procedures; referral agencies and procedures (Such staff may include: Education; Chaplaincy; Visits; Personal Officers; Healthcare; Samaritans Listener Co-ordinator etc). 5.7.8. Listeners should be provided with training that enables them to develop a basic understanding of the potential impact of substance use and recovery on family relationships. 5.7.9. Consider developing reciprocal staff shadowing and training opportunities with other agencies to enable staff to develop appropriate cross discipline skills and awareness. ✗. 5.7.10 Consider joining, or subscribing to, specialist journals/services/ news-sheets (e.g. Prison Service Journal; Action for Prisoners' Families; Adfam Voices & Choices; Druglink). Partners in Reduction | A Good Practice Toolkit for Engaging and Involving Families in the Reduction of Substance Related Problems in Prisons. © NOMS Drug Strategy Unit (2005). 62.
(26)
Figure
Related documents
Resume recovery feature of Stellar Phoenix Photo Recovery allows you to recover photos, audio and video files using saved scan information file or image file.. You can use the
The companies Berlin Partner GmbH and ZukunftsAgentur Branden- burg GmbH (Brandenburg Economic Development Board) support with a large range of services, from recruiting
A process was developed to identify potential defects in previous layers of Selective Laser Melting (SLM) Powder Bed Fusion (PBF) 3D printed metal parts using a mid-IR thermal camera
The aims of this study were to assess whether (1) a single session of TBS was able to improve motor performance in PD immediately after stimulation, (2) TBS was more
In the previous sections, we dis- cuss the expectation that a neural network exploiting the fractional convolution should perform slightly worse than a pure binary (1-bit weights
Steele of Stanford University Online High said that shift is already underway: In a recent survey of ASCA members, she and her colleagues found that more than one-fourth of
(1) Any person holding a valid hotel certificate shall, on payment of a processing fee of 1,000 rupees, make an application in writing to the Committee for a star rating certificate
College Mathematics (3 Credits) Biology (6 Credits) Arts and Humanities 3 Arts and Humanities 3 TOTAL 35 20 8.00 **Total up RED # ** Excess credits 0.00 8.00 Analyzing and
