Preparing
Young
Children
for Hospitalization:
A Comparison
of Two
Methods
Barbara
Faye
Ferguson
From Victoria, British Columbia, Canada
ABSTRACT. This study examined two methods of
pre-paring children aged 3 to 7 years for hospitalization. One
method was a preadmission home contact by a nurse.
The second was a filmed modeling sequence shown on
admission. The effectiveness ofeach condition in reducing
anxiety in the children and mothers was examined sepa-rately and in combination. One group of children experi-enced neither preparatory method. All children were
undergoing elective tonsifiectomies.
The children’s adjustment to the hospital was
mea-sured on three occasions via a self-report measure of
anxiety, electromyographic measures ofmuscular tension,
and ratings of behavioral upset. Posthospital adjustment
was assessed with Vernon et al’s Post-Hospital Behavior Inventory. An assessment of maternal anxiety was ob-tamed twice via a self-report measure of anxiety. Mater-nal satisfaction with care and information was also
ob-tamed.
The results indicate that a preadmission visit
contrib-utes to the lessening of maternal anxiety during and after
the child’s hospitalization. A preadmission visit was also
associated with reduction in the incidence of negative
posthospital behavior particularly with the 6- and
7-year-olds. Mothers who were preadmitted expressed
signifi-cantly greater satisfaction with the care and information
they and their children received.
Viewing a peer modeling film was associated with a decrease in the children’s hospital-specific physiologic anxiety response at the preoperative measure. In addition,
children who viewed a peer modeling film displayed a
significantly lowered incidence of undesirable
posthospi-tam
behavior. Pediatrics 64: 656-664, 1979; hospitalizedchild, tonsillectomies, preoperative preparation, model-ing, psychological preparation.
When a young child must be hospitalized, the effects of the experience can be very detrimental. Several studies have indicated that these effects
may evidence themselves as behavior disturbances,
regressed development, retarded recovery and the
like.’ Two studies from Britain5’6 provide striking
Received for publication Nov 29, 1978; accepted March 13, 1979.
Reprint requests to (B.F.F.) 1010 Joan Crescent, Victoria, British
Columbia, Canada V8S 3L5.
PEDIATRICS (ISSN 0031 4005). Copyright © 1979 by the American Academy of Pediatrics.
evidence that a hospital admission of greater than
one week’s duration, or repeated short admissions
before the age of 5 years are associated with an
increased incidence of behavior disturbances at age
10 years and into adolescence.
There has been much speculation as to the
rea-sons why young children are particularly vulnerable to the hospital experience. Certainly, the limitations imposed on the child by his cognitive developmen-tal level plus his lack of worldly experience contrib-ute toward making the hospital a totally unfamiliar
and unpredictable environment for him.
The need to be able to know and predict the
environment seems to be a universal human trait. The association of this need with the stresses of
hospitalization was first recognized by Janis.7 Janis,
in a study of adult surgical patients, proposed that
the response to stress impact is a function of the accuracy of the individual’s expectations. A patient
who is given global reassurances which minimize
the seriousness of the situation is likely to encounter
unexpected difficulties which may engender
resent-fulness, hostility, or depression. On the other hand,
Janis proposed, a person with more accurate
expec-tations visualizes specific problems in connection with his surgery and counters them with reality-based plans. In this way, he does not feel helpless. Many studies8” with hospitalized adults have indicated that accurate information does indeed have positive effects on the manner in which the individual deals with stress. Some of the effects noted include lessened need for postoperative med-ication and more rapid recovery.
Related to this are fmdings of studies by
John-son’2”3 which suggest that the intensity of anxiety
involved in a pain experience is a function of the degree of incongruity between physical sensations
experienced and sensations expected. Johnson
found that subjects given information about
sensa-tions to expect from a noxious stimulus exhibited
It appears that young children may experience
even more anxiety than adults when confronted with an unfamiliar situation. Castell’4 tested chil-dren aged 15 months to 3 years and found that unknown persons and environments significantly
increased the children’s need to be physically close to their mothers. Brown and Semple’5 studied chil-dren aged 3 to 5 years and noted that children in
unfamiliar environments exhibited significant de-creases in motor-perceptual and verbal behavior,
and increases in global gazing behavior and freezing
behavior (similar to fear reactions in some animals).
One would anticipate, then, that young children
may well find the hospital frighteningly unfamiliar.
The fact that the mother may also feel helpless and unable to predict the events involved in her child’s hospitalization is also worthy of consideration.
Skipper’6 examined the effects of accurate infor-mation on maternal distress. In accord with Jams’7 postulation, Skipper showed that mothers who re-ceived adequate advance information from their physician about their child’s hospitalization ex-hibited less distress and made a more rational adap-tation to the hospitalization than mothers who were
given very little or no advance information.
Expanding on this, Skipper and Leonard’7 hy-pothesized that the anxiety level of the mother will
affect the anxiety level of the child. These
research-ers constructed an experiment in which one group
of mothers were attended to by a “special nurse” on admission who attempted to create an
atmos-phere which would facilitate the communication of
information, would allow freedom to verbalize fear, anxiety, and the asking of questions. The control group of mothers received the regular introduction to the hospital. The mothers in the experimental
group exhibited a lower level of distress and this, in turn, seemed to affect the children. Physiologic and behavioral measures indicated a much lower anxi-ety level in the experimental children. Also, these
children made a more rapid recovery and
experi-enced fewer after-effects of the hospitalization.
It would appear, then, that a great deal of hospi-tal-related stress affecting the mother can be ame-liorated by verbally imparting adequate
informa-tion before and during the experience.’7”8 Giving adequate hospital-related information to a young child requires more than just verbal explanations.
Immature verbal and comprehension skifis make
this method unsatisfactory as the only means of imparting information to a young child. Child-fo-cused methods, such as play therapy, puppet shows, storybooks, etc, have been suggested as appropriate, but, unfortunately, have received limited evaluation as to their comparative effectiveness. There is,
how-ever, considerable evidence in the research on
mod-eling that the use of models is an effective way not
only to show children what to expect, but also to show them how to respond to unfamiliar situations.
Bandura and Menlove’9 have suggested that af-fective learning in humans often occurs as a result
of witnessing others respond fearfully toward, or be
hurt by, certain things. In their study of children with severe fear of dogs, these researchers showed
that the effect of a ifimed model can be most beneficial in fear reduction.
The use of modeling to reduce anxiety in children
experiencing hospitalization has recently received
investigation. Vernon20 examined children experi-encing anesthesia induction. Half of the subjects saw a ifim that showed children of varying ages responding calmly to anesthesia induction. The
control group saw no film. Vernon found that chil-then exposed to the film exhibited less fear of anesthesia induction. Melamed and Siegel21
exam-med 60 children aged 4 to 12 years about to undergo
elective surgery. Half of the children saw a peer-modeling film of a child being hospitalized and
experiencing surgery, and the others saw an
unre-lated control film. Self-report, behavioral, and phys-iologic measures of anxiety revealed a significant
reduction of preoperative and postoperative fear in the experimental group. As well, the experimental
group displayed significantly fewer posthospital be-havior problems. The filmed modeling sequence used in this study exhibited a coping model in light
of Meichenbaum’s22 findings that models who are initially anxious and overcome their anxiety (coping
models) result in greater anxiety reduction than models who exhibit no fear at all (mastery models).
The present study examined two methods of pre-paring young children for hospitalization. One method was the use of a ifimed modeling sequence, similar to that utilized by Melamed and Siegel.2’ The second method employed a procedure some-what similar to that described by Skipper and Leon-ard17 with the exception that, in this instance, the
contact between the nurse and the mother and child
took place prior to hospital admission in the child’s
own home. This preadmission contact had the
ob-jective of imparting preknowledge of the hospital process in the environment that the child and mother would find most comfortable and safe. The effectiveness of each condition (filmed modeling
and preadmission visit) was examined separately and in combination and compared to a control
group who experienced neither.
METHOD
Subjects
During the data collection period of this study,
82 children met the following criteria and were
TABLE. Sample Characteristics for Age and Sex of Experimental Groups
Variables Groups
Contr ol Film Model ing Film
Hospital Preadmission Hospital Preadmission
Admission Visit Admission Visit
Age (yr)
3-4 9 8 9 8
5 6 7 5 8
6-7 6 5 6 5
Sex
Male 9 13 9 12
Female 12 7 11 9
3 and 7; (2) experienced no previous hospitalization; (3) exhibited no medical or psychological condition requiring consultation or special care; (4) admitted to Alberta Children’s Hospital for elective
tonsillec-tomy, alone or in combination with adenoidectomy;
(5) both mother and child spoke English. Seventy-nine of the children were of European descent; three were of Asiatic descent. There were no black or oriental children in the sample. The length of stay in the hospital was two days for all the children. Informed consent was obtained from all mothers.
Group Assignment
Each child was assigned, using a table of random numbers, to one of four groups: (1) those who experienced a regular hospital admission procedure and viewed a nonhospital-related film; (2) those
who experienced a regular hospital admission
pro-cedure and viewed a hospital-related peer-modeling film; (3) those who experienced a preadmission visit
from a nurse in their home prior to their hospital admission and viewed a nonhospital-related film;
(4) those who experienced a preadmission visit from
a nurse in their home prior to their hospital admis-sion and viewed a hospital-related peer-modeling
ifim.
Preadmission Visit
All subjects in the study were given admission information by the same nurse. Those who were preadmitted were contacted by the nurse five to seven days prior to their scheduled admission, and an appointment was made to visit mother and child at their home.
At the time of visit, the nurse completed, with the mother, the necessary hospital admission doc-uments. Following this, the nurse gave information
to mother and child about general hospital rules
and routines, including: what to bring to the hos-pital, routine admission tests to expect, the play-room program, the anesthetist’s examination, the
fasting requirement for the morning of surgery, the
preoperative injection and what the operating room looks like. In addition, mothers were given specific information about the open visiting hours for
par-ents and the amenities available to them at the hospital such as the cafeteria and parent lounge. It
was also explained that the child would have a very
sore throat and might vomit following the surgery, but that this is not abnormal. Throughout these
explanations, the mother was given the opportunity to ask questions and to express concerns.
At the end of the visit, the preadmission nurse
left a hospital pamphlet on which was noted the
nurse’s name, and the date and time of admission.
The mother was directed to contact her physician if the child developed cold symptoms, fever, etc,
prior to the admission date.
On the day of admission, the nurse met mother
and child at the hospital entrance, escorted them to the laboratory, surgical unit, and then to the
playroom.
The children and mothers who were not pread-mitted were called by the nurse a few days prior to their admission date and told when to arrive at the hospital. On the day of admission, they were met at
the main entrance and escorted to the admitting
office where the hospital admission documents were
completed. From there they were taken to the
laboratory and then to the surgical unit, where all
other aspects of the admission procedure were
com-pleted.
For the children and mothers who were
pread-mitted, the admission procedure at the hospital
usually took about 15 minutes. For those who were
hospital admitted, the procedure usually required
about an hour.
The Film
The experimental film was entitled Yolanda and David Have Their Tonsils Out. It depicts two
hospi-talized for tonsillectomies. This film, which is 15
minutes in length, depicts various events that most children encounter when hospitalized for elective tonsillectomy. The film was produced at Alberta Children’s Hospital and includes many places and people that a child would be likely to see there. Throughout the film, the scenes are narrated by the children who describe their experiences plus their feelings, concerns, and physical sensations at each
stage of the hospital process. Both the behavior and
verbal remarks of the two children exemplify the
behavior of coping models, that is, even though each child expresses some initial apprehension, they are able to overcome their fears and complete each
event in an adaptive manner.
The subjects in the control groups were shown a
15-minute film entitled Starship Access. It presents
a futuristic spaceship sequence designed to teach
young children about the metric number system.
Each film was in the form of a color video cassette.
Evaluation Measures
In order to assess the various response classes
considered to be reflective of the multidimensional nature of anxiety, a number of evaluation measures were employed including self-report, behavioral,
and physiologic measures.
Self-Report Measures
HospitalFears Rating Scale. The Hospital Fears Rating Scale was utilized with considerable success
by Melamed and Siegel.2’ This scale is comprised of eight items from the Medical Fears subscale,
factor-analyzed from the Fear Survey for Children23
plus another eight items with face validity for
as-sessing hospital fears and nine nonrelated “filler”
items. The sum of the ratings on the 16 medical fear
items was the child’s score for this measure.
Mood Adjective Checklist. Adopted from Radloff and Helmreich,24 the Mood Adjective Checklist is a forced choice checklist with three alternative
re-sponses for each of 67 adjectives. The subjects (in
this case, the mothers) rated each adjective in
re-spect to how it applied to their present mood. Six
mood scales (anger, happiness, fear, depression,
psychological well-being, and lethargy) were
de-rived. An overall score was computed by adding
together the scores of the four negative moods
(depression, fear, anger, and lethargy) and
subtract-ing the scores for psychological well-being and
hap-piness.
Physiologic Measure: Electromyography
Muscle tension has long been recognized as a motor-expressive aspect of the emotional process25
and electromyography is currently the most popular
technique for measuring muscle tension.26 For the
purpose of this study, the Autogen 1700 Feedback
Myograph was used. This instrument allowed for
painless attachment of electrodes at the selected
muscle site plus an instantaneous metering of EMG
activity.
The trapezius muscle was selected as the site of measurement. Voas27 reported that during stress and frustration, tension was found to be most
prom-inent in the trapezius and masseter muscles. An added advantage of this location with children is the fact that the electrodes are not in the child’s line of vision during measurement. The EMG
read-ings were monitored during administration of the
Hospital Fears Rating Scale. The resultant EMG
scores on each subject were computed into a mean
score and a variance score which measured the
range between the resting EMG score and the
high-est EMG score.
The range score was considered particularly im-portant in monitoring hospital-specific anxiety.
Lip-pold28 states that it is invalid to compare EMG mean scores for individuals across pre- and posttest conditions since replacement of electrodes in even
slightly different positions can result in the
moni-toring of different areas of muscle, and thus produce
very different readings. Consequently, it is
neces-sary to establish resting levels of muscle tension
and gauge responsivity to stimuli as divergences
from this level. The use of a resting muscle tension
measure helps to eliminate the response to the
hospital-specific stimuli of the measurement
situa-tion. Means analysis would not do this. EMG means
may be a better measure of general anxiety alone.
Behavioral Measures
Observer Rating Scale ofAnxiety. The Observer
Rating Scale of Anxiety was used by Melamed and Siegel.2’ This behavioral observation scale is con-structed of 29 categories of verbal and skeletal-motor behavior thought to represent behavioral
manifestations of anxiety in children. A time
sam-pling procedure was used in which an observer
indicated the presence or absence of each behavior
during two intervals in a six-minute observation period. The number of negative behaviors observed
plus the number of positive behaviors not observed
became the subject’s score.
Post-Hospital Behavior Rating Scale. The Post-Hospital Behavior Rating Scale was developed by Vernon et al29 and has received extensive use in
studies of hospitalized children.’3”82#{176} The
question-naire consists of 27 behavioral items comprising
those most frequently cited in the literature as
each item, the mother is asked to compare the child’s typical behavior before hospitalization.
Ver-non et al factor analyzed the questionnaires of 387 children and produced six factors: (1) general
anxi-ety and regression, (2) separation anxiety, (3)
anxi-ety about sleep, (4) eating disturbances, (5)
aggres-sion toward authority, and (6) apathy-withdrawal.
Satisfaction with Care and In formation
The Satisfaction with Care and Information Questionnaire was developed by the researcher and
completed by the mothers following the child’s hos-pitalization. It asked the mothers to evaluate the
adequacy of information that they and their child
received as well as their satisfaction with the care their child was given. Questions were based on findings of Freiberg#{176} in respect to mothers’ reasons for anxiety during their child’s hospitalization.
Procedure
Immediately following hospital admission, each
mother was given the mood checklist form to corn-plete while the child was escorted to a separate
room that had been set aside for the study. The child was introduced to the behavioral observer,
who was present in the room, and instructed to sit in a soft chair. The EMG electrodes were shown to the child and he was encouraged to touch them. The electrodes were placed on the trapezius muscle and the machine engaged. The child was seated in
such a way that he was not easily able to observe the EMG dial. The experimenter then presented the color-coded thermometer diagram of the
hos-pital fears questionnaire and explained that she and
the child would now play a game. Instructions were given as follows: “I’m going to ask you about some
things that some kids are afraid of and some kids aren’t afraid of. I want you to tell me how afraid
you are by pointing to one of these squares. This
blue one tells me you are not afraid at all; this green one tells me you are a little afraid; this yellow one tells me you are a fair amount afraid; this orange one tells me you are pretty much afraid; and this red one tells me you are very afraid. For each thing I say, point to the color that tells me how afraid
you are.”
During the administration of the Hospital Fears
Rating Scale, the experimenter made a notation of the EMG levels immediately following each ques-tion. As well, EMG readings were monitored prior
to the administration of the Hospital Fears Scale and at the completion of it while the child was
sitting quietly.
During this period of time, the second experimen-ter observed the child with the Observer Rating Scale of Anxiety.
After the measures were completed, the child was
shown the experimental or control film depending
on his group assignment. The experimenter who recorded the behavioral observations left the room prior to the start of the film in order to remain
unaware of the treatment condition to which the
subject had been assigned.
The subject’s anxiety level was assessed in the
same manner the morning immediately prior to his
scheduled surgery.
The follow-up visit occurred seven to ten days
after the surgery. At this time, the mother was
instructed to complete the Post-Hospital Behavior
Questionnaire, the Satisfaction With Care and
In-formation Questionnaire, and a Mood Adjective
Checklist. While the mother completed these forms,
the child was taken to the examination room where the three anxiety measures were once again
admin-istered.
RESULTS
Hospital
Fears
Rating ScaleChildren who received a preadmission visit showed a slightly lowered mean score on the Hos-pital Fears Rating Scale at the admission and post-operative measurement. There was, also, a signifi-cant effect due to time alone, F
(2,152)
= 7.286, P< .01; with all scores displaying a lowering trend
over time. When the scores were analyzed for age
groupings, significant differences were noted for
age, F (4,156) = 5.233, P <
.01;
time, F (4,156) =6.64, P < .01; and age-time interaction, F (8,314) =
5.167, P < .001. The youngest group (3- and
4-year-olds) consistently scored highest and showed an
increase in self-report anxiety at the postoperative
measure (Fig 1).
Mood Adjective
Checklist
The Mood Adjective Checklist scores were
sig-nificantly different over time, F (1,68) = 37.29, P
< .01, with a lowering of scores between the two
measurement periods. The mothers of the children
who saw the peer-modeling film reported a
signifi-cant decrease in self-report anxiety over time, F
(1,68) = 5.028, P < .05. The mothers who
experi-enced a preadmission visit also scored lower on the postoperative measure (Fig 2). An examination of
the subcategories of the Mood Adjective Checklist
revealed that the happiness mean scores on the
postoperative measure were significantly higher (t
= 5.614 at 34 df; P < .007) for the mothers in any
of the experimental conditions (preadmitted and/
t’o
0
‘1)
55
50
45
40
35
30
25
Admission Pe-0perat1ve Post-Operative
TIME
15
)bspital-Ldaitt.d Group
- Pr.-Aditt.d Group
10
0
Aad Po.t-c*4rttiY.
Fig 2. Mean scores for Mood Adjective Checklist for
mothers who were preadmitted and those who were hos-pital-admitted.
- 3 and 4 year olds
- 5 year olds
- 6and7yearolds
x
Fig I. Mean scores for Hospital Fears Rating Scale by
age groups over time.
on admission for those mothers who had been
preadmitted.
Electromyogram Scores
The only experimental condition that appeared
to affect EMG mean scores was the peer-modeling ifim, with a lowering of scores through all three
measures. In addition, the peer-modeling film
ex-erted a noticeable lowering effect on the EMG range
scores at the preoperative measure.
Observer
Rating
Scale
of
AnxietyThe Observer Rating Scale of Anxiety scores
showed no significant differences due to group
as-signment, time, or age; The only notable difference occurred at the postoperative measure where the
subjects who saw the peer-modeling film scored
lower than those who saw the control film.
Post-Hospital Behavior Rating Scale
Analysis of the Post-Hospital Behavior Rating
Scale scores indicated a significant lowering of
scores for those who saw the peer-modeling film F
(1,76) = 7.98, P < .01. When the six factors of the
Post-Hospital Behavior Rating Scale were analyzed
separately, it was noted that viewing the
peer-mod-eling film was associated with significantly less aggression towards authority and
apathy-with-drawal. The effects of preadmission were most
ob-vious in reducing the incidence of behaviors asso-ciated with separation anxiety and eating
distur-bances.
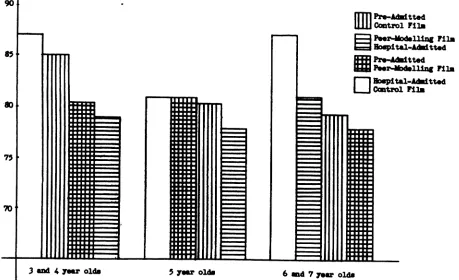
Pictorial representation of Post-Hospital Behav-ior Questionnaire scores according to age grouping
(Fig 3) indicates that the peer-modeling film has an
effect in lowering scores across all age groups. In the older age group (6- and 7-year-olds)
preadmis-sion appears to have a greater influence in lowering
scores than in the younger age group.
Satisfaction With Care and Information
Analysis of the scores of the Satisfaction with Care and Information questionnaire indicated
sig-nificantly higher levels of satisfaction among the
preadmitted mothers, F (1,76) = 4.33, P <
.05.
A correlation analysis of the Satisfaction with Care and Information scores and the Post-Hospitaliza-tion Mood Adjective Checklist scores revealed asignificant negative correlation of r = -0.36 (F =
10.3 at 1,69 dl; P < .01) indicating that mothers
85
7,
70
3 sM 4 y.r old. 5 yr 6 .d 7 ar old.
90
nIH
Pre-Adtt.d[LIJJ
Ccntroi Fil*Peei’-Modslling
spitt1-Att.d P1*44kitted
P#{243}.r-Uing
D
spita1.44itt#{149}dCitro1 Fi]a
Fig 3. Age and group differences in Posthospital Behavior Questionnaire scores.
and information tended to express low levels of
anxiety.
Miscellaneous
No significant differences were noted in the
var-ious dependent variable scores when the subjects
were grouped according to sex or admitting
physi-cian.
DISCUSSION
The results of the present study support the
contention that hospitalization of a young child is
an anxiety-provoking experience for both the child
and the mother. Even in this relatively limited age
range, differences between younger (3- and
4-year-olds) and older (6- and 7-year-olds) children were
evident. The 3- and 4-year-old children report greater hospital-specific anxiety than do the 6- and
7-year-old children across all measurements. As
well, the 3- and 4-year-olds were the only group
that showed an increase in self-report
hospital-spe-cific anxiety on the postoperative measure,
suggest-ing that a return to the hospital was
anxiety-pro-yoking for them. Also, the incidence of undesirable
posthospital behavior is most effectively diminished
in the younger group by the peer-modeling film,
while the 6- and 7-year-old group responded as
positively to the preadmission visit. This would
seem to indicate that the younger group is better
able to internalize information presented in a visual
display. The older group, with better developed
verbal skifis and understanding, were able to
inter-nalize the verbal information given by the
pread-mitting nurse. These differences in age groups
would strongly suggest that examination of
chil-dren’s responses to hospitalization should consider
fairly homogeneous age groupings. Wide age ranges
in experimental samples (eg, 3-12 years) cannot be
expected to give clear information as to age-specific
reactions and responses either to the hospital
proc-ess itself or to intervention techniques.
Considering the total group examined in the
pres-ent study, it seems that the combined effect of the
preadmission visit and the peer-modeling ifim is not
necessarily stronger than the individual conditions.
However, a preadmission visit or the peer-modeling
film or the two combined is more effective than
nothing. The control group in this study scored the
highest on admission self-report anxiety and
showed the highest incidences of undesirable
post-hospital behavior.
The earlier work of Melamed and Siegel2’
mdi-cated that children who view a peer-modeling ifimwill exhibit significantly less preoperative and
post-operative anxiety than children who view a control
effects were noted on the scores of both the Hospital Fears Rating Scale and the Observer Rating Scale
of Anxiety. In the present study these results were
not replicated. The reasons for these discrepancies are not entirely clear. One possible explanation could be the differences in age groupings of the
subjects used. In the Melamed and Siegel2’ study
the subjects were aged 4 to 12 years. These re-searchers did note with their Hospital Fears Rating
Scale results that the 3- to 7-year-old children
re-ported greater fear regardless of film condition. The possible interactional effect of the
preadmis-sion visit may also be an explanation for the results
of the present study. Melamed and her colleagues3’ noted that children who were prepared for hospi-talization one week in advance displayed lowered self-reported anxiety at the time of admission plus a reduction in observed behavioral anxiety. In the present study, the two film condition groups each contain 20 subjects who were preadmitted. It is
feasible to assume that the preadmission experience
may have affected the results to make them less distinctly different between film conditions.
In the present study, the most notable differences
between the two film condition groups were on the
EMG scores and the Post-Hospital Behavior
Ques-tionnaire scores. On the EMG means, the children
who viewed the peer-modeling film scored lower than those who saw a control film on all three
measures.
As well, the EMG range scores showed a notice-able effect due to ifim condition. Because the range
scores represent response to the hospital-specific
stimuli of the experimental situation, a reduction in
range indicates that response to the stimuli has decreased. Since each subject will receive the
stim-uli with variable degrees of threat, the reduction in range scores indicates that areas causing most
con-cern were modified more effectively at the preop-erative measure in the group who saw the peer-modeling ifim than in the group who saw the control
ifim. The admission and postoperative mean range
scores were basically the same.
The Post-Hospital Behavior Rating Scale results showed a strongly significant difference between the children who viewed the peer-modeling film and those who saw the control film (P < .01), with the peer-modeling film group displaying less overall
negative posthospital behavior. As well, when the six factors of the Post-Hospital Behavior Rating
Scale were separately analyzed, it was evident that
viewing the peer-modeling film was associated with
significantly less aggression toward authority (P <
.05) and less apathy-withdrawal (P < .01).
As was expected from the Skipper and Leonard
17 the effects of the preadmission visit was
noted primarily in the responses of the mothers. At
the posthospital measure, the preadmitted mothers displayed a much lower mean score on the Mood Adjective Checklist and a significantly higher
“hap-piness” score. In addition, the Satisfaction with
Care and Information Questionnaire results dis-played a significantly higher level of satisfaction among the preadmitted group.
These results support the concept put forward by Epstein and Rouperman32 that a favorable set to-ward an unfamiliar situation enhances the favorable
evaluation after the situation becomes familiar. In
other words, the preadmission visit functions to
“set” the mother to feel more positively about the
hospital experience by initially exposing her to the pending hospital experience in a relatively
comfort-able situation (ie, her own home). The positive effect of this initial exposure context is thus
trans-ferred to the actual situation (ie, the hospital). Whether or not the decreased anxiety of the
preadmitted mothers affected the anxiety levels of their children is difficult to determine. Preadmitted children did show lower mean scores on the Hos-pital Fears Rating Scale at the admission and
post-operative measures. As well, the mean scores on the
Post-Hospital Behavior Questionnaire suggest the
positive influence of preadmission particularly with
the 6- and 7-year-old group.
In summary, the results support the initial
as-sumption that accurate preknowledge does assist in
reducing hospital-specific anxiety in children and their mothers. The effects of this preknowledge may not be evidenced immediately (ie, at the time
of admission), but may become more evident over
time. The results suggested no correlation between the children’s self-reported and physiologic anxiety and behavioral manifestations during the
hospital-ization period. This would suggest that children’s
outward behavior may not be an accurate
assess-ment of their anxiety level. This is a very important
observation, as decisions regarding children’s care
needs in the hospital have historically been based on the children’s behavioral manifestations of
dis-tress. The results of this study suggest that this
may not be an adequate basis for determining the
individual child’s responses to hospitalization. Be-havioral manifestations of distress appear to be-come more evident later after the child’s discharge from the hospital, once the child is in the more
psychologically safe environment of his own home.
It is clear, then, that an accurate evaluation of
children’s responses to hospitalization can only be obtained if anxiety is viewed and measured as a multidimensional phenomenon. Moreover, effects
of hospitalization may well become more evident
after the experience is over; therefore, the posthos-pital period must be an important part of the
REFERENCES
1. Gellert E: Reducing the emotional stress of hospitalization
for children. Am J Occup Ther 12:125, 1958
2. Jackson K, Winkley R, Faust OA, et al: Behavior changes
indicating emotional trauma in tonsillectomised children.
Pediatrics 12:33, 1953
3. Jessner L, Blom GE, Waldfogel S: Emotional implications of tonsillectomy and adenoidectomy in children, in Eisslen, RS
(ed): The Psychoanalytic Study of the Child. New York,
International Universities Press, 1952, vol 7
4. Prugh DG, Straub E, Sands HH, et al: A study of the
emotional reactions of children and families to
hospitaliza-tion and illness. Am J Orthopsychiatry 23:70, 1953
5. Douglas JWB: Early hospital admissions and later
distur-bances of behavior and learning. Dev Med Child Neurol 17:
456, 1975
6. Quinton D, Rutter M: Early hospital admissions and later
disturbances of behavior: An attempted replication of
Doug-las’ findings. Dev Med Child Neurol 18:447, 1976
7. Janis IL: Psychological Stress: Psychoanalytic and
Behav-ioral Studies of Surgical Patients. New York, John Wiley
and Sons, 1958
8. Vernon DTA, Bigelow DA: Effect of information about a
potentially stressful situation on responses to stress impact.
J Pers Soc Psychol 29:50, 1974
9. Andrew JM: Recovery from surgery with and without
pre-paratory instruction for three coping styles. J Pers Soc
Psychol 15:223, 1970
10. Eghert LD, Battit GE, Welch CE, et al: Reduction of post-operative pain by encouragement and instruction of patients. N Engi JMed 49:786, 1959
11. Healy KM: Does pre-operative instruction make a
differ-ence? Am J Nurs 68:62, 1968
12. Johnson JE: Cognitive control of the emotional component
of the pain experience. Diss Abstr
mt
B Sci Eng 32(7B):4186, 1971
13. Johnson JE: Effects of structuring patient’s expectations on their reactions to threatening events. Nurs Res 21:499, 1971 14. Castell R: Effect of familiar and unfamiliar environments on
proximity behavior of young children. J Exp Child Pjychol
9:342, 1970
15. Brown RD, Semple L: Effects of unfamiliarity on the overt
verbalization and preconceptual motor behavior of nursery
school children. Br J Educ Psychol 40:291, 1970
16. Skipper JK: Mothers’ distress over their children’s
hospital-ization for tonsillectomy. J Marr Fam 28:145, 1966
17. Skipper JK, Leonard RC: Children, stress and
hospitaliza-tion: A field experiment. J Health Soc Behav 9:275, 1968
18. Visintainer MA, Wolfer JA: Psychological preparation for
surgical pediatric patients: The effect on children’s and
par-ents’ stress responses and adjustment. Pediatrics 56:187,
1975
19. Bandura A, Menlove FL: Factors determining vicarious
ex-tmction of avoidance behavior through symbolic modeling.
JPers Soc Psychol 13:175, 1969
20. Vernon DTA: Use of modelling to modify children’s re-sponses to a natural potentially stressful situation. J Appl
Psychol 58:351, 1973
21. Melamed BC, Siegel U: Reduction of anxiety in children
facing hospitalization and surgery by use offilmed modelling.
J Consult Clin Psychol 43:511, 1975
22. Meichenbaum DH: Examination of model characteristics in
reducing avoidance behavior. J Pers Soc Psychol 17:298,
1971
23. Scherer MW, Nakamura CY: A fear survey schedule for
children (FSS-FC): A factor analytic comparison with
man-ifest anxiety (CMAS). Behav Res Ther 173, 1968
24. Radloff R, Helmreich R: Groups Under Stress:
Psycholog-ical Research in Sealab II. New York, Appleton-Century-Crofts, 1968
25. Goldstein IB: Role of muscle tension in personality theory.
Psychol Bull 61:413, 1964
26. Goldstein IB: Electromyography: A measure ofskeletal
mus-cle response, in Greenfield NS (ed): Handbook of
Psycho-physiology. New York, Holt, Rinehart and Winston, 1972
27. Voas RB: Generalization and Consistency ofMuscle
Ten-sion Level, thesis. Los Angeles, University ofCalifornia, 1952 28. Lippold OCJ: Electromyography, in Venables PH, Martin I
(eds): A Manual of Psychophysiological Methods.
Amster-dam, North Holland Publishing Co, 1967
29. Vernon DTA, Schulman JL, Foley JM: Changes in children’s
behavior after hospitalization. Am JDiS Child 111:581, 1966
30. Freiberg KH: How parents react when their child is
hospi-talized. Am J Nurs 72:1270, 1972
31. Melamed BC, Meyer R, Gee C, et a!: The influence of time
and type of presentation on children’s adjustment to
hospi-talization. J Pediatr Psychol 5:31, 1976
32. Epstein S, Rouperman A: Heart rate and skin conductance
during experimentally induced anxiety: The effect of
uncer-tainty about receiving a noxious stimulus. J Pers Soc Psy.