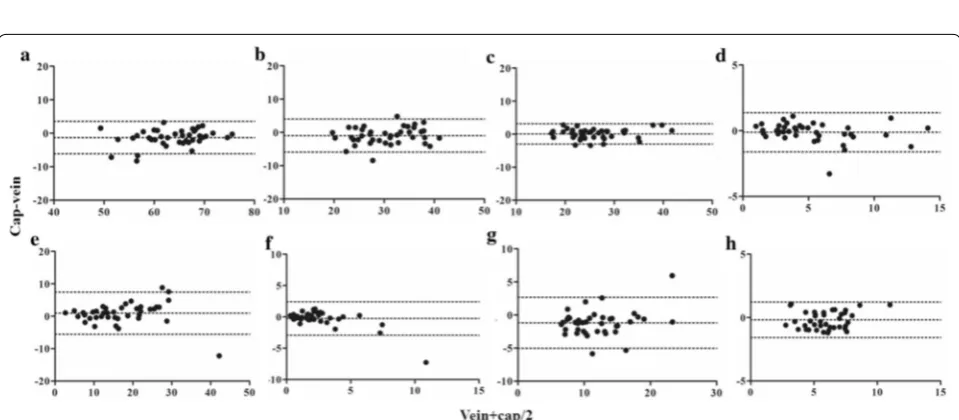
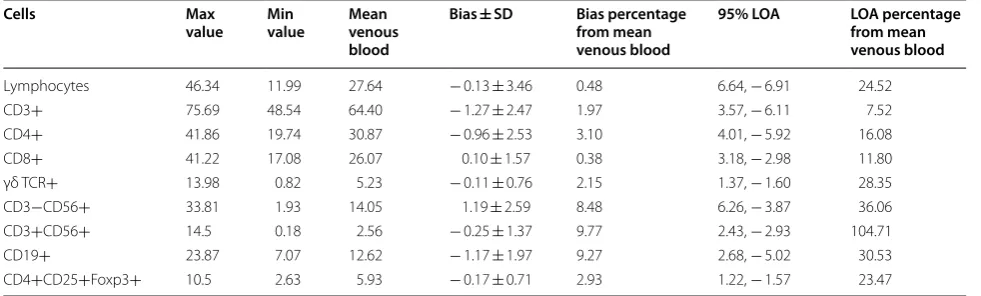
Capillary blood as an alternative specimen for enumeration of percentages of lymphocyte subsets
Full text
Figure
Related documents
Colletogloeum (1953) has hitherto been a somewhat confused genus, including many species that appear to belong to Teratosphaeria. However, the ITS sequence from
By employing PBG structures, the second antenna presented 5.5 dB, 0.3 dB and 4 dB lower cross-polarization level in the E -plane of three resonant-bands respectively, and 3 dB
Moreover, a combination of the PMT delay and the channel cable delay are also measured by calibration runs with PMT built-in calibration LEDs, which provides a cross check of the
High temperature water (HTW) (pressurised aque- ous reactions at > 100°C) has been found to be an effective solvent for Heck coupling reactions of aro- matic halides with
One critic of the FCC's actions toward cable contended that "[t]here is considerable evidence that the Commission has been more concerned with protecting the
1) tentative discourse patterns similar to the English ones are used in Georgian and Russian by some native speakers in certain situations, but their frequency is negligible
In this note, using only elementary techniques, we demonstrate that the sequence S n is strictly increasing and that 1.1a holds; in addition, we establish a sharp estimate of
There are differences in the ways in which grounded theory researchers approach the coding process. For most grounded theorists, initial open coding involves the generation of
