SPECIAL ARTICLE
The Human Capacity to Thrive in the Face of
Potential Trauma
George A. Bonanno, PhD, Anthony D. Mancini, PhD
Department of Counseling and Clinical Psychology, Teachers College, Columbia University, New York, New York
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
For decades, researchers have documented remarkable levels of resilience in children who were exposed to corrosive early environments, such as those in which poverty or chronic maltreatment were present; however, relatively little research has exam-ined resilience in children or adults who were exposed to isolated and potentially traumatic events. The historical emphasis on psychological and physiologic dysfunc-tion after potentially traumatic events has suggested that such events almost always produce lasting emotional damage. Recent research, however, has consistently shown that across different types of potentially traumatic events, including bereave-ment, serious illness, and terrorist attack, upward of 50% of people have been found to display resilience. Research has further identified substantial individual variation in response to potentially traumatic events, including 4 prototypical and empirically derived outcome trajectories: chronic dysfunction, recovery, resilience, and delayed reactions. Factors that promote resilience are heterogeneous and include a variety of person-centered variables (eg, temperament of the child, personality, coping strate-gies), demographic variables (eg, male gender, older age, greater education), and sociocontextual factors (eg, supportive relations, community resources). It is surpris-ing that some factors that promote resilience to potentially traumatic events may be maladaptive in other contexts, whereas other factors are more broadly adaptive. Given the growing evidence that resilience is common, psychotherapeutic treatment should be reserved for those in genuine need.
B
AD THINGS HAPPEN.As much as we might wish otherwise, close friends and relatives die, painful things happento our bodies, there are natural disasters and wars, and sometimes people do senselessly horrible things to other people. Epidemiologic studies indicate that most adults experience at least 1 potentially traumatic event (PTE) during
the course of their life.1Children are also commonly exposed to such events.2Perhaps owing to the way these events
are dreaded, it has become a common assumption that they almost always cause lasting emotional damage, but this is usually not true. In this article, we use the phrase “potentially traumatic” to underscore that there are measurable
and important individual differences in how people respond to such events.3Simply put, highly aversive events that
typically fall outside the range of normal everyday experience are “potentially” traumatic because not everyone experiences them as traumatic. Research on PTEs has consistently revealed a wide range of reactions; apart from a relatively finite subset of people who experience extreme distress, most people cope with such events extremely
well.3,4 In this article, we briefly review the historical background on psychological trauma, then consider recent
empirical studies on individual differences in response to PTEs. We consider the most common or prototypical outcomes that people exhibit, including chronic and pathologic reactions, but also relatively healthy reactions. We focus particular on the growing evidence for the human capacity to thrive even after the most difficult of events and on the emergent concept of psychological resilience. Finally, we review the available evidence on factors that predict resilience to PTEs, suggest ways in which these data might inform a more empirically sound public health conception of trauma, and discuss the implications of the study of resilience for treatment.
TRADITIONAL CONCEPTS OF PSYCHOLOGICAL TRAUMA
Almost since the beginnings of psychology and psychiatry as formal disciplines, researchers, theorists, and practi-tioners have looked to violent or life-threatening events as antecedents to psychological and physiologic
dysfunc-www.pediatrics.org/cgi/doi/10.1542/ peds.2007-1648
doi:10.1542/peds.2007-1648
Key Words
resilience, posttraumatic stress disorder, death and dying, psychological adaptation, child, child development
Abbreviations
PTE—potentially traumatic event PTSD—posttraumatic stress disorder
Accepted for publication Jul 16, 2007
Address correspondence to George A. Bonanno, PhD, Department of Counseling and Clinical Psychology, Teachers College, Columbia University, 525 W 120th St, New York, NY 10027. E-mail: [email protected]
tion5,6; however, it was not until late in the 20th century
that consensus emerged about the nature of trauma-related dysfunction. The formalization of posttraumatic stress disorder (PTSD) as a legitimate diagnostic category
in 19807filled an enormous gap in public health
knowl-edge. The PTSD category also helped promote a surge of
new research on traumatic stress.8
Unfortunately, the nearly exclusive emphasis on PTSD also had a down side. With little attention devoted to anything other than PTSD, reactions to PTEs were conceptualized in increasingly simplistic, binary terms of pathology versus the absence of pathology. With this simplistic view came lingering controversies about the sometimes elusive distinction between genuine psycho-logical trauma and malingering. Nowhere does this issue cut closer to the bone than in the case of war trauma. Warfare throughout the 20th century was plagued by an enduring tension about the proper time and place for
diagnosis or treatment,6,9and these issues have persisted
into the 21st century. One survey10found, for example,
that many soldiers who returned from combat opera-tions in Iraq and Afghanistan desired but did not seek treatment because of prevailing stigma about percep-tions of weakness.
The bereavement literature has evidenced a similar historical confusion among grief, healthy functioning, and denial. As was the case with trauma, bereavement research has tended to emphasize chronic grief reactions while offering little insight about possible resilience to loss. A summary of current bereavement knowledge in the 1980s reported that it was commonly assumed, par-ticularly by clinicians, “that the absence of grieving phe-nomena following bereavement represents some form of
personality pathology.”11(p18) Bowlby12(p138)
consid-ered the “prolonged absence of conscious grieving” a type of disordered mourning. A 1993 survey of self-identified bereavement experts reported that a majority (65%) endorsed beliefs that “absent grief” exists, that it usually stems from denial or inhibition, and that it is
generally maladaptive in the long run.13
TOWARD AN INDIVIDUAL-DIFFERENCES MODEL
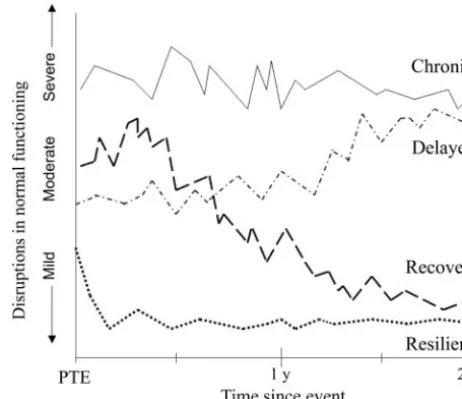
A stark contrast to the binary view of traumatic stress is offered by empirical studies of individual variation in response to PTEs. These studies reveal a number of unique and variable patterns or outcome trajectories. Most of the variability can be capture by 4 prototypical trajectories: chronic dysfunction, recovery, resilience,
and delayed reactions (Fig 1).4 We elaborate on each
trajectory next.
Chronic Dysfunction
Despite the highly aversive nature of most PTEs, only a relatively small subset of exposed individuals typically exhibit chronic psychopathology. Although there is con-siderable variability in the type, severity, and duration of
PTEs,14 typically PTSD is observed in 5% to 10% of
exposed individuals.1 When exposure is exceptionally
prolonged or severe, the proportion who exhibit PTSD or other types of psychopathology may reach higher levels,
sometimes as high as one third of the sample. For ex-ample, among a representative sample of 2752 New Yorkers who were interviewed in the months after the September 11th terrorist attack, the PTSD prevalence
was estimated at 6%.15Among those physically injured
in the attack, however, PTSD prevalence was 26%. In a careful reanalysis of the National Vietnam Veterans Re-adjustment data, a representative sample of 1200 veter-ans, chronic PTSD was estimated at 9% but rose to 28% among veterans with the highest levels of combat expo-sure.16
Studies of psychopathology during bereavement suggest
similar proportions. Typically only⬃10% of bereaved
peo-ple will exhibit chronically elevated grief reactions17;
how-ever, chronic grief reactions tend to be more prevalent after more extreme losses, such as when the death event in-volves violence18,19or when a child dies.20
It is surprising that there are relatively few data on trauma and grief reactions among children; however, the child data that are available suggest similar levels of
complicated grief21 but somewhat less PTSD compared
with adults.2As we discuss next, however, it is important
to keep in mind that the question of adjustment is in many ways more complex among children. For exam-ple, children who are exposed to aversive events may fail to evidence PTSD or complicated grief but show in-creased externalizing symptoms, substance use, aca-demic problems, or peer conflict.
Delayed Reactions
What about delayed reactions? A long-held assumption in the bereavement literature is that the absence of overt signs of grieving will eventually manifest in delayed grief
reactions.11–13,22–25 Despite the strength of this belief,
however, empirical evidence for delayed grief has never
been reported,26,27even in longitudinal studies explicitly
designed to measure the phenomenon.28,29There is some
FIGURE 1
evidence for delayed PTSD reactions after potentially
traumatic events, occurring in⬃5% to 10% of exposed
individuals.30,31It is crucial to note, however, that this
pattern does not conform to the traditional idea of denial manifesting in delayed reactions. Rather, when it is ob-served, delayed PTSD seems to resemble more closely subthreshold psychopathology that gradually grew
worse over time.4,30,31
Resilience and Recovery
Until recently, it was widely assumed that the enduring absence of psychopathology after exposure to a PTE occurred only in people with exceptional emotional
strength.32–34As noted previously, bereavement theorists
have persistently regarded the relative absence of grief as
a form of hidden psychopathology.14There is now
com-pelling evidence, however, that genuine resilience to PTEs is not rare but common and not a sign of excep-tional strength or psychopathology but rather a
funda-mental feature of normal coping skills.4Moreover,
sev-eral studies have demonstrated that resilience and recovery can be mapped as discrete and empirically sep-arable outcome trajectories. Distinctions between
resil-ience and recovery have been identified after loss,35
ma-jor illness,36and potential trauma.31
DEVELOPMENT OF THE CONSTRUCT OF PSYCHOLOGICAL RESILIENCE
Much of the original theorizing on resilience came from developmental psychologists and psychiatrists during the 1970s. These pioneering researchers documented the large number of children who despite growing up in caustic socioeconomic circumstances (eg, poverty) nonetheless
ev-idenced healthy developmental trajectories.37–40A
surpris-ing feature of this work was that it showed resilience in
children at risk to be common.41Whereas traditional
defi-cit-focused models of development had assumed that only children with remarkable coping ability could thrive in such adverse contexts, these studies suggested that resil-ience is a result of normal human adaptational
mecha-nisms.41As noted previously, however, almost all of this
research focused on chronically aversive contexts, rather than isolated PTEs.
The construct of resilience has slowly “trickled up” to
the trauma literature.4,42 As the idea gained currency
among trauma researchers, differences between resilient outcomes in adults and children and between chronic
and acute stressors became apparent.3,4Some of the key
differences seemed to hinge on the temporal and socio-contextual characteristics of stress and adaptation at dif-ferent points in the lifespan. For developing children, the
definition of healthy adaptation is a complex issue.41,43
Children at risk may evidence competence in 1 domain but fail to meet long-term developmental challenges in
other domains.44This situation is arguably more
straight-forward among adults.3,4Most but certainly not all of the
PTEs with which adults might be confronted can be classi-fied as isolated stressor events (eg, an automobile accident) that occur in a broader context of otherwise normative (ie, low stress) circumstances. There may be concomitant
stres-sors accompanying or extending the PTE (eg, change in financial situation), but this level of variability is usually
straightforward and can be reliably measured.16,45Because
developmental considerations are less pronounced in adults, responses to PTEs can usually be assessed in terms of deviation from or return to normative (baseline) func-tioning.46
On the basis of these considerations, Bonanno4
pro-posed that resilience to potential trauma be defined as “the ability of adults in otherwise normal circumstances who are exposed to an isolated and potentially highly disruptive event such as the death of a close relation or a violent or life-threatening situation to maintain rela-tively stable, healthy levels of psychological and physical functioning, as well as the capacity for generative expe-riences and positive emotions” (p 20 –21). In this article, we propose that this definition be extended to encom-pass children who are exposed to isolated PTEs, with the caveat, however, that evidence for resilience in children typically requires more careful and elaborate monitoring across multiple domains (eg, peer relations, school per-formance). Whether applied to children or adults, this definition contrasts resilience with the traditional recov-ery from trauma pathway characterized by readily ob-servable elevations in psychological problems that en-dure for at least several months or longer before gradually returning to baseline, pretrauma levels.
A key point is that even resilient individuals may experience at least some form of transient stress reac-tion; however, these reactions are usually mild to mod-erate in degree, are relatively short-term, and do not significantly interfere with their ability to continue
func-tioning.35,45,47,48This is not to say that people who show
resilient outcomes are not upset, disturbed, or unhappy about the occurrence of the event. Our point is merely that as undesirable as PTEs might be, many people cope with such events extremely well and are able to con-tinue meeting the normal daily demands of their lives.
The earliest observations of resilience in response to isolated PTEs came from retrospective and unsystematic
accounts.42,49More recently, a number of studies have
demonstrated widespread resilience among people con-fronted with the untimely death of a spouse or a
child.35,45Across studies, resilience was consistently
ob-served in approximately half of the bereaved partici-pants. Moreover, the resilient trajectory was validated using different measures of adjustment, including low levels of psychopathologic symptoms, ratings of positive adjustment obtained from close friends, and measures of positive emotional experiences.
Recent studies have demonstrated widespread resil-ience among survivors of the September 11th terrorist attack in New York City. Among a sample of people in or
near the World Trade Center at the time of the attack,31
resilient individuals had little or no symptoms of PTSD or depression. They also showed high levels of adjustment across a number of different domains of functioning (eg, mental health, physical health, goal achievement) on the basis of anonymous ratings that were obtained from close friends and relatives. Another, more encompassing
using data from a large probability sample (N⫽ 2752) that closely matched the more recent New York census data. Resilient individuals had 1 or 0 PTSD symptoms, no depression, and reduced substance use. Consistent with previous studies, the proportion with resilient outcomes
wasⱖ50% across most exposure groups and across most
aspects of demographic variation. Importantly, even among the groups with the most pernicious levels of exposure and highest probable PTSD, the proportion of individuals who were resilient never dropped below one third of the sample.
Similar findings have also begun to emerge after se-rious health-related stressors. Among a large sample of hospitalized survivors of the 2003 severe acute respira-tory syndrome epidemic in Hong Kong, 42% evidenced chronically low levels of psychological functioning across an 18-month period, but 35% had consistently high levels of psychological functioning across the same
period.50 Deshields et al36 mapped the same outcome
trajectories depicted in Fig 1 using depression scores that were obtained from women immediately after radiation treatment for breast cancer and again 3 and 6 months after treatment. Although 21% of the sample evidenced clinically significant levels of depression at 6 months, the majority (61%) had extremely low levels of depression throughout the study.
A HETEROGENEOUS ARRAY OF RISK AND PROTECTIVE FACTORS
We next turn to the questions of why some people are more or less likely to be resilient after a specific PTE. The initial pioneering research on resilience in children sug-gested that there are multiple protective factors that might buffer against adversity, including person-centered vari-ables (eg, temperament) and sociocontextual factors (eg,
supportive relations, community resources).39,51,52Research
on resilience among adults who were exposed to isolated
PTEs suggests a similar conclusion.3,53A particularly
com-pelling aspect of this story is that resilience does not result from any 1 dominant factor. Rather, there seem to be multiple independent risk and protective factors, each con-tributing to or subtracting from the overall likelihood of a resilient outcome. Consider, for example, an enduring mis-conception that resilience depends almost exclusively on qualities in the person. Personality undoubtedly does play
a role in resilience to trauma; however, as Mischel54
fa-mously observed, personality rarely explains⬎10% of the
actual variance in people’s behavior across situations. It is more accurate, therefore, to conceive of personality as 1 of many potential contributors to resilient outcomes.
Flexible Adaptation and Pragmatic Coping
We recently proposed a basic grouping of person-cen-tered factors into 2 broad categories: pragmatic coping
and flexible adaptation.3,55 Because PTEs usually occur
outside the range of normal human experience, they often pose unique and highly specific coping demands. Successfully meeting these demands may require a highly pragmatic, or “whatever it takes,” approach that is single-minded and goal-directed. Sometimes
prag-matic coping involves behaviors that under normal cir-cumstances may be less effective or even maladaptive. We have also referred to this type of coping as “coping
ugly”3to underscore the idea that coping does not
nec-essary need to be a thing of beauty; it just needs to get the job done.
Pragmatic coping can also be observed as a conse-quence of relatively rigid personality characteristics. For example, the construct of trait self-enhancement de-scribes people who are narcissistic and habitually use self-serving biases. Trait self-enhancers tend to evoke negative reactions in other people; however, they also have high self-esteem and cope well with isolated PTEs,
such as war56 and terrorist attack.31 Another group of
individuals, known as repressive copers, tend to avoid unpleasant emotional experiences. Although there is ev-idence linking repressive coping to health deficits, they have also been found to cope extremely well with
PTEs.57,58 The confluence of costs and benefits that are
associated with these personality types suggests that
they may be something of a “mixed blessing.”59
A more genuinely health personality dimension is suggested by the concept of adaptive flexibility. A core aspect of flexibility is the capacity to shape and modify one’s behavior to meet the demands of a given stressor event. This capacity for flexibility has been observed very early in development yet can change over time as a result of the dynamic interplay of personality and social
interactions with key attachment figures.60 Practically
speaking, then, flexibility is a personality resource that helps bolster resilience to aversive events, such as
child-hood maltreatment,61 but may also be enhanced or
re-duced by developmental experiences.62Recent research
also suggests that flexibility eventually becomes stable
and can effectively bolster resilience to PTEs.63,64
Exposure
As described previously, the type, duration, and inten-sity of exposure during a PTE has been shown to influ-ence the prevalinflu-ence of healthy adjustment, with
resil-ience varying from 33% to ⬎50% across exposure
categories.3,16
Demographic Variables
A more prosaic set of predictors is found in simple de-mographic variation. Resilience to trauma has been as-sociated with male gender, older age, and greater
edu-cation.50,65 Although there has been relatively little
research on race/ethnicity as a predictor of resilience, recent evidence indicated that ethnic Chinese were more
likely to be resilient after the September 11th attack.65
Personal and Social Resources
Numerous theorists have delineated a crucial role for social
and personal resources in coping with stress.53,66,67There is
also considerable research linking resources or change in
resources with adjustment after PTEs.68–71Recent research
been widely observed as a protective resource against PTSD
in both children72and adults.73Although there are not yet
data linking cognitive resources to resilience in the face of trauma, we suspect that such a link is highly probable.
Additional Life Stress
There is abundant evidence linking PTSD with increased
life stress before and after the marker traumatic event.73,74
Resilience to trauma has been associated with the relative
absence of current and previous life stress.65An important
qualifier of these findings, however, is the outcome of previous life stressors. Prospective research suggests that only previous stressors that result in PTSD tend to predict
PTSD at subsequent exposure.75 It seems likely also that
resilience to past stressors will predict subsequent resil-ience.
IMPLICATIONS FOR INTERVENTION
The burgeoning literature on resilience has important implications for how physicians, mental health profes-sionals, and close others respond to people who are exposed to a PTE. Although in many ways a deeply ingrained cultural assumption that psychotherapeutic intervention for PTEs is invariably beneficial, the study of resilience suggests that this assumption is misguided and could even lead to harm. For most people, intrinsic recovery processes will restore equilibrium relatively soon after exposure. Early interventions, such as critical incident stress debriefing, targeted indiscriminately at people immediately after exposure to a PTE, are not only ineffective but also may exacerbate trauma reactions by
interfering with natural recovery processes.76Moreover,
although a recently developed intervention has shown
promise for treating chronic forms of grief,77traditional
grief counseling models, which have defined grieving as “work,” have also had a notoriously poor track record, achieving small gains for some but exposing others to
significant risk for deterioration.78
Although people who experience trauma-related psy-chopathology clearly benefit from empirically validated psychotherapeutic treatments, the study of resilience makes clear that such people are only a small minority; the far greater majority are not appropriate candidates for intervention. For this reason, appropriate assessment and, by extension, diagnosis are perhaps the central task before referral, as would be the case in the treatment of disease. Indeed, only people who evidence genuine dys-function in the face of PTEs, as defined by recurring symptoms and interference with social roles and obliga-tions, should be referred for treatment. Although the general efficacy of psychotherapeutic intervention is now beyond question, this does not preclude the possi-bility of iatrogenic effects, as witnessed in traditional grief treatments and blanket early interventions after PTEs. This cautionary note only underscores the impor-tance of seeing resilient responses to PTEs as a basic human capability—neither rare nor extraordinary.
REFERENCES
1. Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumatic stress disorder in the National Comorbidity Sur-vey.Arch Gen Psychiatry.1995;52(12):1048 –1060
2. Copeland WE, Keeler G, Angold A, Costello EJ. Traumatic events and posttraumatic stress in childhood.Arch Gen Psychi-atry.2007;64(5):577–584
3. Bonanno GA. Resilience in the face of potential trauma.Curr Dir Psychol Sci.2005;14(3):135–138
4. Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events?Am Psychol.2004;59(1):20 –28
5. Ellenberger HF. The Discovery of the Unconscious: History and Evolution of Dynamic Psychiatry. New York, NY: Basic Books; 1970
6. Lamprecht F, Sack M. Posttraumatic stress disorder revisited. Psychosom Med.2002;64(2):222–237
7. Association AP.Diagnostic and Statistical Manual of Mental Disorders. 3rd ed. Washington, DC: American Psychiatric Association; 1980 8. McNally RJ. Progress and controversy in the study of
posttrau-matic stress disorder.Annu Rev Psychol.2003;54:229 –252 9. Shepard B. A War of Nerves: Soldiers and Psychiatrists in the
Twentieth Century. Cambridge, MA: Harvard University Press; 2001
10. Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koff-man RL. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med. 2004;351(1): 13–22
11. Osterweis M, Solomon F, Green F.Bereavement: Reactions, Con-sequences, and Care. Washington, DC: National Academy Press; 1984
12. Bowlby J.Loss: Sadness and Depression.Vol 3: Attachment and Loss. New York, NY: Basic Books; 1980
13. Rando TA.Treatment of Complicated Mourning. Champaign, IL: Research Press; 1993
14. Association AP.Diagnostic and Statistical Manual of Mental Disor-ders.4th ed, Text Revision. Washington, DC: American Psychi-atric Association; 2000
15. Bonanno GA, Galea S, Bucciarelli A, Vlahov D. Psychological resilience after disaster: New York City in the aftermath of the September 11th terrorist attack. Psychol Sci. 2006;17(3): 181–186
16. Dohrenwend BP, Turner JB, Turse NA, Adams BG, Koenen KC, Marshall RD. The psychological risks of Vietnam for U.S. veterans: a revisit with new data and methods.Science.2006; 313(5789):979 –982
17. Bonanno GA, Kaltman S. The varieties of grief experience.Clin Psychol Rev.2001;21(5):705–734
18. Kaltman S, Bonanno GA. Trauma and bereavement: examin-ing the impact of sudden and violent deaths.J Anxiety Disord. 2003;17(2):131–147
19. Zisook S, Chentsova-Dutton Y, Shuchter SR. PTSD following bereavement.Ann Clin Psychiatry.1998;10(4):157–163 20. Bonanno GA, Papa A, Lalande K, Zhang N, Noll JG. Grief
processing and deliberate grief avoidance: a prospective com-parison of bereaved spouses and parents in the United States and the People’s Republic of China. J Consult Clin Psychol. 2005;73(1):86 –98
21. Christ GH. Healing Children’s Grief: Surviving a Parent’s Death From Cancer. New York, NY: Oxford University Press; 2000 22. Middleton W, Moylan A, Raphael B, Burnett P, Martinek N.
An international perspective on bereavement related concepts. Aust N Z J Psychiatry.1993;27(3):457– 463
23. Deutsch H. Absence of grief.Psychoanal Q.1937;6:12–22 24. Parkes CM, Weiss RS. Recovery From Bereavement. New York,
NY: Basic Books; 1980
MS, Stroebe W, Hansson RO, eds.Handbook of Bereavement: Theory, Research, and Intervention. Cambridge, England: Cam-bridge University Press; 1993:255–267
26. Bonanno GA, Kaltman S. Toward an integrative perspective on bereavement.Psychol Bull.1999;125(6):760 –776
27. Wortman CB, Silver RC. The myths of coping with loss. J Consult Clin Psychol.1989;57(3):349 –357
28. Bonanno GA, Field NP. Examining the delayed grief hypoth-esis across 5 years of bereavement.Am Behav Sci.2001;44(5): 798 – 816
29. Middleton W, Burnett P, Raphael B, Martinek N. The bereave-ment response: a cluster analysis.Br J Psychiatry.1996;169(2): 167–171
30. Buckley TC, Blanchard EB, Hickling EJ. A prospective exami-nation of delayed onset PTSD secondary to motor vehicle ac-cidents.J Abnorm Psychol.1996;105(4):617– 625
31. Bonanno GA, Rennicke C, Dekel S. Self-enhancement among high-exposure survivors of the September 11th terrorist attack: resilience or social maladjustment? J Pers Soc Psychol. 2005; 88(6):984 –998
32. Tucker P, Pfefferbaum B, Doughty DE, Jones DE, Jordan FB, Nixon SJ. Body handlers after terrorism in Oklahoma City: predictors of posttraumatic stress and other symptoms.Am J Orthopsychiatry.2002;72(4):469 – 475
33. McFarlane AC, Yehuda R. Resilience, vulnerability, and the course of posttraumatic reactions. In: van der Kolk BA, McFar-lane AC, Weisaeth L, eds. Traumatic Stress. New York, NY: Guilford; 1996:155–181
34. Casella L, Motta RW. Comparison of characteristics of Vietnam veterans with and without posttraumatic stress disorder. Psy-chol Rep.1990;67(2):595– 605
35. Bonanno GA, Wortman CB, Lehman DR, et al. Resilience to loss and chronic grief: a prospective study from preloss to 18-months postloss.J Pers Soc Psychol.2002;83(5):1150 –1164 36. Deshields T, Tibbs T, Fan MY, Taylor M. Differences in patterns
of depression after treatment for breast cancer.Psychooncology. 2006;15(5):398 – 406
37. Rutter M. Protective factors in children’s responses to stress and disadvantage. In: Kent MW, Rolf JE, eds.Primary Preven-tion of Psychopathology: Social Competence in Children. Vol 3. Hanover, NH: University Press of New England; 1979:49 –74 38. Garmezy N. Resilience and vulnerability to adverse
develop-mental outcomes associated with poverty.Am Behav Sci.1991; 34(4):416 – 430
39. Werner EE. Resilience in development. Curr Dir Psychol Sci. 1995;4(3):81– 85
40. Murphy LB, Moriarty AE. Vulnerability, Coping, and Growth. New Haven, CT: Yale University Press; 1976
41. Masten AS. Ordinary magic: resilience processes in develop-ment.Am Psychol.2001;56(3):227–238
42. Rachman SJ.Fear and Courage. New York, NY: Freeman; 1978 43. Luthar SS, Cicchetti D, Becker B. The construct of resilience: a critical evaluation and guidelines for future work.Child Dev. 2000;71(3):543–562
44. Luthar SS, Doernberger CH, Zigler E. Resilience is not a uni-dimensional construct: insights from a prospective study of inner-city adolescents.Dev Psychopathol.1993;5(4):703–717 45. Bonanno GA, Moskowitz JT, Papa A, Folkman S. Resilience to
loss in bereaved spouses, bereaved parents, and bereaved gay men.J Pers Soc Psychol.2005;88(5):827– 843
46. Carver CS. Resilience and thriving: issues, models, and link-ages.J Soc Issues.1998;54(2):245–266
47. Bisconti TL, Bergeman CS, Boker SM. Social support as a predictor of variability: an examination of the adjustment tra-jectories of recent widows.Psychol Aging.2006;21(3):590 –599 48. Ong AD, Bergeman CS, Bisconti TL, Wallace KA. Psychological
resilience, positive emotions, and successful adaptation to stress in later life.J Pers Soc Psychol.2006;91(4):730 –749 49. Janis IL.Air War and Emotional Stress. New York, NY: McGraw
Hill; 1951
50. Bonanno GA, Ho SMY, Chan JCK, et al. Psychological resil-ience and dysfunction among hospitalized survivors of the SARS epidemic in Hong Kong: a latent class approach.Health Psychol.In press
51. Cowen EL. In pursuit of wellness. Am Psychol. 1991;46(4): 404 – 408
52. Rutter M. Resilience concepts and findings: implications for family therapy.J Fam Ther.1999;(2):119 –144
53. Hobfoll SE. Social and psychological resources and adaptation. Rev Gen Psychol.2002;6(4):307–324
54. Mischel W. Continuity and change in personality.Am Psychol. 1969;24(11):1012–1018
55. Mancini AD, Bonanno GA. Resilience in the face of potential trauma: clinical practices and illustrations.J Clin Psychol.2006; 62(8):971–985
56. Bonanno GA, Field NP, Kovacevic A, Kaltman S. Self-enhancement as a buffer against extreme adversity: civil war in Bosnia and traumatic loss in the United States.Pers Soc Psychol Bull.2002;28(2):184 –196
57. Coifman KG, Bonanno GA, Ray RD, Gross JJ. Does repressive coping promote resilience? Affective-autonomic response dis-crepancy during bereavement.J Pers Soc Psychol.2007;92(4): 745–758
58. Bonanno GA, Keltner D, Holen A, Horowitz MJ. When avoid-ing unpleasant emotions might not be such a bad thavoid-ing: verbal-autonomic response dissociation and midlife conjugal bereave-ment.J Pers Soc Psychol.1995;69(5):975–989
59. Paulhus DL. Interpersonal and intrapsychic adaptiveness of trait self-enhancement: a mixed blessing? J Pers Soc Psychol. 1998;74(5):1197–1208
60. Block J, Block JH. Venturing a 30-year longitudinal study.Am Psychol.2006;61(4):315–327
61. Flores E, Cicchetti D, Rogosch FA. Predictors of resilience in maltreated and nonmaltreated Latino children. Dev Psychol. 2005;41(2):338 –351
62. Shonk SM, Cicchetti D. Maltreatment, competency deficits, and risk for academic and behavioral maladjustment.Dev Psy-chol.2001;37(1):3–17
63. Fredrickson BL, Tugade MM, Waugh CE, Larkin GR. What good are positive emotions in crisis? A prospective study of resilience and emotions following the terrorist attacks on the United States on September 11th, 2001. J Pers Soc Psychol. 2003;84(2):365–376
64. Bonanno GA, Papa A, Lalande K, Westphal M, Coifman K. The importance of being flexible: the ability to both enhance and suppress emotional expression predicts long-term adjustment. Psychol Sci.2004;15(7):482– 487
65. Bonanno GA, Galea S, Bucciarelli A, Vlahov D. What predicts psychological resilience after disaster? The role of demograph-ics, resources, and life stress.J Consult Clin Psychol.2007;75(5): 671– 682
66. Murrell SA, Norris FH. Resources, life events, and changes in psychological states: a prospective framework.Am J Community Psychol.1983;11(5):473– 491
67. Holahan CJ, Moos RH. Life stressors, personal and social re-sources, and depression: a 4-year structural model.J Abnorm Psychol.1991;100(1):31–38
68. Freedy JR, Shaw DL, Jarrell MP, Masters CR. Towards an understanding of the psychological impact of natural disasters: an application of the conservation resources stress model. J Trauma Stress.1992;5(3):441– 454
stress symptoms, intrusive thoughts, loss, and immune function after Hurricane Andrew.Psychosom Med.1997;59(2):128 –141 70. Norris FH, Kaniasty K. Received and perceived social support
in times of stress: a test of the social support deterioration deterrence model.J Pers Soc Psychol.1996;71(3):498 –511 71. Kaniasty K, Norris FH. A test of the social support deterioration
model in the context of natural disaster. J Pers Soc Psychol. 1993;64(3):395– 408
72. Breslau N, Lucia VC, Alvarado GF. Intelligence and other pre-disposing factors in exposure to trauma and posttraumatic stress disorder.Arch Gen Psychiatry.2006;63(11):1238 –1245 73. Brewin CR, Andrews B, Valentine JD. Meta-analysis of risk
factors for posttraumatic stress disorder in trauma-exposed adults.J Consult Clin Psychol.2000;68(5):748 –766
74. Kubiak SP. Trauma and cumulative adversity in women of a disad-vantaged social location.Am J Orthopsychiatry.2005;75(4):451–465 75. Breslau N. Epidemiologic studies of trauma, posttraumatic
stress disorder, and other psychiatric disorders.Can J Psychiatry. 2002;47(10):923–929
76. Litz BT, Gray MJ, Bryant RA, Adler AB. Early intervention for trauma: current status and future directions.Clin Psychol Sci Pract.2002;9(2):112–134
77. Shear K, Frank E, Houck PR, Reynolds CF. Treatment of com-plicated grief: a randomized controlled trial. JAMA. 2005; 293(21):2601–2608
78. Neimeyer RA. Searching for the meaning of meaning: grief therapy and the process of reconstruction.Death Stud.2000; 24(6):541–558
A LIFESAVING CHECKLIST: WASHINGTON IS BLOCKING RESEARCH ON A PROMISING MEDICAL TOOL
“In Bethesda, MD, in a squat building off a suburban parkway, sits a small federal agency called the Office for Human Research Protections. Its aim is to protect people. But lately you have to wonder. Consider this recent case. A year ago, researchers at Johns Hopkins University published the results of a program that instituted in nearly every intensive care unit in Michigan a simple five-step checklist designed to prevent certain hospital infections. It reminds doctors to make sure, for example, that before putting large intra-venous lines into patients, they actually wash their hands and don a sterile gown and gloves. The results were stunning. Within three months, the rate of bloodstream infections from these IV lines fell by two-thirds. The average ICU cut its infection rate from 4 percent to zero. Over 18 months, the program saved more than 1,500 lives and nearly $200 million. Yet this past month, the Office for Human Research Protections shut the program down. The agency issued notice to the researchers and the Michigan Health and Hospital Asso-ciation that, by introducing a checklist and tracking the results without written, informed consent from each patient and health-care provider, they had violated scientific ethics regulations. Johns Hopkins had to halt not only the program in Michigan but also its plans to extend it to hospitals in New Jersey and Rhode Island. The government’s decision was bizarre and dan-gerous. But there was a certain blinkered logic to it, which went like this: A checklist is an alteration in medical care no less than an experimental drug is. Studying an experimental drug in people without federal monitoring and explicit written permission from each patient is unethical and illegal. There-fore it is no less unethical and illegal to do the same with a checklist.”
DOI: 10.1542/peds.2007-1648
2008;121;369
Pediatrics
George A. Bonanno and Anthony D. Mancini
The Human Capacity to Thrive in the Face of Potential Trauma
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/2/369 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/2/369#BIBL This article cites 62 articles, 4 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/trauma_sub Trauma
sub
http://www.aappublications.org/cgi/collection/emergency_medicine_ Emergency Medicine
ub
http://www.aappublications.org/cgi/collection/psychosocial_issues_s Psychosocial Issues
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2007-1648
2008;121;369
Pediatrics
George A. Bonanno and Anthony D. Mancini
The Human Capacity to Thrive in the Face of Potential Trauma
http://pediatrics.aappublications.org/content/121/2/369
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.