The 2015 Cancer System
Performance Report
June 2015
1.
Prevention
Smoking
prevalence
Definition:Percentageofpopulationaged12yearsandolderineachspecifiedgroup–daily,occasional, formerorneversmokers
Numerator:Numberofdaily,occasional,former,orneversmokers,aged12yearsandolder
Denominator:Totalpopulationaged12yearsandolder
DataSource:CanadianCommunityHealthSurvey
Measurementtimeframe:2013
CCHSvariables:1.Inyourlifetime,haveyousmokedatotalof100ormorecigarettes(about4packs)? 2.Haveyoueversmokedawholecigarette?3.Atthepresenttime,doyousmokecigarettesdaily, occasionallyornotatall? 4.Haveyoueversmokedcigarettesdaily?
Stratificationvariables:Province/territory,Sex
Provinces/territorieswithdataavailable:AB,BC,MB,NB,NL,NS,NT,ON,PE,QC,SK,NU,YT
Notes:CCHSdataarebasedonarepresentativesamplewhichisthenextrapolatedtotheoverall population.
Human
papillomavirus
(HPV)
vaccination
Definition:Theproportionoffemalesinthetargetedcohorttoreceivethefirstof3dosesoftheHPV vaccination
Numerator:NumberoffemaleswhohavereceivedthefirstdoseoftheHPVvaccinationthroughthe provincially/territoriallyorganizedprogram
Denominator:Numberoffemalesinthetargetgrade/agegroupinschoolswheretheprovincialHPV vaccinationprogramhasbeenoffered.Itdoesnotnecessarilyrepresenttheentirefemalepopulation withinthetargetagerangefortheprovince.
DataSource:Pan‐CanadianCervicalScreeningNetwork,PrinceEdwardIslandChiefPublicHealth Office
Measurementtimeframe:2012/2013or2013/2014schoolyear,dependingontheprovinceandas indicatedinTable1.1(approximatelySeptember1sttoAugust31st)
Stratificationvariables:Province/territory
Provinces/territorieswithdataavailable:AB,BC,MB,NB,NL,NS,NT,ON,PE,QC,SK,NU,YT
Provincespecificnotes:NB:Dataarefor3rddoseofHPVvaccine.NT:Datareportedarebasedon estimates.ON:Dataarefor3rddoseofHPVvaccine.PE:Dataarefor3rddoseofHPVvaccine.
Generalnotes:1.Thetargetgradeandagegroupvariesbyprovince/territory;2.Itwasnotpossibleto collectstandardizeddatafromallprovincesandterritories.Provincialandterritorialprogramshave differenttargetpopulations,implementationplansandphasesforvaccination.Withbettercollection ofstandardizeddataandcontinuedroll‐outofHPVvaccination,itisexpectedthatthepercentages willincreaseandinter‐provincial/territorialvariationwilldecrease.
Physical
activity ‐
Active
transportation
Definition:Percentageofadultsaged18andolderwhoreportengaginginphysicalactivityaspartof transportationinthepast3months
Numerator:Numberofindividualsaged18andolderwhowalk/biketoschoolorworkinthepast3 months
DataSource:CanadianCommunityHealthSurvey
Measurementtimeframe:2013
CCHSvariables:1.Wasthereanytime*inthepast3monthswhenyouwalkedtoandfromworkor school?2. Wasthereanytime*inthepast3monthswhenyoubikedtoandfromworkorschool?
*Forthosewhoansweredyestowalkingorbikingforleisure,thebeginningofthequestionswere phrasedasfollows:1.Otherthanthe(X)timesyoualreadyreportedwalkingforexercisewasthereany othertime…";2.Otherthanthe(X)timesyoualreadyreportedbicyclingwasthereanyothertime…”
Stratificationvariables:Province/territory,agegroup
Provinces/territorieswithdataavailable:AB,BC,MB,NB,NL,NS,NT,ON,PE,QC,SK,NU,YT
Notes:CCHSdataarebasedonarepresentativesamplewhichisthenextrapolatedtotheoverall population.
2.
Screening
Cervical
cancer
screening:
self‐reported
Definition:Age‐standardized(2011standardpopulation)percentageofwomenaged18–69whohadat leastonePapanicolau(Pap)smearinthepast3years
Numerator:Totalnumberofwomenaged18–69reportinghavinghadatleastonePaptestinthepast3 years
Denominator:Totalnumberofwomenaged18–69(excludingwomenwhohavehadahysterectomy)
Datasource:CanadianCommunityHealthSurvey
Measurementtimeframe:2012,2013
CCHSvariables:1.HaveyoueverhadaPAPsmeartest?2.Whenwasthelasttime?3.Haveyouhada hysterectomy?
Stratificationvariables:Province/territory,householdincome,immigrationstatus
Provinces/territorieswithdataavailable:Allfor2012;NB,PE,NL,YT,NT,NUfor2013
Notes:1.CCHSdataisbasedonarepresentativesamplewhichisthenextrapolatedtotheoverall population.2.CervicalcancerscreeningwasoptionalcontentinCCHS2013.
Breast
cancer
screening:
self‐reported
Definition:Percentageofasymptomaticfemalesaged50‐69receivingamammogramwithinthepast 2years,whereasymptomaticisdefinedasrespondentswhoindicatedgoingforamammogramfor anyofthefollowingreasons:1.Familyhistory;Routinescreen/check‐up;2.Age;3.Hormone replacementtherapy(HRT).Mammogramsreceivedforanyofthefollowingreasonswereexcluded: lump;breastproblem;follow‐uptobreastcancertreatment;other.
Numerator:Asymptomaticfemalesaged50 ‐69whoindicatedgoingforamammogramwithinthe past2years
Denominator:Totalnumberofasymptomaticfemalesaged50 ‐69
Datasource:CanadianCommunityHealthSurvey
Measurementtimeframe:2012,2013
CCHSvariables:1.Haveyoueverhadamammogramthatis,abreastx‐ray?2.Whydidyouhaveit? (markallthatapply):familyhistory;partofregularcheck‐up/routinescreening;age;HRT;lump;follow‐
uptobreastcancertreatment;breastproblem;other;3.Whenwasthelasttime?
Stratificationvariables:Province/territory,householdincomequintile,immigrantstatus
Provinces/territorieswithdataavailable:Allprovincesandterritoriesfor2012;AB,NB,NS,NTfor 2013.
Notes:1.CCHSdataisbasedonarepresentativesamplewhichisthenextrapolatedtotheoverall population.2.BreastcancerscreeningwasoptionalcontentinCCHS2013.
Colorectal
cancer
screening:
self‐reported
Definition:Percentageofasymptomaticindividualsaged50 ‐74whoareup‐to‐datewiththeir
colorectalcancerscreening.Up‐to‐dateisdefinedashavinghadascreeningfecaltest(FOBT)inthepast 2yearsand/orsigmoidoscopy/colonoscopyinthepast5years,andasymptomaticisdefinedas
respondentswhoreportedhavingaCRCscreeningtestforanyofthefollowingreasons: familyhistory; regularcheck‐up/routinescreening;age;race.Colorectalscreeningreceivedforanyofthefollowing reasonswereexcluded:follow‐upofproblem;follow‐upofcolorectalcancertreatment;other.
Numerator:Numberofasymptomaticindividualsaged50 ‐74reportinghavinghadanFOBTwithinthe past2yearsand/oracolonoscopy/sigmoidoscopywithinthepast5years
Denominator:Totalnumberofasymptomaticindividualsaged50 ‐74
Datasource:CanadianCommunityHealthSurvey
CCHSvariables:1.HaveyoueverhadanFOBTtest?Whenwasthelasttime?Whydidyouhaveit?2. Haveyoueverhadacolonoscopyorsigmoidoscopy?Whenwasthelasttime?Whydidyouhaveit?
Measurementtimeframe:2012,2013
Stratificationvariables:Province/territory,agegroup,sex,householdincomequintile,immigrantstatus
Provinces/territorieswithdataavailable:Allprovincesandterritoriesfor2012;AB,MB,QC,NB,PE, NL,YT,NTfor2013
Notes: 1.CCHSdataisbasedonarepresentativesamplewhichisthenextrapolatedtotheoverall population.2.ColorectalcancerscreeningwasoptionalcontentinCCHS2013.
3.
Diagnosis
Breast
cancer
diagnosis
wait
time:
from
abnormal
breast
screen
to
resolution
Definition:1.Themedianand90thpercentileelapsedtime(inweeks)fromabnormalbreastscreento resolution(testdateofdefinitivediagnosis)2.Thepercentageofwomenforwhichtheabovewaittime waswithintargettimeframes
Population:Womenaged50–69participatingintheorganizedbreastscreeningprogramwithan abnormalbreastscreenresult(mammogramorclinicalbreastexamination);1.Requiringatissuebiopsy 2.Notrequiringatissuebiopsy
Datasource:Provincialbreastcancerscreeningprograms
Measurementtimeframe:2012
Datareported:BC,AB,SK,MB,ON,QC,NB,NS,PE,NL,NT
Provincespecificnotes:AB:WaittimedatawerebasedonthescreeningmammogramsdonebyScreen Test,whichispartofAlbertaBreastCancerScreeningPrograms(accountingforabout10%ofscreening mammogramsinAlberta).
SK:Participationrateincludedpatientswhohavehadbreastcancerinthepastwhoareallowedtore‐
screenwiththescreeningProgramforbreastcancer.
ON:Medianandpercentilearenotavailablefrom2009onward.
QC:Dataarenotavailablefor2004,2009and2011.
NT:2011waittimedataincludedonesite(Stanton)only.
Generalnotes:
1.Indicatorexcludestestsbeyond6monthspostscreen.
2.Timetodiagnosisisbasedonthedateofthefirstpathologicalbiopsyresultofbreastcancer (excludesfineneedleaspirationandallinconclusiveprocedures)orthedateofthelastbenigntestor pathologicalbiopsy.
3.Definitivediagnosisofcanceristhefirstcoreoropensurgicalbiopsythatconfirmscancer.Inrare occasions,fineneedleaspiration(FNA)biopsymayalsobeusedasadefinitivediagnosisofcancer. Definitivediagnosisofbenigncasesisthelastbenigntestupto6monthsfollowinganabnormalscreen. 4.Tissuebiopsyincludesopenandcoreneedlebiopsy.
Colorectal
cancer
diagnosis
wait
time:
from
abnormal
fecal
test
to
colonoscopy
Definition:Time(indays)betweenanabnormalcolorectalcancerscreeningfecaltestresultanda follow‐upscreeningcolonoscopyprocedure
Population:Individualswithanabnormalfecaltest(forCRCscreening)whowentontoreceivea colonoscopywithin180daysofthefecaltestresult
Measures:1.Median2.90thpercentile3.Numberofindividualshavingafollow‐upcolonoscopywithin 180days
DataSource:ReportedbytheprovincialcolorectalscreeningprogramsthroughtheNationalColorectal CancerScreeningNetwork
MeasurementTimeframe:First‐roundscreeningtestsconductedbetweenJanuary1,2011and December31,2012
DataReported:SK,MB,NS,NL,andPE
NL:Referralsforcolonoscopyoccuraftertheindividualhasbeencontactedbythescreeningprogram regardingtheabnormalfecaltestandahealthassessmentcompleted. Thismayinfluencemedianand 90thpercentileforwaittimefromabnormalfecaltesttofollow‐upcolonoscopy.
PE:FTgwasdiscontinuedbyJuneof2012aftertransitiontoFTi. FTiwasimplementedinearly2012.
GeneralNotes:
1.Thisindicatordoesnotincludepatientswhoreceivedacolonoscopymorethan6monthsfollowing anabnormalfecaltest.
2.ThecolonoscopymayhavebeenperformedinsideoroutsidetheProgrambutonlyincludesindividuals whoseabnormalfecaltestwasperformedinthescreeningProgram.
Use
of
PET
scans
among
patients
diagnosed
with
non‐small
cell
lung
cancer
Definition:Percentageofpatientsdiagnosedasnon‐smallcelllungcancer(NSCLC),receivingatleast onePETscanwithinthreemonthsbeforeanduptooneyearafterdiagnosis
Numerator:Numberofpatientswhodiagnosedasnon‐smallcelllungcancerandreceivedatleastone PETscanwiththreemonthsbeforeanduptooneyearafterdiagnosis
Denominator:Numberofpatientswhowerediagnosedasnon‐smallcelllungcancer
Datasources:Provincialcanceragencies
Measurementtimeframe:2009to2011diagnosisyear
Stratificationvariables:province,sex,agegroupandcancerstage
Provincessubmittingdata:BC,AB,MB,ON,NB,NS
Provincespecificnotes:
BC:DatawereonlyforNSCLCpatientsdiagnosedin2010and2011,sincestagedatawerenotavailable for2009.Datamaynotbecompleteandcomparablewithotherprovincesduetolackofinformation aboutsurgeryforthediagnosisyears2010and2011,whichwereusedtodeterminethetreatment modality.CaseswithStageIIIdiseasewerestagedupwardtoStageIIIA.
AB:Theclassificationofcancerstagefor2009werebasedonAJCC6th,for2010and2011werebased onAJCC7th.CaseswithDeathCertificateOnly(DCO)orconfirmedbyautopsyonlywereexcluded. CaseswithstageIIIwerecategorizedasstageIIIB.
MB:CaseswithstageIIIwerecategorizedasstageIIIB.
NS: CaseswithstageIIIwerecategorizedasstageIIIB.
Generalnotes:
1.Datawerecollectedbytreatmentmodalityandstage.Resultsfromtreatmentmodalitywere combinedforreporting. Provinceswithnotreatmentdataavailable(i.e.BCandNB)werepartially excludedfromtheanalysis.
2.InvasiveNon‐SmallCellLungcancer(NSCLC)incidencecasesweredefinedasC34withbehaviorcode 3,excludinghematopoietichistology(M‐95toM‐98),smallcell,neuroendocrinecarcinomaandsarcoma codesusingInternationalClassificationofDiseasesforOncology,ThirdEdition(ICD‐O‐3).
3.Onlypatientswithageatdiagnosis>=18wereincluded,whoweredividedtotwogroups:18‐69and 70+.
4.IncidencecasesthroughDeathCertificateonly(DCO)wereexcluded.
5.Treatmentmodalitywasclassifiedintothreegroups:firstsurgery,firstradiationtherapyandnoany treatment.
Distribution
of
diagnostic
PET
scans
by
stage
for
non‐small
cell
lung
cancer
cases
Definition:PercentageofdiagnosticPETscanbystagefornon‐smallcelllungcancercases(NSCLC).
Numerator:NumberofdiagnosticPETscanfornon‐smallcelllungcancercasesforaspecificstage.
Datasources:Provincialcanceragencies
Measurementtimeframe:2009to2011diagnosisyear
Stratificationvariables:province,sex,agegroupandcancerstage
Provincessubmittingdata:BC,AB,MB,ON,NB,NS
Provincespecificnotes:
BC:DatawereonlyforNSCLCcasesdiagnosedin20010and2011,sincestagedatawasnotavailablefor 2009.Datamaynotbecompleteandcomparablewithotherprovincesduetolackofinformationabout surgeryforthediagnosisyears2010and2011,whichwereusedtodetermineifPETscanswerefor diagnosis.CaseswithStageIIIdiseasewerestagedupwardtoStageIIIA.
AB:Theclassificationofcancerstagefor2009werebasedonAJCC6th,for2010and2011werebasedon
AJCC7th.CaseswithDeathCertificateOnly(DCO)orconfirmedbyautopsyonlywereexcluded.Cases
withstageIIIwerecategorizedasstageIIIB.
MB:CaseswithstageIIIwerecategorizedasstageIIIB.
NS: CaseswithstageIIIwerecategorizedasstageIIIB.
NB: Datawerenotcompleteandcomparableduetolackofradiationtherapyinformationforthe diagnosisyears,whichwereusedtodetermineifPETscanswerefordiagnosis.
Generalnotes:
1.Datawerecollectedbytreatmentmodalityandstage.Resultsfromtreatmentmodalitywere combinedforreporting. Provinceswithnotreatmentdataavailable(i.e.BCandNB)werepartially excludedfromtheanalysis.
2.InvasiveNon‐SmallCellLungcancer(NSCLC)incidencecasesweredefinedasC34withbehaviorcode 3,excludinghematopoietichistology(M‐95toM‐98),smallcell,neuroendocrinecarcinomaandsarcoma codesusingInternationalClassificationofDiseasesforOncology,ThirdEdition(ICD‐O‐3).
3.Onlypatientswithageatdiagnosis>=18wereincluded,whoweredividedtotwogroups:18‐69and 70+.
4.IncidencecasesthroughDeathCertificateonly(DCO)wereexcluded.
5.DiagnosticPETscanswasdeterminedbythedateinwhichPETscansoccurredandthefirstdateof surgeryand/orradiationtherapy.ThereweretwoscenariostodetermineifPETscanswerefor diagnosticpurpose:
a. Forthecases,therewerenosurgeryorradiationtherapywithinoneyearofdiagnosis,any PETscanshappenedbetween3monthspre‐diagnosisand4monthspostdiagnosiswere consideredasdiagnostic.
b. Forthecases,thereweresurgeryorradiationtherapywithinoneyearofdiagnosis,anyPET scanshappenedbetween3monthspre‐diagnosisandthefirstsurgeryorthefirstradiation therapywereconsideredasdiagnostic.
4.
Treatment
4.1 Surgery
Removal
and
examination
of
12
or
more
lymph
nodes
in
colon
resections
Definition:Theproportionofcoloncancerresectionsforwhich12ormorelymphnodeswereremoved andexamined
Numerator:Coloncancercasesdiagnosedduringtheyearandresectedwithin1yearofdiagnosisfor which12ormorelymphnodeswereremovedandexamined
Denominator:Allcoloncancercasesdiagnosedintheprovinceduringtheyearandresectedwithin12 monthsofdiagnosis
Datasource:Provincialcanceragencies
Measurementtimeframe:2008,2009,2010and2011diagnosisyears
Stratificationvariables:Province,agegroup,sex
Provincessubmittingdata:AB,SK,MB,ON,NB,NS,PE,NL
Provincespecificnotes:AB:For2011,treatmentinformationisbasedoninitiallyplannedtreatmentto primarysite(ACRdata). ExcludesC18.1Appendix. CCIcodesarenotidentifiedintheACR,assuchall codedsurgerieswereincludedforcompletecolonresection. Ifmorethanonesurgicalprocedureis performed;themostdefinitiveprocedureisdocumented.Thedefinitionofdefinitiveisthesurgical procedurewiththeintenttocure. Throughqualityassurance,wenoticedthatanumberofthecases codedassurgeryontheACRhadCCIcodesorBillingcodesotherthantheoneslisted. Themajorityof thesecasesappeartobecasesinwhichthebillingdatabasehad60.5otherresectionoftherectumeven thoughthepatientonlyhadC18.7sigmoidcolon. However,therearealsosomecasesinwhichtheACR codessurgeryforpolypectomyandhencethesehavealsobeenincluded. ON: CasesforAppendix C18.1wereexcluded.NS:For2011,collaborativestagevariableusedtoidentifythosehavinga resection.Resectionsdatesmanuallyreviewedfromchartreview.PE:For2011,casesforAppendix C18.1wereexcluded.
Generalnotes:
1. Caseswithunknownnumberofnodesremovedandexaminedwereexcludedfromboth numeratoranddenominator.
2. Casesforpatientsunder18yearsofage(atdiagnosis)wereexcluded. 3. ColoncasesdefinedasICDO3codes:C18.0toC18.9withbehaviorcode3.
4. ExcludelymphomaCodesM‐95toM‐98.From2010onwarddataalsoexcludesarcomacodes, neuroendocrinecarcinoma,squamouscellcarcinoma.
5. ColonresectionsidentifiedasCCIcodes:1NM87or1NM89or1NM91ordescriptorslistedinTable 1.
6. Allresectedcaseswereincluded,regardlessofmarginstatus(duetodatalimitations). 7. Includedcaseswhichlastresectiondate(ifmultiple)–diagnosisdate<=365days.
Breast
cancer
resections
that
are
mastectomies
Definition:Thepercentageofsurgicalresectionsamongwomenwithunilateralinvasivebreastcancer thataremastectomies.
Numerator:Womeninthedenominatorwhoreceivedamastectomyfirstaswellaswomenwho receivedbreastconservingsurgery(BCS)firstfollowedbyamastectomywithinoneyear
Denominator:Womenwithunilateralinvasivebreastcancerwhoreceivedbreastconservingsurgery and/oramastectomy
Datasource:HospitalMorbidityDatabase,CanadianInstituteforHealthInformation(CIHI);National AmbulatoryCareReportingSystem,CIHI;FichierdeshospitalisationsMED‐ÉCHO,ministèredela Santé etdesServices sociauxduQuébec;AlbertaAmbulatoryCareReporting System,AlbertaHealthand Wellness
Measurementtimeframe:2007‐08to2011‐12
Stratificationvariables:Province/territory
Provincessubmittingdata:BC,AB,SK,MB,ON,QC,NB,NS,PE,NLandTerritories
Generalnotes:
1.Thefollowingsurgicalanddiagnostic codes,asdocumentedinhospitalpatientrecordsandreported toCIHI,wereusedtoidentifydiagnosesandproceduresperthefollowing:
a. Inordertoidentifyabreastcancerdiagnosis,thefollowingICD‐10‐CAcodeswereused: C50.00, C50.01,C50.09,C50.10,C50.11,C50.19,C50.20,C50.21,C50.29,C50.30,C50.31,C50.39,C50.40, C50.41,C50.49,C50.50,C50.51,C50.59,C50.60,C50.61,C50.69,C50.80,C50.81,C50.89,C50.90, C50.91,C50.99.Womenwithunilateralinvasivebreastcancerwerethefocusofthisanalysis (comprising98%ofwomenwithinvasivebreastcancer).
b. Inordertoidentifyamastectomy,thefollowingsurgicalcodeswereusedaccordingtoCCI: 1.YM.89to1.YM.92.
c. ThefollowingCCIcodeswereusedtoidentifyabreastconservingsurgery: 1.YM.87,1.YM.88.
4.2 Radiation Therapy
Radiation
therapy
wait
time:
from
ready‐to‐treat
to
start
of
treatment
Definition:1.Themedianand90thpercentileelapsedtimefromreadytotreattostartofradiation therapy,measuredindays;2.Thepercentageofradiationtherapycasesforwhichtheabovewaittime waswithintargettimeframes
Datasource:Provincialcanceragencies
Measurementtimeframe:2013treatmentyear
Stratificationvariables:Province,bydiseasesite(allcancers,breast,colorectal,lung,prostate)
Provincessubmittingdata:BC,AB,SK,MB,ON,NB,NS,PE,NL
Provincespecificnotes:AB:For2013,dataincludedallcaseswhohadradiationtherapyataCancer ControlAlbertaFacilitywiththeirfirsttreatmentbetweenJan1,2013 ‐Dec31,2013;itincludesthose whowerelivinginanotherprovinceattimeofdiagnosisbutreceivingradiationtherapyinAlberta. Tumorgroupclassificationforthisindicatorisbasedonreferraltumorgroups. SK: For2013,data werereportedbytreatmentsite,anyRTtreatmentmodalitywasincluded. NS:For2013,waittime werecomputedusingthesamerulesforproducingwaittimeforNSDepartmentofHealthandWellness. Assuch,waittimewerebasedonpatientfirstcoursesoftreatmentintheperiodofinterest. PE:For 2013,datawerebasedonnewtreatmentstartswithinthetimeframeof2013.Individualcancerpatients couldhavemorethanonetreatmentstartinthetimeframeandcouldthereforebecountedmorethan once.
Generalnotes:
1.Allbehaviorcodesareincluded.
2.Caseswithtreatmentdonein2013areincluded.
3.Toidentifybreast,colorectal,lung,prostatecancerandallcancers,pleaseincludethemorphology codesthatarecurrentlyusedwithinyourregistry.
4.Ofnoteforbreastcancerdata,iftheprovinceobtainsthisdatafromawaittimedatabaseas opposedtoaregistry,thenbreastcancercasesweretobeincludedperthedatabasedefinition. 5.Thereareknowndiscrepanciesinthewaysinwhichdifferentprovincesmeasurewaittimes.Oneof thekeysourcesofvariationisthewaythe“ReadytoTreat”timeframeisdefined.Effortsareunderway tostandardizethesedefinitions.Thefollowingsectionoutlinesthedefinitionsusedbythedifferent provinces.
Provincialdefinitions:
AB:Thedatewhenthepatientisphysicallyreadytocommencetreatment.BC:Thedateatwhichboth oncologistandpatientagreethattreatmentcancommence.Beingreadytotreatrequiresthatall diagnostictestsandproceduresrequiredtoassesstheappropriatenessof,indicationsfor,andfitness toundergoradiationtherapyarecomplete.MB:Thedatewhenadecisionhasbeenmadebythe radiationoncologistandisagreedtobythepatientthatradiationtherapyisappropriateandshould commenceANDthepatientismedicallyreadytostarttreatmentANDthepatientiswillingtostart treatment.NB:Thedatewhenanyplanneddelayisoverandthepatientisreadytobegintreatment frombothasocial/personalandmedicalperspective.NL:Thedatewhenallpre‐treatment
investigationsandanyplanneddelayareover,andthepatientisreadytobeginthetreatmentprocess frombothasocial/personalandmedicalperspective.NS:Thedatewhenallpre‐treatment
investigationsandanyplanneddelayareover,andthepatientisreadytobeginthetreatmentprocess frombothasocial/personalandmedicalperspective.NovaScotiadidnothaveareadytotreatdate untilFebruary2010;aproxydatewasusedpriortothistime.ON:Thetimefromwhenthespecialistis confidentthatthepatientisreadytobegintreatmenttothetimethepatientreceivestreatment.PE:
Thedatewhenallpre‐treatmentinvestigationsandanyplanneddelayareover,andthepatientis readytobeginthetreatmentprocessfrombothasocial/personalandmedicalperspective.QC:At consultation,theradiationoncologistentersthedateatwhichthepatientwillbereadytotreatona formularyrequestingtreatment.SK:Thedatewhenthepatientisreadytoreceivetreatment,taking intoaccountclinicalfactorsandpatientpreference.Inthecaseofradiationtherapy,anypreparatory activities(e.g.,simulation,treatmentplanning,dentalwork)donotdelaythereadytotreatdate.
Pre‐operative
radiation
therapy
for
stage
II
or
III
rectal
cancer
patients
Definition:PercentageofresectedstageIIandIIIrectalcancercasesreceivingpre‐operative(neo‐
adjuvant)radiationtherapy
Numerator:StageIIandIIIrectalcancercasesdiagnosedduringtheyearreceivingpre‐operative radiationtherapyupto120daysbeforeresection
Denominator:StageIIandIIIrectalcancercasesdiagnosedintheprovinceduringtheyearandhavinga rectalresectionwithinoneyearofdiagnosis
Datasource:Provincialcanceragencies
Measurementtimeframe:2008,2009,2010and2011diagnosisyear
Stratificationvariables:Province,agegroup,sex
Provincespecificnotes:AB:For2011,treatmentinformationwasbasedoninitiallyplannedtreatment toprimarysite.CCIcodesarenotidentifiedintheACR,assuchallcodedsurgerieswereincludedfor completerectumresection.Ifmorethanonesurgicalprocedureisperformed,theACRcodesthemost definitiveproceduresisdocumented.Thedefinitionofdefinitiveisthesurgicalprocedurewiththe intenttocure.Caseswithradiationtherapyaftersurgerywereexcluded.
Generalnotes:
1.RectalcasesdefinedasICDO3codes:C19.9orC20.9,excludelymphomacodes(M‐95toM‐98).2010 dataalsoexcludesarcomacodes–8800/3,neuroendocrinecarcinomaandsquamouscellcarcinoma. 2.IncludedAJCCGroupStageatDiagnosis=IIorIII.
3.Casesforpatientsunder18yearsofage(atdiagnosis)wereexcluded.
4.RectalresectionsdefinedasCCIcodes1NQ59or1NQ87or1NQ89orseelistofdescriptorslistedin Table2.
5.Allresectedcaseswereincludedregardlessofmarginstatus(duetodatalimitations).
6.Includedcaseswhich1stresectiondate(ifmultiple)–diagnosisdate<=365days.1st resectiondate–
radiationtherapystartdate<=120days.
4.3 Systemic
Therapy
Post‐operative
chemotherapy
for
stage
II
or
IIIA
non‐small
cell
lung
cancer
patients
Definition:PercentageofstageIIandIIIAnon‐smallcelllungcancercasesreceivingchemotherapy followingsurgicalresection
Numerator:StageIIandIIIAnon‐smallcelllungcancercasesdiagnosedduringtheyear,resected withinoneyearofdiagnosisandstartingadjuvantchemotherapywithin120daysofsurgery
Denominator:StageIIandIIIAnon‐smallcelllungcancercasesdiagnosedintheprovinceduringthe yearandhavingalungresectionwithinoneyearofdiagnosis
Datasource:Provincialcanceragencies
Measurementtimeframe:2009,2010and2011diagnosisyears
Stratificationvariables:Province,agegroup,sex
Provincessubmittingdata:AB,SK,MB,ON,NS,PE
Provincespecificnotes:AB: For2011,Treatmentinformationisbasedoninitiallyplannedtreatmentto theprimarysite(ACRdata).CCIcodesarenotidentifiedintheACR,assuchallcodedsurgerieswere includedforcompletelungresection.Ifmorethanonesurgicalprocedureisperformed;themost definitiveprocedureisdocumented.Thedefinitionofdefinitiveisthesurgicalprocedurewiththeintent tocure.SCCwereexcluded. Allcodedsurgerieswereincludedascompletelungresection. SK:Data includedSCCin2011. NS:For2011,collaborativestagevariableswereusedtoidentifythosehaving resections.Individualchartwerereviewedtoobtainresectiondate.PE:For2011,dataincluded squamouscellcarcinomacases.
Generalnotes:
1.Casesforpatientsunder18yearsofage(atdiagnosis)wereexcluded.
2.Non‐smallcelllungcasesweredefinedasC34.0toC34.9,withbehaviorcode3,usingInternational ClassificationofDiseasesofOncology,ThirdEdition(ICD‐O‐3).HistologycodesforlymphomaM‐95to M‐98,andhistologycodesforsmallcell:8002,8041,8043,8044,8045,8073and8803wereexcluded.
3.For2010,dataexcludedsarcomacodes,neuroendocrinecarcinoma,andsquamouscellcarcinoma.For 2011,dataexcludedsarcomacodes,neuroendocrinecarcinoma.
4.IncludedAJCCGroupStageIIandIIIAatDiagnosis.
5.ResectionsdefinedasCCIcodes:1GR87,1GR89,1GR91,1GT59,1GT87,1GT89or1GT91ordescriptors listedinTable2below.
6.Allresectedcasesareincludedregardlessofmarginstatus(duetodatalimitations).
7.IncludedcaseswhichLastresectiondate(ifmultiple)–diagnosisdate<=365days.Chemotherapystart date–lastresectiondate(ifmultiple)<=120days.
8.Chemotherapyincludesoral(asavailableindata)andIVchemotherapy.
9.Nofilterfortreatmentintentwasused,unlessotherwisespecifiedbyprovince.
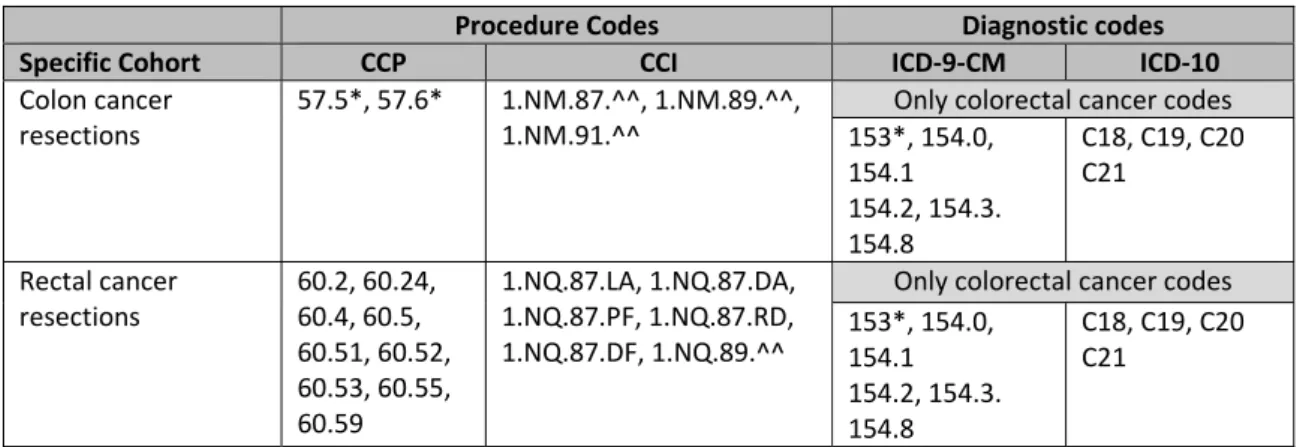
Table1:ProcedureCodes
Procedure Codes Diagnostic codes
Specific Cohort CCP CCI ICD‐9‐CM ICD‐10
Coloncancer 57.5*,57.6* 1.NM.87.^^,1.NM.89.^^, Onlycolorectalcancercodes
resections 1.NM.91.^^ 153*,154.0, 154.1 154.2,154.3. 154.8 C18,C19,C20 C21 Rectalcancer resections 60.2,60.24, 60.4,60.5, 60.51,60.52, 60.53,60.55, 60.59 1.NQ.87.LA,1.NQ.87.DA, 1.NQ.87.PF,1.NQ.87.RD, 1.NQ.87.DF,1.NQ.89.^^
Onlycolorectalcancercodes
153*,154.0, 154.1 154.2,154.3. 154.8 C18,C19,C20 C21
Table2:ClinicalDescriptors
ClinicaldescriptorsforColonCancer ClinicaldescriptorsforRectalCancer
righthemicolectomy, lefthemicolectomy segmentalcolectomy partialcolectomy transversecolectomy subtotalcoloectomy
anteriorresection(noteoverlapwithrectal cancerbelow)
anteriorresection(overlapwithcoloncancer above)
lowanteriorresection abdominoperinealresection segmentalresectionrectum Harmannprocedure totalproctectomy
5.
Person Centred‐Perspective
Screening
for
distress
Definition:Extenttowhichprovincesandtheircancerprogramshaveimplementedstandardizedtools toscreenforpatient‐reportedsymptomssuchasemotionalandphysicaldistress(includingpain)
ExtentofImplementation:1.Provincewideimplementation*standardizedsymptomscreening undertakenforatleastaportionofpatientsateachprovincialcancercentreanddatacollected centrally;2.Partialimplementation*standardizedsymptomscreeningundertakenforatleastaportion ofpatientsatselectedprovincialcancercentres;3.Notprovinciallycoordinated(somelocaluse possible)*provinciallymanagedimplementationofsymptomscreeningdoesnotexist;however,some individualcentres/regionsmayuseascreeningtoolbutdonotreportdataataprovinciallevel
Measurementtimeframe:2007,2014
Datasource:Provincialcanceragenciesandprograms
6.
Research
Adult
clinical
trial
participation
Definition:Theratioofthetotalnumberofallpatients(≥19years)newlyenrolledincancer‐related therapeutictrialsorclinicalresearchstudiesin2013totheprojectednumberofnewcancercases(all ages)in2013
Numerator:Numberofcancerpatients(≥19years)newlyenrolledincancer‐relatedtherapeuticclinical trialsorclinicalresearchatprovincialcancercentresin2013.Forpatientenrolledinmultipleclinical trials,countalloccurrences.
Denominator:Projectednumberofnewinvasivecancercases(allages)in2013.
Datasource:NumeratorswerereportedbyprovincialcanceragenciesorequivalenttotheCanadian PartnershipAgainstCancer.Denominatorswereretrievedfrom“CanadianCancerStatistics2013”– StatisticsCanada.
Measurementtimeframe:2013
Stratificationvariables:Province,diseasesite:1.Allinvasivecancers2.Breast3.Colorectal4.Lung;5. Prostate
Provincessubmittingdata:Allinvasivecancers:BC,AB,SK,MB,ON,NB,NS,PE,NL.
Bycancertype:BC,AB,SK,MB,NB,NS,PE,NL.
Provincespecificnotes:AB:For2013,thetotalnumberofaccrualsforcancerpatients(>=19years) includednewlyenrolledincancerrelatedtherapeutictrialsorclinicalresearchwhowereonthe AlbertaCancerClinicalTrials(ACCT)database. Ifapatientwentonmultipleclinicaltrialaccrualsinthe givenyear,apatientwouldbecountedforeachaccrual.TheACCTdatabasealsoincludespatientswho werelivingoutsideofAlberta,aslongastheywereonaclinicaltrialinAlberta.TheACCTdatabase includesbothfemalesandmalesintheBreastTumorGroupandmayincludeclinicaltrialsfornon‐
melanomaskinpatients.
Generalnote:
7.
Appropriateness
Breast
cancer
screening
within
and
outside
recommended
guidelines
Definition:Percentageofasymptomaticfemalesaged35+receivingamammogramwithinthepast2 years,whereasymptomaticisdefinedas:Respondentswhoindicatedgoingforamammogramforany ofthefollowingreasons:Familyhistory;Routinescreen/check‐up;Age;HRT;andNOTforanyofthe followingreasons:Lump;Breastproblem;Follow‐uptobreastcancertreatment;Other.
Numerator:Asymptomaticfemalesaged35+whoindicatedgoingforamammogramwithinthepast2 years
Denominator:Totalnumberofasymptomaticfemalesaged35+receivingamammogramwithinthe past2years
Datasource:CanadianCommunityHealthSurvey
CCHSVariable:1.Everhadamammogram;2.Reasonsforhavingmammogram(markallthatapply): Familyhistory;Routinescreen;Age;HRT;Lump;Follow‐uptobreastcancertreatment;Breastproblem; Other;3.Lasttimerespondenthadundergoneamammogram
Measurementtimeframe:2012
Stratificationvariables:Province/territory
Provincessubmittingdata:Allprovincesandterritories
GeneralNotes:CCHSdataarebasedonarepresentativesamplewhichisthenextrapolatedtothe overallpopulation.
Breast
cancer
mastectomies
performed
as
day
surgery
Definition:Percentageofbreastcancermastectomiesdoneasdaysurgeries,byprovince/territory
Numerator:Mastectomiesperformedasdaysurgery
Denominator:Totalmastectomies
Exclusion:Potentialduplicaterecordsareremovedfromtheanalysis.Potentialduplicaterecordsare identifiedasdischargeswithidenticalvaluesinthefollowingdataelements:
1.ForHMDB:Institution,healthcardnumber,admissiondate,admissiontime,dischargedate,discharge time,healthcardprovince3,birthdate,gender,postalcode,MRDx/mainproblem,principalCCI/main intervention
2.ForAlbertaAmbulatoryCaredata:INSTHEALTH_CARD_ENCRYPT_NUMSTDATESTHOURENDDATE
ENDHOURDOBSEXPOSTCODEMDIAGMINT
3.InvalidHealthCardNumber(“000000000000”). 4.HealthCardProvinceCode=’CA’.
5.Invalidpostalcode.
6.Procedurescodedasabandoned.
7.Newborns,stillbirthsandcadavericdonors. 8.Invalidepisodedate(i.e.,01JAN9999).
Datasource:HospitalMorbidityDatabase,NationalAmbulatoryCareReportingSystem,Canadian InstituteforHealthInformation;AlbertaAmbulatoryCareReportingSystem,AlbertaHealthand Wellness
Measurementtimeframe:2007/08to2011/12combinedfiscalyears
Stratificationvariables:Province/territory
Provincessubmittingdata:AllprovincesandTerritories
recordcontainingthesurgicalepisodeassociatedwiththepatient’sfirstbreastresectionareconsidered mastectomycases
8.
Long‐Term Outcomes
Age‐standardized
incidence
rates
Definition:Theincidenceratethatwouldhaveoccurrediftheagedistributioninthepopulationof interestwasthesameasthatofthestandard,whereincidencerateisdefinedasthenumberofcases ofcancer(malignantneoplasms)newlydiagnosedduringayear,per100,000peopleatrisk
Numerator:Numberofnewcancercases(allages):1.Breast(female)2.Colorectal3.Lung4.Prostate (male)5.Pancreas
Denominator:1.Annualfemalepopulationestimateinhundredsofthousands;2,3,5.Annual populationestimatesinhundredsofthousands4.Annualmalepopulationestimateinhundredsof thousands
Agestandardization:Directmethodusingthe2011CanadianCensuspopulation
Datasources:CanadianCancerRegistry(CCR)Database–cancerincidencedata;DemographyDivision ofStatisticsCanada–populationestimates
Measurementtimeframe:Foroveralltrends,Canada–1992to2010.Byprovince:3‐yearcombined (2008–2010)
Stratificationvariables:Province,sex
Generalnotes:
1.WorldHealthOrganization,InternationalClassificationofDiseasesforOncology,ThirdEdition(ICD‐
O‐3)andtheInternationalAgencyforResearchonCancer(IARC)rulesfordeterminingmultiple primariessiteswereused:colorectal(ICD‐O‐3:C18.0toC18.9,C19.9,C20.9,C26.0),lungandbronchus (ICD‐O‐3:C34.0toC34.9),femalebreast(ICD‐O‐3:C50.0toC50.9),prostate(ICD‐O‐3:C61.9),pancreas (ICD‐O‐3:C25.0‐C25.9)
2.JoinpointRegressionProgram4.1.1forWindowswasusedtoanalyzelineartrendsacrossyears. The softwaretakestrenddataandfitsthesimplestjoinpointmodelthatthedataallow. Theprogramstarts withtheminimumnumberofjoinpoints(e.g.0joinpoints,whichisastraightline)andtestswhether morejoinpointsarestatisticallysignificantandmustbeaddedtothemodel(uptothatmaximum number).Thisenablestheusertotestwhetheranapparentchangeintrendisstatisticallysignificant. ThetestsofsignificanceuseaMonteCarloPermutationmethod. AnnualPercentChange(APC)was reportedtocharacterizetrendsincancerratesovertime. APCassumesthatcancerratesarechanging ataconstantpercentageoftherateofthepreviousyear. Theminimumandmaximumnumberof joinpointsusedinthisanalysiswere0and4respectively. Forfurtherdetails,refertotheJoinpoint RegressionProgramdocumentation(http://surveillance.cancer.gov/joinpoint/).
Age‐standardized
incidence
rates
by
stage
Definition:Thestage‐specificincidenceratethatwouldhaveoccurrediftheagedistributioninthe populationofinterestwasthesameasthatofthestandard,whereincidencerateisdefinedasthe numberofcasesofcancer(malignantneoplasms)newlydiagnosedduringaspecifictimeperiod,per 100,000peopleatrisk.
Numerator:Numberofnewcancercasesforeachstageduringthegiventimeperiod.
Denominator:Totalpopulation(person‐time)atriskforaspecificsexduringthegiventimeperiod.
Measurementtimeframe:2010to2012combined
Stratificationvariables:Province,stage(includingstageI,II,IIIandIV)
Agestandardization:Directmethodusingthe2011CanadianCensuspopulationasstandardweights
Provincespecificnotes:AB:Hematology,sarcomaandmelanomamorphologieswereremovedfrom thesite‐specificcancers.
Generalnotes:
1.WorldHealthOrganization,InternationalClassificationofDiseasesforOncology,ThirdEdition(ICD‐
O‐3)andtheInternationalAgencyforResearchonCancer(IARC)rulesfordeterminingmultiple primariessiteswereused:colorectal(ICD‐O‐3:C18.0,C18.2toC18.9,C19.9,C20.9,C26.0),lungand bronchus(ICD‐O‐3:C34.0toC34.9),breast(ICD‐O‐3:C50.0toC50.9),prostate(ICD‐O‐3:C61.9). 2.AppendixC18.1wasexcludedfromcolorectalcancer.
3.SiteswithhistologycodesforlymphomaM‐95toM‐98,sarcomacodes–8800/3wereexcluded. 4.Casesforpatientswithageunder18(notincluded)atdiagnosiswereexcluded.
5.AmericanJointCommitteeonCancer7edition(AJCC7)wasusedtoclassifycancergroupstage.
Age‐standardized
mortality
rates
Definition:Themortalityratethatwouldhaveoccurrediftheagedistributioninthepopulationof interestwasthesameasthatofthestandard,wheremortalityrateisdefinedasthenumberofdeaths duetocancer(malignantneoplasms)inayearper100,000peopleatrisk
Numerator:Numberofdeathsfromcancer(allages):1.Breast(female);2.Colorectal;3.Lung;4. Prostate(male);5.Pancreas
Denominator:1.Annualfemalepopulationestimateinhundredsofthousands2,3,5Annual populationestimatesinhundredsofthousands;2.Annualmalepopulationestimateinhundredsof thousands
Agestandardization:Directmethodusingthe2011CanadianCensuspopulation
Datasources:CanadianVitalStatistics–DeathDatabase–cancermortalitydata;DemographyDivision ofStatisticsCanada–populationestimates
Measurementtimeframe:Foroveralltrends,Canada–1992to2011.Byprovince:3‐yearcombined (2009–2011).
Stratificationvariables:Province
Generalnotes:
1. Uptotheyear1999,causesofdeathwerecodedaccordingtoWorldHealthOrganization(WHO), InternationalClassificationofDiseases,NinthRevision(ICD‐9):Colorectal(ICD‐9153‐154),lung (ICD‐9:162),femalebreast(ICD‐9:174),prostate(ICD‐9:185),pancreas(ICD‐9:157)2.Afterthe year1999,causesofdeathwerecodedaccordingtotheWorldHealthOrganization(WHO), InternationalStatisticalClassificationofDiseasesandRelatedHealthProblems,TenthRevision (ICD‐10): Colorectal(ICD‐10:C18‐C20,C26.0),lung(ICD‐10:C34),femalebreast(ICD‐10:C50), prostate(ICD‐10:C61),pancreas(ICD‐10:C25)
2. JoinpointRegressionProgram4.1.1forWindowswasusedtoanalyzelineartrendsacrossyears. Thesoftwaretakestrenddataandfitsthesimplestjoinpointmodelthatthedataallow. The programstartswiththeminimumnumberofjoinpoints(e.g.0joinpoints,whichisastraightline) andtestswhethermorejoinpointsarestatisticallysignificantandmustbeaddedtothemodel(up tothatmaximumnumber).Thisenablestheusertotestwhetheranapparentchangeintrendis statisticallysignificant.ThetestsofsignificanceuseaMonteCarloPermutationmethod. Annual PercentChange(APC)wasreportedtocharacterizetrendsincancerratesovertime. APCassumes thatcancerratesarechangingataconstantpercentageoftherateofthepreviousyear. The minimumandmaximumnumberofjoinpointsusedinthisanalysiswere0and4respectively. For furtherdetails,refertotheJoinpointRegressionProgramdocumentation
Age‐standardized
relative
survival
ratios
Definition:Relativesurvivalratio(RSR)istheratiooftheobservedsurvivalforagroupofcancer patients(malignantneoplasms)totheexpectedsurvivalformembersofthegeneralpopulationwho havethesamemainfactorsaffectingsurvival(sex,age,placeofresidence)asthecancerpatients.The age‐standardizedRSRisthatrelativesurvivalthatwouldhaveoccurrediftheagedistributionofthe cancerpatientsunderstudyhadbeenthesameasthatofthestandardpopulation
Numerator:Forperiodanalysismethod(2006‐2008):Observedcumulativesurvivalprobabilitiesof cancerpatientsafterdiagnosiswithfollow‐upin2006to2008forbreast,lungandcolorectal;2005to 2007forpancreas.Forcohortanalysismethod(1992‐1994):Observedcumulativesurvivalprobabilities ofcancerpatientswhowerediagnosedduring1992‐1994:1.Breast;2.Colorectal;3.Lung;4.Pancreas
Denominator:Expectedsurvivalofcomparisonpopulationthatwasalivefor5yearsforpatientswith follow‐upin2006to2008forbreast,lungandcolorectal;2005to2007forpancreas.
Age‐standardized:Forbreast,lungandcolorectal:age‐standardizedtopeoplediagnosedwiththat cancerinCanadabetween1992and2001. Forpancreas,age‐standardizedtopopulationdiagnosed withpancreaticcancerinCanadabetween2001and2005
Datasources:Breast,lungandcolorectal:CanadianCancerStatistics2013;Pancreas:Canadian CancerRegistry(annualfile,releasedate2011);Provinciallifetables(providedfromStatisticsCanada, 2012)
Measurementtimeframe:Forperiodanalysismethod,patientswithfollow‐upduring2006to2008for breast,lungandcolorectal;2005to2007forpancreas.Forcohortanalysismethod,patientsdiagnosed during1992to1994
Stratificationvariables:Province
Generalnotes:
1.WorldHealthOrganization,InternationalClassificationofDiseasesforOncology,ThirdEdition(ICD‐
O‐3)andtheInternationalAgencyforResearchonCancer(IARC)rulesfordeterminingallprimaries siteswereused:colorectal(ICD‐O‐3C18.0toC18.9,C19.9,C20.9,C26.0),lungandbronchus(ICD‐O‐3 C34.0toC34.9),breast(ICD‐O‐3C50.0toC50.9),pancreas(ICD‐O‐3:C25.0‐C25.9)
2.“Canada”representsallprovincesandterritories,exceptQuebec.DatafromQuebechavebeen excluded,inpart,becausethemethodofascertainingthedateofcancerdiagnosisdiffersfromthe methodusedbyotherregistriesandbecauseofissuesincorrectlyascertainingthevitalstatusofcases. 3.Theanalysiswasconductedusingbothcohortandperiodanalysismethods(Reference:BrennerH, GefellerO.Analternativeapproachtomonitoringcancerpatientsurvival.Cancer.1996;78:2004–10). 4.Expectedsurvivalproportionswerederivedfromsex‐specificcompleteprovinciallifetables
producedbyStatisticsCanada,usingtheEdererIIapproach.(Reference:EdererF,HeiseH.Theeffectof eliminatingdeathsfromcancerongeneralpopulationsurvivalrates(methodologicalnote11,End ResultsEvaluationsection).NationalCancerInstitute;August1959)
5. Periodanalysis was used to estimate the survival for the cases diagnosed 2006 – 2008 for breast, lung andcolorectal;2005–2007forpancreas.Relativesurvivalratiosfor1992to1994werecalculated usingcohortanalysis.Forbreast,lungandcolorectal,thesedataarebasedonpeopleaged15–99years atdiagnosis.SurvivalratiosforNewfoundlandandLabradorarenotshownastheyareartificiallyhigh. Forpancreas,thesedataarebasedonpeopleaged15‐74,MB,NBandPEhassparsedatainsomeofthe agegroups,therefore,resultswerenotpresentedsincetheestimatewouldbeunstable.