Daytime Functioning
WHAT’S KNOWN ON THIS SUBJECT: Breastfed infants are reported to awaken more often and to sleep less. Because of its well-established benefits for both infants and mothers, any perceived disadvantage of breastfeeding should be evaluated carefully. Feeding method effects on maternal sleep are relatively unknown.
WHAT THIS STUDY ADDS: We did not find any objective, subjective, or sleepiness/fatigue differences among women who used different feeding methods. The risks of not breastfeeding should be weighed against the cumulative lack of evidence of any benefit of formula feeding on maternal sleep.
abstract
OBJECTIVE:Our purpose was to explore maternal actigraphically mea-sured sleep, subjective sleep reports, and daytime functioning on the basis of current feeding method status during postpartum weeks 2 through 12.
METHODS:Objectively measured total sleep time, sleep efficiency, and fragmentation, subjectively reported numbers of nocturnal awaken-ings, total nocturnal wake time, and sleep quality, and sleepiness/ fatigue measured by using the fatigue visual analog scale, the Stanford Sleepiness Scale, or the Epworth Sleepiness Scale were assessed.
RESULTS:We did not find differences between women who were exclu-sively breastfeeding, excluexclu-sively formula feeding, or using a combina-tion of the 2 methods, with respect to the assessed parameters.
CONCLUSIONS:Efforts to encourage women to breastfeed should in-clude information about sleep. Specifically, women should be told that choosing to formula feed does not equate with improved sleep. The risks of not breastfeeding should be weighed against the cumulative lack of evidence indicating any benefit of formula feeding on maternal sleep.Pediatrics2010;126:e1562–e1568
AUTHORS:Hawley E. Montgomery-Downs, PhD,aHeather
M. Clawges, MD, IBCLC, D-ABSM,band Eleanor E. Santy,
BAa
Departments ofaPsychology andbPediatrics, (School of Medicine), West Virginia University, Morgantown, West Virginia
KEY WORDS
infant, breastfeeding, formula, sleep, postpartum, maternal
ABBREVIATIONS
AAP—American Academy of Pediatrics PDA—personal digital assistant
www.pediatrics.org/cgi/doi/10.1542/peds.2010-1269 doi:10.1542/peds.2010-1269
Accepted for publication Sep 3, 2010
Address correspondence to Hawley E. Montgomery-Downs, PhD, West Virginia University, Department of Psychology, 53 Campus Dr, PO Box 6040, Morgantown, WV 26506-6040. E-mail: hawley. [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2010 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
The cumulative evidence supporting the benefits of breastfeeding is so sig-nificant that the American Academy of Pediatrics (AAP) 2005 policy statement concludes, “the AAP firmly adheres to the position that breastfeeding en-sures the best possible health as well as the best developmental and psychoso-cial outcomes for the infant. Enthusiastic support and involvement of pediatri-cians in the promotion and practice of breastfeeding is essential to the achieve-ment of optimal infant and child health, growth, and development.”1
Because of its well-established bene-fits for both infants and mothers,2
any perceived disadvantage of breastfeeding should be evaluated carefully. One obstacle to a woman’s decision to breastfeed may be con-cern about how breastfeeding will affect her sleep. Panchula recom-mends that, “We will want to reas-sure her that she will do fine with less sleep (don’t we all?) and edu-cate her about the important and very real needs of her infant, who is still an immature being not yet ready to be independent.”3A growing body
of evidence shows that mothers may not, in fact, “do fine with less sleep.”
Postpartum affect4,5is related to sleep
and fatigue to the extent that that Fisher et al6proposed that postpartum affect is
on a continuum indistinct from fatigue. Although distinguishing the cause-effect relationship between postpartum sleep and depression has been difficult,7
frag-mented sleep as a cause of negative af-fect is supported by evidence that im-provements in infant sleep lead to improvements in maternal depres-sion.7–9 Maternal sleep disturbance
also may have a negative impact on in-fants; maternal depression is predic-tive of worse infant-parent interac-tions and infant emotional and cognitive outcomes,10–12 failure to
thrive, and greater behavioral, emo-tional, and social problems.13
Although the benefits of breastfeeding are undisputed, mothers’ concerns about how feeding methods might af-fect their sleep are legitimate and should be met with understanding, and mothers should be given the most-current evidence to help them make decisions regarding feeding methods. There is some subjective evidence from maternal diaries of infant sleep that, compared with formula-fed in-fants, breastfed infants have less total sleep time14–17 and more nighttime
awakenings,15–17 although others
re-ported no differences for either infant sleep measure.18,19The single objective
(actigraphic) study showed more-fragmented infant sleep with in-creased nocturnal breastfeeding.20
The impact of feeding methods on mater-nal sleep has been understudied. By us-ing actigraphy, Gay et al21reported that
breastfeeding mothers spent more time awake during the night but did not differ from formula-feeding mothers with re-spect to total sleep time. In another study, those authors reported that breastfeeding mothers slept⬃40 min-utes more per night.22 Breastfeeding
mothers demonstrated no total sleep time difference when home-based poly-somnography was used, although they did demonstrate lower sleep efficiency and more nocturnal awakenings.23
The objective of our study was to build on this literature by exploring potential dif-ferences between mothers who breast-fed, mothers who formula-breast-fed, and moth-ers who used a combination of the 2 methods, with respect to both objective and subjective measures of maternal sleep and daytime functioning, by using data from a longitudinal, field-based study of the first 3 postpartum months.
METHODS
Participants
The study was approved by the West Virginia University Office of Research Compliance. Women were recruited
prenatally through childbirth classes, community advertisements, and word of mouth. Telephone screening was conducted before administration of in-formed consent procedures and Health Information Portability and Ac-countability Act authorization. Women were excluded from participation and referred for further evaluation and treatment, as appropriate, on the ba-sis of a history of major depressive or anxiety disorder, a score ofⱖ16 on the Center for Epidemiologic Studies De-pression scale,24pregnancy with
mul-tiple fetuses, premature delivery, or in-fant admission to the NICU. All other respondents who were pregnant or whose infants were ⬍1 week of age were recruited for participation.
Data were collected from 2 overlap-ping postpartum phases. The first phase included a convenience sample of primiparous and multiparous women who participated during post-partum weeks 9 through 16. On the ba-sis of the success of the first phase, the second phase was begun earlier in the postpartum period, lasted for a longer time, and included only primiparous women, who participated during post-partum weeks 2 through 13.
After participation, mothers were in-terviewed by a researcher via tele-phone and asked to recall their feeding methods during the first week after birth. If they breastfed their child at any time, they were asked if or when they supplemented with formula and if or when they weaned their child off of breast milk, which yielded 3 groups at each postpartum week, that is, ers who breastfed exclusively, moth-ers who used formula exclusively, and mothers who used a combination of the 2 methods.
Protocol
A member of the research team visited the homes weekly, to give the mothers a new actigraph and a personal digital
ized experience sampling method.25
Objective Sleep Measures (Actigraphy)
Sleep measures were recorded ob-jectively by using continuous wrist actigraphy (Actiwatch-64 [MiniMitter, Bend, OR]). Use of the Actiwatch-64 has been validated for recognition of adult sleep.26–28 The highest-resolution
set-ting (15-second epoch) and validated default wake threshold value (40 movement counts per epoch) were used to interpret movement signals. Periods of nocturnal sleep and day-time naps were identified by partici-pants by using PDA-based sleep diaries (Bruner Consulting, Longmont, CO), which were completed in real time at every bedtime and arising time for nocturnal sleep and diurnal nap peri-ods. The software also has a method for retrospective entries, which are annotated as retrospective. By using the sleep diary, nocturnal sleep peri-ods were identified on the actigraphic signal. The following measures were analyzed for identified sleep periods by using Actiware software (Mini-Mitter): total sleep time, that is, min-utes of sleep between initial sleep onset and final awakening; sleep effi-ciency, that is, proportion of sleep time between initial sleep onset and final awakening; sleep fragmentation index, that is, percent mobile epochs plus the ratio of percent 1-minute immobile bouts to percent mobile.
Subjective Sleep Measures
Each morning, participants used the PDA to report the following. “How many times do you think you woke up last night (drop-down menu of 0 –99)?” “Please indicate how long you were awake last night (total) (fill-in hours and minutes).” “Where 100 is fully rested, please indicate your quality of sleep (Likert scale of 0 –100).”
Stanford Sleepiness Scale, and the Ep-worth Sleepiness Scale were self-administered by using the PDA. Partic-ipants were asked to complete these measures whenever they fed their in-fants during the day.
The fatigue visual analog scale29 is a
100-point scale that was used previ-ously to measure fatigue among post-partum women,21rating, “How
tired/fa-tigued do you feel right now?” (from 0⫽not at all tired/fatigued to 100⫽ very tired/fatigued). The Stanford Sleepiness Scale30 measures how
sleepy subjects feel in their current state (scale of 1–7, with 1 ⫽feeling active, vital, alert, or wide awake and 7⫽no longer fighting sleep, sleep on-set soon, or having dream-like thoughts); scores of ⱖ3 indicate ex-treme sleepiness. The Epworth Sleepi-ness Scale31measures subjects’
likeli-hood of falling asleep (with a scale of 0 –3), in each of 8 different real-life sit-uations. Total scores on this scale can range from 0 to 24, and scores of⬎10 indicate extreme sleepiness. The Ep-worth Sleepiness Scale typically is used to reflect trait-like behavior in the past month, but for this study we used this measure to reflect present state.
Statistical Analyses
Feeding methods (breastfeeding, for-mula feeding, or both) were identified for each postpartum week and com-pared with outcomes during the same week. To reduce the number of analy-ses and to avoid type 2 errors, we ex-amined only postpartum weeks 2, 4, 6, 8, 10, and 12. In other words, if a mother began formula supplementa-tion at week 4 and then weaned from breast milk entirely at week 7, she was categorized as breastfeeding during week 2, using both methods during weeks 4 and 6, and formula feeding at week 8. Each participant’s objective
tion), subjective sleep measures (noc-turnal awakenings, total wake time, and sleep quality), and daytime func-tioning measures (fatigue visual ana-log scale, Stanford Sleepiness Scale, and Epworth Sleepiness Scale results) were averaged within each postpar-tum week. At least 4 nights of record-ing were required for calculation of each participant’s weekly average.
Data were analyzed with SPSS 16.0 (SPSS Inc, Chicago, IL). Descriptive sta-tistics were calculated. One-way analy-sis of variance was used to determine statistically significant differences be-tween feeding method groups with re-spect to outcome measures at each week. Results were considered statis-tically significant atP⬍.05. Cohen’sd was used to describe effect sizes, with the conventional interpretation ofd⫽ 0.2 being considered small,d⫽0.5 be-ing considered medium, andd⫽0.8 being considered large.32Data on
fig-ures are shown as mean⫾SEM.
Because this was an exploratory study and the results were negative, we per-formed a posthoc power analysis. With 80 participants and a 2-tailed␣value of⬍.05, we had power of 0.94 to find a strong effect size (d⫽0.8) and power of 0.60 to find a moderate effect size (d⫽0.5). Therefore, with our current sample size, we would expect to find a true difference (P⬍ .05) 60% of the time if it was moderate and 94% of the time if it was strong.
RESULTS
contact were younger (P⫽.004), had fewer years of education (P⬍.001), had lower incomes (P ⬍ .001), and were less likely to be breastfeeding at the beginning of the study (contacted, 80%; unable to be contacted, 54%; P⫽.035). Mothers whom we could not contact were not statistically different with respect to marital status or delivery method. No infant had a birth defect or syndrome (such as trisomy 21) that would be expected to affect feeding.
The analyses presented here are based on data for the remaining 80
subjects. The number of mothers in each of the 3 feeding method groups at each postpartum week and the weekly numbers of sleepiness/fatigue reports they made are presented in Table 1. Participant demographic features are presented in Table 2.
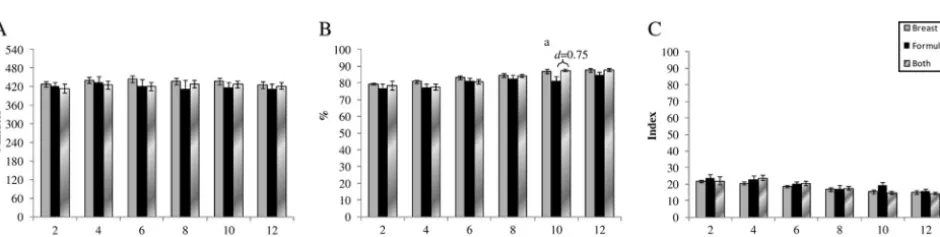
Figure 1 shows the actigraphically re-corded total sleep time, sleep effi-ciency, and sleep fragmentation for the 3 groups at each postpartum week. The only statistically significant differ-ence among these objective sleep mea-sures was on postpartum week 10,
when mothers who used both feeding methods had greater sleep efficiency than did those who used formula feed-ing alone (F⫽5.8;P⫽.021). The effect size was moderate (d⫽0.75).
Figure 2 shows the subjective number of nocturnal awakenings, total noctur-nal wake time, and sleep quality for the 3 groups at each postpartum week. There were no statistically significant differences between groups at any postpartum week with respect to ma-ternal reports of these subjective sleep measures. Despite the lack of statistically significant differences, it seemed that breastfeeding women had more self-reported nocturnal wake time, compared with formula-feeding women, especially at postpar-tum weeks 2, 6, and 8 (Fig 2B). To ex-plore this further, we calculated effect sizes for those 2 groups at each week. Cohn’sdwas 0.88 (strong) at week 2, 0.09 (trivial) at week 4, 0.70 (moder-ate) at week 6, 0.54 (moder(moder-ate) at week 8, 0.18 (trivial) at week 10, and 0.29 (small) at week 12. We suspect that the large variability (shown in the error bars in Fig 2B) accounts for the lack of statistical significance at week 2.
Figure 3 shows the subjective fatigue visual analog scale, Stanford Sleepi-ness Scale, and Epworth SleepiSleepi-ness Scale results for the 3 groups at each postpartum week. Scores on the Stanford Sleepiness Scale among all groups across weeks clustered TABLE 1 Numbers of Mothers Who Fed Their Infants Exclusively Breast Milk, Exclusively Formula,
or Both Breast Milk and Formula and Numbers of Sleep and Sleepiness Reports at Each Postpartum Week
Postpartum Week
n Average No. of
Subjective Sleep Reports
Average No. of Sleepiness/ Fatigue Reports Exclusive
Breastfeeding
Exclusive Formula Feeding
Both Breastfeeding and Formula Feeding
2 43 4 14 6.4 23.2
4 37 7 17 6.3 19.2
6 28 11 22 6.1 18.5
8 26 12 23 6.0 17.5
10 29 15 36 6.3 18.3
12 27 18 35 6.0 17.8
TABLE 2 Participant Demographic Features
Age, mean⫾SD (range), y 27.9⫾4.8 (18.4–40.1) Education, mean⫾SD (range), y 16.5⫾2.7 (10–22) Income, mean⫾SD (range), $ 68 352⫾35 383 (6904–180 000)
Married, % 88.8
White, % 92a
Vaginal delivery, % 75b
Primiparous, % 87c
Term, % 100
aAmerican Indian, 1%; black, 1%; Hispanic, 1%; unreported, 1%; biracial, 4%. bCesarean section, 24%; unreported, 1%.
cSecond child, 9%; third child, 3%; unreported, 1%.
FIGURE 1
Objective measures of total sleep time (A), sleep efficiency (B), and sleep fragmentation (C) among mothers who fed their infants breast milk, formula, or both at each postpartum week.aP⬍.01.
around 3, which indicates “awake, but relaxed; responsive but not fully alert” and represents the generally accepted cutoff point indicating extreme sleepi-ness. Scores on the Epworth Sleepi-ness Scale were generally below the cutoff value of 10. There were no statis-tically significant differences between groups at any postpartum week with respect to maternal reports of these subjective measures of sleepiness or fatigue.
DISCUSSION
We found no differences in measures of objective sleep, subjective sleep, or sleepiness/fatigue between mothers who were breastfeeding, mothers who were formula feeding, and mother who were using a combination of the 2 methods. Negative findings such as ours must have acceptable statistical power to ensure that they are not spu-rious; if we did not have sufficient power, then it would be tempting to make deductions from visual
inspec-tion of our graphs. However, our posthoc power analyses bolster our confidence that, if a moderate to large effect existed, we would have found it within our sample.
Our use of actigraphy makes our ob-jective results most directly compara-ble to those of 2 other studies that used similar methods. One found that breastfeeding mothers spent more time awake during the night but dem-onstrated no total sleep time differ-ences.21 The other reported that
breastfeeding mothers slept an aver-age of 40 minutes more per night.22
Similar to the study by Gay et al,21a
report based on home polysomnogra-phy found that breastfeeding mothers had lower sleep efficiency and more nocturnal awakenings but no total sleep time difference.23
To our knowledge, we have replicated the only other study to include subjec-tive sleep disturbance and fatigue re-ports, which also showed no
signifi-cant differences between mothers who breastfed and mothers who both breastfed and formula fed their in-fants.21The contrast between our
neg-ative subjective maternal sleep find-ings and previous studies that showed that mothers reported that their breastfed infants awakened more of-ten at night15–17are intriguing. Without
our and others’ evidence, it would
stand to reason that, if the infants awakened more often, their mothers would too. It is possible that, despite their self-reports, breastfeeding moth-ers are awakening more often during the night to feed their infants but they return to sleep more quickly or sleep during feedings and consequently do not remember those awakenings. Ob-jective actigraphy cannot be used to determine whether this is true, be-cause actigraphy is not validated for identification of discrete awakenings.
We suggest that, if breastfeeding mothers are awakening more often at FIGURE 3
night, then breastfeeding itself may have a compensatory effect. In other words, breastfeeding mothers awak-ening more often at night may return to sleep more quickly and not remem-ber these awakenings. Possible rea-sons for this may include the fact that they are not exposed to as much ambi-ent light or physical activity, compared with preparing formula. It also is pos-sible that breastfeeding mothers sleep during feedings; Quillin and Glenn33
re-ported that breastfeeding mothers who coslept slept more than did breastfeeding mothers who did not cosleep or formula-feeding mothers.
The notion that breastfeeding may have a soporific effect has some sup-port. Sánchez et al34showed that 4
nu-cleotides present in breast milk have strong maternal circadian rhythms and seem to facilitate a “hypnotic ac-tion” in infants. In addition, differences in circulating prolactin levels are sus-pected to have a primary role in sleep architecture differences among breastfeeding and formula-feeding mothers. Prolactin shows a nocturnal peak, which is vital for milk produc-tion, and usually is associated with fa-cilitation of sleep onset and␦wave ac-tivity important for restorative sleep.35
There are some limitations to our
re-sults. Because we excluded from par-ticipation women with Center for Epi-demiologic Studies Depression scale scores of⬎16 and those with a history of depression or anxiety, our results may not be generalizable to depressed or anxious women. This is important, because women who are depressed are less likely to continue breastfeed-ing.36In addition, the 15% of the
origi-nal study participants whom we were unable to contact for the breastfeed-ing interviews were younger, had less education, had lower incomes, and were less likely to breastfeed at the beginning of the study, compared with the subjects whom we were able to contact for follow-up interviews. This loss might have caused a bias in our data, with the average annual house-hold income of our participants being 23% higher than the national average for the United States in 2007.37
How-ever, our participants resided in an Ap-palachian region known for social risk, and they demonstrated a high level of demographic socioeconomic variance. Finally, although the Epworth Sleepi-ness Scale has been validated for use with several sleepy populations, it has not been validated specifically for use with postpartum women, and it has not been validated for use as a mea-sure of state, as we used it here;
rather, it has been validated and gen-erally is used as a trait measure of general recent experience.
CONCLUSIONS
To date, there is little evidence to sup-port the notion that breastfeeding has a negative impact on maternal sleep. Efforts to encourage women to breast-feed, as currently endorsed enthusias-tically by the American Academy of Pediatrics,1 should include
informa-tion about sleep. Specifically, women should be told that a choice to formula feed does not necessarily equate with improved sleep. The risks of not breastfeeding should be weighed against the cumulative lack of evi-dence showing any benefit of formula feeding on maternal sleep.
ACKNOWLEDGMENTS
Support was provided by National In-stitutes of Health grant R21 HD053836.
We thank the families who participated in the study. M. Clegg-Kraynok, S. In-sana, and L. Mancini each performed significant data collection and pro-cessing. C. Gould, A. Karpinski, S. Or-bon, J. Peterson, J. Sanchez, E. Santy, S. Schwartz, A. Smith, and M. Verzino assisted with data collection and/or processing.
REFERENCES
1. Gartner LM, Morton J, Lawrence RA, et al. Breastfeeding and the use of human milk.
Pediatrics. 2005;115(2):496 –506
2. Wu TC, Chen PH. Health consequences of nu-trition in childhood and early infancy. Pedi-atr Neonatol. 2009;50(4):135–142 3. Panchula J. Is breastfeeding compatible
with obtaining a restful night’s sleep?J Hum Lact. 2003;19(3):310 –312
4. Swain AM, O’Hara MW, Starr KR, Gorman LL. A prospective study of sleep, mood, and cognitive function in postpartum and non-postpartum women.Obstet Gynecol. 1997; 90(3):381–386
5. Gardner DL, Campbell B. Assessing postpar-tum fatigue.MCN Am J Matern Child Nurs. 1991;16(5):264 –266
6. Fisher JR, Feekery CJ, Rowe-Murray HJ. Nature, severity and correlates of psychological distress in women admitted to a private mother-baby unit.J Paediatr Child Health. 2002;38(2):140 –145 7. Armstrong KL, Van Haeringen AR, Dadds MR, Cash R. Sleep deprivation or postnatal de-pression in later infancy: separating the chicken from the egg.J Paediatr Child Health. 1998;34(3):260 –262
8. Lee KA, McEnany G, Zaffke ME. REM sleep and mood state in childbearing women: sleepy or weepy?Sleep. 2000;23(7):877– 885
9. Armstrong KL, O’Donnell H, McCallum R, Dadds M. Childhood sleep problems: asso-ciation with prenatal factors and maternal distress/depression. J Paediatr Child Health. 1998;34(3):263–266
10. Murray L, Cooper P, Hipwell A. Mental health of parents caring for infants.Arch Womens Ment Health. 2003;6(suppl 2):S71–S77 11. Paulson JF, Dauber S, Leiferman JA.
Individ-ual and combined effects of postpartum de-pression in mothers and fathers on parent-ing behavior. Pediatrics. 2006;118(2): 659 – 668
12. Righetti-Veltema M, Conne-Perréard E, Bousquet A, Manzano J. Postpartum de-pression and mother-infant relationship at 3 months old.J Affect Disord. 2002;70(3): 291–306
13. Bell AJ, Land NM, Milne S, Hassanyeh F. Long-term outcome of post-partum psychi-atric illness requiring admission.J Affect Disord. 1994;31(1):67–70
infants.Early Hum Dev. 1998;53(1):9 –18 15. Quillin SI. Infant and mother sleep patterns
during 4th postpartum week.Issues Compr Pediatr Nurs. 1997;20(2):115–123 16. DeLeon CW, Karraker KH. Intrinsic and
ex-trinsic factors associated with night waking in 9-month-old infants.Infant Behav Dev. 2007;30(4):596 – 605
17. Schwichtenberg AJM, Poehlmann J. A trans-actional model of sleep-wake regulation in infants born preterm or low birth weight.J Pediatr Psychol. 2009;34(8):837– 849 18. Butte NF, Jensen CL, Moon JK, Glaze DG,
Frost JD. Sleep organization and energy ex-penditure of breast-fed and formula-fed in-fants.Pediatr Res. 1992;32(5):514 –519 19. Thomas KA. Differential effects of
breast-and formula-feeding on preterm infants: sleep-wake patterns.J Obstet Gynecol Neo-natal Nurs. 2000;29(2):145–152
20. Tikotzky L, de Marcas G, Har-Toov J, Dollberg S, Bar-Haim Y, Sadeh A. Sleep and physical growth in infants during the first 6 months.
J Sleep Res. 2010;19(1):103–110
21. Gay CL, Lee KA, Lee SY. Sleep patterns and fatigue in new mothers and fathers.Biol Res Nurs. 2004;5(4):311–318
22. Doan T, Gardiner A, Gay CL, Lee KA. Breast-feeding increases sleep duration of new
23. Blyton DM, Sullivan CE, Edwards N. Lactation is associated with an increase in slow-wave sleep in women. J Sleep Res. 2002;11(4): 297–303
24. Radloff LS. The CES-D scale: a self-report de-pression scale for research in the general population.Appl Psychol Meas. 1977;1(3): 385– 401
25. Barrett LF, Barrett DJ. An introduction to computerized experience sampling in psy-chology. Soc Sci Comput Rev. 2001;19(2): 175–185
26. Oakley NR.Validation With Polysomnogra-phy of the Sleepwatch Sleep/Wake Scoring Algorithm Used by the Actiwatch Activity Monitoring System. Technical report to MiniMitter Co, Inc; 1997
27. Edinger JD, Means MK, Stechuchak KM, Ol-sen MK. A pilot study of inexpensive sleep assessment devices. Behav Sleep Med. 2004;2(1):41– 49
28. Benson K, Friedman L, Noda A, Wicks D, Wak-abayashi E, Yesavage J. The measurement of sleep by actigraphy: direct comparison of 2 commercially available actigraphs in a nonclinical population. Sleep. 2004;27(5): 986 –989
29. Monk TH. A visual analogue scale technique to measure global vigor and affect. Psychi-atry Res. 1989;27(1):89 –99
new approach. Psychophysiology. 1973; 10(4):431– 436
31. Johns MW. A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale.Sleep. 1991;14(6):540 –545
32. Cohen J.Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Erlbaum; 1988
33. Quillin SI, Glenn LL. Interaction between feeding method and co-sleeping on maternal-newborn sleep.J Obstet Gynecol Neonatal Nurs. 2004;33(5):580 –588 34. Sánchez CL, Cubero J, Sánchez J, Chanclón
B, Rivero M, Rodríguez AB, Barriga C. The possible role of human milk nucleotides as sleep inducers.Nutr Neurosci. 2009;12(1): 2– 8
35. Ross LE, Murray BJ, Steiner M. Sleep and perinatal mood disorders: a critical review.
J Psychiatry Neurosci. 2005;30(4):247–256 36. McLearn KT, Minkovitz CS, Strobino DM,
Marks E, Hou W. Maternal depressive symp-toms at 2 to 4 months post partum and early parenting practices.Arch Pediatr Adolesc Med. 2006;160(3):279 –284
DOI: 10.1542/peds.2010-1269 originally published online November 8, 2010;
2010;126;e1562
Pediatrics
Hawley E. Montgomery-Downs, Heather M. Clawges and Eleanor E. Santy
Infant Feeding Methods and Maternal Sleep and Daytime Functioning
Services
Updated Information &
http://pediatrics.aappublications.org/content/126/6/e1562 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/126/6/e1562#BIBL This article cites 34 articles, 2 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/breastfeeding_sub Breastfeeding
http://www.aappublications.org/cgi/collection/nutrition_sub Nutrition
milestones_sub
http://www.aappublications.org/cgi/collection/growth:development_ Growth/Development Milestones
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2010-1269 originally published online November 8, 2010;
2010;126;e1562
Pediatrics
http://pediatrics.aappublications.org/content/126/6/e1562
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.