Acute kidney injury in major abdominal surgery: incidence, risk factors, pathogenesis and outcomes
Full text
Figure
Related documents
AKI: Acute kidney injury; CABG: Coronary artery bypass graft; CKD: Chronic kidney disease; COPD: Chronic obstructive pulmonary disease; CPB: Cardioplumonary bypass; GFR:
AKI: Acute kidney injury; CKD: Chronic kidney disease; eGFR: estimated glomerular filtration rate; ESRF: End-stage renal failure; ET-1: Endothelin-1; HIF: Hypoxia-inducible
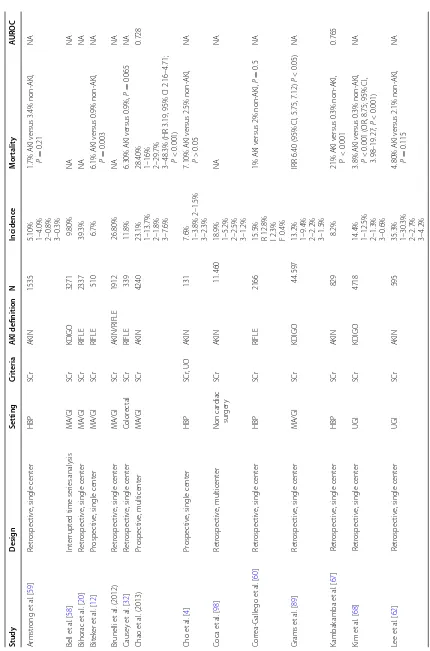
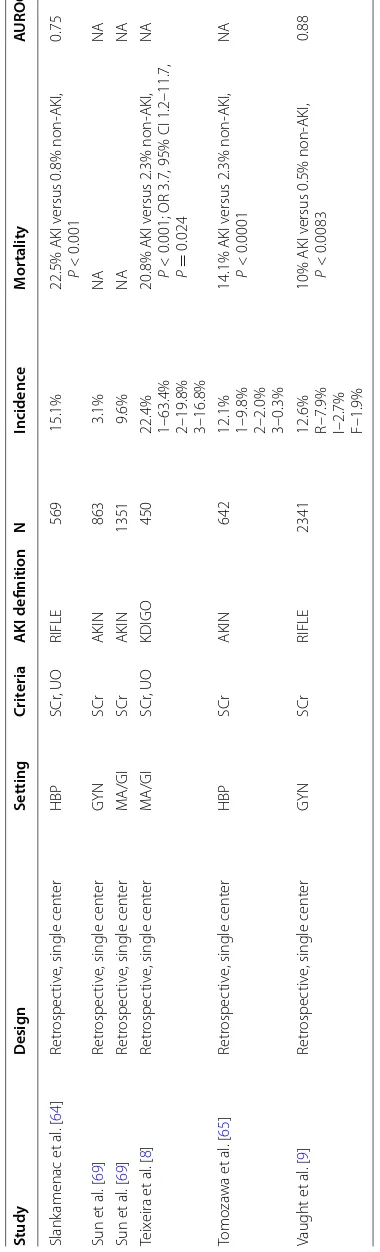
Acute Dialysis Quality Initiative “ RIFLE ” criteria (risk, injury, failure, loss, End Stage Renal Disease), “ AKIN ” (Acute Kidney Injury Network), “ AKIB ” Acute Kidney
AKI: acute kidney injury; AKIN: acute kidney injury network; CKD: chronic kidney diseases; CKD-EPI: chronic kidney disease epidemiology collaboration; eGFR: estimated
AKI: Acute kidney injury; AKIN: Acute kidney injury network; APACHE: Acute physiology and chronic health evaluation; CCF: Congestive cardiac failure; CI: Confidence interval;
AKI: Acute kidney injury; AKIN: Acute Kidney Injury Network; APACHE II: Acute Physiology and Chronic Health Evaluation II; ICU: Intensive care unit; KDIGO: Kidney Disease
CKD: Chronic kidney disease; CSA-AKI: Cardiac surgery-associated acute kid- ney injury; eGFR: Estimated glomerular filtration rate; ESRF: End stage renal failure; HR: Heart rate;
Abbreviations: AKI, acute kidney injury; AKIN, Acute Kidney Injury Network; CKD, chronic kidney disease; EMRs, electronic medical records; FDA, US Food and Drug Administration;
