Copyright © 2003, American Society for Microbiology. All Rights Reserved.
Detection of Enterococcal Surface Protein Gene (
esp
) and Amplified
Fragment Length Polymorphism Typing of Glycopeptide-Resistant
Enterococcus faecium
during Its Emergence in a Greek
Intensive Care Unit
C. Routsi,
1* E. Platsouka,
2R. J. L. Willems,
3M. J. M. Bonten,
4O. Paniara,
2G. Saroglou,
1and C. Roussos
1Department of Critical Care, Medical School of Athens University,1and Department of Clinical Microbiology,2
Evangelismos Hospital, Athens, Greece, and Diagnostic Laboratory for Infectious Diseases and Perinatal Screening, National Institute of Public Health and the Environment, Bilthoven,3
and Department of Internal Medicine, University Medical Center, Utrecht,4The Netherlands
Received 8 May 2003/Returned for modification 23 June 2003/Accepted 5 September 2003
The emergence of glycopeptide-resistantEnterococcus faecium (GREF) in a Greek intensive care unit was
studied by amplified fragment length polymorphism analysis and esp gene detection. Three GREF clones
harboring theespgene were recovered from 17 out of 21 patients, indicating the dissemination of genetically
homogenous and virulent strains of GREF.
Glycopeptide-resistant enterococci (GRE) have become in-creasingly important as a cause of hospital-acquired infections. By the year 2000, 25.9% of enterococci isolated from intensive care units (ICUs) in the United States were vancomycin resis-tant (3). Although first detected in France and England, GRE strains have not disseminated extensively in Europe, having an incidence of less than 3% (2, 13). However, the number of GRE-affected European hospitals is now increasing (2).
Previously considered low-virulence pathogens, enterococci can cause life-threatening infections. Traits that have been mentioned as potential virulence factors include antibiotic re-sistance determinants, a cytolytic toxin, gelatinase, an aggrega-tion substance, extracellular superoxide producaggrega-tion, and the enterococcal surface protein (Esp) (7, 14, 15). The enterococ-cal surface protein gene (esp), encoding a cell wall-associated peptide, was originally found in Enterococcus faecalis (14). Recently a variantespgene has been detected in glycopeptide-resistantEnterococcus faecium(GREF) strains from hospital outbreaks, while it was absent in all nonepidemic and animal isolates, suggesting that its presence is a marker of increased virulence (18).
In Greece, following the detection of an increasing propor-tion ofE. faeciumstrains in ICU patients (12), GREF infec-tions first emerged in February 1999 (11). During the next 30 months, we experienced a GREF outbreak with 21 ICU pa-tients infected. To control the spread of glycopeptide-resistant strains, we studied the characteristics of this outbreak, focusing on molecular typing with amplified fragment length polymor-phism (AFLP) analysis andespgene detection. AFLP analysis was used to investigate the genetic relationship among the
GREF strains, as this technique is fast, reproducible, and as discriminatory as pulsed-field gel electrophoresis for studying the molecular epidemiology of enterococci (1, 16, 17).
Identification and antibiotic susceptibility.Identification of
enterococci was performed by classic methods and PASCO identification panels. MICs of ampicillin, chloramphenicol, ciprofloxacin, gentamicin (500g/ml), streptomycin (1,000g/ ml), tetracycline, rifampin, teicoplanin, and vancomycin were determined by the broth microdilution method (PASCO sys-tem). The susceptibility testing was performed according to NCCLS guidelines (9).E. faecalis ATCC 29212 was used as quality control strain. The MICs of vancomycin and teicopla-nin were also determined by E test.
Molecular typing.The presence of thevanAgene and esp
gene was detected by PCR as proposed by Dutka-Malen et al. (6) and Shankar et al. (14), respectively. The expectedespPCR product size was 510 bp. AFLP analysis was performed as described by Willems et al. (17).
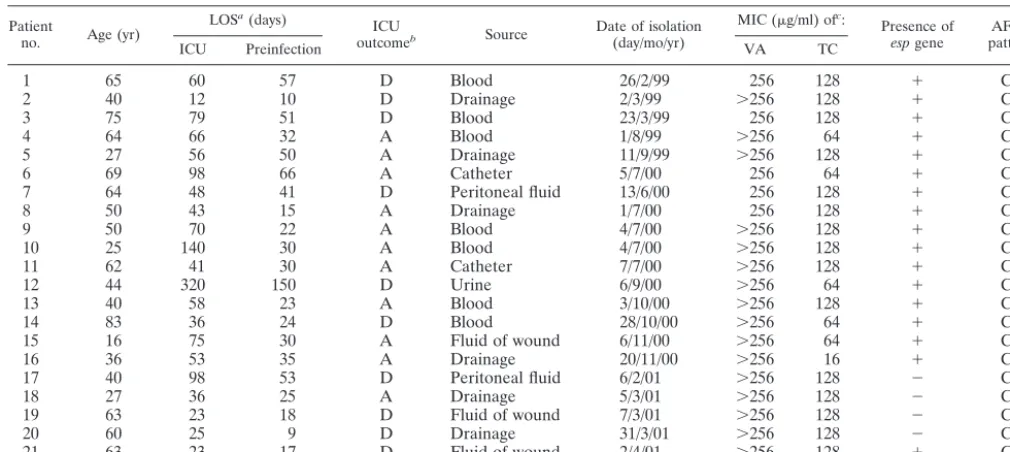
From February 1999 to April 2001, GREF strains were iso-lated from 21 medical and surgical patients in the multidisci-plinary ICU (Table 1). Characteristics of the patients and the GREF strains are shown in Table 1. Theespgene was present in 17 of the 21 strains. None of theesp-negative strains came from blood. GREF strains from patients 6, 8, 9, 10, and 11 were isolated in the same month and in the same ward of the ICU.
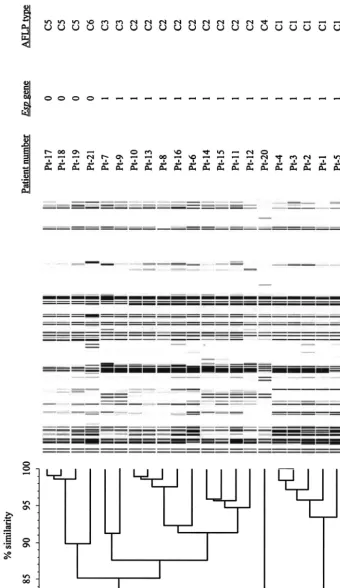
The genetic relationships, as determined by the AFLP band-ing patterns, are shown in Fig. 1. All strains formed a highly homologous group since AFLP banding patterns were at least for 80% similar. GREF isolates with a similarity of ⬎90% between AFLP patterns were considered identical (18). Based on these criteria six different AFLP types (clones C1 to C6) were discerned. AFLP types are shown in Table 1.
Figure 2 describes the relationship between the length of
* Corresponding author. Mailing address: Evangelismos Hospital, Critical Care Department, 45-47 Ipsilantou Str., Athens 106 75, Greece. Phone: 210 7243320. Fax: 210 7244941. E-mail: [email protected].
5742
on May 15, 2020 by guest
http://jcm.asm.org/
ICU stay for each patient, the preinfection period, the infec-tion period, and AFLP types during the study period. Isolates belonging to clones C2 and C3 were recovered during the same period of time. This and the fact that clones C2 and C3 are highly similar suggest that these isolates belong in fact to a single clone (C2/3). The same is probably true for the esp -negative isolates belonging to clones C5 and C6. In summary, these results show that, during the period February 1999 to April 2001, three different GREF clones (C1, C2/3, and C4) harboring theespvirulence gene were recovered from clinical sites, mainly blood, of 17 patients. In addition, one GREF clone (C5/6) lacking theespgene was isolated from peritoneal fluid, drainage, and wound fluid of four patients.
The predominance of the speciesE. faecium among GRE has been widely reported.vanA E. faeciumwas mainly respon-sible for the emergence and the dissemination of glycopeptide resistance in European hospitals (2), while in the United States, the GRE isolates show considerable diversity, with
vanBresistance also being a common type (4, 8).
All GREF strains isolated during July 2000, when the peak of the outbreak occurred, wereesppositive, which may indicate an increased virulence associated with the presence ofesp.Our findings seemingly contrast with the results of Shankar et al. (14), who found theespgene in 43 out of 133 infection-derived
E. faecalisisolates and did not find it in 34E. faeciumisolates, but they are in accordance with those of Willems et al. (18), who detected the gene in vancomycin-resistant E. faecium
strains associated with hospital outbreaks.
Theespgene has also been detected in glycopeptide-suscep-tibleE. faeciumstrains (5; L. Baldassari, L. Bertuccini, M. G.
Ammendolia, G. Gherardi, and R. Creti, Letter, Lancet357:
1802, 2001; N. Woodford, M. Soltani, and K. J. Hardy, Letter, Lancet358:584, 2001), supporting the hypothesis thatesp -pos-itiveE. faeciumstrains may have existed for some time, even before the acquisition of resistance to glycopeptides. We did not screen for esp gene-positive glycopeptide-susceptible E. faecium(GSEF) strains since it was not the rationale of this study. Therefore, we have no data on the frequency of esp -positive GSEF strains in our ICU.
In general, GRE isolates are genetically diverse (4), while single clones have also been reported in outbreaks on single hospital wards (10). However, the molecular epidemiology of GRE within an institution may change over time, going from an epidemic situation to the establishment of endemicity (8). In the present study, the transmission of a particular clone could be explained by the fact that infected patients stayed in the ICU during overlapping periods of time. Interestingly, the disappearance of one particular GREF clone was followed by the appearance of another. In addition the acquisition of GREF occurred 30 days (median value) after the ICU admis-sion. These findings strongly suggest intra-ICU transmission of GREF strains.
[image:2.603.41.546.81.307.2]In summary, genetically homogenous GREF strains harbor-ing the esp virulence gene were identified during the emer-gence and the evolving outbreak of GREF infections in our ICU. The results of this study emphasize the importance of molecular monitoring of GREF infections in understanding their epidemiology and may be useful to control and prevent their further spread.
TABLE 1. Characteristics of ICU patients and the isolatedvanAGREF strains
Patient
no. Age (yr)
LOSa(days)
ICU
outcomeb Source Date of isolation(day/mo/yr)
MIC (g/ml) ofc:
Presence of
espgene patternAFLP
ICU Preinfection VA TC
1 65 60 57 D Blood 26/2/99 256 128 ⫹ C1
2 40 12 10 D Drainage 2/3/99 ⬎256 128 ⫹ C1
3 75 79 51 D Blood 23/3/99 256 128 ⫹ C1
4 64 66 32 A Blood 1/8/99 ⬎256 64 ⫹ C1
5 27 56 50 A Drainage 11/9/99 ⬎256 128 ⫹ C1
6 69 98 66 A Catheter 5/7/00 256 64 ⫹ C2
7 64 48 41 D Peritoneal fluid 13/6/00 256 128 ⫹ C3
8 50 43 15 A Drainage 1/7/00 256 128 ⫹ C2
9 50 70 22 A Blood 4/7/00 ⬎256 128 ⫹ C3
10 25 140 30 A Blood 4/7/00 ⬎256 128 ⫹ C2
11 62 41 30 A Catheter 7/7/00 ⬎256 128 ⫹ C2
12 44 320 150 D Urine 6/9/00 ⬎256 64 ⫹ C2
13 40 58 23 A Blood 3/10/00 ⬎256 128 ⫹ C2
14 83 36 24 D Blood 28/10/00 ⬎256 64 ⫹ C2
15 16 75 30 A Fluid of wound 6/11/00 ⬎256 64 ⫹ C2
16 36 53 35 A Drainage 20/11/00 ⬎256 16 ⫹ C2
17 40 98 53 D Peritoneal fluid 6/2/01 ⬎256 128 ⫺ C5
18 27 36 25 A Drainage 5/3/01 ⬎256 128 ⫺ C5
19 63 23 18 D Fluid of wound 7/3/01 ⬎256 128 ⫺ C5
20 60 25 9 D Drainage 31/3/01 ⬎256 128 ⫺ C4
21 63 23 17 D Fluid of wound 2/4/01 ⬎256 128 ⫹ C6
aLOS, length of stay.
bD, dead; A, alive.
cVA, vancomycin; TC, teicoplanin.
on May 15, 2020 by guest
http://jcm.asm.org/
FIG.
1.
Dendrogram
of
the
genetic
similarity
of
all
isolates
by
AFLP
analysis.
AFLP
types
are
based
on
90%
genetic
similarity.
The
presence
(1)
or
absen
ce
(0)
of
the
esp
gene
is
indicated.
on May 15, 2020 by guest
http://jcm.asm.org/
[image:3.603.117.458.101.690.2]FIG.
2.
Admission
of
patients
at
the
ICU.
Bars
indicate
the
preinfection
period
(open
part)
and
infected
period
(solid
part).
The
numbers
on
the
left
ar
e
the
patient
numbers.
on May 15, 2020 by guest
http://jcm.asm.org/
REFERENCES
1. Antonishyn, N. A., R. R. McDonald, E. L. Chan, G. Horsman, C. E. Wood-mansee, P. S. Falk, and C. G. Mayhall.2000. Evaluation of fluorescence-based amplified fragment length polymorphism analysis for molecular typing in hospital epidemiology: comparison with pulsed-field gel electrophoresis
for typing strains of vancomycin-resistantEnterococcus faecium. J. Clin.
Microbiol.38:4058–4065.
2. Bonten, M. J. M., R. Willems, and R. A. Weinstein.2001. Vancomycin-resistant enterococci: why they are here, and where do they come from?
Lancet Infect. Dis.1:314–325.
3. Centers for Disease Control and Preventation.National nosocomial infec-tions surveillance (NNIS) system report, data summary from January 1990–
May 1999, issued June 1999. Am. J. Infect. Control27:520–532.
4. Clark, N. C., R. C. Cooksey, B. C. Hill, J. M. Swenson, and F. C. Tenover.
1993. Characterization of glycopeptide-resistant enterococci from U.S.
hos-pitals. Antimicrob Agents Chemother.37:2311–2317.
5. Coque, T. M., R. Willems, R. Canton, R. Del Campo, and F. Baquero.2002. High occurrence of esp among ampicillin-resistant and
vancomycin-suscep-tibleEnterococcus faeciumclones from hospitalized patients. J. Antimicrob.
Chemother.50:1035–1038.
6. Dutka-Malen, S., S. Evers, and P. Courvalin.1995. Detection of glycopep-tide resistance genotypes and identification to the species level of clinically
relevant enterococci by PCR. J. Clin. Microbiol.33:24–27.
7. Jett, B. D., M. M. Huycke, and M. S. Gilmon.1994. Virulence of enterococci.
Clin. Microbiol. Rev.7:462–478.
8. Kim, W. J., R. A. Weinstein, and M. Hayden.1999. The changing molecular epidemiology and establishment of endemicity of vancomycin resistance in
enterococci at one hospital over a 6-year period. J. Infect. Dis.179:163–171.
9. National Committee for Clinical Laboratory Standards.2000. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; 5th ed. Approved standard M7-A5. National Committee for Clinical Labo-ratory Standards, Wayne, Pa.
10. Pegues, D. A., C. F. Pegues, P. L. Hibbert, D. S. Ford, and D. C. Hooper.
1997. Emergence and dissemination of a highly vancomycin-resistantvanA
strain ofEnterococcus faeciumat a large teaching hospital. J. Clin. Microbiol.
35:1565–1570.
11. Platsouka, E. D., H. Dimopoulou, V. Miriagou, and O. Paniara.2000. The
first clinical isolates ofEnterococcus faeciumwith the VanA phenotype in a
tertiary Greek hospital. J. Antimicrob. Chemother.46:1039–1040.
12. Routsi, C., E. Platsouka, O. Paniara, E. Dimitriadou, G. Saroglou, C. Rous-sos, and A. Armaganidis.2000. Enterococcal infections in a Greek intensive
care unit: a 5-year study. Scand. J. Infect. Dis.32:275–280.
13. Schouten, M. A., A. Voss, and J. A. Hoogkamp-Korstanje.1999. Antimicro-bial susceptibility patterns of enterococci causing infections in Europe.
An-timicrob. Agents Chemother.43:2542–2546.
14. Shankar, V., A. S. Baghdayan, M. M. Huycke, G. Lindah, and M. S. Gilmore.
1999. Infection-derivedEnterococcus faecalisstrains are enriched inesp, a
gene encoding a novel surface protein. Infect. Immun.67:193–200.
15. Vergis, E. N., N. Shankar, J. W. Chow, M. K. Hayden, D. R. Snydman, M. J. Zervos, P. K. Linden, M. M. Wagener, and R. R. Muder.2002. Association between the presence of enterococcal virulence factors gelatinase, hemoly-sin, and enterococcal surface protein and mortality among patients with
bacteremia due toEnterococcus faecalis.Clin. Infect. Dis.35:570–575.
16. Vos, P., R. Hogers, M. Bleeker, M. Reijans, T. van de Lee, M. Hornes, A. Frijters, J. Pot, J. Peleman, M. Kuiper, et al.1995. AFLP: a new technique
for DNA fingerprinting. Nucleic Acids Res.23:4407–4414.
17. Willems, R. J. L., J. Top, N. van den Braak, A. van Belkum, H. Endtz, D. Mevious, E. Stobberingh, A. van den Bogaard, and J. D. A. van Embden.
2000. Host specificity of vancomycin-resistantEnterococcus faecium.J.
In-fect. Dis.182:816–823.
18. Willems, R. J. L., W. Homan, J. Top, M. van Santen-Verheuvel, D. Tribe, X. Manzioros, C. Gaillard, C. M. Vandenbroucke, E. M. Mascini, E. van Kregten, J. D. van Embden, and M. J. Bonten.2001. Variantespgene as a
marker of a distinct genetic lineage of vancomycin-resistantEnterococcus
faeciumspreading in hospitals. Lancet357:853–855.