280524173X
DOES CEREBRAL MALARIA CONSTITUTE A RISK FACTOR FOR SPECIAL EDUCATIONAL NEEDS?
Penny Anne Holding
Thesis submitted for the Degree of Doctor of Philosophy
1997
ProQuest Number: 10014389
All rights reserved
INFORMATION TO ALL USERS
The quality of this reproduction is dependent upon the quality of the copy submitted.
In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if material had to be removed,
a note will indicate the deletion.
uest.
ProQuest 10014389
Published by ProQuest LLC(2016). Copyright of the Dissertation is held by the Author.
All rights reserved.
This work is protected against unauthorized copying under Title 17, United States Code. Microform Edition © ProQuest LLC.
ProQuest LLC
789 East Eisenhower Parkway P.O. Box 1346
ABSTRACT
In a malarial endemic area it is pre-school children who are at most risk of developing cerebral malaria. This study was designed to increase the understanding of the expected outcome for survivors through investigating both
cognitive and behavioural aspects of development.
A broad assessment battery was developed, taking into account both potential neurological impairments, and the particular social and cultural background of the children being assessed. Tasks, adapted from the Kaufman Assessment Battery for Children, and measuring information processing skills formed the core. The battery also included measures of attention, visuo-motor speed, language, and behaviour. Modifications were made to all the tests used, following assessment of the reliability and validity of the tools within the study population.
A matched pairs design was applied, each "case" being matched on age; sex; and measures of socio-economic and nutritional status. The 87 pairs were assessed at 6 years old, (approximately 50 months post discharge). An investigation was made of the symptoms of the acute stage of the disease, to determine if there were any distinctive characteristics associated with poor outcome.
Results on the information processing battery showed no impairments in performance for the majority of children, although a significantly greater number of cases had an impaired performance. This sub-group were identified as in need
of specialist educational facilities. A combination of coma; hypoglycaemia; and fits provided the best-fit predictive model for membership of the impaired sub group.
cases and controls. This combination of deficits is suggestive of an immaturity in the development of survivors, which, if it should continue, may place these children at risk of educational difficulties at higher levels of schooling, when tasks
ACKNOWLEDGEMENTS
It would not have been possible to plan, execute, nor complete this study without
the support and advice which has been so freely offered to me, and for which I am extremely grateful. My most particular thanks g o t o :
• The assessment team: Sidi, Khamis, Thadeus, Joseph, Leonard, Bernard and Mzee Magongo.
• My other colleagues at KEMRI-Wellcome, Kilifi for their technical assistance, advice, and patience. Most especially the inspirational guidance of Kevin Marsh.
• Psychologists and child development specialists around the world who have responded to my queries with useful suggestions and guidance. Not least of which has been Alan Kaufman, for his support of my use of his assessment battery; Michael Boivin, who provided a great deal of information on his African studies; and Jane Kvalsvig, who shared insight into the contextual details of research in Africa.
• The Behavioural Sciences Unit at ICH for providing me a home.
• My family, both close and extended, for their continued support throughout the ups and downs of this research.
• Jim Stevenson, whose insightful and stimulating supervision has made it all
possible.
CONTENTS
Page
SECTION 1 : INTRODUCTION. BACKGROUND AND THEORETICAL FRAMEWORK
A: Introduction 26
Chapter 1 : The Elements of the Study 27
Chapter 2: Malaria: the disease and the implications 29 for cognitive development
The relationship of transmission to morbidity 31
Cerebral Malaria 33
C.M.: The impact on survivors 34
C.M.: The impact on the community 34
C.M.: A continuum of deficits? 35
C.M.: Measuring the nature and extent 33
of impairment
B: Cognitive Development And Cognitive Impairment: 38 The Theoretical Framework
Chapter 3: Cognitive Development - A Vygotskian Framework 39
Stages of Development 39
Functional Systems 40
Agents of Change 41
The Socio-Historical Context Of Learning 42
The Process of Development 43
Thought and Speech 46
The Development of Concepts 47
The Specific Influence Of Literacy 49
And Schooling
Page The socio-cultural influence on impairment 49
Capacity and Performance 51
Vygotsky and malaria 52
Summary and Implications 52
Chapter 4: Luria's Neural Base to Cognitive Functioning 54
The Roots of Development 54
Equipotentiality versus Localisation 55
Assessment and Syndrome Analysis 56
Syndrome analysis: a case study 57
Models of Functional Systems, and Models of Development 57
The Two Forms of Synthesis or Processing 58
The Three Principal Functional Units Of The Brain 59 The hierarchical structure of functional units 60
The laws governing cortical maturation 61
Normal and Abnormal Development 62
Dynamic Development 63
Summary and Implications 64
Chapter 5: The Information Integration Model 66
The Coding Component 66
Simultaneous Processing 68
Successive Processing 69
Examples of Assessment Materials 69
Determinants of the selection of processing strategy 69
age/developmental stage 70
the influence of the socio-cultural environment 71
Information processing, achievement and schooling 72 Application versus slection of processing strategies 72
The Attention Component 73
The Planning Component 73
Page
Validity of the Model 74
Application Of The Model To The Understanding Of Impaired Performance 77
Summary and Implications 78
C: The Relationship Between Cognitive Function And Disease 80
Chapter 6: Cerebral Malaria: The Potential Mechanisms 81
Cerebral Insults 81
Coma 81
Fits/Seizures 82
Hyperpyrexia 85
Hypoglycaemia 85
The Evidence Of Other Encephalopathies 86
Reye's Syndrome 87
Meningitis 88
General Health and Development 92
Other parasitic infections 92
Nutrition 95
Malnutrition 95
Anaemia/iron deficiency 96
Other nutritional deficiencies 98
Summary 98
Chapter 7: Predicting Impairment and Recovery 100
Predicting Impairment 101
The site of the lesion and the localisation of brain function 101 The age of onset: early plasticity versus early vulnerability 103
Gender 105
Stages of Development - A theoretical model for the prediction of 105 impairment
Influences Upon Recovery 108
Page
A threshold of damage 109
Vulnerability of functions 109
Socio-economic status 111
Other environmental influences 114
The Threshold Hypothesis 116
Summary ' 119
Chapter 8: A Summary of the Implications for 120
the Study of Cerebral Malaria
Cerebral Insults 120
Coma 121
Fits/Seizures 121
Hypoglycaemia 122
Hyperpyrexia 123
Malnutrition 123
Anaemia 124
Other Parasitic Infections 125
Socio-Economic Status 125
Summary and Development of Hypotheses 126
SECTION 2: THE METHODOLOGY AND ITS DEVELOPMENT 129
Chapter 9: Assessment in Context: culture, cognition and assessment 130
Standardised Tests: strengths and weaknesses 130
The Issue of Test Bias 132
Culture Free Assessments 135
“The Developmental Niche” 138
The physical and social setting in which the child lives 138
Dynamic Assessment 141
The physical and social setting in which the child lives (cont.) 144
Page
Specific linguistic environment 148
Customs of child care 149
The psychology of the caretaker 151
Test Format and Test Procedure: accounting for culture 153
Chapter 10: Familiarisation , 155
The Observation and Sampling of Behaviours and Activities 155 Assessing Different Materials and Presentations 156
Assessing an Appropriate Level of Difficulty 156
Chapter 11 : The Main Pilot Study 157
The Assessment Team 157
Content of the Assessment Battery 157
Procedure 158
Subjects 159
Results 159
Description of the subject group 159
Family Background Interview 160
Chapter 12: Information Processing- The K-ABC and the Kilifi Battery 162
Description of the Battery of Sub-Tests 163
Simultaneous Scale 163
Magic Window 163
Face Recognition 164
Gestalt Closure 164
Matrix Analogies 164
Triangles/Construction 164
Sequential Processing Scale 165
Hand Movements 165
Number Recall 165
Word Order 165
Page
Arithmetic 166
Pilot Study of Kilifi Simultaneous-Sequential Sub-tests 166
Procedure 166
Results 167
Practice Effects 171
Goals of the K-ABC ' 171
The Theoretical And Research Basis And The Definition Of Intelligence 172
Studies of construct validity 174
Evidence from the interpretive manual 174
The verbal component 175
The attention component 179
Developmental differences in factor structure 180
Cross-cultural validation 181
The Laotian Study 182
The Zairian Study 183
Educational Implications 184
Predictive Validity 184
Appropriate Redemption: Aptitude-Treatment-lnteraction 185
Dealing with Novelty 187
Sensitivity to Different Groups of Children 188
Issues of Design 188
Summary and Conclusions 189
A more complete test battery 191
Chapter 13: Achievement 192
Arithmetic 192
Rhyming and Alliteration 193
Chapter 14: Attention 196
Page
Intervention and Remediation 202
The Evidence of Specific Disorders of Attention 203
Attention deficit disorders 203
Acquired brain disorders 205
Epilepsy and seizure activity 206
Meningitis ' 207
Traumatic brain injury 207
The Selection of An Attention Task 208
Task Description and Development 209
Chapter 15: Planning/Adaptive Intelligence 211
Problem Solving 212
Chapter 16: Relative Hand Skill and Developmental Disorders 214 The Development of Handedness , the Normal and the Pathological 214
The Right Shift Theory of Handedness 215
Is Left-Handedness Pathological 216
Relative Hand Skill and Cognitive Impairment 217
Speed and Cognitive Impairment 218
Task Description and Development 218
Pilot study pegboard 218
Main study pegboard 219
Chapter 17: Speech and Language Development 220
Development of the Language Assessment 225
Stage 1 : Pre-pilot study 225
Stage 2: Pilot study 225
Stage 3: Final procedure 226
Language Comprehension 226
Expressive Language 228
The expressive language checklist 230
Page
Discourse Analysis and Pragmatic Errors 231
The measurement of pragmatic errors in the current context 234
Assessing the semantic level 236
Assessing the syntactic level 237
Assessing the phonological level 238
Summary " 239
Chapter 18: Behaviour 241
Introduction 241
Why is the Investigation of Behaviour Important ? 243
Persistence of Behaviour Problems 246
Risk Factors Associated with Onset and Persistence 246
Approaches to the Analysis of Behaviour 248
How Context Specific are Behaviour Measures? 249
What Constitutes a Behavioural Problem? Issues of culture and age 251
Prevalence of Behavioural Disorders 252
Sex Differences 253
Sampling Techniques: Which method to use? 254
Development of the Kilifi Behavioural Assessment 257
The Behaviour Questionnaire for Parents 257
Initial pilot work 257
Procedure 257
Main pilot study results 259
Behavioural observations 260
Main pilot study results 261
Chapter 19 Health Screening 263
Current Nutritional Status 263
Development of the procedure 263
Hearing 264
Otoscopic screening 264
Page
Pure tone audiometry 264
Vision 264
Inspection 265
Screening for visual acuity 265
Screening for visual field 265
SECTION 3: DEVELOPMENTAL SEQUELAE OF MALARIA: THE MAIN
STUDY 266
Chapter 20: Main Study: Outline And Procedures 267
The Assessment Team 267
Subjects and Matching 267
Inclusion Criteria 268
Exclusion Criteria 268
Sample Size 269
Matching 269
Content 270
Procedure 271
Health screening 271
Assessment sessions 272
Analysis of Results 273
Chapter 21 : Background Details: Comparing CASES and CONTROLS 274
Sample Size for Analysis 274
Part 1 : Matching 274
Combined level of matching 274
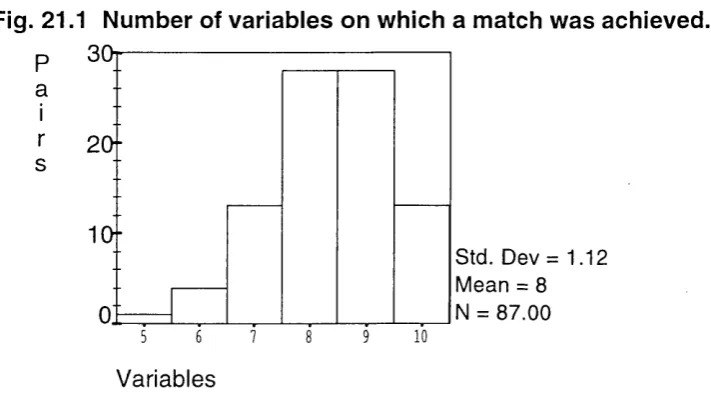
Verification of matching 276
Summary 281
Part 2: Background Details at the Time of Follow Up 281
Socio-economic measures 281
Family composition and schooling 282
Page
Employment and income source 284
Developmental history 287
Health status, past and present 288
Summary 292
Chapter 22: Health Screening Assessment 293
Nutritional status 293
Hearing 293
Sight 294
Chapter 23: Investigations of Procedure and Methodology 296 Factor Structure of the Kilifi Assessment Battery 296
Nutritional Status and Performance 299
Test Performance and Environmental Indicators 301
School experience 301
Gender differences 302
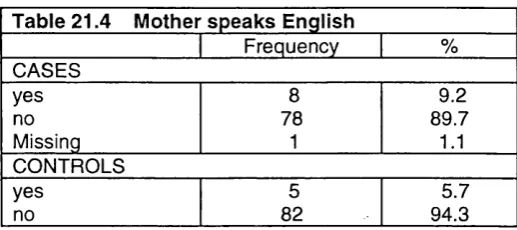
Mother can speak English 304
Family school index 305
Others : a summary table 306
Assessor Effect Upon Test Performance 306
Behavioural Measures 308
Chapter 24: Description of the Performance on 311
the Assessment Battery
Information Processing 311
Achievement 312
Attention/Planning 312
Visuo-Motor Speed 313
Language 313
Behaviour 314
Test taking behaviour 314
Parental report of behaviour in the home 314
Page
Summary 315
Chapter 25: Differences in Performance 316
Information Processing 316
Achievement 318
Attention/Planning - 318
Visuo-Motor Speed 318
Language 318
Behaviour 320
Observation of test taking behaviour 320
Parental report of behaviour in the home 320
Summary 321
Chapter 26: Comparison Of The Pattern Of Performance 322 Between Cases and Controls
Impaired Performance, and the Comparison of “Outliers”. 322
Information processing 328
Handedness 329
Attention/Planning 329
Language 330
Behaviour 332
Gender 334
Summary 334
Chapter 27: The Composition of the Impaired Case Group 336
The Performance Profile 336
Looking at possible gender effects 338
Predicting Group Membership from Clinical Variables 339 Predicting Group Membership from Neurological Impairment on Discharge 341 Protection and Risk : Socio-Environmentai and General Health Factors 342
Matching variables 342
Page
Summary of Results 344
Chapter 28: Discussion 347
Introduction 347
A: Describing the Pattern of Impairments Found 347
Summary of results 347
Behaviour 350
Parental rating 350
Gender 351
Test session behaviour 352
Language 354
Attention/Planning 356
Concluding the Evidence on Group Differences 358
B: Predicting Outcome from the Severity of the Damage 361
Neurological Impairment on Discharge 362
Other Clinical Variables as Predictors 363
Coma 363
Hypoglycaemia 364
Seizures 365
Hyperpyrexia 366
Parasitisation/summary on other clinical variables 367 The Association Between Clinical Variables and Cognitive 367 Impairment : The best fit predictive model
Factors Affecting Vulnerability and Protection 369
Pre-insult history 369
Nutritional status 370
Conclusion to pre-insult investigations 371
Age of onset 372
Gender 373
Post insult factors influencing outcome 374
Page
Family size 374
School attendance 374
Income and social environmental measures 376
General health 377
Sensory impairment 378
Conclusion to post-insult investigations 378
General Summary of Case Group Analysis 379
0: Methodological Issues 380
Construct validity 380
Simultaneous/Sequential 380
Planning/Attention 381
Achievement 382
The third factor 382
Test of speed 382
Language 383
Behaviour 383
Predictive validity 384
Gender 385
An evaluative summary 386
Summary and Conclusion on the Kilifi Assessment Battery 387
Chapter 29: Summary, Conclusions And Implications For Future 389 Research
Future Research 391
References 393
APPENDICES
Appendix 1
Appendix 2
Appendix 3
Appendix 4
Appendix 5
Appendix 6
Appendix 7
Appendix 8
Appendix 9
Description of Pragmatic Errors
Expressive Language Checklist
Parent Questionnaire
Key to Behavioural Observation
Box Plots of Raw Scores
Bar Charts of Raw Scores, showing outliers
Distribution of Performance Llevels, standard deviation groups
Blantyre Coma Scales
Examples of Assessment Materials Record Booklet
Gestalt Closure drawings
Verbal Comprehension drawings Construction- drawings
Visual Search sheets (word order stimuli) Instruction Sheets
Page
430
432
435
438
441
443
445
448
449
TABLES AND FIGURES
Page
Figure 1.1 The parasite in the human host 29
Figure 1.2 Malaria, the progression to death 31
Table 5.1 Results of confirmatory factor analysis on PASS model 75
Figure 7.1 Categories of impairment 100
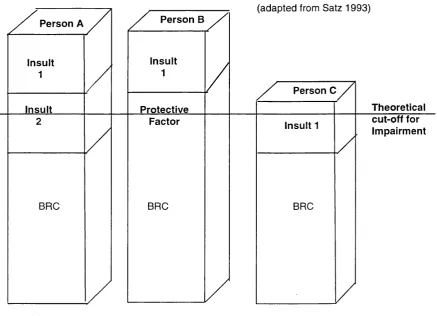
Figure 7.2 Brain reserve capacities and the threshold hypothesis 117 Figure 8.1 Hypothetical distribution of performance 126
Table 12.1 Pilot study results: Magic Window 167
Table 12.2 Pilot study results: Face Recognition a 167 Table 12.3 Pilot study results: Face Recognition b 168
Table 12.4 Pilot study results: Gestalt Closure 168
Table 12.5 Pilot study results: Matrix Analogies a 168 Table 12.6 Pilot study results: Matrix Analogies b 169
Table 12.7 Pilot study results: Construction a 169
Table 12.8 Pilot study results: Construction b 169
Table 12.9 Pilot study results: Hand Movements a 170 Table 12.10 Pilot study results: Hand Movements b 170
Table 12.11 Pilot study results: Number Recall 170
Table 12.12 Pilot study results: Word Order simple 171 Table 12.13 Pilot study results: Word Order interference 171
Table 12.14 Construct validity : K-ABC 174
Table 12.15 Construct validity :Kilifi Battery 175
Table 12.16 Construct validity :The verbal component 177 Table 12.17 Inter-correlations- K-ABC vs. WISC-R 178 Table 12.18 Construct validity :The attention component 180
Table 12.19 Construct validity : Laotian Study 183
Table 12.20 Construct validity : Zairian Study 184
Table 13.1 Pilot study results: Arithmetic 193
Table 13.2 Pilot study results: Rhyming 194
Table 13.3b Pilot study results: Alliteration b
Table 14.1 Pilot study results: Attention Table 16.1 Pilot study results: Pegboard one Table 16.2 Pilot study results: Pegboard two
Table 17.1 Pilot study results: Verbal Comprehension Table 17.2 Pilot study results: Syntax
Table 17.3 Pilot study results: Articulation
Figure 18.1 Quay’s categories of behaviour disorders Table 18.1 Test Session Observation Schedule results Figure 21.1 Level of matching
Figure 21.3 Age at admission: Cases Figure 21.4 Age at admission: Controls Figure 21.5 Time since admission: Cases Figure 21.4 Time since admission: Controls Table 21.1 Age at time of assessment Table 21.2 Matching variables: malnutrition Table 21.3 Matching Variables: malnutrition Table 21.4 Matching variables: mother’s English Table 21.5 Matching variables: mother’s English
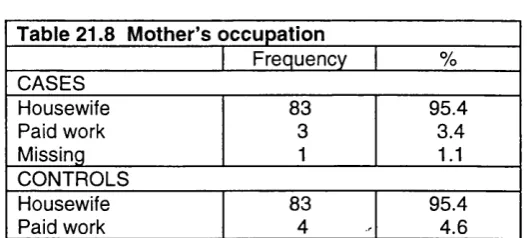
Table 21.6 Matching variables: mean corpuscular volume Table 21.7 Matching variables: mean corpuscular volume Table 21.8 Matching variables: mother’s occupation Table 21.9 Matching variables: mother’s occupation Table 21.10 Matching variables: mother’s schooling
Table 21.11 Matching variables: mother’s schooling Table 21.12 Matching variables: hookworm density Table 21.13 Matching variables: hookworm density
Table 21.14 Matching variables: mid-upper arm circumference
Table 21.15 Matching variables: mid-upper arm circumference Table 21.16 Family composition and schooling
Figure 21.6 Level of School Attendance
Page
Table 21.17 Main caretaker 283
Table 21.18 Main caretaker cross-tabulation 283
Table 21.19 Contact with father 283
Table 21.20 Contact with father: cross-tabulation 283 Table 21.21 Households with only one language used 284
Table 21.22 Languages spoken to the child 284
Table 22.23 Languages spoken by the child 284
Table 21.24 Mother’s current occupation 285
Table 21.25 Mother’s current occupation: cross-tabulation 285
Table 21.26 Father’s occupation 286
Table 21.27 Father’s occupation-reduced categories 286
Table 21.28 Main source of family income 286
Table 21.29 Main source of family income-reduced categories 286
Figure 21.7 Developmental milestones 287
Table 21.30 Crying at birth 288
Figure 21.8 Age at weaning 288
Figure 21.9 Hospital admissions: controls 289
Table 21.31 Length of stay in hospital 290
Table 21.32 Fits/Seizures 290
Table 21.33 Kwashiorkor 291
Figure 21.10 Current health status 291
Table 22.1 Mid-upper arm circumference at assessment 293
Figure 22.1 Outcome of hearing screening 294
Figure 22.2 Outcome of acuity screening 295
Table 23.1 Kilifi Battery - Six factor solution 297 Table 23.2 Kilifi Battery - Three factor solution 298 Table 23.3 MANOVA - simultaneous processing vs. nutritional status 300
Table 23.4 MANOVA - sequential processing vs. nutritional status 300 Table 23.5 MANOVA - co-operation factor vs. nutritional status 300
Table 23.6 MANOVA-current nutritional status 300
Page
Table 23.8 MANOVA - sequential processing vs. school attendance 302 Table 23.9 MANOVA - co-operation factor vs. school attendance 302 Table 23.10 MANOVA - simultaneous processing vs. gender 303
Table 23.11 MANOVA - sequential processing vs. gender 303 Table 23.12 MANOVA - co-operation factor vs. gender 303 Table 23.13 Comparison of group means for gender groups 304 Table 23.14 MANOVA - simultaneous processing vs. English spoken 304 Table 23.15 MANOVA - sequential processing vs. English spoken 305 Table 23.16 MANOVA - co-operation factor vs. English spoken 305 Table 23.17 MANOVA - simultaneous processing vs. family school index 305 Table 23.18 MANOVA - sequential processing vs. family school index 306 Table 23.19 MANOVA - co-operation factor vs. family school index 306
Table 23.20 MANOVA- a summary table 306
Table 23.21 Assessor by Group 307
Table 23.22 MANOVA - simultaneous processing vs. assessor 307 Table 23.23 MANOVA - sequential processing vs. assessor 307 Table 23.24 MANOVA - co-operation factor vs. assessor 307 Table 23.25 Comparison of Test Scores by assessor 308 Table 23.26 Factor reduction on observational measures 308 Table 23.27 Correlations between behaviour measures 310
Table 24.1a Simultaneous Processing Scale 311
Table 24.1b Sequential Processing Scale 311
Table 24.2 Achievement 312
Table 24.3a Attention - raw scores 312
Table 24.3b Attention - composite scores 313
Table 24.4 Visuo-Motor Speed 313
Table 24.5 Language Measures 314
Table 24.6a Behavioural observation 318
Table 24.6b Behaviour questionnaire 315
Table 25.3 MANOVA - information processing scales
Page 317
Table 25.4 MANOVA - language measures 318
Figure 25.1a Syntax 319
Figure 25.1b Semantics 319
Figure 25.1c Articulation 320
Table 25.5 Expressive language ratings 320
Table 25.6 Behaviour observation 320
Figure 26.1 Outliers by sub-test 323
Table 26.1 Significance tests of proportion of outliers 323
Figure 26.2 Outlier scores 324
Table 26.2 Levels of cognitive impairment 324
Figure 26.3 Gentile ranks: Visuo-Motor Speed 325
Figure 26.4 Gentile ranks: Arithmetic 325
Figure 26.5 Gentile ranks: Gonstruction 325
Figure 26.6 Gentile ranks: Face Recognition 326
Figure 26.7 Gentile ranks: Gestalt Glosure 326
Figure 26.8 Gentile ranks: Matrix Analogies 326
Figure 26.9 Gentile ranks: Magic Window 326
Figure 26.10 Gentile ranks: Hand Movements 327
Figure 26.11 Gentile ranks: Number Recall 327
Figure 26.12 Gentile ranks: Word Order 327
Figure 26.13 Gentile ranks: Verbal Gomprehension 328
Figure 26.14 Box plot: difference score 328
Table 26.3 Balance between information processing scales 329
Table 26.4 Balance between scale scores 329
Table 26.5 Attention: difference in error types 330
Figure 26.15 Gentile ranks: attention/planning 330
Figure 26.16 Pragmatic errors by type: cases 331
Figure 26.17 Pragmatic errors by type: controls 331
Figure 26.18 Behaviour questionnaire composite score 332
Table 26.7 Correlation between performance and behaviour
Page 334
Table 26.8 MANOVA: case/control by gender 334
Figure 27.1 Outliers by sub-test: performance measures 336
Figure 27.2 Outliers by sub-test : ratings 337
Figure 27.3 Gender distribution outliers by performance measures 338 Figure 27.4 Gender distribution outliers by ratings 338
Table 27.1 Clinical variables 339
Table 27.2 Univariate analyses of clinical variables 340
Table 27.3 Best prediction logistic regression model 341 Table 27.4 Neurological impairment and cognitive impairment 342 Table 27.5 Matching variables - significance levels 343 Table 27.6 Background measures - significance levels 345
Figure 27.5 Outcome - death 345
Figure 27.6 Outcome - cognitive impairment 345
SECTION 1: INTRODUCTION. BACKGROUND AND THEORETICAL FRAMEWORK
A: INTRODUCTION
CHAPTER 1: THE ELEMENTS OF STUDY
This study investigates the link between brain insult, cognitive development and the measurement of cognitive ability, particularly as it relates to the impact of
cerebral malaria.
Cerebral Malaria is a severe form of malarial disease which has been associated with the development of gross neurological impairments in up to 20% of survivors. It is the most common acute encephalopathy in children in Africa, and possibly in the world. Yet, prior to the inception of this study there was no published literature on the effect on the longer term cognitive development of affected children. Thus little information exists regarding either the nature or degree of any cognitive impairments associated with cerebral malaria (C.M.). An understanding of the extent of the impact of C.M. on cognitive development, and the nature and persistence of associated cognitive deficits, would aid a) the allocation of appropriate educational resources, and may aid b) the clinical management of affected children.
Following an introduction to malarial disease. Section One provides details of a theoretical framework to the investigation, which attempts to pull together the disparate strands involved. This is supplied by a synthesis of two strongly connected theoretical approaches, those of Vygotsky and Luria. There are a number of features of their work which make it appropriate to the current context. Firstly, they provide a theory of intelligence and cognitive development which link
the biological and the cultural. Secondly, whilst their primary focus is on normally occurring developmental processes, they also examine the effects of possible disruptions and interventions on the process of development. Their theoretical approaches also provide direct guidelines for assessment, but these will be
measurement process , but also to provide a framework for the interpretation of results.
The methodology required to answer the question "Does cerebral malaria constitute a risk factor for special educational needs?" has to take into account two extremely important issues. One concerns the nature of the disease itself, such that the measurements applied are sensitive to the possible impact of cerebral malaria. To provide such guidelines it was thus necessary to turn to the literature spanning a wide range of related topics, including that on malarial disease; other brain diseases and insults; and issues related to the risk factors for cognitive sequelae of brain insult in childhood. Each of these topics will be looked at in turn in chapters six to eight, in a section entitled ‘The relationship between cognitive function and disease”.
Having identified the cognitive functions which may be affected, the second issue, as it is impossible to isolate the investigation from the socio-cultural context of the disease, concerns the selection of assessment material appropriate within the particular cultural setting. This required the development of a test battery for use with the current study population. The work involved constitutes the first half of this study. Section 2: ‘The methodology and its development” reports the background to, and the results of, the test battery development.
Section 3 deals with the application of this battery to the assessment of the impact of cerebral malaria upon subsequent development. Conclusions are then drawn regarding the management of affected children both subsequent to the disease episode, and during the illness itself.
CHAPTER 2 MALARIA: THE DISEASE AND THE IMPLICATIONS FOR COGNITIVE DEVELOPMENT.
"Such is the gravity of the maiaria problem in some countries, that not only is the health of the population threatened, but also the social and economic development of the communities. " (Phillips 1983 p 1 )
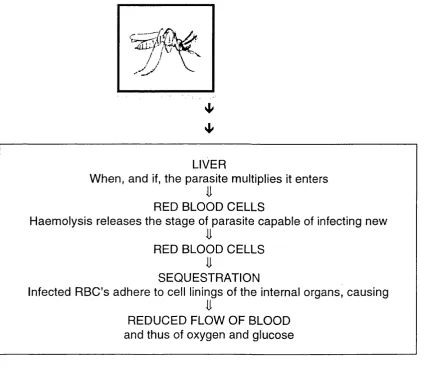
Malaria is a pathogenic parasite transmitted to humans via mosquito bites.
'■"V
LIVER
When, and if, the parasite multiplies it enters
RED BLOOD CELLS
Haemolysis releases the stage of parasite capable of infecting new
li
RED BLOOD CELLS
SEQUESTRATION
Infected RBC’s adhere to cell linings of the internal organs, causing
li
REDUCED FLOW OF BLOOD and thus of oxygen and glucose
Figure 1.1 The Parasite In The Human Host
There are four malaria parasites which can infect humans; Plasmodium
falciparum, vivax, ovale, and malarias. The following discussion will concentrate upon the malaria parasite Plasmodium falciparum because the majority of severe, life threatening, complications occur as a consequence of P.falciparum
estimates that there are 1-2 million malaria related deaths a year, the vast majority being in children aged 1-5 years (Warrell et al 1990), with about 90% of
P.falciparum related deaths concentrated in sub-Saharan Africa (World Bank 1993). Annual malaria related mortality rates in children are cited as being
between 24 per thousand in Zaire to 12 per thousand in Nigeria (Molyneux et al. 1989). Studies in the Kilifi District of Kenya have shown a minimum mortality rate of 1.1 per thousand in the under fives, based upon hospital records. However, as only 20% of all deaths were found to occur in hospital, the malaria mortality rate in the community is likely to be much higher (Snow et al 1993).
As with mortality, morbidity rates are difficult to measure accurately as the majority of endemic areas are rural, although the scale of the problem can also be estimated through hospital records (Greenwood et al 1991). For example in The Gambia 45% of all paediatric admissions were found to be related to
P.falciparum malaria (Brewster et al 1990). In coastal Kenya a study of 7538 paediatric admissions over a period of 2.5 years detected P.falciparum in the peripheral blood films of 40% of these children, with 25% of admissions recieving a primary diagnosis of malaria (Marsh et al 1995). Hospital surveilance in Kilifi, Kenya also looked at the incidence rate for under fives, of severe malaria by geographical origin of admissions, with rates as high as 46 per thousand recorded (Snow et al 1993).
In endemic areas it is not unusual to find 100% of the population infected with the malaria parasite, although this is not matched by the same levels of morbidity or mortality (Marsh 1992). High levels of malaria parasitaemia in the individual are associated with disease, but the relationship is not linear. It is not certain what causes the infection to turn to disease, or even what makes the disease take on
be rapid, taking between 1-3 days (Greenwood et al 1987). Severe disease is characterised by one, or a combination of the following: prolonged convulsions; coma; severe anaemia (Hb <5g/dl); hypoglycaemia (glucose concentration <40 mg/d I) and respiratory distress associated with severe metabolic acidosis (Warrell et al 1990, Marsh et al 1995). Once developed several of these patho physiological processes associated with severe malaria appear to run a course separate to the level of parasitization of the individual, and their effect upon the individual may also be separate from the actual malaria infection.
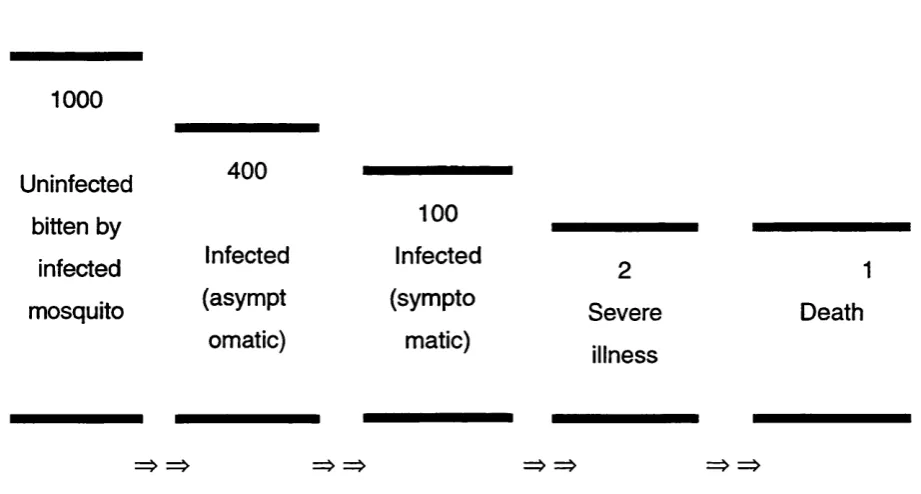
Figure 1.2
Malaria, the progression to death.
1000
Uninfected 400
bitten by 100
infected Infected Infected
mosquito (asympt (sympto
omatic) matic)
2 Severe
illness
1 Death
(reproduced from Marsh (1992) p.856)
The Relationship Of Transmission To Morbidity
Not all infective mosquito bites lead to malarial disease, and the proportion producing an infection varies widely between regions. In some areas it has found
to be as low as 1 in 20 (Mbogo 1994). Figure 1.2 is based on the average of many studies, and shows the passage of progression from mosquito bite to death, illustrating the decreasing numbers of people involved as the severity of
the outcome increases. The entomological inoculation rate (number of infectious bites per person per annum) is used as a marker for transmission pressure (Mbogo 1994, Mbogo et al 1995). Paradoxically, in areas of lower transmission pressure significant levels of malaria mortality and morbidity exist. These levels may actually decline under situations of very intense transmission (Snow et al
1994). The most marked differences observed between areas of high and low transmission are in the age profile of malaria admissions. For example, in Ifakara, Tanzania, an area of high transmission, the highest rates of malaria admissions were among children less than 1 year old. Whilst in Kilifi, Kenya, with much lower transmission, the highest rates of malaria admission were in children aged 1 - 4 years (Snow et al 1994). The explanation for this most probably centers on the speed at which protective immunity against malaria develops, a factor also held as important in determining the specific nature of malarial disease at different ages (see below for more details).
As has already been stated, in endemic areas the susceptibility to serious illness changes with age (Marsh 1992). During the first few months, probably largely due to the passive transfer of maternal antibodies in utero, there appears to be protection against disease, though not to parasitization. This immunity reduces at around 6 months of age, with the majority of extreme cases, and death, concentrated in those between one and three - four years old, the exact range varying with transmission rates (Brewster et al 1990, Marsh 1992, Snow et al
1997). Active immunity develops over early childhood, depending on the degree of exposure to infective bites. For example in the Kilifi District of Kenya the frequency of severe disease begins to diminish at around 5 years, becoming very low in adolescence and adulthood. On average each child could be expected to have experienced 4-5 discrete periods of illness by the time they are 6 years old.
1990, Marsh et al 1995). In the same studies the mean ages of occurance for cerebral malaria were recorded at 45 months and 40 months respectively. Transmission rates impact upon the spread of disease, such that in areas of lower transmission cerebral malaria is a more common feature of clinical
admissions. In the comparison of data taken from Kilifi and Ifakara, referred to above, cerebral malaria was found to be nearly four times as common in the lower transmission site (Snow et al 1994).
Cerebral Malaria
Cerebral malaria (C.M.) is the most common fatal syndrome of P. falciparum. Altered consciousness/coma, associated with widespread abnormalities of brain functioning, is the single most characteristic feature (see earlier list of other associated symptoms). There is some controversy over the defintion of impaired consciousness as it relates to cerebral malaria (Marsh et al 1995). W.H.O. criteria for C.M. centre upon deep coma, with an inability to make a localising response. A modification of this has been adopted in Kilifi to allow comparison with other research previously carried out on African children (Molyneux et al 1989, Brewster 1990). This alters the defintion to include a wider continuum of severity of illness, the diagnosis requiring impaired consciousness, with a Blantyre score of 4 or less (see Appendix 1 for specific details, Marsh et al (1995)).
C.M. has a mortality rate of betweeen 10 - 40% (Greenwood et al 1987, Molyneux et al 1989, Marsh et al 1995). The cerebral insult which results from this form of severe malaria is the patho-physiological basis for the development of long term neurological sequelae. There are a number of mechanisms which
have been suggested as implicated in the onset of cerebral insult in severe malarial disease. For example, the sequestration of infected cells in the cerebral
unknown. Secondly, cases of C.M. where no obstruction of the microvasculature has been found are not uncommon (Marsh et al 1996). Other mechanisms implicated in the onset of neurological disturbance are: Raised intra-cranial
pressure, associated with acute brain swelling (Newton et al 1991, Newton et al 1994); Seizures (Waruiru et al 1996, Crawley et al 1996); Severe metabolic disruptions, particularly of blood glucose, and lactic acid levels (Marsh et al
1996); and the prescence of high concentrations of tumour necrosis factor and other cytokines (Clark & Rocket 1996). Cytokines are produced as part of the bodies immune response. When their concentrations become very highly concentrated, it is proposed that the immune response itself becomes pathogenic (Clark & Rocket 1996). Finally, preliminary evidence from Kilifi suggests that excitotoxic mechanisms may also be present in cerebral malaria (Dobbie et al in prep.). Excitoxicity refers to the ability of naturally occuring substances, such as glutamate and amino acids, to destroy neurons when, for example, their quantity is significantly increased (Choi 1992). Such mechanisms are hypothesised to contribute to the pathogenesis of central neuronal cell loss (Choi 1992), and may therefore also have an important role to play in pathogenesis of cerebral malaria.
C.M: The impact on survivors.
Although the majority of survivors appear to make a full recovery, in studies in the Gambia, Malawi, Kenya, Tanzania and Nigeria between 5-20% of children have been found to remain with gross neurological sequelae over six months after recovery from C.M. (Molyneux et al 1989, Brewster et al 1990, Bondi 1992, Peshu et al in preparation). The following have been identified as being amongst the most common: monoparesis (weakening of a single limb); cortical blindness (loss of the capacity to distinguish forms or patterns); aphasia (inability to
express or understand words), ataxia (inability to co-ordinate voluntary movements), and hemiplegia (paralysis of one side of the body).
C.M.: The impact on the community.
unit in the Kilifi District of Kenya has concentrated on a defined study area which is under continuous demographic surveillance. It is estimated that in this area each child has a 1:15 chance of having developed severe, life threatening malaria warranting in-patient care before his/her fifth birthday. At this age
children start to attend nursery classes (there are approximately 30 in the area). Of the 1,800 children reaching this age every year there will be about 120 who have had severe malaria, 30+ of whom are survivors of cerebral malaria, (potentially one per class). A number of these, about 3-6, will have gross
neurological sequelae, and may need long term support from health and educational facilities. To date no published data is available to indicate the prevalence of more subtle impairments, and the question of how many, if any, of the remaining survivors have more subtle conditions requiring special educational support remains to be answered.
C.M.: A continuum of deficit?
It is hypothesized that there are essentially two possibilities. Firstly that there are no "hidden" impairments. This would be the case if cognitive functions are unaffected unless the cerebral insult is sufficient to also manifest itself in gross neurological deficits. Research on brain damage in children is supportive of this "critical level" for damage, before which the young brain appears to recover lost functioning, but beyond which it is unable to do so (The Kennard Principle and the "crowding effect" cited in Fingers et al 1988, and described in Chapter 7). A threshold of severity of damage for intellectual impairment is also discussed by Chadwick and colleagues in studies of children with head injuries (Chadwick et al 1981).
The second possibility is that in addition to those children with gross neurological
sequelae there is a larger group whose impairments are of a more subtle cognitive or behavioural nature, and which might only become apparent at school entry. This would be the case if the gross impairments identified are part of a
that whilst the presenting features associated with eventual neurological sequelae are, in the main, the same as those associated with mortality (that is coma and hypoglycaemia) (Brewster et al 1990; Molyneux et al 1989; Marsh et al 1995), there are additional features which are associated with neurological sequelae alone. These include severe fitting, which may also contribute to the development of more subtle sequelae. Futher research on the longer term
development of all survivors of C.M., is required in order to establish whether deficits follow an all or nothing principle, or whether a continuum of impairments emerge.
C.M.: Measuring the nature and extent of impairment.
In reviewing research on parasitic infections and cognitive functions Kvalsvig (1988) points out that for an assessment battery to be sensitive to the effect of an infection there needs to be prior knowledge of the cognitive functions which are likely to be affected by the disease in question, relevant tests can then be included to assess these functions. Despite the importance of cerebral malaria in the non-industrialised world only one study was located in literature on the effects of cerebral malaria on cognitive functioning. This compared the performance, on a battery of psychological tests, of nine adults defined as having cerebral malaria, with a non-cerebral malaria group (KastI et al 1968). The tests were administered both during illness, and at discharge. Whilst the cerebral group was found to perform at a significantly lower level on tasks of short term memory, visuo-spatial organization, sequential processing and speed of
processing when ill, the two groups no longer differed on discharge. The pattem of results found was interpreted to mean that although during illness there is evidence of cerebral dysfunction, the adult brain appears to recover fully when health is restored. It needs to be stressed, however, this is a non-comparable
group to that of the current study. Firstly the assessemnts were made upon adults, and secondly the defintion of cerebral malaria given did not necessarily include impaired consciousness. Therefore these results are of little current relevance.
The results of another, much more closely comparable study, was published after the data collection on the current study had been completed (Muntendam et al 1996). It therefore could have no influence upon the design of the current study. The study was carried out in the Gambia on 36 matched pairs of children, one of
each pair being a survivor of C.M.. Their performance was compared on a battery of eleven neuropsychological tests. No evidence was found of a serious long-term impairment on the C.M. children. This study will be reviewed in more detail in the discussion section of the current study.
In the abscence of any further direct precedents, a wider literature, relating to the
B: COGNITIVE DEVELOPMENT AND COGNITIVE IMPAIRMENT - THE THEORETICAL FRAMEWORK
CHAPTER 3 COGNITIVE DEVELOPMENT - A VYGOTSKIAN FRAMEWORK
"At the beginning of development there stands the act, independent of the word, then at the end of it there stands the word which becomes the act, the word makes man’s action free. ” (Vygotsky & Luria 1994 p.170)
This chapter is an interpretation of Vygotsky's theoretical explanations of the path of cognitive development. It aims to describe the main influences upon cognitive development, and the main causes of differential development. In so doing it also aims to draw implications for the design and implementation of the current study.
Stages of development
In Vygotskian theory change can be characterised as occurring in stages. The early stages being dominated by natural processes and elementary mental functions. The later stages are dominated by social processes and higher mental functions (Wertsch 1985). The passage from one stage to another is accounted for not by quantitative differences, but by qualitative shifts (Vygotsky 1966/1991 ) \ Take for example the development of memory, this does not develop simply by being able to remember ever increasing amounts, but by becoming "logical memory", guided by meaning and deliberately applied by the child. In a series of experiments described by Leont’ev (1932/1994) the memory functions of young children were found to depend upon direct memory, that is memory functioning which is not organised with the use of memory aids (mnemonic devices). Changes with age were not caused by merely a quantitative increase in capacity. Rather the integration of mnemonic devices into memory function, that is the integration of thought with memory, appeared to create a qualitatively different form of memory, mediated memory. The use of mnemonic devices was found to dominate in the performance of adults on memory tasks
(Leont'ev 1932/1994).
In the case of attention, change is said to be from behaviour which functions by being attracted by an external source, to becoming dependent upon the child's own thinking, that is 'selective attention' (Leont'ev 1932/1994). The theory suggests, as the example of memory given above also illustrates, that the end point is the development of conscious activity and deliberate mastery, where
consciousness is defined as the state of awareness and understanding (Vygotsky 1934/1986).
Functional Systems
Describing development purely in terms of individual functions, such as memory,
perception and attention, is inappropriate within the Vygotskian framework, as mental functions are seen to be combined in a highly complex inter-relationship. Individual functions do not develop separately because they do not operate in isolation from other mental functions. Rather, successful completion of any psychological activity depends upon their operating together. In Vygotsky's words,
"the fate of each functional ingredient of consciousness thus depends upon the deveiopment of the entire system." (Vygotsky 1934/1986 p 167).
This was illustrated in a lecture given by Vygotsky on the development of perception (Vygotsky 1960/1987). A series of experiments was described which investigated the processes involved in the perception of magnitude. Of particular interest was how compensation for changes in distance was achieved, when
judging relative size. For example how are two pencils of identical length, one close and one far, perceived as being equal in size, even though on a sensory level the retinal image of the further pencil is smaller? These experiments involved judgements of relative size being made for different combinations of: objects, projected images, and the dependence upon memory of an object
constancy of perceptions are closely inter-linked with memory functions (Vygotsky 1960/1987).
Each level of maturity is characterised by a different relationship between mental
functions. In the course of development behaviour becomes governed by increasingly more complex, and inter-related systems of functions (Vygotsky & Luria 1994). However regression to earlier less complex and more independent functioning can happen when damage or decay affects the physiological
structure of the brain (Vygotsky 1966/1991).
Agents of Change
A common thread underlying change and development across all functions and domains, though not necessarily occurring simultaneously in each domain, is the mastery and use of tools and signs. Tools (also referred to as technical tools) are objects used to complete a task, such as a stick for digging. Vygotsky differentiated between human tools and animal tools. The differences between the ape and the young child lie primarily in the different combinations of psychological functions that guide the use of the tool (Vygotsky & Luria 1994). The behaviour of the ape takes place within a narrow time frame. A problem is encountered, e.g. termites are found down a narrow hole, a stick is seen and used to solve the problem by digging the termites out. Visual perception therefore dominates the process (Kohler cited in Vygotsky 1960/1987). Human activity is not so dependent upon visual perception, but is guided by a combination which includes memory functions. For example, a stick may be specifically sought from another location, or, later in development, it may be carried in anticipation of its use. Human activity is therefore more purposeful and directive.
Signs and symbols (psychological tools) are also important in distinguishing between animal and human intellect. They are central to the development of
speech; counting systems; mnemonic techniques/devices; art; writing; maps etc. (Wertsch 1985). Since, as stated earlier, development is a process of qualitative change, the process of learning these mediational means will facilitate both the specific psychological activity to which they are being applied, and change the
very nature of thought, of psychological activity in general (Vygotsky 1934/1986).
The essential difference between technical and psychological tools is that the former are external and act externally to the person to change the object of the
activity being undertaken, whilst signs and symbols are psychological, in that they alter mental functioning internally. Psychological tools act more as a catalyst to activity, not altering the external object directly, but influencing the ability of
internal mental processes to complete the activity (Vygotsky and Luria 1994).
The Socio-Historical Context Of Learning
The tools available to the individual have been referred to as "socio-cultural technologies" (Rogoff 1989/1991), the selection being largely determined by those used in the immediate cultural environment. In Vygotskian theory learning and development occur within the social context, which is also referred to as the historical domain (Wertsch 1985). The young child experiences acts outside of itself, which are often being carried out in relation to itself. It is the process of assigning meaning to this activity, and of bringing it into voluntary control, which is central to the development of higher mental functions (Vygotsky & Luria 1994). The action is given meaning by the 'adult' involved, (not necessarily an adult per se, but at least a person operating at a higher level of mental functioning). The child does not need to understand the purpose of the activity, or share a common goal with the adult, to take an active part. S/he eventually acquires that meaning
as his/her own, but not necessarily in the same form as it was presented. The process of the internalisation of meaning is not one of passive acquisition, of a straightforward transferral of knowledge. Rather it is a process of transformation,
Yssevich; Leont'ev; cited in Vygotsky & Luria 1994). Zankov's tests required the subjects to memorise word lists, with abstract figures provided as potential memory aids. Young children ignored the aids. Older children did use them, but only after transforming the figures into meaningful symbols. Thus if a symbol
presented could, through rotation or inversion, be made to resemble the object to which it was attached, only then would it be used. (E.g. a triangle might be used to remember ice-cream cone, but a square would not).
This description of the child as an active learner is similar to that supplied by Piaget in relation to the concepts of assimilation and accommodation (Vygotsky 1934/1986). The difference between the two theoretical approaches arises in the importance attached to the context in which psychological activity occurs. From the Vygotskian perspective child development is a social activity, s/he is not the Piagetian solitary thinker. Thinking develops through social guidance, and is thus moulded and developed, and may even be constrained, by it. That is not to say that the child is only a product of his/her environment. Vygotsky described two equally important roots of development, the natural/biological, and the social/historical. They begin independently, with biological development pre dating the social. As internalisation of the social experiences increases they do not supplant the biological processes. Rather the two become interdependent, creating a qualitatively different potential from that to be expected if they should act independently. The biological influence upon development is not expanded upon in the same detail as the social-historical by Vygotsky himself. It is to the closely related work of his colleague, Luria, that one must turn for a working model of brain functions and the brain - behaviour link.
The Process Of Development
To complete this summary of the Vygotskian description of the social-historical stages of development, it is appropriate to look next at the concept of the Zone of
Proximal Development, which, in the words of Minick is;
"the primary locus of change in human psychological development”.
The Zone of Proximal Development, or ZPD, has been defined by Vygotsky as the distance between a child's
"actual developmental level as determined by independent problem solving" and the higher level of " potential development as determined through problem solving under guidance or in collaboration with more capable peers."(Vygotsky cited in Wertsch 1985 p.67).
As an example, take two children whose test performance places them both at the 6 year level. With careful prompting one child succeeds at tasks at the 7 year level, and the other, with the same prompts, at a 9 year level. Their understanding is not therefore at the same level, as was suggested by the first measure.
Tharp and Gallimore presented a four stage model which clearly illustrates transition through the ZPD (Tharp and Gallimore 1988). During Stage 1 performance is assisted by more capable others. Instruction at this stage is characterised by the manipulation of a number of features of the activity by the adult even before the interaction with the child begins. The adult anticipates the level of functioning of the child by adjusting: the choice of the tasks to be given; the selection of tools and materials; and the form of instructions. To solve the problem of finding a missing shoe, for example, the adult may ask the older child "Where did you last remember having it ?". Task analysis would be applied for a younger child, with a series of more directed questions such as " Did you have it in the kitchen?..in the bedroom? etc.". A younger child still would be accompanied on the hunt, with appropriate verbal labels being attached to define the activity being carried out. "Let's look in the kitchen, is it here? etc.".
Modifications and reductions occur in the quantity and quality of help the child requires in order to complete a task, up until the point where, in that domain. Stage 2 in reached. At this point performance has begun to be assisted by the
of the importance of this stage are several sources, many cited in Tharp and Gallimore, indicating that teaching overt self-instruction improves performance particularly in 'impulsive' children (Gaddes & Edgell 1994).
During Stage 3 performance is "developed, automatised and fossilized"
(Tharp and Gallimore 1988). It no longer requires external assistance, and in fact at this stage assistance might even be considered to be disruptive. For example early counting at Stage 2 may be aided by the use of external aids such as fingers or beads. At Stage 3 counting skills will have been internalised to the point where such external aids are longer used. Indeed the imposition of an external system at this level can actually slow down the completion of the activity.
The achievement of independent internally controlled performance is not the final stage however. Learning and development continue in other domains, and during Stage 4 the learner will revert to earlier stages, actively seeking assistance where necessary to master new skills. Although placed later than Stage 3, performance at Stage 4 is characterised by performance at earlier levels. Returning to the example of counting activities, and mental arithmetic, at Stage 4 the child who can now count internally will probably need to return to earlier stages when the problems involve either larger numbers, or other processes, such as subtraction, as well.
What is highlighted by the Tharp and Gallimore model is the dynamic nature of cognitive ability, a concept central to the Vygotskian approach. This has important implications for the assessment of cognitive abilities, and the measurement of levels of development. The concept of the ZPD provides a framework for developing informative assessment tools. In support of its
importance and value Vygotsky found through investigation,
"... that the child with the larger zone of proximal development will do much better in school."(Vygotsky 1934/1986 p.187).
Indeed he stated the measurement of the ZPD had more pedagogical value than one session, test only, measures of ability. The measurement of the ZPD will be discussed in more detail in Chapter 10.
Another important theme to be touched on above is the role of instruction in cognitive development. Whilst it is of major importance in guiding development, the reference to the child being actively involved in the internalisation of the use of signs must not be forgotten. It would be erroneous therefore to see the role of instruction as exclusively to pull development behind it, although this may be the
case at times.
Thought And Speech
Amongst the signs involved in the development of higher mental functions, language is the most important (Vygotsky 1934/1986). At the point in development where the external operations mediated by language turn inwards, the specific language environment becomes an integral part of the thought processes. A comparison was made between the conceptual categorisation of Native and Anglo Americans by Carrol and Casagrande (1958), which clearly illustrates this. Subjects were required to select the two, out of three, pictures which they judged to be illustrating the same concept. It was hypothesised that the two groups would differ in the pairings made, and that these differences would be attributable to differences in linguistic structure between Hopi and English, the two languages involved. Results supported these hypotheses. For example, where the three pictures portrayed pouring, spilling and dropping, Hopi speakers classified the first two together, and English speakers the last two. In Hopi a distinction is made between dropping objects and liquid, but not between intentional and accidental pouring. Whilst to English speakers the more salient
dimension seemed to be the intentionality of the act.
After studying the results of research on apes and humans (Kohler cited in
thought and speech have different genetic routes, initially developing independently, upon different lines. Early thought is pre-linguistic, and early speech is at a pre-intellectual level. At a later point in development thought
becomes verbal and speech rational. When the two lines of development do meet "the nature o f the development Itself changes" (Vygotsky 1934/1986 p.94). One aspect of this relationship can be illustrated by the example of studies
of aphasies, carried out by Vygotsky and colleagues (cited in Vygotsky & Luria 1994). The loss of language abilities was found to be associated with fundamental changes in behaviour, particularly evident in an inability to organise and co-ordinate functions in the completion of a task. Language appears to have been an integral part of thought processes, guiding planning and strategies. The impairment of language left the functions required to complete the tasks unimpaired, but the implementation of activity severely disrupted.
The Development of Concepts
Another perspective on the relationship between language/speech and thought, and the changing relationship between the two throughout development, comes from the study of the development of concepts. Vygotsky's description of the development of concepts was based upon experiments carried out in collaboration with Sakharov (cited in Sakharov 1930/1994 and Vygotsky 1934/1986). These experiments consisted of categorisation tasks requiring that wooden blocks, varying in size, colour and shape, be sorted according to concepts fabricated for the study, and labelled with nonsense words. The process by which solutions were sought by adults, adolescents and children was compared. Qualitative differences emerged between children and the other two age groups, in the way objects were categorised, and the way relationships between objects were perceived. In childhood the focus was upon concrete and
perceptual similarities between objects. In adolescence, continuing into adulthood, concepts emerged which were abstract and logical. In childhood the process of selection for inclusion into a category was often done on an item by item basis, with each successive item only being compared to the one