ARTICLE
An Intervention to Decrease Narcotic-Related
Adverse Drug Events in Children’s Hospitals
Paul J. Sharek, MD, MPHa,b, Richard E. McClead, Jr, MDc, Carol Taketomo, PharmDd, Joseph W. Luria, MDe, Glenn S. Takata, MD, MSf,g, Beverly Walti, MSN, CPNP, CNSh, Marla Tanski, PharmDi, Carla Nelson, MPH, CPHQj, Tina R. Logsdon, MSk, Cary Thurm, PhDk, Frank Federico, PharmDl
aDivision of General Pediatrics, Department of Pediatrics, Stanford University School of Medicine, Palo Alto, California;bDepartment of Quality Management, Lucile
Packard Children’s Hospital, Palo Alto, California;cDepartment of Pediatrics, Ohio State University School of Medicine, Columbus, Ohio;dDepartment of Pharmacy and fDivision of General Pediatrics and Patient Safety Program, Childrens Hospital Los Angeles, Los Angeles, California;eDivision of Emergency Medicine, Cincinnati Children’s
Hospital Medical Center, Cincinnati, Ohio;gDepartment of Pediatrics, University of Southern California Keck School of Medicine, Los Angeles, California;hDepartment of
Nursing, Children’s Hospital of Orange County, Orange, California; Departments ofiPharmacy andjQuality Management, All Children’s Hospital, St Petersburg, Florida; kPerformance Improvement Division, Child Health Corporation of America, Shawnee Mission, Kansas, and Quintiles, Overland Park, Kansas;lInstitute for Healthcare
Improvement, Cambridge, Massachusetts
The authors have indicated they have no financial relationships relevant to this article to disclose.
What’s Known on This Subject
ADEs occur at the rate of 15.7 per 1000 patient-days in hospitalized children. Narcotics are the most frequent drug class associated with these harms, resulting in 51% of ADEs in hospitalized children.
What This Study Adds
To our knowledge, this study is the first to reveal a significant collaborative-wide reduc-tion in narcotic-related ADE rates in hospitalized children after implementareduc-tion of a simple “change package” of best practices.
ABSTRACT
OBJECTIVES.Narcotic-related adverse drug events are the most common adverse drug events in hospitalized children. Despite multiple published studies describing inter-ventions that decrease adverse drug events from narcotics, large-scale collaborative quality improvement efforts to address narcotic-related adverse drug events in pe-diatrics have not been described. The purpose of this study was to evaluate collab-orative-wide narcotic-related adverse drug event rates after a collection of expert panel– defined best practices was implemented.
METHODS.All 42 children’s hospitals in the Child Health Corporation of America were invited to participate in the Institute for Healthcare Improvement–style quality improvement collaborative aimed at reducing narcotic-related adverse drug events. A collection of interventions known or suspected to reduce narcotic-related adverse drug events was recommended by an expert panel, with each site implementingⱖ1 of these best practices on the basis of local need. Narcotic-related adverse drug event rates were compared between the baseline (December 1, 2004, to March 31, 2005) and postimplementation periods (January 1, 2006, to March 31, 2006) after an a priori– defined intervention ramp-up time (April 1, 2005, and December 31, 2005). Secondary outcome measures included constipation rates and narcotic-related au-tomated drug-dispensing-device override percentages.
RESULTS.Median narcotic-related adverse drug event rates decreased 67% between the
baseline and postimplementation time frames across the 14-site collaborative. Constipation rates decreased 68.9%, and automated drug-dispensing-device overrides decreased from 10.18% to 5.91% of all narcotic doses administered.
CONCLUSIONS.Implementation ofⱖ1 expert panel–recommended interventions at each participating site resulted in a significant decrease in narcotic-related adverse drug events, constipation, and automated drug-dispensing-device overrides in a 12-month, 14-site children’s hospital quality collaborative.Pediatrics2008;122:e861–e866
A
DVERSE DRUG EVENTS(ADEs) in pediatric inpatients are common, costly, and occasionally life-threatening or fatal. In a recently published study that reviewed 960 inpatients from 12 children’s hospitals,1the mean rate ofADEs in US children’s hospitals was 11.1 per 100 admissions with 22.4% classified as preventable. This extrapolates to a mean of 174 preventable ADEs per children’s hospital per year. In addition, Kaushal et al2found that 7% of
pediatric inpatient ADEs were “fatal or life-threatening.” Using an estimated cost of $4685 per preventable ADE,3
these preventable ADEs resulted in direct costs of $909 644 per children’s hospital per year.
The national implications of these rates are striking; extrapolating from US hospital statistics4an estimated 160 840
preventable ADEs and 11 260 preventable fatal or life-threatening events at an estimated cost of $753.5 million occur www.pediatrics.org/cgi/doi/10.1542/ peds.2008-1011
doi:10.1542/peds.2008-1011
Key Words
adverse drug event, narcotic, pediatrics, harm, patient safety
Abbreviations ADE—adverse drug event CHCA—Child Health Corporation of America
IRB—institutional review board IHI—Institute for Healthcare Improvement
Accepted for publication Jun 17, 2008 Address correspondence to Paul J. Sharek, MD, MPH, Lucile Packard Children’s Hospital, 700 Welch Rd, No. 227, Palo Alto, CA 94304. E-mail: [email protected]
in US pediatric inpatients annually. Interventions aimed at decreasing preventable ADEs in pediatrics are needed to reduce the serious public health and social conse-quences of this harm to our nation’s most vulnerable patient population.
To understand better the ability of interventions to reduce or eliminate ADEs in pediatric inpatients, we studied narcotic-related ADE rates in the 14-site Reduc-ing Narcotic-Related Adverse Drug Events in Children improvement collaborative. Narcotics were specifically targeted because this medication class is high risk,5high
priority,6 frequently used in inpatient children (data
from Child Health Corporation of America’s [CHCA’s] Pediatrics Health Information Systems, an administra-tive database from 38 freestanding, academic, not-for-profit, tertiary care pediatric hospitals in the United States, suggest that 41% of the 363 689 discharges from 38 children’s hospitals in 2004 were provided at least 1 dose of a narcotic)7and is associated with 33% to 51% of
pediatric ADEs.1,2 The objective of this study was to
evaluate the effect of a combination of evidence-based interventions on narcotic-related ADE rates in hospital-ized children during the course of a 12-month, 14-site quality improvement collaborative project.
METHODS
Study Population
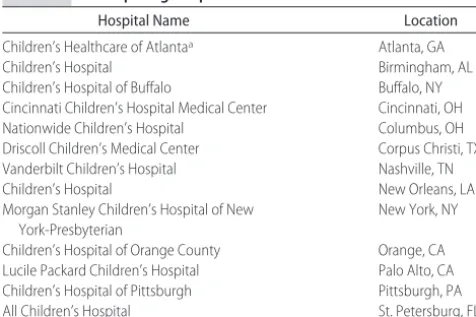
Fourteen freestanding children’s hospitals participated in a 12-month improvement collaborative project enti-tled the Reducing Narcotic-Related Adverse Drug Events in Children improvement collaborative (Table 1). Inclu-sion criteria required participation for the entire 12-month project period and a minimum requirement of at least 50% of monthly data submitted. Sites were ex-cluded from this analysis when they joined after April 1, 2005, or when they contributed data for ⬍6 of the 12 months of the collaborative. This project was sponsored by the CHCA (Shawnee Mission, KS), a business alliance of 42 children’s hospitals. The project was open to all 42 freestanding children’s hospitals affiliated with the CHCA as of January 1, 2005, and was funded by a grant from the Agency for Healthcare Research and Quality
and CHCA Research and Development funds. The CHCA obtained institutional review board (IRB) approval for data management and analysis from an external IRB (Western IRB, Olympia, WA), and each participating site obtained local IRB approval or waiver before project participation.
Intervention
The project design and content were developed by a multidisciplinary pediatric expert panel that consisted of invited staff from participating hospitals and external subject matter experts (7 clinical and 4 improvement/ process experts [see Acknowledgments]). This panel de-veloped a comprehensive, pediatric-specific “change package” of evidence-based practices organized into the broad categories of (1) narcotic use, (2) medication sys-tems, (3) medication reconciliation, and (4) culture of safety. The change package (available at www.chca. com) was based on high-risk medication change pack-ages previously developed by the Institute for Healthcare Improvement (IHI).8 Because the change package was
broad in scope, 4 primary areas for active collaboration were selected. First, constipation, known to be a fre-quent narcotic-associated ADE,1was addressed by
rec-ommending the routine proactive use of laxatives and stool softeners when narcotics are prescribed. This type of order, called a “corollary order,” has been shown in the literature to decrease the frequency of medication-related errors of omission.9 Second, overrides of
auto-mated medication dispensing devices, known to increase the risk for medication errors,10 were targeted with a
recommendation to limit override opportunities. Third, withdrawal symptoms, a significant ADE with ineffec-tive weaning of medication doses after extended nar-cotic use, was targeted for improvement by recom-mending a standardized weaning protocol. Finally, ADEs that occur at the high-risk transfer process11
were addressed by recommending consistent medica-tion reconciliamedica-tion strategies.11,12
The IHI collaborative quality improvement model,13
including meeting structure (3 face-to-face learning ses-sions), communication strategies (monthly conference calls, active Listservs, and available content and quality experts), and monthly data submission and reporting, was used to facilitate quality improvement in this col-laborative. Each site assembled a multidisciplinary team and designated a site leader and a senior leader. Hospi-tals learned improvement methods and strategies that were based on the Model for Improvement,14 which
emphasizes small tests of change (plan-do-study-act), as well as specific sustain and spread strategies. Hospitals were also free to apply other improvement methods, such as Lean15or Six Sigma.16During the collaborative,
site teams made numerous process improvements and reported key outcome and process measures on a Web-based data repository. Full transparency in the form of unblinded data and open sharing of successes and bar-riers was a critical requirement for participation. The effort was coordinated by central staff who were em-ployed by the CHCA. These CHCA staff members pro-vided feedback and formal reports to sites monthly,
TABLE 1 Participating Hospitals
Hospital Name Location
Children’s Healthcare of Atlantaa Atlanta, GA
Children’s Hospital Birmingham, AL
Children’s Hospital of Buffalo Buffalo, NY Cincinnati Children’s Hospital Medical Center Cincinnati, OH Nationwide Children’s Hospital Columbus, OH Driscoll Children’s Medical Center Corpus Christi, TX Vanderbilt Children’s Hospital Nashville, TN
Children’s Hospital New Orleans, LA
Morgan Stanley Children’s Hospital of New York-Presbyterian
New York, NY
Children’s Hospital of Orange County Orange, CA Lucile Packard Children’s Hospital Palo Alto, CA Children’s Hospital of Pittsburgh Pittsburgh, PA
All Children’s Hospital St. Petersburg, FL
planned and implemented learning sessions, provided content oversight and process management for the col-laborative, communicated progress to site-specified se-nior leaders on an ongoing basis, and produced final deliverables describing the results of the project. All site members had access to a project-specific Web site and listserv coordinated by the CHCA. The baseline phase occurred between December 1, 2004, and March 31, 2005, and the “implementation phase” of the project spanned 12 months from April 1, 2005, to March 31, 2006. For determination of the effects of the collabora-tive on outcomes, results were reported on a quarterly basis; the collaborative defined a priori that the final results would be reported on the basis of the final quar-ter of the project, January 1, 2006, through March 31, 2006.
Patients were eligible for inclusion when they were pediatric inpatients discharged between December 1, 2004, and March 31, 2006; had a minimum 24-hour length of stay; and received at least 1 dose of a narcotic medication. Patients were selected and classified on the basis of discharge date, regardless of when the narcotic medications were administered. ADEs were identified using a modified trigger tool specifically designed for narcotic ADE detection, a method developed by the IHI17–19 and adapted for pediatric patients by the
CHCA.1,20The trigger tool detection method was used in
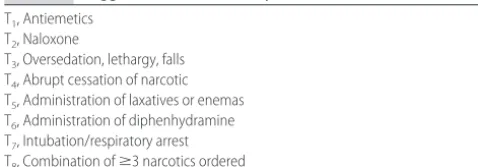
a consistent manner throughout the course of the study. ADE data were collected for 20 randomly selected eligi-ble patient discharges per site per month. Chart review-ers were instructed to focus on 8 triggreview-ers that typically are associated with narcotic ADEs (Table 2) and spend a maximum of 20 minutes per chart reviewed as recom-mended by the IHI trigger tool method.17,21 Sites
col-lected information on narcotics dispensed from auto-mated medication dispensing devices, both as total narcotic doses dispensed and the number of doses dis-pensed via an override. An override was defined as any process that allowed the pharmacist order verification step to be bypassed so that nurses can obtain medica-tions before a pharmacist review.
Outcome Measures
An ADE (harm) was defined as an injury, large or small, caused by the use of a drug, including both preventable and nonpreventable events.1,21,22This project did not
in-clude harm from nonuse of narcotics (“error of omis-sion”), such as unrelieved pain. All events classified as categories E through I of the National Coordinating
Council for Medication Error Reporting and Prevention Index for Categorizing Errors23were included.
The primary outcome measure was narcotic-associ-ated ADE rates (expressed as either per 1000 narcotic patient-days or per 1000 narcotic doses). Secondary out-comes included constipation rates (per 1000 narcotic patient-days or per 1000 narcotic doses) and percentage of narcotics dispensed via an automated medication dis-pensing device using an override (doses overridden di-vided by total doses dispensed). Most sites did not ac-tively pursue withdrawal-related ADEs or medication reconciliation related specifically to narcotics; therefore, no outcomes related to these interventions were system-atically collected. The estimated number of ADEs averted was calculated for each site and for the collabo-rative as a whole by using the difference between the baseline ADE rate and the rates reported during each month of the collaborative. Collaborative-wide targets were established for each measure; teams were encour-aged to customize and/or set additional targets to meet individual site goals.
Sites were instructed to collect monthly baseline data for the period December 1, 2004, through March 31, 2005, and to report project data on a monthly basis for 12 months (April 1, 2005, through March 31, 2006). Monthly site data were reported to the CHCA via a secure Web-based data repository hosted by the IHI. Hospitals used either standardized data collection forms developed by the CHCA or processes developed at the individual institution to translate chart review and elec-tronic data to monthly results.
Statistical Methods
The primary outcome measure for this project was the rate of narcotic-related ADEs per 1000 narcotic doses or per 1000 narcotic days. Sites were encouraged to use the denominator most appropriate for their particular site. To combine results from hospitals that submitted the measure in terms of doses and days, we computed, for each hospital, a percentage change from baseline for each of the postbaseline quarters. We then used the Wilcoxon signed-rank test to determine whether the percentage change was different from 0. A similar strat-egy was used to determine the statistical significance of the percentage change in constipation rates. To assess whether a significant change occurred from baseline to postimplementation time period for override percent-ages, we used the nonparametric Wilcoxon rank-sum test. We hypothesized that the primary and secondary outcome measure rates would be reduced between base-line and the postimplementation time frame. Because of the variation in the specific interventions implemented by each site and the variable time frames for implemen-tation, the rates of successful implementation of any given improvement practice were not calculated.
The total number of ADEs averted during the project was computed for the sample population on the basis of the difference between the baseline rate and rates re-ported during each month of the collaborative. The number of ADEs averted for the entire 14-site collabo-rative was extrapolated from the project sample
popula-TABLE 2 Trigger List Used to Identify Narcotic-Related ADEs T1, Antiemetics
T2, Naloxone
T3, Oversedation, lethargy, falls
T4, Abrupt cessation of narcotic
T5, Administration of laxatives or enemas
T6, Administration of diphenhydramine
T7, Intubation/respiratory arrest
tion (20 per month per site) to the entire 14-site hospital population.
The data for the measures were nonnormally dis-tributed. Thus, measures were aggregated on a quar-terly basis by using medians with interquartile ranges. Missing data were imputed by using the previous data point carried forward.24 The reported P values are
2-sided, and P ⬍ .05 was considered significant. All analyses were performed by using SAS 9.1 (SAS In-stitute, Inc, Cary, NC).
RESULTS
Forty-two children’s hospitals in the CHCA were invited to participate in the Reducing Narcotic-Related Adverse Drug Events in Children improvement collaborative, 17 of which agreed to participate. Two of these 17 hospitals were excluded from data analysis on the basis of subop-timal data submission (1 site submitted 5 months of data, the second submitted 0 months of data), 1 hospital was excluded on the basis of late entrance into the collabo-rative (July 2005), and 1 hospital declined release of its data for publication. Thus, 14 children’s hospitals met all inclusion requirements; 13 sites composed the final group for analysis (Table 1).
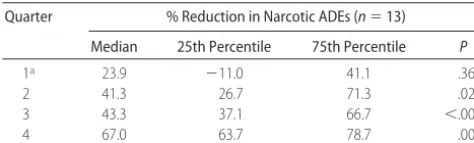
Narcotic-related ADE rates, measured either per 1000 narcotic doses or per 1000 narcotic days, decreased 67% between baseline and postimplementation time frames (n ⫽ 13; P ⬍ .001; Table 3). Statistically significant reductions in rates were noted in quarters 2 and 3 as well as 4 (the postimplementation time frame). The median rate at baseline was 41.0 narcotic-related ADEs per 1000 narcotic doses (n⫽10 sites) and 164.9 narcotic-related ADEs per 1000 narcotic days (n⫽3). Median constipa-tion rates increasingly declined each quarter as well, with a statistically significant reduction of 69% seen in the postimplementation time frame (n⫽13;P⬍.005; Table 4). The median rate at baseline was 14.1
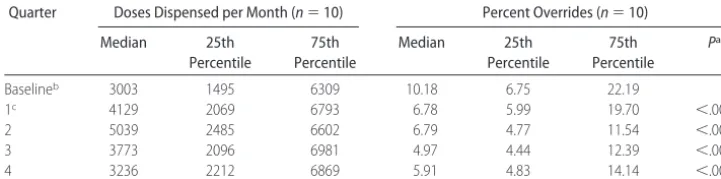
constipa-tion events per 1000 narcotic doses (n⫽ 10 sites) and 36.1 constipation events per 1000 narcotic days (n⫽3). Median override rates declined significantly each quar-ter, with the postimplementation time frame reduced from 10.2% to 5.9% (n⫽10 [42%];P⬍.001; Table 5). Three sites submitted ⬍50% of override data and thus were excluded from this outcome analysis on the basis of our a priori– defined inclusion criteria.
On the basis of these results, we extrapolated the difference between the absolute number of expected (baseline) ADEs and the actual ADEs during the imple-mentation and postimpleimple-mentation time frames to esti-mate that 14 594 ADEs were averted during the full 12-month intervention time frame in the 13 hospitals that submitted ADE data.
DISCUSSION
The goal of the Reducing Narcotic-Related Adverse Drug Events in Children improvement collaborative was to improve narcotic-related medication safety in participat-ing children’s hospitals. Narcotic-related ADE rates de-creased 67% between the baseline and postimplemen-tation time frames. The constipation subset of ADEs decreased significantly as well, as did the percentage of narcotic overrides. We believe this to be the first report of a pediatric-specific medication safety collaborative to demonstrate a significant reduction in narcotic-related ADEs.
This study suggests that a large-scale collaborative project, focused on reducing the incidence of narcotic-related ADEs in children’s hospitals, is feasible and can have important public health consequences. This is of particular importance because, to our knowledge, no published studies have shown significant reductions in ADEs in large-scale pediatric collaboratives. We believe that this collaborative was successful at reducing narcotic-related ADEs for several reasons, including the availabil-ity of a robust performance improvement infrastructure at the CHCA to facilitate this work, the willingness of each site to share openly data and practices (transpar-ency), and a public commitment to remaining on sched-ule with assigned tasks (accountability). Each of these success factors is thought to be a crucial component of an effective collaborative.25
On the basis of these results, we believe that impor-tant reductions in morbidity and health care costs are possible if our change package to reduce narcotic-related ADEs in hospitalized children is introduced nationwide. Between 33% and 51% of all pediatric ADEs are caused by narcotics,1,2 and an estimated 160 840 preventable
ADEs and 11 260 preventable fatal or life-threatening ADEs occur annually in pediatric inpatients in the United States. Because ADEs in the pediatric population are frequently associated with narcotics, our experience suggests that a significant amount of the total ADE bur-den in children could be eliminated with universal im-plementation of our change package.
This study had several limitations. First, the pre–post intervention study design limits our ability to assign causality between the intervention and the primary out-come of decreased narcotic-related ADE rates. Evidence
TABLE 3 Percentage Reduction in Narcotic-Related ADE Rates Collaborative-wide From Baseline
Quarter % Reduction in Narcotic ADEs (n⫽13)
Median 25th Percentile 75th Percentile P
1a 23.9 ⫺11.0 41.1 .367
2 41.3 26.7 71.3 .021
3 43.3 37.1 66.7 ⬍.001
4 67.0 63.7 78.7 .001
aApril 1, 2005, through June 30, 2005.
TABLE 4 Percentage Reduction in Constipation Rates Collaborative-Wide From Baseline
Quarter % Reduction in Constipation (n⫽13)
Median 25th Percentile 75th Percentile P
1a 29.0 ⫺7.8 66.8 .14648
2 38.3 ⫺5.1 61.6 .15137
3 45.6 0.9 72.8 .09229
4 68.9 60.5 94.2 .00049
supporting that this decrease is related to the implemen-tation of the change package is reflected in attainment of the collaborative-wide goal of decreasing constipation, a major subset of ADEs resulting from narcotic adminis-tration in pediatric inpatients. In pre–post studies, there is no way to determine the effect of secular trends on outcomes; however, we are not aware of any clear na-tionwide interventions implemented during the course of our project that could account for large-scale im-provements at these 14 geographically and demograph-ically diverse children’s hospitals. Hence, although we believe that these improvements were the direct result of collaborative implementation of the change package, it is possible that other, unmeasured and unrecognized fac-tors could have contributed.
Second, there is the risk for underreporting of nar-cotic-related ADEs after implementation of the interven-tion. Local site data were not verified by study personnel for accuracy, and data collectors were not blinded to study time frames. If postimplementation narcotic-re-lated ADEs were underreported, then this would create a measurement bias that would exaggerate the results. We believe that this is unlikely because a standard trig-ger tool method17–21 was used at the beginning of the
project and used in a consistent manner throughout by consistent personnel at each site.
Third, we did not evaluate compliance with the change package, limiting our ability to link directly the intervention with the outcome. Measuring compliance with the change package would have been challenging, particularly in light of the heterogeneity among site practices at baseline, and was beyond the scope of this pragmatic quality improvement project. Fourth, we did not attempt to evaluate the impact of each of the indi-vidual components of the change package. Because our goal was to improve maximally patient safety of inpa-tient children, rapid implementation of change package components relevant to individual sites rather than stressing compliance to specific components offered the best opportunity to do so. Fifth, this project was open only to children’s hospitals in the CHCA, which by def-inition are freestanding. These results therefore may not be applicable to pediatric inpatients in an adult hospital or a pediatric hospital within an adult hospital, poten-tially rendering our national estimates of effect inaccu-rate. Sixth, we did not formally evaluate the risks asso-ciated with implementing components of the change
package because of our belief that none of the interven-tions recommended was likely to cause harm. Finally, the baseline data collection period was short and thus potentially inaccurate in terms of true baseline collabo-rative-wide ADE burden. In an effort to increase the stability of the baseline period, we defined the baseline period a priori to be 4 months in duration. This short baseline was factored into the statistical analysis, the result being a statistically significant decrease in narcotic-related ADEs collaborative-wide with 95% confidence.
CONCLUSIONS
Narcotic-related ADEs in pediatrics are frequent, ex-pensive, and occasionally life-threatening or fatal. As part of a children’s hospital patient safety initiative, 14 freestanding children’s hospitals collaboratively im-plemented various interventions from an expert-con-structed change package of multiple interventions to decrease narcotic-related ADEs in hospitalized children. Coincident with these interventions, we saw a decrease in narcotic-related ADEs of 67% across the collaborative. Broad use of these interventions could significantly re-duce morbidity and the costs of care associated with narcotic-related ADEs in hospitalized children. Future studies to explore the implementation of these and sim-ilar interventions in pediatric inpatients who are cared for outside freestanding children’s hospitals is war-ranted.
ACKNOWLEDGMENTS
This study was funded by Agency for Healthcare Re-search and Quality grant 1 U18 HS013698-01.
We thank Stuart Levine, PharmD, Jane Taylor, EdD, Lloyd Provost, MS, Spence Byrum, Lee Flowers, Matt Hall, PhD, Jane Roessner, PhD, and Frank Davidoff, MD, for contributions to this collaborative effort resulting from participation on the expert panel (Levine, Taylor, Provost, Byrum, and Flowers), guidance with the statis-tical analysis (Hall), and thoughtful review of the draft manuscript (Roessner and Davidoff).
REFERENCES
1. Takata G, Mason W, Takatoma C, Logsdon T, Sharek PJ. De-velopment, testing, and findings of a pediatric-focused trigger tool to identify medication related harm in US children’s hos-pitals. Pediatrics. 2008;121(4). Available at: www.pediatrics. org/cgi/content/full/121/4/e927
TABLE 5 Automated Medication-Dispensing-Device Override Percentage Collaborative-Wide
Quarter Doses Dispensed per Month (n⫽10) Percent Overrides (n⫽10)
Median 25th Percentile
75th Percentile
Median 25th Percentile
75th Percentile
Pa
Baselineb 3003 1495 6309 10.18 6.75 22.19
1c 4129 2069 6793 6.78 5.99 19.70 ⬍.001
2 5039 2485 6602 6.79 4.77 11.54 ⬍.001
3 3773 2096 6981 4.97 4.44 12.39 ⬍.001
4 3236 2212 6869 5.91 4.83 14.14 ⬍.001
aReflects comparison between baseline and each quarter using Wilcoxon’s rank-sum test. bDecember 1, 2005, through March 31, 2005.
2. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001; 285(16):2114 –2120
3. Bates DW, Spell N, Cullen DJ, et. al. The costs of adverse drug events in hospitalized patients. Adverse Drug Events Preven-tion Study Group.JAMA.1997;277(4):307–311
4. HCUP Kids’ Inpatient Database (KID). Healthcare Cost and Utilization Project (HCUP). Rockville, MD: Agency for Health-care Research and Quality; 2003. Available at: www.hcup-us. ahrq.gov/kidoverview.jsp. Accessed March 20, 2008
5. Institute of Safe Medication Practices. ISMP’s list of high-alert med-ications. Available at: www.ismp.org/Tools/highalertmedmed-ications. pdf. Accessed March 20, 2008
6. Institute for Healthcare Improvement. 5 million lives cam-paign. Available at: www.ihi.org/IHI/Programs/Camcam-paign. Accessed March 20, 2008
7. Child Health Corporation of America.Pediatric Health Informa-tion System (PHIS) Database. Shawnee Mission, KS: Child Health Corporation of America; 2004
8. Leape LL, Kabcenell A, Berwick DM, Roessner J. Reducing Adverse Drug Events: Breakthrough Series Guide. Boston, MA: Institute for Healthcare Improvement; 1998
9. Overhage JM, Tierney WM, Zhou XH, et al. A randomized trial of corollary orders to prevent errors of omission.J Am Med Inform Assoc.1997;4(5):364 –375
10. Oren E, Shaffer ER, Guglielmo BJ. Characteristics of antimi-crobial overrides associated with automated dispensing ma-chines.Am J Health Syst Pharm.2002;59(15):1445–1448 11. Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The
100,000 lives campaign: setting a goal and a deadline for im-proving healthcare quality.JAMA.2006;295(3):324 –327 12. Joint Commission on Accreditation of Healthcare
Organiza-tions. National patient safety goals, 2005. Available at: www. jointcommission.org/PatientSafety/NationalPatientSafetyGoals/ 05㛭hap㛭npsgs.htm. Accessed March 20, 2008
13. Institute for Healthcare Improvement.The Breakthrough Series: IHI’s Collaborative Model for Achieving Breakthrough Improvement.
IHI Innovation Series White Paper. Boston, MA: Institute for Healthcare Improvement; 2003. Available at: www.ihi.org/IHI/ Results/WhitePapers/TheBreakthroughSeriesIHIsCollaborativeModel forAchieving⫹BreakthroughImprovement.htm. Accessed March 20, 2008
14. Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP.The
Improvement Guide: A Practical Approach to Enhancing Organiza-tional Performance. San Francisco, CA: Jossey-Bass Publishers; 1996
15. Institute for Healthcare Improvement. Going Lean in Health Care.IHI Innovation Series White Paper. Cambridge, MA: In-stitute for Healthcare Improvement; 2005. Available at: www. ihi.org/IHI/Results/WhitePapers/GoingLeaninHealthCare.htm. Accessed March 20, 2008
16. Printezis A, Gopalakrishnan M. Current pulse: can a produc-tion system reduce medical errors in health care?Qual Manag Health Care.2007;16:226 –238
17. Rozich JD, Haraden CR, Resar RK. Adverse drug event trigger tool: a practical methodology for measuring medication related harm.Qual Saf Health Care.2003;12(3):194 –200
18. Resar RK, Rozich JD, Classen DC. Methodology and rationale for the measurement of harm with trigger tools.Qual Saf Health Care.2003;12(suppl 2):ii39 –ii45
19. Resar RK, Rozich JD, Simmonds T, Haraden CR. A trigger tool to identify adverse events in the intensive care setting.J Comm J Qual Patient Saf.2006;32(10):585–590
20. Sharek PJ, Horbar JD, Mason W, et al. Adverse events in the neonatal intensive care unit: development, testing, and find-ings of a NICU-focused trigger tool to identify harm in North American NICUs.Pediatrics.2006;118(4):1332–1340
21. Institute for Healthcare Improvement.IHI Trigger Tool for Measur-ing Adverse Drug Events. IHI Innovation Series White Paper. Cam-bridge, MA: Institute for Healthcare Improvement; 2004. Avail-able at: www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/ Tools/Trigger%20Tool%20for%20Measuring%20Adverse%20Drug %20Events%20(IHI%20Tool). Accessed March 20, 2008
22. Classen DC, Pestotnik SL, Evans RS, Burke JP. Computerized surveillance of adverse drug events in hospital patients.JAMA.
1991;266(20):2847–2851
23. National Coordinating Council for Medication Error Report-ing and Prevention. Taxonomy of medication errors. Available at: www.nccmerp.org/pdf/indexColor2001-06-12.pdf. Accessed March 20, 2008
24. Little RA, Rubin DB.Statistical Analysis With Missing Data. New York, NY: Wiley Publishing; 1987
25. Kilo CM. Improving care through collaboration. Pediatrics.
DOI: 10.1542/peds.2008-1011
2008;122;e861
Pediatrics
and Frank Federico
Takata, Beverly Walti, Marla Tanski, Carla Nelson, Tina R. Logsdon, Cary Thurm
Paul J. Sharek, Richard E. McClead, Jr, Carol Taketomo, Joseph W. Luria, Glenn S.
Hospitals
An Intervention to Decrease Narcotic-Related Adverse Drug Events in Children's
Services
Updated Information &
http://pediatrics.aappublications.org/content/122/4/e861
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/122/4/e861#BIBL
This article cites 12 articles, 5 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/therapeutics_sub Therapeutics
sub
http://www.aappublications.org/cgi/collection/hematology:oncology_ Hematology/Oncology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2008-1011
2008;122;e861
Pediatrics
and Frank Federico
Takata, Beverly Walti, Marla Tanski, Carla Nelson, Tina R. Logsdon, Cary Thurm
Paul J. Sharek, Richard E. McClead, Jr, Carol Taketomo, Joseph W. Luria, Glenn S.
Hospitals
An Intervention to Decrease Narcotic-Related Adverse Drug Events in Children's
http://pediatrics.aappublications.org/content/122/4/e861
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.