A total of 47 patients with sleep disorder (36 male and 11
female) with a mean age of 47.5 ±15 years were evaluated for daytime symptoms with a Multiple Sleep Latency Test (MSLT) and a Maintenance of Wakefulness Test (MWT) given on the same day—once at the time of their diagnostic evaluation and again after one to six months of treatment. The MSLT and MWT data are consistent with the notion that sleep tendency, as measured by the MSLT and ability to remain awake, as measured by the MWT, represent different physiologic processes. Data show a marked treat ment-related improvement in ability to stay awake as measured by the MWT and no treatment-related improve ment in sleepiness as measured by the MSLT. We conclude that there is a heterogeneous subpopulation ofpatients with
sleep disorders whose symptoms of daytime sleepiness will show no treatment-related improvement in daytime symp toms if they are evaluated only by the MSLT. We suggest that, since ability to stay awake (and not ability to fall asleep) is a requisite for all job-related duties, an objective, physiologically based test such as the MWT should be used to assess the impact of sleep disorders in cases where there
is a clinical concern about fitness to drive or work.
(Chest 1992; 102:699-703)
MSLTMultiple Sleep Latency Test; MWTMaintenance of Wakefulness Test; REI respiratory event index; UPPP uvu lopalatopharyngoplasty
S ituated comfortably in a quiet, dark bedroom, how quickly could you fall asleep? How long could you stay awake? For years the Multiple Sleep Latency Test (MSLT) was used in clinical and research studies to quantify physiologic sleep tendency. After a night's sleep, subjects are asked to get into bed four or five times throughout the day and try to sleep. Measuring the EEG to mark the onset of sleep and hence the time it takes to fall asleep (Sleep Latency), the MSLT is the standard tool for determining pathologic sleep iness that is associated with sleep apnea, narcolepsy, chronic sleep loss, and a host of other conditions that predispose people to fall asleep. In addition to being an objective, physiologically based test, the MSLT has obvious validity: If someone is sleepy, they should fall asleep quickly, but how does sleepiness relate to alertness? Are sleepiness and alertness opposites? Or, can some sleepy people stay awake and others not? Which sleepy people should drive cars, direct aircraft landings, or operate trains? Physicians who diagnose and treat patients with sleep apnea, narcolepsy, and other disorders associated with the symptom of exces sive somnolence must frequently confront these ques tions.
*From the Sleep Disorders Institute, Troy, Mich (Dr. Sangal and Mr. Thomas), and the Scripps Clinic and Research Foundation, La Jolla, Calif(Dr. Mitler).
Primary funding and support for this project came from the Sleep Disorders Institute of Troy, Mich. Dr. Mitler is supported by Public Health Service grants, RO! NS20459 and R03 AA08235 and by Clinical Research Center grant RR00833 to Scripps Clinic and Research Foundation and by a grant from the American Narcolepsy Association.
Manuscript received August 19; revision accepted January 2, 1992.
Reprint requests: Dr. Sangal, 44199 Dequindre, Suite 311, Troy, MI 48098
The MSLT is a standard procedure used to assess and diagnose disorders of excessive somnolence . ‘¿The Maintenance of Wakefulness Test (MWT) employs a variation on the protocol used in the MSLT and was designed by Miller et al2 to assess daytime function when there are clinical questions concerning treat ment efficacy or concerning patient safety.
In a previous reports on 258 consecutive patients given the MSLT and MWT on the same day, we showed that the two tests measure different abilities. Some patients with abnormally low MSLT scores were able to stay awake when asked to do so on the MWT and, conversely, some patients who failed to stay awake when asked to do so on the MWT were unable to fall asleep quickly on the MSLT The MSLT seems to measure ease offalling asleep and the MWT seems to measure ability to stay awake.
The present study was performed to determine how the MSLT and the MWF compare in their ability to measure change in daytime sleepiness with treatment. We administered a standard four-nap MSLT and a four-trial MWT consecutively on the same day to a group ofpatients with the initial complaint of daytime sleepiness. After treatment, we administered MSLT and MWT consecutively again on the same day to measure objective change in sleepiness. We now report that only the MWT changed in the expected therapeu tic direction. The MSLT showed no treatment-related change.
METHODS
We studied a total of 47 patients (36 male and 11 female) with a mean age of47.5 ±15 years that included patients with the following diagnosis: 27 with obstructive sleep apnea, seven with narcolepsy,
CHEST I 102 I 3 I SEPTEMBER, 1992 699
Disordersof ExcessiveSleepiness*
TreatmentImprovesAbilityto Stay AwakeBut Does Not
ReduceSleepiness
Rahul B. Sangal, M.D.; Larry Thoma@ R.Psg.T; and
Cl) w
z
seven with idiopathichypersomnia,one with head trauma,four
with depression, and one with periodic leg movement during sleep. Diagnostic criteria were as described by the Association of Sleep Disorders Centers.4 All patients were free of medications that significantly affected the central nervous system for at least one week before their pretreatment testing. All patients had symptoms
of daytime sleepiness or sleep apnea. We first administered a
nocturnal polysomnogram with a monitoring montage consisting of central and occipital electroencephalogram, submental electromy ogram, and eye movement electrodes. Respiratory parameters were also studied. The next morning, they were administered a standard
diagnostic MSLT that entailed four 20-mm long opportunities to
fall asleep while lyingin bed, which were offeredat approximately
1 AM,12 noon, 2 PM,and 4 PM.Each MSLTwas followed within 20 to 60 mm by an MWF trial. For MWI@trials, patients were seated upright in bed and asked to remain awake for 40 min as described by Puceta et al.56
@ in our previous report using this protocol,@
neithersleep latencieson the MWFnorotherdiagnosticfindings
were statistically influenced by the duration ofthe interval between
the end of each MSLTnap and the startof each MWTtrial.We
also concluded from this lack of effect of the length of interval
between each MSLT and MWF trial that the order effect of an MSLTtrial preceding each MWT trialwas not a majorfactor in cor
results. Each MWF test was terminated as soon as the patient was
clearly asleep. Sleep onset was defined as three continucos epochs
ofstage 1 sleep or any epoch ofstage 2 to 4 or rapid eye movement (REM) sleep. Sleep latency was then calculated from the beginning
ofeach test to the first epoch ofsleep. The lights were then turned on, and patients were awakened and instructed to stay awake until
the next sleep latency test. If no sleep occurred,the test was
terminated after 40 mm. Four tests were administered during the
day, one after each sleep latency nap. Scoring of both MSLT and
MWF trials was done in the standard way for the MSLT.― The initial test results for these patients were included in our earlier report on 258 consecutive patients given both the MSLT and the
MWt3
Patients were then treated based on the final diagnosis: 15 were treated with nasal continuous positive airway pressure (CPAP); 11, with uvulopalatopharyngoplasty (UPPP) or jaw advancement sur
gery; 16, with other therapy including pemoline or methylpheni
date; four, with tricyclic antidepressant; and one patient with periodic leg movement during sleep was treated with alprazolam.
One to six months after treatment, a polysomnogramwas repeated followed by MSLT and MWF as described earlier.
Since we were dealing with truncated, and possibly nonnormal
distributions for both MSLT and MWF data, we evaluated treat
ment-related changes in MWT and MSLT sleep latencies with a
nonparametric test, the Mann-Whitney U test, as well as the
Student's t test for correlated means (matched pairs t test). In this
particular application, we expected the Mann-Whitney U test to produce lower levels ofsignificance than the t test. However, since
we are comparingthe relativesensitivitiesof the MSLTand the
MWF, we have reported results for both statistical tests throughout
the present article.
RESULTS
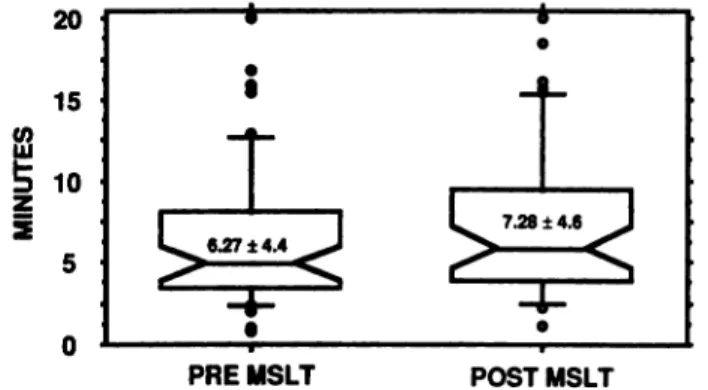
Figure 1 shows box plots that summarize the
distributions for the MSLT tests administered before and after treatment. Box plots are useful ways to present truncated data sets such as those resulting when individual scores frequently reach a protocol
dependent maximum such as 20 min for the MSLT
and 40 mm for the MWT Each box encompasses the middle 50 percent ofthe distribution and the horizon tal line within the box represents the median. The
20
15
10
5
0
Ficuns 1. Box plots of the distributions for the MSLT tests
administered before and after treatment. Each box encompasses
the middle 50 percent of the distribution and the horizontal line
within the box represents the median. The notches about the horizontal line denote the 95 percent confidence band about the
median. The vertical lines above and below denote the extent of
the middle 80 percent ofthe distribution. Outliers above and below
the middle 80 percent are denoted by individual dots. The
mean ±standard deviation for each condition is printed within the box.
Ficuna 2. Box plots of the distributions for the MWT tests administered before and after treatment. The mean ±standard
deviation for each condition Is printed within the box. See Figure
1 for a description ofbox plot presentations.
notches about the horizontal line denote the 95 percent
confidence band about the median. The vertical lines
above and below denote the extent of the middle 80
percent of the distribution. Outliers above and below
the middle 80 percent are denoted by individual dots. The pretreatment average MSLT sleep latency was 6.27 and the median MSLT sleep latency was 4.89 and a large proportion of these patients had average MSLT sleep latencies between 5 and 10 min. In our experience, the distribution of MSLT scores that we obtained is typical ofpatients who present to the sleep disorders center with a clinical history that necessi tates daytime testing for disorder of excessive somno lence. Using the most recent classification of sleep disorders,7 the degree ofsomnolence ofthe central 50
percent of the present series qualifies as moderate to
severe. Statistical tests for differences between pre treatment and posttreatment were done. The Mann
Whitney U test (z= —¿1.183;p=ns) did not detect a
treatment-related change. A matched pairs t test on the pretreatment vs posttreatment means (6.33 ±4.3 vs 7.28 ±4.6) was also nonsignificant.
40
35 30 Cl) 25@20
@ 15 10 5 0700 Dèeordere01ExcessIve S1eeç@ness(Sange@Thomas@Miser)
PRE MSLT POSTMSLT
MWFNoYesTotalsMSLTNo
Yes6 49 715
11Totals101626
Figure 2 summarizes in box plot format the results for the MWT tests administered before and after treatment.
The Mann-Whitney U test (z = —¿2.21; p<O.03) indicated a statistically significant treatment-related change. A matched pairs t test on the pretreatment vs
posttreatment means (23.4 ±14.0 vs 30.00 ±12.0) was
also significant (p<0.001).
A detailed analysis was done on a relatively homo
geneous subgroup of 26 patients (mean age, 54.6±10
years; 24 male and 2 female) who had the diagnosis of obstructive sleep apnea and who were treated with nasal CPAP and/or UPPP and no central nervous system (CNS) active medications. Their average pre
treatment respiratory event index (REI) was
49.58 ±26.9 and their posttreatment REI was
23.39 ±30.4. We consider the degree of sleep apnea in this subsample to range from moderate to severe and the amount ofposttreatment improvement in REI to be typical, although not at all ideal, for apneics
aftertheirfirsttreatmenttrial.Theoveralltreatment
related reduction in REI was statistically significant (t = 5.20; p<O.000l), but considerable apnea remained in the subsample at the time of posttreatment evalu ation.
The pretreatment and posttreatment results for the mean sleep latency on the MSLT and the MWT are summarized in Figure 3.
Note the obvious trend for steeper slopes in the
MWF data. Note also that there were discordancies
in pretreatment MSLT and MWT sleep latencies. A number of patients at the pretreatment stage were in the bottom half of the range in MSLT sleep latencies and the top half of the range in MW'!' sleep latencies.
Table 1—TheNumber of26 Sleep Apneics Who Showed Improvement on the MSLT and the MWT after Treatment
Conversely, a few patients at the pretreatment stage were in the top half of the range in MSLT sleep latencies and the bottom half of the range in MWT sleep latencies. Such MSLT-MWT discordancies have been described and discussed elsewhere.3 In these 26 patients, as with the 47 subject parent group, the Mann-Whitney U test did not detect a treatment related change in the MSLT (z —¿. 156; p ns). The
pretreatment vs posttreatment MSLT means
(7.00 ±5.2 vs 6.29 ±4.2) changed in the wrong direc tion, but the Student's t test was nonsignificant.
However, the Mann-Whitney U test disclosed a large
treatment-related change in the MWT (z = —¿1.93; p<O.05). The pretreatment vs posttreatment MWT means (24.29± 14.3 vs 32.01 ±11.7) also changed significantly (p<0.007).
A frequency of improvement analysis, based on whether there was any posttreatment increase in sleep latency for either the MSLT or the MWT, is summa
rizedinTable1.
As can be seen in Table 1, 11 showed improvement in the mean MSLT, whereas 16 showed improvement in the MWT The x2 did not reach statistical significance, however.
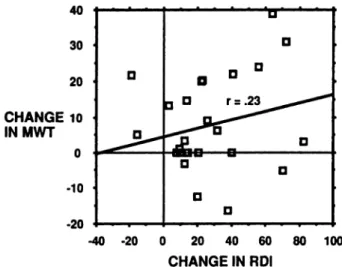
There was a weak, but apparent, trend (r .23,
20 40 18 36 16 32 14 28 12 24 10 20 8 16 6 12 4 8 2 4 0 0
FIGURE 3. Line plots of the mean sleep latencies on the MSLT and the MWT for 26 patients before and after treatment for sleep apnea.
0U
D
3 aD
0
0
26 sleep apneic subjects remained below an MW'!' sleep latency ofl5 mm—the level suggested by Poceta
et al6 as a criterion for restricting driving privileges.
We do not believe that the greater sensitivity and selectivity of the MW!' vs the MSLT is an artifact of our protocol. In an earlier article,3 we showed that
the combined MWT and MSLT protocol produced
internally consistent results for both the MWF and the MSLT The individual MWT trials correlated about 0.6 with one another. Also, the individual MSLT trials correlated about 0.6 with one another. Furthermore, there was no trend for MW!' trials late in the day to be longer in association with sleep accumulated on MSLT trials. The most likely explanation for the discrepancy in the present data and previous work is that Zorick et al―studied 12 patients with severe
obstructive sleep apnea (pretreatment mean
RE! = 55. 1 ±28.4, posttreatment RE! = 6.0 ±6. 1) and Wittig et al@studied ten patients with severe obstruc
tive sleep apnea (pretreatment mean
RE! = 79.0 ±26.5, posttreatment REI = 8.2 ±10.0). By contrast, the 26 apneics in our present series had somewhat less severe sleep apnea (pretreatment RE! = 49.68 ±26.9) and were less completely treated at the time of our second evaluation (posttreatment RE! = 23.39 ±30.4). Moreover, some of our sleep ap neic subjects were treated with surgery, rather than nasal CPAP Those patients who received surgical treatment had less improvement in RE! and less improvement in MWF sleep latencies. Thus, it may be that less than maximal reduction in the number of sleep apnea episodes accorded via surgery reduced the likelihood ofthe MSLT detecting treatment related change in sleep tendency. Such an explanation is consistent with the findings of Zonck et al―of less dramatic improvement in sleep apneics after UPPP than after nasal CPAP and with the data of Caddy and Doghramji.'°
Thus, the present data, when viewed in perspective ofprevious work,&hlsuggest that the MSLT can detect large treatment-related changes in sleep tendency
provided the pretreatment and posttreatment meas
urements are done at points representing very differ ent seventies of disease. The MW'!', on the other hand, seems to be more sensitive to treatment-related changes. As we have described elsewhere,3 it is unlikely that the MW'!' is simply a more powerful tool to measure the same ability that the MSLT measures. It is more likely that the MWF and the MSLT measure different abilities (eg, alertness and sleepiness, respec tively). If this is so, then a sleep disorder giving rise to the symptom of daytime sleepiness may actually impair both alertness and sleepiness. Also, treatment of such disorders brings about a greater change in alertness than in sleepiness. More generally, we sug gest that sleepiness (or lack ofalertness) is a complaint 40 30 20 CHANGE 10
INMWT
0 -10 -20 -40 -20 0 20 40 60 80 100 CHANGE INRDIFIGURE 4. Scatter plot of the pretreatment and posttreatment
change in mean RE! vs change in mean MWT sleep latency.
p = ns) toward greater improvement in REI and greater change in MWT sleep latency as is summarized in Figure 4.
We examined this weak REI-MWT relationship
separately for the 15 patients treated with CPAP and the 11 patients treated with surgery. The patients with CPAP had a significant improvement in RE! (44.88 to 7.38; p<O.001); the patients who had surgery did not have a significant improvement in RE! (56.02 to 45.00; p = ns). For MWT sleep latency, the patients with CPAP also had a significant improvement (23.89 to 31 .64; p<O.O5); the improvement for patients who had surgery was less pronounced and only approached statistical significance (25.05 to 32.37; p<O.09).
DISCUSSION
Our data clearly indicate that for a heterogeneous sample of patients with the clinical question of exces sive daytime sleepiness and for a homogeneous sub sample of patients with obstructive sleep apnea, the
MWTissensitivetochangesinabilityto remainawake
that result from therapeutic maneuvers. The MSLT,
however, did not change with therapy. The treatment
related changes in MW'!' sleep latencies are compa rable in magnitude to those observed by Poceta et al6 in 322 patients with sleep apnea treated with nasal CPAP However, our treatment-related changes in MSLT sleep latencies are not in agreement with the CPAP results of Sangal and Thomas8 or with Wittig et al.9 Not all investigators, however, have found normal ization of MSLT sleep latencies after effective treat ment ofsleep apnea. Caddy and Doghramji'°reported
63 apneic subjects before and after treatment with
CPAP The RDI in this study went from 59.3 to 10.2, but the mean MSLT sleep latency only went from 6.9 to 9.0. Some 60 percent of the treated patients of
Caddy and Doghramji remained sleepy by MSLT
criteria. By contrast, after treatment, only four of our
that probably has many components. These compo nents include but are not limited to the following: (1) ability to fall asleep rapidly as measured by MSLT; (2) inability to stay awake as measured by MW'!'; (3) reduced attention as measured by cognitive (long latency) evoked potentials;1213 and (4) fatigue that may be a separate component or a complex composite of the other components. A patient complaining of sleep mess may have abnormal test results reflecting some or all ofthese components. We have shown previously that patients may fall asleep rapidly on the MSLT and be able to stay awake on the MW1@or they may fall asleep on the MWT but not on the MSLT We are planning further studies to compare the MSLT with
cognitive (long-latency) evoked potentials. Evaluating
a patient with a complaint of sleepiness or lack of alertness may ultimately require a battery of tests, not
just an MSLT measuring only one component of
sleepiness. To state that a patient has no objective
findings based on only the MSLT may be a disservice
to the patient.
Whether our line of thinking ultimately proves to be correct, the present MSLT and MW'!' data are consistent with the notion that sleep tendency, as measured by the MSLT and ability to remain awake, as measured by the MWT, subtend different physio logic processes. At the very least, these findings indicate that there is a heterogeneous subpopulation ofpatients with sleep disorders with the symptoms of
daytime sleepiness who will show no treatment-related
improvement in daytime symptoms if they are evalu
ated only by the MSLT We suggest that, since ability to stay awake (and not ability to fall asleep) is required for all job-related duties, an objective, physiologically based test such as the MW'F should be used to assess the impact of sleep disorders on clinical questions concerning fitness to drive or work. Poceta et al5 have
suggested that clinicians might recommend that pa
tients with a MWT mean of less than 15 mm do not drive or, presumably, engage in other activity where sustained attention is required for safety. The 15-mm level was approximately 1 SD below the mean for their series of 322 sleep apneic patients. Nothing in our data would argue against the use of a 15-mm cutoff. About 30 percent ofour 48 patients were below the 15-mm level on their pretreatment MWF and less
than 15 percent were below the 15 mm level on their posttreatment MWT Clearly, however, the clinician should follow all applicable local laws, standards of practice, and institutional policies when deliberating these issues.
ACKNOWLEDGMENT: BarbaraBigby assisted with manuscript preparation.
REFERENCES
1 Carskadon MA, Dement WC, Mitler MM, Roth R, Westbrook PR, Keenan S. Guidelines for the multiple sleep latency test (MSLT): a standard measure of sleepiness. Sleep 1986; 9:519-24
2 Mitler MM, Gujavarty KS, Browman CE Maintenance of
wakefulness test: a polysomnographic technique for evaluating
treatment in patients with excessive somnolence. Electroen cephalogr Clin Neurophysiol 1982; 53:658-61
3 Sangal RB, Thomas L, Mitler MM. The maintenance of wakefulness test (MW'F) and the multiple sleep latency test (MSLT)measure different abilities in patients with sleep disor ders. Chest 1992; 101:898-902
4 Association of Sleep Disorders Centers. Diagnostic classification of sleep and arousal disorders. 1st ed Prepared by the Sleep Disorders Classification Committee, HP Roffwarg, Chairman. Sleep 1979; 2:1-137
5 Poceta JS, Ho S. Jeong D, Mitler MM. The maintenance of
wakefulness test in obstructive sleep apnea syndrome. Sleep
Res 1990; 19:268
6 Poceta JS, limms RM, Jeong D, Ho S. Erman MK, Mitler MM. The maintenance of wakefulness test in obstructive sleep apnea syndrome. Chest 1992; 101:893-97
7 Diagnostic Classification Steering Committee. Thorpy MJ,
Chairman, International classification of sleep disorders: ding nostic and coding manual. Rochester, Minn: American Sleep Disorders Association, 1990
8 Sangal RB, Thomas L. Obstructive sleep apnea: improvement in somnolence with continuous positive airway pressure. Sleep Res 1991; 20:319
9 Wittig R, Zorick F, Conway W, Ward J, Roth T Normalization ofthe MSLT after six weeks ofCPAP for sleep apnea syndrome. Sleep Res 1986; 15:185
10 Gaddy JR. Doghramji K. Daytime sleepiness after nCPAP treatment. Sleep Res 1991; 20:245
11 Zorick FJ, Roehrs T, Conway W, Potts G, Roth T. Response to CPAP and UPPP in apnea. Henry Ford Hosp Med J 1990; 38: 223-26
12 Walsleben JA, Squires NK, Rothenberger VL. Auditory event related potentials and brain dysfunction in sleep apnea. Electroencephalogr Clin Neurophysiol 1989; 74:297-311 13 Broughton R, Aguirre M, Dunham W. A comparison of multiple
and single sleep latency and cerebral evoked potential (P300)
measure in the assessment of excessive daytime sleepiness in narc()lepsy-cataplexy. Sleep 1988; 11:537-45