STRESS AND COPING AMONG PREDOCTORAL AND ADVANCED DENTAL EDUCATION STUDENTS/RESIDENTS
Philip M. Worthington
A thesis submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the UNC Adams School of
Dentistry (Orthodontics).
Chapel Hill 2020
Approved by: Ceib Phillips
© 2020
ABSTRACT
Philip M. Worthington: Stress and Coping among Predoctoral and Advanced Dental Education Students/Residents
(Under the direction of Ceib Phillips)
ACKNOWLEDGEMENTS
TABLE OF CONTENTS
LIST OF FIGURES ... vii
LIST OF TABLES... viii
STRESS AND COPING AMONG PREDOCTORAL AND ADVANCED DENTAL EDUCATION STUDENTS/RESIDENTS ... 1
Introduction ... 1
Materials and Methods ... 4
Results ... 8
Discussion ... 11
Conclusions ... 16
Figures ... 17
Tables ... 19
LIST OF FIGURES
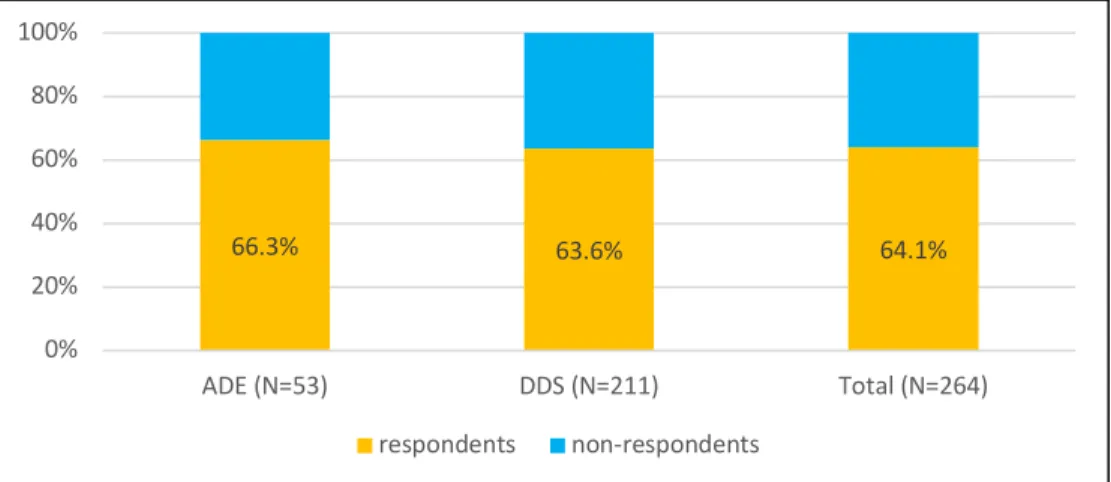
Figure 1 – Survey Response Rate………..18
Figure 2 – Age of Respondents ... 18
Figure 3 – Relationship Status of Respondents ... 18
Figure 4 – Responsibility for Children of Respondents ... 19
LIST OF TABLES
Table 1 – Respondents' demographics by number and percentage of total ... 20
Table 2 – Anxiety ... 21
Table 3 – Depression ... 21
Table 4 – Burnout ... 21
Table 5 – Social Support ... 21
Table 6 – Suicidal Ideation ... 22
STRESS AND COPING AMONG PREDOCTORAL AND ADVANCED DENTAL EDUCATION STUDENTS/RESIDENTS
Introduction
In 2018, the University of North Carolina at Chapel Hill administered an online mental health/wellness survey to its Doctor of Philosophy (PhD) candidate students in the Biomedical Sciences department. The results of that unpublished survey showed a high prevalence of depression among these students, and a greater than 10% incidence of suicidal ideation among the students in the two weeks prior to completing the survey1. These findings appear consistent
with widespread concern over a growing mental health crisis in graduate education. A 2018 survey of 2,279 PhD and Master’s candidates across 26 countries showed that these graduate students were six times more likely than the general population to experience symptoms of depression and anxiety2.
For many years the popular press has portrayed the dental profession as prone to poor mental health and an increased risk of suicide3. These claims are difficult to support
scientifically4 but a review of past surveys of the profession reveals high levels of burnout and a
perception among dentists that their profession is more stressful than other occupations5. The
literature on mental wellness in dentistry is unable to pinpoint a specific causative factor contributing to adverse mental health in the profession but suggests that a combination of work and nonwork-related stressors could be potentiated instances of previous mental pathology4.
would represent a useful step in understanding if mental health deteriorates as dental training progresses4.
Recent publications suggest high levels of stress and mental unease amongst graduate students in biomedical fields of study. A 2014 report on wellbeing conducted by UC Berkeley reported a 43–46% rate of depression for graduate students in the biomedical sciences6. A
survey conducted in 2015 at the University of Arizona report concluded that a majority of doctoral students reported ‘more than average’ current stress or ‘tremendous’ stress7.
Furthermore, a 2016 nationwide survey of pharmacy residents, using the depression screening component of the Patient Health Questionnaire (PHQ-9) reported a 39.9% incidence of
moderate-severe depressive symptoms8, significantly higher than the 6.6-7.6% incidence in the
general population9. The report also found that depressive symptoms seemed to build over the
course of the residency year, as scores indicative of major depressive symptoms increased from 2.9% in the September survey distribution to 7.3% in responses to the same survey in March8.
Although the body of research concerning mental health in dental students remains limited, a few reports suggest reason for concern. A 2002 study of UK Dental students found that levels of pathological anxiety grew from 47% amongst second year students to 67% for the same students in their final year, but dropped to 19% once the students reached their first year of dental practice10. This study found that the opposite trend existed in medical students, with
anxiety levels dropping as training progressed, before rising again in the first year of medical practice10.
A more encouraging 2016 study at the University of Florida College of Dentistry
predoctoral students reported feeling a sense of purpose about their futures9. The survey found
that only 15% of respondents reported a lack of self-perceived wellness. Students with children reported significantly lower levels of perceived wellness, and Asian and Hispanic students reported more concern over the state of their mental health9.
According to research by the American Dental Association, 39.4% of Class of 2017 dental graduates enrolled in an advanced dental education residency (ADE) following
completion of their pre-doctoral (DDS) program11. With increasing years of specialized study,
dental students accumulate higher levels of educational debt, experience more burdensome academic demands and increase the number of patient and clinical experiences that could lead to professional burnout. A multi-institutional study of orthodontic residents in India showed that students in their second and third year of advanced training had higher odds of developing moderate to high levels of depression, anxiety and psychological stress12.
Given the increased stressors associated with dental residency training, it follows that ADE students may tend to exhibit more signs of adverse mental health and need more
Materials and Methods
The Institutional Review Board of the University of North Carolina Office of Human Research Ethics approved this study (#18-1870). A web-based survey was distributed to all DDS (N=332) and ADE (N=80) students at the University of North Carolina Claude A. Adams Jr. and Grace Phillips Adams School of Dentistry in the Fall of 2018. The students received an email explaining the purpose of the study as well as an individualized link that would permit them to complete the survey only once. Due to the potentially sensitive nature of the survey queries, the email explained that survey responses would be kept confidential and that no data with respect to subgroups of less than 10 individuals would be reported in order to prevent possible deductive identity disclosures. The final survey consisted of 70 questions. The
questions targeted the outcome variables of anxiety, depression, burnout and suicidal ideation in the student population. Additional questions gathered explanatory variable data in the form of social support and demographic information.
Diagnosis Total Score For Score Action
Minimal depression 0 - 4 £ 4 The score suggests the patient may not need depression treatment
Mild depression Moderate depression
5 - 9 10 - 14
5 - 14 Physician uses clinical judgement about treatment based upon patient’s duration of symptoms and functional impairment
Moderately severe depression Severe depression
15 – 19 20 - 27
> 14 Warrants treatment for depression using a combination of medication and/or psychotherapy Despite its brevity, the PHQ-9 has been shown to be a useful and valid instrument for identifying the signs and symptoms of severe depression13.
The symptoms of generalized anxiety disorder (GAD) were assessed using the GAD-7 instrument. The GAD-7 is a seven-item questionnaire that focuses on the occurrence of symptoms such as irritability, restlessness and nervousness over the two-week period
immediately prior to the date of survey completion. The GAD-7 uses the same frequency scale as the PHQ-9 with a possible scoring range from 0-21. Increasing total score correlates with higher levels of anxiety in the respondent as dictated by the following scoring scale:
Interpretation Total Score
Mild anxiety 5 - 9
Moderate anxiety 10 – 15
10 ≥ probable diagnosis of GAD; confirmed by further evaluation
Severe anxiety 15 - 21
Despite some overlap in the signs of depression and anxiety, the GAD-7 has shown the
specificity to identify distinct manifestations of anxiety and is therefore regarded as a valid and efficient screening tool for GAD with 89% sensitivity and 82% specificity14.
Provider burnout was assessed through an abbreviated version of the Maslach Burnout Inventory (MBI). Developed in 1981, the MBI has been a frequently used assessment tool to measure burnout in a wide range of healthcare and professional research. The concept of
mistakes that might result in harm to patients. In a 2010 survey of American surgeons, investigators found a strong correlation between major medical errors in surgery and the surgeon’s degree of burnout and mental quality of life16.
The MBI measures three dimensions of burnout: emotional exhaustion,
depersonalization, and personal accomplishment17, and the abbreviated version includes three
questions directly pertaining to each category. The survey included nine questions from the original MBI with items scored using a 7-level frequency scale from ‘never’ to ‘daily.’ Possible scores for each category range from 0-18, with heightened levels of professional burnout
indicated by higher overall values.
The final outcome variable captured through the survey pertained to suicidal ideation. Suicidal ideation, or suicidal thinking, is the contemplation of ending one’s own life. The term encompasses a broad spectrum of individual thought, from momentary ideas to detailed
planning. Suicidal ideation can represent the next step in a progression of adverse mental health signs and symptoms such as hopelessness, anxiety, depression, drug and alcohol abuse or lack of social support. While instances of suicidal ideation do not always result in a suicide attempt, the existence of suicidal ideation in individuals demands serious attention. Past research shows that about 20% of individuals who die by suicide had previously mentioned their thoughts to a physician or mental health provider18. Suicidal ideation was assessed through a dichotomous
question asking respondents if they had thought about ending their life in each of three retrospective time periods: ever, in the last 12 months and while enrolled at UNC.
Additional questions used a Likert scale to assess students’ perceptions of the sufficiency of their daily sleep, diet, exercise, leisure and productivity with possible responses for each category ranging from 1-5. Due to recent research suggesting an association between increased social media use and depression in young adult populations19, the survey included questions about the
amount of time participants spent visiting social media sites. The survey also queried the concept of loneliness using an abbreviated form of the Revised UCLA Loneliness Scale. Consisting of only three questions, the short form the R-UCLA scale has been shown to be psychometrically valid despite its limited inquiries20.
A final explanatory variable of potential significance was the perceived presence or absence of social support. Social support describes the ability of positive interpersonal
relationships in buttressing individuals against stressful life events. Increasing evidence suggests that the availability of social support may positively affect an individual’s overall mental
wellness21. One of the most psychometrically validated instruments for measuring social support
is the MOS Social Support Survey developed as part of the Medical Outcomes Survey. This 19-part module includes questions about emotional, tangible, information and affectionate support. The researchers at the University of Florida College of Dentistry included a modified version of the MOS Social Support Survey in their investigation of the self-perceived mental wellness of pre-doctoral dental students9. The survey included all 19 elements of the MOS with minor
modifications to increase the applicability of the four tangible components of the survey to the dental school environment.
continuous outcome variables, and the MH correlation statistic for continuous explanatory and outcome variables. Bivariate analyses were also performed to assess the relationship among the outcome variables. Additionally, multivariate analysis using multi-nominal logistic regression was generated to assess how individual demographic and social support factors affected the outcome mental health markers, while controlling for the presence or absence of other explanatory variables. Level of significance was set at 0.05 for all analyses.
Results
The overall response rate for the survery was 64.1% (N=264), with 66.3% of ADE (53/80) and 211/332 of DDS partipicating (See Figure 1). Respondent characteristics are shown in Table 1. Participants predominantly identified as white (DDS=64.5%, ADE=52.8%) and female (DDS=59.2%, ADE=52.8%). ADE respondents were significantly older, with 51% of respondents being at least 30 years of age as compared to only 8% of DDS respondents (p<0.0001, see Figure 2). ADE respondents were also more likely to be in a committed
relationship wife a spouse or partner (p=0.002, See Figure 3) and to have children (p=0.001, See Figure 4). ADE residents also maintained significantly higher levels of educational debt, with 36% reporting over $200,000 in outstanding loans as compared to only 11% of DDS respondents (p=0.002, See Figure 5).
When considering anxiety outcomes, a GAD-7 score of 10 is considered an indicator of moderate to severe anxiety and equates to a probable diagnosis of generalized anxiety disorder14.
with moderately severe or severe depression and justifies pharmacologic and/or psychotherapy treatment13. The prevalence of moderately severe or severe depression was 17.9% among total
respondents. As with anxiety, the DDS population showed a higher prevalence (18.4%) than the ADE (15.7%) students, but once again the difference was not significant (P=0.33, See Table 3).
Both ADE and 3rd and 4th year DDS students indicated relatively high feelings of
personal accomplishment through the MBI, recording mean scores of 13.7 and 14.1 respectively on an 18-point scale (See Table 4). MBI scores for personal accomplishment (p=0.64), emotional exhaustion (p=0.68), and depersonalization (P=0.50) did not differ significantly between ADE students and 3rd/4th year DDS students.
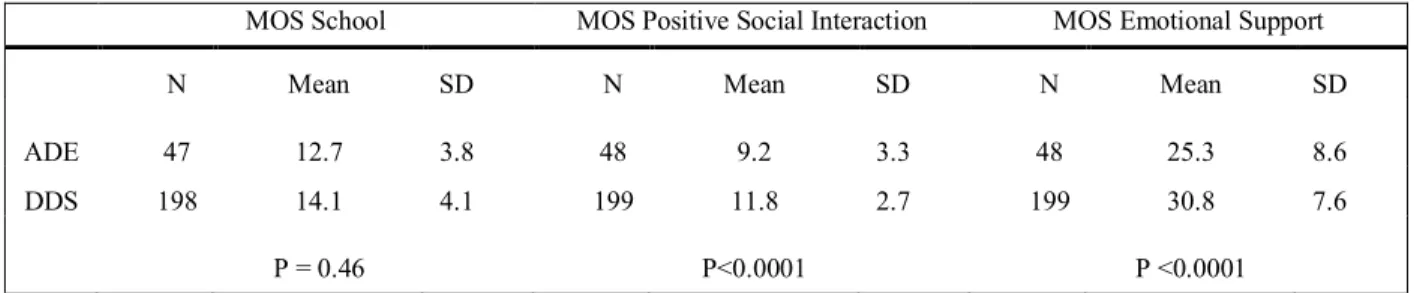
The results of the MOS portion of the survey indicated that that DDS experienced higher levels of social support (See Table 5). DDS students reported receiving significantly more support than ADE students in all three measured subscales: tangible (in school) support (P=0.046), positive social interactions (P<0.0001) and emotional support (P<0.0001).
A total of 187 students (76%) reported never experiencing suicidal ideation (See Figure 6). 10% of surveyed students reported incidents of suicidal ideation while studying at UNC, with 7% reporting ideation in the 12 months preceding the survey. The difference in the
incidence of suicidal ideation both at UNC (p=0.79) and in the last 12 months (P=0.53) was not significant between ADE and DDS respondents.
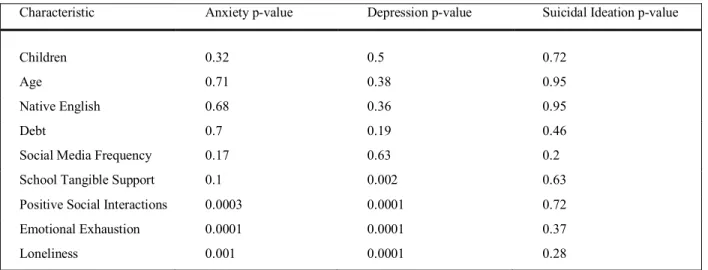
were more likely to shower higher levels of anxiety (p=0.0001) and depression (p=0.0001). Respondents who expressed higher levels of loneliness were also significantly more likely to show to report higher levels of anxiety (p=0.001) and depression (p=0.0001). None of the demographic or coping variables showed a significant correlation with the presence of suicidal ideation. However, 54% of students with recent suicidal ideation (within the previous 12
months) also exhibited scores within the range of moderate to severe or severe depression on the survey (p=0.01). 58% of this same group of respondents exhibited anxiety scores consistent with moderate to severe or severe anxiety (p=0.01).
To assess the relationship of covariates and control for confounding factors, a
multivariate logistic regression analysis was performed on the outcome variables of anxiety and depression. The final logistic regression analysis was multilayered, where the demographic covariates of program (ADE/DDS), age, race, debt load, native English speaker status,
relationship status and the presence of children were used to find associations with the outcome variables of anxiety and depression. Following this initial regression analysis, any demographic covariates with a p<0.10 were included in a final multivariate which also included the previously identified significant covariates of In School support (MOS), Emotional Support (MOS),
proved to be a significant protective factor for depression in students (p=0.02). The adjusted odds ratio of 0.9 indicated that for each one unit increase in emotional social support, the odds of a student reporting moderately severe/severe depression decreased by 10%.
Discussion
This study examined the difference in overall mental health perception between DDS and ADE students, finding no significant difference in the prevalence of anxiety, depression or suicidal ideation between these distinct student populations. However, overall levels of anxiety and depression among DDS and ADE respondents proved higher than those of the general population. The covariates showing the most significant correlation with the presence of anxiety and depression were the socially-related factors of loneliness and emotional support. Practical explanatory variables such as age, student debt level, relationship status and the presence of children showed no significant correlation with overall levels of anxiety and depression in the collective survey population.
Consistent with prior reports documenting psychological distress among dental students
22,23,10, the results of this study demonstrate elevated levels of depression and anxiety amongst the
respondent population. Although estimates of the prevalence of mental health disorders in the general population vary by report, epidemiologic studies in psychiatry put the annual prevalence rate of generalized anxiety disorder at anywhere between 0.2 – 4.3 %24. With 25.1% of survey
severe to severe depression was six times higher than the estimated 2.4% prevalence in the general US population25.
Although there is a lack of evidence comparing levels of psychological distress between undergraduate dental students and graduate dental residents, higher levels of mental unwellness could reasonably be presumed based on previous reports highlighting the stressors common to dental education. Anxiety scores for UK dental students increased with increasing years of study10, as did anxiety and depression levels for Indian orthodontic residents12. High levels of
student debt represent a reality for many dental students and residents, and evidence suggests that stress levels increase with increasing levels of student loan responsibility26. Personal
circumstances and family responsibilities represent another stressor, and one survey of US dental students showed significantly lower levels of perceived mental wellness amongst students
shouldering parenting responsibilities9. In the present study, ADE students were significantly
older, significantly more likely to have children, and carried significantly higher levels of student debt. Despite the increased presence of these stressors, and the concomitantly greater time in training necessitated by choosing to pursue a specialty residency, this study found no significant difference in the reported levels of moderate to severe anxiety or moderately severe to severe depression between DDS and ADE students.
The significant correlation between social support parameters and levels of anxiety and depression found in this study is consistent with prior reports suggesting the positive role of social support in promoting mental wellness in dental students9,27. However, the responses
for class ranking that characterize ADE programs could be thought to theoretically increase the social support tendency amongst participants. However, the significantly greater likelihood of the surveyed ADE participants to have partners and children might represent a factor that increases distraction and decreases motivation to seek support from colleagues. This study also found that ADE respondents were significantly less likely to be native English speakers than their DDS counterparts (40% versus 5%, p<0.0001). The potentially isolating effect of being a non-Native English speaker in the milieu of dental education is a factor that warrants further investigation.
Loneliness proved to be the explanatory factor showing the most predictive power in the present study, showing significant correlations with elevated anxiety and depression levels in both the bivariate and multivariate analysis. A 2019 study of graduate health sciences students at a public Midwestern university found that nearly one-fifth (19.4%) reported feelings of social isolation28. Although that study did not investigate correlations with manifestations of
diminished mental health such as anxiety and depression, the study did find a significant
correlation between feelings of social isolation and such factors as English as a second language, the presence of social support and hours spent caring for dependents28. Investigators in a 2015
study of US internal medical residents at an urban academic center used the abbreviated UCLA Loneliness scale to demonstrate a significant correlation between loneliness scores and
increasing levels of the depersonalization and emotional exhaustion components of professional burnout29. Despite the finding of correlation in the present study, the potentially reciprocal
anxiety and depression of an unknown cause might be prompting feelings of loneliness represents an equally plausible conclusion.
Although causation remains unclear, the notable correlation between loneliness and anxiety/depression in the student and resident population warrants further investigation.
Although the 3-item UCLA Loneliness scale that was used in this study has shown psychometric validity and consistency with the 20-item UCLA Loneliness scale20,30, use of the longer form of
the scale might have revealed more specific insight into the specific factors driving loneliness in the surveyed population. The 20-item scale includes questions about being understood and a sense of commonality with a surrounding peer group, and may have helped to identify specific interventions for combatting loneliness amongst the respondents. Another possibility remains that the abbreviated UCLA Loneliness scale lacked specificity and generated false positive responses in the form of individuals who desire or remain comfortable with a greater degree of isolation. Although there is a lack of recent, detailed evidence regarding personality types in dentistry, a 1991 study found that dentists identified as introverts at a rate greater than the general population31. The more extensive loneliness scale may have proved useful in identifying
true indicators of loneliness rather than a more general predisposition toward independence that may possibly characterize trainees in a graduate dental education program.
Other than loneliness, the only other explanatory variable that showed a multivariate correlation with either anxiety or depression was the emotional social support component of the MOS social support scale. The emotional portion of the MOS is designed to measure the presence of support in the form of empathetic understanding and the encouragement of expressions of feelings32. The survey data from this study suggests that the presence of
respondent population. The adjusted odds ratio of 0.9 reflects that for each single unit increase in the MOS emotional support score, the odds of a student reporting moderately severe to severe depression decreased by 10% (p=0.02).
Another potential protective factor that was not addressed in this study is the presence of positive mindfulness disciplines. Mindfulness refers generally to self-awareness that promotes a greater appreciation of the role the mind plays in contributing to feelings, actions and overall control of the body. A growing body of literature suggests that higher levels of mindfulness can be associated with reduced presence of anxiety, depression and stress33,34. Mindfulness practices
have increasingly been touted as not only a way to treat individuals with mental health disorders, but as a tool to incorporate into professional healthcare training to prevent burnout by fostering empathy and connection to patients34. Accordingly, graduate healthcare education programs
have begun to develop mindfulness educational programs to supplement their professional training curricula35. One recent study showed that graduate healthcare students completing an 8
week Mindfulness Based Stress Reduction course showed a significant reduction in anxiety and an increase in empathy compared to baseline measurements20. A controlled study exposing DDS
and ADE students to a similar curriculum could prove useful in determining the efficacy of
into the ways in which mental wellness may fluctuate with the progress and duration of training. The given study also represents the student population at a single institution, and a multi-site approach to this research would provide a more generalized overview of the mental health climate across all of dental higher education.
Conclusion
Figure 1. Survey Response Rate
Figure 2. Age of Respondents
Figure 3. Relationship Status of Respondents 49.00% 92.00% 51.00% 8.00% 0% 20% 40% 60% 80% 100% ADE DDS
Age
(P< 0.0001)≤ 30 > 30
47.00% 25.00% 53.00% 75.00% 0% 20% 40% 60% 80% 100% ADE DDS
Relationship Status
(P=0.002)Has Spouse/Partner Single
66.3% 63.6% 64.1%
0% 20% 40% 60% 80% 100%
ADE (N=53) DDS (N=211) Total (N=264)
Figure 4. Responsibility for Children of Respondents
Figure 5. Debt Level of Respondents
21.00% 6.00%
79.00% 94.00%
0% 20% 40% 60% 80% 100%
ADE DDS
Children
(P=0.001)Students with Children Students Without Children
55%
9%
36% 60%
29%
11%
0% 20% 40% 60% 80%
≤ 100K 101-200K > 200K
Educational Debt Load
(P=0.002)Table 1. Respondents' demographics by number and percentage of total
Characteristic DDS ADE Total
Gender
Female 59.2% (125) 52.8% (28) 58.0% (153)
Male 40.8% (86) 47.2% (25) 42.0% (111)
Race/Ethnicity
White 64.5% (136) 52.8% (28) 62.1% (164)
African American 9.5% (20) 0.0% (0) 7.6% (20)
Asian 11.8% (25) 20.8% (11) 13.6% (36)
Hispanic 7.1% (15) 7.5% (4) 7.2% (19)
Middle Eastern 3.8% (8) 9.4% (5) 4.9% (13)
Pacific Islander 0.5% (1) 0.0% (0) 0.4% (1)
Other or prefer not to identify 2.8% (6) 9.4% (5) 4.2% (11)
Age in Years
20-25 64.9% (137) 1.9% (1) 52.3% (138)
26-30 27.0% (57) 47.2% (25) 31.1% (82)
31-35 5.2% (11) 35.8% (19) 11.1% (30)
36 or older 2.8% (6) 15.1% (8) 5.3% (14)
Year in Training
1st 35.5% (75) 30.2% (16) 34.5% (91)
2nd 25.6% (54) 28.3% (15) 26.1% (69)
3rd 16.1% (34) 15.1% (8) 15.9% (42)
3rd or more 19.4% (41) 20.8% (11) 19.7% (52)
4th or more 3.3% (7) 5.7% (3) 3.8% (10)
Educational Debt Load
0 to 50,000 22.7% (47) 37.4% (20) 25.8% (67)
51,000 to 100,000 37.2% (77) 17.0% (9) 33.1% (86)
101,000 to 150,000 18.4% (38) 0.0% (0) 14.6% (38)
151,000 to 200,000 11.1% (23) 9.4% (5) 10.8% (28)
201,000 to 250,000 5.3% (11) 3.8% (2) 5.0% (13)
251,000 to 300,000 4.4% (9) 15.1% (8) 6.5% (17)
More than 300,000 1.0% (2) 17.0% (9) 4.2% (11)
Parent with Child/Children
Yes 5.7% (12) 20.8% (11) 8.8% (23)
No 94.3% (197) 79.2% (42) 91.2% (239)
Relationship with Spouse/Partner
Yes 24.9% (52) 47.2% (25) 29.4% (77)
Table 2. Anxiety
Reported Anxiety Level DDS Percentage Reporting(N) ADE Percentage Reporting(N) p-value
Mild 50.7% (104) 52.0% (26)
Moderate 23.4% (48) 26.0% (13)
Moderate to Severe/Severe 25.9% (53) 22.0% (11) 0.98
Table 3. Depression
Reported Depression Level DDS Percentage Reporting(N) ADE Percentage Reporting(N) p-value
Mild 54.9% (113) 49.0% (25)
Moderate 26.7% (55) 35.3% (18)
Moderate to Severe/Severe 18.4% (38) 15.7% (8) 0.33
Table 4. Burnout
Emotional Exhaustion Depersonalization Accomplishment N Mean SD N Mean SD N Mean SD ADE 45 9.4 4.5 45 3.8 4.0 46 13.7 4.0 DDS 71 9.7 4.7 71 3.3 3.1 71 14.1 3.0
P = 0.68 P = 0.50 P = 0.64
Note: Only 3rd and 4th year DDS students included in reported results. All scores on a 0-18 scale. Emotional exhaustion: higher scores indicate greater burnout and greater
emotional exhaustion. Depersonalization: higher scores indicate greater depersonalization and greater burnout. Personal accomplishment: higher scores indicate greater personal accomplishment and less burnout.
Table 5. Social Support
MOS School MOS Positive Social Interaction MOS Emotional Support
N Mean SD N Mean SD N Mean SD
ADE 47 12.7 3.8 48 9.2 3.3 48 25.3 8.6 DDS 198 14.1 4.1 199 11.8 2.7 199 30.8 7.6
P = 0.46 P<0.0001 P <0.0001
Table 6. Suicidal Ideation
Ever While at UNC Last 12 Months
N No Yes N No Yes N No Yes
Table 7. Association of Select Explanatory Variables with Mean Responses for Anxiety, Depression and Suicidal Ideation
Characteristic Anxiety p-value Depression p-value Suicidal Ideation p-value
Children 0.32 0.5 0.72
Age 0.71 0.38 0.95
Native English 0.68 0.36 0.95
Debt 0.7 0.19 0.46
Social Media Frequency 0.17 0.63 0.2 School Tangible Support 0.1 0.002 0.63 Positive Social Interactions 0.0003 0.0001 0.72 Emotional Exhaustion 0.0001 0.0001 0.37
REFERENCES
1. Schad, Alli. 2018. Personal Communication.
2. Evans TM, Bira L, Gastelum JB, Weiss LT, Vanderford NL. Evidence for a mental health crisis in graduate education. Nat Biotechnol. 2018 Mar 6;36(3):282–4.
3. Alexander RE. Stress-related suicide by dentists and other health care workers. Fact or folklore? J Am Dent Assoc. 2001 Jun;132(6):786–94.
4. Sancho FM, Ruiz CN. Risk of suicide amongst dentists: myth or reality? International Dental Journal. 2010 Dec 1.
5. Rada RE, Johnson-Leong C. Stress, burnout, anxiety and depression among dentists. J Am Dent Assoc. 2004 Jun;135(6):788–94.
6. Graduate Assembly. Graduate Student Happiness & Well-Being Report. University of California, Berkeley. 2014.
7. Smith E, Brooks Z. Graduate student mental health 2015. National Association of Graduate-Professional Students (NAGPS) and the Graduate Graduate-Professional Student Council (GPSC),
University of Arizona. 2015.
8. Williams E, Martin SL, Fabrikant A, Wang A, Pojasek M. Rates of depressive symptoms among pharmacy residents. Am J Health Syst Pharm. 2018 Mar 1;75(5):292–7.
9. Harrison PL, Shaddox LM, Garvan CW, Behar-Horenstein LS. Wellness among dental students: an institutional study. J Dent Educ. 2016 Sep;80(9):1119–25.
10. Newbury-Birch D, Lowry RJ, Kamali F. The changing patterns of drinking, illicit drug use, stress, anxiety and depression in dental students in a UK dental school: a longitudinal study. Br Dent J. 2002 Jun 15;192(11):646–9.
11. American Dental Association, Health Policy Institute, 2018-19 Survey of Dental Education (Group I, Questions 1-4).
12. Madhan B, Rajpurohit AS, Gayathri H. Mental health of postgraduate orthodontic students in India: a multi-institution survey. J Dent Educ. 2012 Feb;76(2):200–9.
13. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001 Sep;16(9):606–13.
15. Maslach C, Jackson SE. The measurement of experienced burnout. J Organ Behav. 1981 Apr;2(2):99–113.
16. Shanafelt TD, Balch CM, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995-1000.
17. Maslach, C.; Jackson, S.E.; Leiter, M.P. (1996–2016). Maslach Burnout Inventory Manual (Fourth Edition). Menlo Park, CA: Mind Garden, Inc.
18. Pedersen, T. (2018). Suicidal Ideation. Psych Central. Retrieved on April 26, 2020, from
https://psychcentral.com/encyclopedia/suicidal-ideation/.
19. Lin LY, Sidani JE, Shensa A, Radovic A, Miller E, Colditz JB, et al. Association between social media use and depression among u.s. young adults. Depress Anxiety. 2016
Apr;33(4):323–31.
20. Hughes ME, Waite LJ, Hawkley LC, Cacioppo JT. A Short Scale for Measuring Loneliness in Large Surveys: Results From Two Population-Based Studies. Res Aging. 2004;26(6):655–72. 21. Harandi TF, Taghinasab MM, Nayeri TD. The correlation of social support with mental health: A meta-analysis. Electron Physician. 2017 Sep 25;9(9):5212–22.
22. Lloyd C, Musser LA. Psychiatric Symptoms in Dental Students. The Journal of Nervous and Mental Disease. 1989;177(2):61-69.
23. Stewart DW, de Vries J, Singer DL, Degen GG, Wener P. Canadian dental students’
perceptions of their learning environment and psychological functioning over time. J Dent Educ. 2006 Sep;70(9):972–81.
24. Bandelow B, Michaelis S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin Neurosci. 2015 Sep;17(3):327–35.
25. Shim RS, Baltrus P, Ye J, Rust G. Prevalence, treatment, and control of depressive symptoms in the United States: results from the National Health and Nutrition Examination Survey (NHANES), 2005-2008. J Am Board Fam Med. 2011 Feb;24(1):33–8.
26. Boyles JD, Ahmed B. Does student debt affect dental students’ and dentists’ stress levels? Br Dent J. 2017 Oct 27;223(8):601–6.
27. Crego A, Carrillo-Diaz M, Armfield JM, Romero M. Stress and Academic Performance in Dental Students: The Role of Coping Strategies and Examination-Related Self-Efficacy. J Dent Educ. 2016 Feb;80(2):165–72.
29. Shapiro J, Zhang B, Warm EJ. Residency as a social network: burnout, loneliness, and social network centrality. J Grad Med Educ. 2015 Dec;7(4):617–23.
30. Russell DW. UCLA Loneliness Scale (Version 3): reliability, validity, and factor structure. J Pers Assess. 1996 Feb;66(1):20–40.
31. Westerman GH. Personality types of dentists. American journal of dentistry. 12/1991;4(6):298-302.
32. Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991;32(6):705– 14.
33. Jimenez SS, Niles BL, Park CL. A mindfulness model of affect regulation and depressive symptoms: Positive emotions, mood regulation expectancies, and self-acceptance as regulatory mechanisms. Pers Individ Dif. 2010 Oct;49(6):645–50.
34. McConville J, McAleer R, Hahne A. Mindfulness Training for Health Profession Students-The Effect of Mindfulness Training on Psychological Well-Being, Learning and Clinical Performance of Health Professional Students: A Systematic Review of Randomized and Non-randomized Controlled Trials. Explore (NY). 2017;13(1):26–45.
35. Kinser P, Braun S, Deeb G, Carrico C, Dow A. “Awareness is the first step”: An
interprofessional course on mindfulness & mindful-movement for healthcare professionals and students. Complement Ther Clin Pract. 2016 Nov;25:18–25.