1
Abstract
HIV has had a devastating impact on communities around the world since its emergence as an epidemic in the early 1980s. Today, over 1.1 million Americans are living with HIV, with new infection rates remaining relatively stable overall, yet increasing in certain vulnerable populations. Over 35,000 North Carolinians live with HIV, with adults between the ages of 20 to 29, gay and bisexual men, and African Americans being disproportionately affected.
Historically, HIV prevention has centered around behavioral risk reduction, including the promotion and utilization of condoms as risk reduction strategies. Emtricitabine-tenofovir (brand name Truvada®) was the first antiretroviral medication approved by the United States Food and Drug Administration (FDA) for pre-exposure prophylaxis (PrEP) as a new evidence-based prevention strategy. In clinical trials, emtricitabine-tenofovir/PrEP was shown to reduce the risk of acquiring HIV by approximately 90 percent in participants who took the medication as indicated.
Emtricitabine-tenofovir/PrEP is prescribed to HIV-negative patients who are at a high risk for becoming infected with HIV. These include gay and bisexual males, individuals with multiple sexual partners, transgender women, injection drug users, and people with an HIV-positive partner, among others. Multiple clinical studies have concluded that there is no significant change in sexual behaviors, nor are there significant increases in rates of sexually transmitted infection in patient populations regularly taking emtricitabine-tenofovir/PrEP.
Cost is a huge barrier to emtricitabine-tenofovir/PrEP access. Gilead, the maker of Truvada® (emtricitabine-tenofovir/PrEP), offers an Advancing Access Program, aimed at assisting with co-pay costs. The company also offers a Medication Assistance Program which provides emtricitabine-tenofovir/PrEP free of charge to those without health insurance. Primary care provider awareness is also a barrier to access, with many primary care providers reporting being unaware of emtricitabine-tenofovir/PrEP or not feeling comfortable prescribing it.
Mecklenburg and Durham counties, two of the top seven North Carolina counties that have the highest average rates of new HIV infections, offer referrals for
emtricitabine-tenofovir/PrEP. Patients can obtain prescriptions through their primary care doctor. Telemedicine options, like PlushCare, also exist as a convenient and discreet alternative.
2
Introduction
The goal of this paper is to discuss the status of HIV in the United States and North Carolina,
with emphasis on pre-exposure prophylaxis (PrEP) as a new evidence-based prevention
strategy. This is accomplished through discussion of the clinical trial background of
emtricitabine-tenofovir/PrEP, as well as the effects of its expanded use on rates of other
sexually transmitted infections. Additionally, prescribing concerns, as well as policy
considerations, implications, and consequences within North Carolina are discussed.
HIV: The Emergence of the Epidemic
In its June 5, 1981 edition of Morbidity and Mortality Weekly Report (MMWR), the
United States Centers for Disease Control and Prevention (CDC) reported cases of Pneumocystis
pneumonia, a rare form of pneumonia, among five young gay men in Los Angeles, California.
The following month, the CDC issued another MMWR indicating an unusually odd increase in
reports of Kaposi’s Sarcoma, a rare form of skin cancer, in young gay men (Kaiser Family
Foundation, 2018). In 1982, the CDC created the term Acquired Immune Deficiency Syndrome
(AIDS) to describe the phenomenon, identifying male homosexuality, intravenous drug abuse,
Haitian origin, and hemophilia A as risk factors, although these factors were later discredited.
Health care professionals, as well as reporters in the media, also referred to the disease as
“gay-related immune-deficiency” (GRID) due to the incorrect inherent link between AIDS and
homosexual sexual activities (Kaiser Family Foundation, 2018). In 1983, the U.S. Public Health
Service issued recommendations regarding prevention through sexual contact and blood
3
1984, Dr. Robert Gallo of the U.S. National Cancer Institute and Dr. Luc Montagnier of the
Pasteur Institute held a joint press conference announcing their discoveries that a retrovirus,
later named Human Immunodeficiency Virus (HIV), was the cause of AIDS (Kaiser Family
Foundation, 2018). By the end of that year, there had already been over 7,500 reported AIDS
cases in the United States, with more than 3,500 deaths (Avert, 2018).
HIV Today in the United States
In 2017, the CDC released its most recent HIV Surveillance Report which estimated that
as of 2015, over 1.1 million Americans over the age of 13 were living with HIV, 15 percent
whose infections had not yet been diagnosed (Centers for Disease Control, 2017). The number
of annual new infections was largely stable from 2012 to 2016, although variations in trends
were observed. HIV infections decreased among Americans aged 13–24, 35–44, and 45–54.
Decreases were also observed in women, as well as heterosexual males (Centers for Disease
Control, 2017). HIV infections remained stable among persons ≥55 years, as well as bisexual
and homosexual males as an entire group, but there was considerable variation by race and
ethnicity.
Between 2012 and 2016, HIV diagnoses among white gay and bisexual men decreased
14 percent, remained the same among African American gay and bisexual men, and increased
12 percent among Hispanic and Latino gay and bisexual men. African Americans, Hispanics, and
Latinos constitute an approximate 31 percent of the US population yet represent 69 percent of
all new HIV infections (Centers for Disease Control, 2019). Based on current infection rates, an
4
become infected with HIV during their lifetime (Gilead Sciences, 2018). These disproportionate
rates have been attributed to stigma, fear, discrimination, and homophobia among African
Americans, and poverty, migration patterns, lower educational level, and language barriers
among Hispanics and Latinos (Centers for Disease Control, 2019).
HIV Today in North Carolina
As of December 31, 2017, there were over 35,000 North Carolinians diagnosed and
living with HIV; 1,310 of these were diagnosed that year, representing a slight decrease in the
overall rate of new infections compared to 2016 (North Carolina Department of Health and
Human Services, 2018). Like trends seen nationally, North Carolinians between ages 20 and 29
years old had the highest rates of newly diagnosed HIV in 2017, making up 41.0 percent of the
newly diagnosed population. African Americans represented 64.8 percent of all new HIV
infections, with African American men, specifically, experiencing the highest rates of infection
(North Carolina Department of Health and Human Services, 2018). Gay and bisexual men
accounted for 64.5 percent of new HIV diagnoses, while heterosexuals accounted for 29.8
percent. Injection drug use only comprised 3.4 percent of new infections (North Carolina
Department of Health and Human Services, 2018). The top seven North Carolina counties,
ranked from highest to lowest average new HIV infection rates from 2015 to 2017, were
Mecklenburg, Edgecombe, Guilford, Bertie, Cumberland, Durham, and Pitt counties,
representing a range of urban and rural counties (North Carolina Department of Health and
5
Table A: 2015-2017 Annual Average Newly Diagnosed HIV Cases (per 100,000 residents)
Rank North Carolina County Newly Diagnosed HIV Cases (per 100,00 residents)
1 Mecklenburg 31.4
2 Edgecombe 29.2
3 Guilford 29.1
4 Bertie 28.9
5 Cumberland 27.1
6 Durham 26.8
7 Pitt 22.9
Adapted from North Carolina Department of Health and Human Services, 2018
Historical Prevention Strategies
HIV prevention strategies have historically centered around prevention of virus
transmission by means of behavior risk reduction methods. Most commonly, the use of
condoms for anal and vaginal sexual intercourse is encouraged based on the low cost of
condoms per unit, the overall familiarity, and the ease of access (Bertozzi et al., 2006).
Condoms are effective at preventing the transmission of HIV and other sexually transmitted
infections, as the materials used to make them physically block the transmission of the virus,
although they are prone to breakage, slippage, and leakage during sexual intercourse (Holmes,
Levine, and Weaver, 2004). A 2018 study set out to determine the per-partner condom
effectiveness against HIV for gay and bisexual men, using logistic regression to estimate the
HIV-6
positive and the other was HIV-negative, in both condom-protected receptive anal intercourse
and condom-less/unprotected receptive anal intercourse (Johnson, O’Leary, and Flores, 2018).
In calculating condom failure rates due to physical failure, as well as incorrect usage, the
researchers concluded that the increase in odds of new HIV infection per HIV-positive partner
for receptive anal intercourse was reduced by 91 percent for each partner with whom condoms
were always used (Johnson, O’Leary, and Flores, 2018).
A different study in 2015 used data from American participants in the 1999-2001
EXPLORE trial and the 1998-1999 VAX 004 trial data sets (Smith, Herbst, Zhang, and Rose,
2015). Researchers suggested that condom success rates were typically calculated based on
heterosexual sexual activities, so they wanted to derive an estimate of condom effectiveness
during anal sex for gay and bisexual men. The study found that among gay and bisexual men
reporting consistent condom use with an HIV-positive partner, there was a 70 percent
effectiveness of condoms with consistent use at preventing HIV transmission. The study also
found that only 16 percent of the participants reported consistent condom use during anal sex
with male partners, irrespective of their HIV status (Smith, Herbst, Zhang, and Rose, 2015). Both
studies show that condoms do not provide complete coverage or protection from HIV and are
prone to misuse and failure but are undoubtedly a fundamental piece of HIV prevention
strategies.
Regular sexually transmitted infection screening is also a means of HIV prevention.
Sexually transmitted infections increase one’s vulnerability for acquiring HIV, so early detection
and treatment might play a protective role in reducing the likelihood of HIV infection (Centers
7
are most infectious due to high viral loads prior to intake of antiretroviral therapy. These
individuals are also the most at risk for not knowing they are infected, and as such, may be
unknowingly passing on the virus to other sexual partners. Once they are identified as
HIV-positive, they can begin taking antiviral medication, bringing their viral load to undetectable
levels, meaning they will not transmit the virus to other individuals (Centers for Disease
Control, 2017). This conclusion, after years of data analysis and multiple supporting studies, has
sparked the U=U (undectable=untransmittable) educational movement, aimed at additional
patient awareness. Ultimately, the goal is that there will be additional patient compliance with
HIV medication adherence, thereby reducing community viral load and reducing overall
population level incidence (Calabrese and Mayer, 2019).
PrEP: The New Frontier in HIV Prevention
Pre-exposure prophylaxis (abbreviated as ‘PrEP’) has emerged as an important modality
to prevent HIV infection, as the search for an HIV vaccine continues. PrEP refers to
antiretroviral medication that is prescribed to HIV-negative patients at risk of HIV infection to
lower their risk of infection (Pebody, 2015). Antiretroviral medications have traditionally been
prescribed to an HIV-negative person immediately after possible exposure to HIV (known as
post-exposure prophylaxis, PEP), to an HIV-positive woman during pregnancy and childbirth
(known as prevention of mother-to-child transmission, PMCT), as well as by an HIV-positive
person as treatment (known as treatment as prevention, TasP) (Pebody, 2015). In 2012,
Truvada® (emtricitabine-tenofovir) was the first antiretroviral medication approved by the U.S.
8
Truvada® was approved based on its overall safety profile and efficacy, with patients reporting
limited adverse events, most commonly short-term nausea, tiredness, gastrointestinal
disruption, and headaches. Adverse events were reported by less than ten percent of patients,
with most resolving in the first few weeks of taking Truvada® (Pebody, 2015).
PrEP Clinical Background and Evidence
iPrEx Clinical Study
The multinational Preexposure Prophylaxis Initiative (iPrEx) trial of
emtricitabine-tenofovir was open for enrollment from 2007 to 2009 at 11 investigative sites in six different
countries. The study enrolled 2,499 HIV-negative men or transgender women who have sex
with men, randomly assigning the subjects into a placebo arm or an
emtricitabine-tenofovir/PrEP arm (Grant et al., 2010). Study visits occurred once monthly and included drug
dispensation and accountability, drug adherence counseling, testing for HIV antibodies, and
medical history review. At these monthly visits, study participants were also provided condoms
and counseled on risk-reduction strategies, specifically being instructed to protect themselves
from HIV through traditional means. Participants also had behavioral risk assessments
performed once every 12 weeks, and full physical examinations and evaluations for sexually
transmitted infections performed every 24 weeks (Grant et al., 2010). If participants tested
positive for any sexually transmitted infections, they and their sexual partners were offered
treatment. Participants with known exposure to HIV through an HIV-positive partner were
discontinued from study medication temporarily (in the event they were on placebo) and
9
During the study, investigators noted similar sexual practices between the placebo and
active emtricitabine-tenofovir/PrEP groups, although all groups showed a decrease in the
number of sexual partners and an increase in condom usage following study enrollment, as
compared to before enrollment (Grant et al., 2010). Elevated serum creatine levels were noted
in many participants, along with participant-reported nausea and unintentional weight loss.
HIV infections were detected in 110 participants, although ten were detected at the first
enrollment visit prior to beginning emtricitabine-tenofovir/PrEP or placebo. Thirty-six
infections were observed in the emtricitabine-tenofovir/PrEP group, and 64 were observed in
the placebo group, representing a 44 percent relative reduction of HIV incidence, or 44 percent
of additional protection. Investigators noted that participant reported pill use was high, but
laboratory testing for drug exposure was substantially lower (Grant et al., 2010). This lower
drug adherence was suspected as the reasoning for the lower than expected reduction in HIV
incidence. The successful results from the trial, as well as the drug’s overall safety profile,
prompted the U.S. FDA to approve combination emtricitabine-tenofovir for market in 2012,
branded Truvada® by Gilead Sciences.
PROUD Clinical Study
The PROUD study was a clinical trial in the United Kingdom that recruited gay and
bisexual men who were HIV-negative but had had unprotected anal intercourse at least once in
the previous 90 days (McCormack et al., 2015). After the results of the previously discussed
iPrEx study, researchers wanted to determine if the benefit from emtricitabine-tenofovir as
10
was uncontrolled and open-label, meaning all participants were on known active medication
and not placebo, although they were randomized to either begin receiving
emtricitabine-tenofovir/PrEP immediately at enrollment or after a deferral period of one year (McCormack et
al., 2015). Participants returned to the investigational clinic every three months where they
were given an HIV test, as well as a screening for bacterial sexually transmitted infections;
Hepatitis C screening was performed for participants who reported higher risk activities like
snorting drugs or the use of sex toys. After the visits, participants were given sufficient
emtricitabine-tenofovir/PrEP to cover them one month after their next expected clinic visit.
Routine safety bloodwork was also performed, including serum creatine laboratory work
(McCormack et al., 2015).
Overall, 544 participants were enrolled, with 275 assigned to the group immediately
receiving emtricitabine-tenofovir/PrEP, while 269 were assigned to the deferred group. Twenty
participants developed new HIV infections in the deferred group, while only three occurred in
the immediate group. In the immediate group, one of the participants tested positive at their
four-week visit, suggesting that infection started prior to beginning
emtricitabine-tenofovir/PrEP, based on the provided sexual history. The second participant was identified as
HIV-positive at 61 weeks but had not been prescribed emtricitabine-tenofovir/PrEP since the
enrollment visit. The third participant seroconverted at 53 weeks but had last attended the
clinic at 12 weeks, where he was prescribed only 90 tablets of study drug. Altogether, these
findings suggested no breakthrough HIV infections in participants on
emtricitabine-tenofovir/PrEP, while showing an 86 percent reduction in risk of HIV infection. Additionally,
11
infections, including rectal gonorrhea and chlamydia between the study arms (McCormack et
al., 2015).
IPERGAY Clinical Study
The Intervention Préventive de l’Exposition aux Risques avec et pour les Gays (IPERGAY)
study assessed the safety and efficacy of emtricitabine-tenofovir/PrEP in a sexual-activity
dependent manner among high-risk gay and bisexual men in France and Canada. The study
hypothesized that rate adherence (therefore efficacy) might be higher if dosing was dependent
on sex, as opposed to a daily regimen (Molina et al., 2015). Researchers recruited HIV-negative
males and transgender females who have sex with gay or bisexual men who were considered
high-risk based on having a history of unprotected anal sex with at least two partners in the six
months preceding screening. Participants were randomized in a 1:1 ratio to either receive
emtricitabine-tenofovir/PrEP or placebo. Placebo use was justified based on inconsistent
efficacy in previous trials, as well as the moderate efficacy of emtricitabine-tenofovir as
pre-exposure prophylaxis in the iPrEx trial although the results of these trials are now attributed to
poor drug adherence (Molina et al., 2015).
Study participants were instructed to take two pills (emtricitabine-tenofovir/PrEP or
placebo) 2 to 24 hours prior to engaging in sexual activity, followed by a third pill 24 hours after
the first pill, and then a fourth pill 24 hours after the third. Participants engaging in multiple
consecutive sexual acts were advised to take one pill per day until the last sexual encounter,
and to then take two post-exposure pills. Following enrollment, participants returned to the
12
accountability, biochemical analyses, as well as diagnosis of different sexually transmitted
infections. Participants completed questionnaires at home prior to each visit to assess
information on use of alcohol and recreational drugs, sexual behavior, as well as their
adherence to taking the pills during recent sexual intercourse (Molina et al., 2015).
In analyzing drug adherence, researchers concluded that 28 percent of participants did
not take emtricitabine-tenofovir/PrEP or placebo, 29 percent took the assigned drug at a
suboptimal dose, and 43 percent took the assigned drug correctly (Molina et al., 2015). Sexual
activity levels remained largely consistent during the study, compared to baseline, in both the
placebo and emtricitabine-tenofovir/PrEP groups. Additionally, there were no significant
differences between the groups in instances of higher risk sexual activities such as receptive
anal intercourse without condoms, or the overall proportion of condom-less anal sex (Molina et
al., 2015). Proportions of participants who acquired new sexually transmitted diseases of the
throat, anus, and urinary tract combined also remained similar between groups during
follow-up. Of those with a new infection, 39 percent were rectal infections, with 20 percent of all
subjects acquiring chlamydia, 22 percent acquiring gonorrhea, and 10 percent acquiring syphilis
during follow-up (Molina et al., 2015).
HIV infection was documented in 19 participants, although three of these occurred
between the screening/enrollment visit and randomization. Two participants in the
emtricitabine-tenofovir/PrEP group became infected with HIV, while 14 participants in the
placebo group became infected, indicating an overall relative reduction in incidence of HIV
acquisition in the emtricitabine-tenofovir/PrEP group of 86 percent (Molina et al., 2015). The
13
returned 60 and 58 pills, out of the 60 administered, and were therefore deemed to be
non-adherent, increasing their risk of acquiring HIV (Molina et al., 2015).
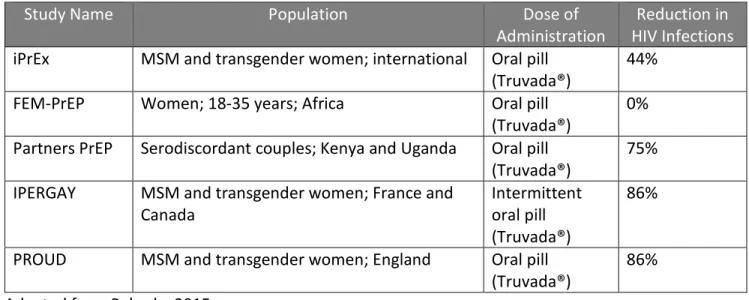
Table B: PrEP Clinical Study Summary
Study Name Population Dose of
Administration HIV Infections Reduction in
iPrEx MSM and transgender women; international Oral pill
(Truvada®) 44% FEM-PrEP Women; 18-35 years; Africa Oral pill
(Truvada®) 0% Partners PrEP Serodiscordant couples; Kenya and Uganda Oral pill
(Truvada®) 75% IPERGAY MSM and transgender women; France and
Canada Intermittent oral pill
(Truvada®)
86%
PROUD MSM and transgender women; England Oral pill
(Truvada®) 86% Adapted from Pebody, 2015
Prescribing Requirements and Concerns
Combined with safer sex practices, emtricitabine-tenofovir (Truvada®) is recommended
to reduce the risk of HIV infection in individuals at higher risk for HIV acquisition by the U.S.
CDC, the World Health Organization (WHO), the American College of Obstetricians and
Gynecologists, as well as the International Antiviral Society-USA (Gilead Sciences, 2018).
Physicians are encouraged to screen patients to identify those who might be at higher risk for
HIV acquisition using a variety of clinical, sexual, and circumstantial risk factors. Clinical risk
factors might include a patient requesting testing for sexually transmitted infections, being
14
prophylaxis (PEP). Sexual risk factors would include multiple sexual partners, non-monogamous
relationships, sexual activity in high HIV-prevalent areas or networks, as well as use of dating
and “hook up” apps, such as Grindr or Tinder. Circumstantial risk factors include exchanging
sex for commodities, recreationally abusing drugs and alcohol, domestic violence or sexual
assault situations, or having a partner who is incarcerated, using injecting drugs or already
HIV-positive (Gilead Sciences, 2018).
Emtricitabine-tenofovir (Truvada®) can be prescribed for pre-exposure prophylaxis once
an individual has been confirmed to be HIV-negative immediately before use and does not have
any signs or symptoms that might suggest acute HIV infection. Patients are expected to have
HIV testing at least every 3 months while on Truvada®, as well as re-testing at any point if the
patient is diagnosed with a different sexually transmitted infection (Gilead Science, 2018).
Renal monitoring is also recommended, given the creatine safety findings observed in prior
clinical studies. Physicians are also recommended to counsel patients on safer sex practices,
including the regular use of condoms, as well as the importance of taking the medication every
day, as prescribed, for efficacy reasons. Failure to properly adhere to the medication regimen
will decrease the protective effects of emtricitabine-tenofovir (Truvada®), as shown in the
FEM-PrEP trial in which women across Africa reported regular drug adherence (despite blood plasma
15
Effects of Expanded PrEP Use
Behavior Changes Resulting in Increased Incidence of Non-HIV Sexually
Transmitted Infections
The CDC’s 2017 Sexually Transmitted Disease Surveillance Report revealed that rates of
chlamydia, gonorrhea, and syphilis have increased consistently in recent years, yet one of the
biggest concerns regarding the expanded use of pre-exposure prophylaxis is that it will result in
behavioral disinhibition (i.e. condom-less sex when otherwise condoms might have been used)
and thereby increase the rates of other sexually transmitted infections (Centers for Disease
Control, 2018). As previously discussed, the IPERGAY and PROUD studies analyzed whether or
not emtricitabine-tenofovir/PrEP had any changes on the incidence of other sexually
transmitted infections or modified the sexual behaviors of study participants. Participants in
both studies were considered high-risk based on their reported sexual practices, including
having unprotected anal intercourse with multiple sexual partners. Participants in the PROUD
study were at higher risk for HIV acquisition given their reported number of sexual partners,
histories of recreational alcohol and drug abuse, as well as their prior use of post-exposure
prophylaxis (PEP) after suspected contact with an HIV-positive sexual partner (Pebody, 2015).
Despite the higher than average risk in the groups, results from the IPERGAY and PROUD
studies both suggested that taking emtricitabine-tenofovir/PrEP did not result in any significant
behavior changes, nor did it result in a specific increase in incidence of other sexually
16
PrEP Effects on Gonorrhea and Chlamydia Rates
The CDC conducted a joint modeling study with Emory University’s Rollins School of
Public Health to evaluate whether emtricitabine-tenofovir/PrEP, along with the recommended
follow-up testing for sexually transmitted infections, could reduce not just HIV incidence, but
also chlamydia and gonorrhea incidence (Centers for Disease Control, 2017). CDC analysts
estimate that there are approximately 492,000 sexually active gay and bisexual men in the
United States that are at substantial risk of HIV infection and could benefit from starting
emtricitabine-tenofovir/PrEP. Using this number, as well as estimates from data that some men
might reduce their usage of condoms while taking emtricitabine-tenofovir/PrEP, researchers
created a model to forecast the number of new cases of gonorrhea and chlamydia that could be
prevented if 10 to 90 percent of emtricitabine-tenofovir/PrEP-eligible gay and bisexual men in
the U.S. started taking emtricitabine-tenofovir/PrEP and had routine sextually transmitted
infection testing every six months, as minimally recommended by the CDC.
Forecasts from the model showed that more than 40 percent of chlamydia infections
and 42 percent of gonorrhea infections could be prevented over the next ten years if just 40
percent of emtricitabine-tenofovir/PrEP-eligible gay and bisexual men started taking
emtricitabine-tenofovir/PrEP and were tested twice a year for sexually transmitted infections. A
reduction of this magnitude would occur even in the presence of a 40 percent reduction in
condom usage among men while taking emtricitabine-tenofovir/PrEP. Reduction was attributed
to early detection of sexually transmitted infections that frequently have a delay in diagnosis,
resulting in delayed treatment and transmission to sexual partners. The model also showed that
17
emtricitabine-tenofovir/PrEP users, indicating the importance of appropriate medical care and
management of individuals who may be at higher risk for HIV acquisition. In contrast to the
conclusions done with real world-data by researchers at the LGBT health center in New York
and the San Francisco Department of Public Health, Emory and CDC researchers determined
than increasing testing for sexually transmitted infections from two to four times per year
would only reduce new gonorrhea and chlamydia cases by five percent.
Centers for Disease Control Guidelines for Sexually Transmitted Infection Testing
Frequency
Current CDC guidelines recommend sexually active gay and bisexual men be tested at
least once a year for syphilis, chlamydia, and gonorrhea, while those with multiple partners be
tested at more regular intervals, such as every three to six months (Centers for Disease Control,
2014). The CDC also advises that sexually active gay and bisexual men might benefit from HIV
testing every three to six months (Centers for Disease Control, 2014). Prescriber
recommendations state that patients active on emtricitabine-tenofovir/PrEP be tested for HIV
every three months, and at these appointments, providers often choose to do a full screening
panel for other sexually transmitted infections (Gilead Sciences, 2018).
To evaluate the effectiveness of the CDC’s guidelines, researchers at the largest LGBT
health center in New York City analyzed medical records of 280 patients on
emtricitabine-tenofovir/PrEP, analyzing their sexually transmitted infection data in the six months before, as
well as their 12-months after beginning emtricitabine-tenofovir/PrEP. In their study, 21 percent
18
infection in the six months before starting emtricitabine-tenofovir/PrEP, including 11 percent
who were positive for a sexually transmitted infection at their appointment where they
received their first emtricitabine-tenofovir/PrEP prescription (Golub et al., 2016). At the first
follow-up appointment (three months after starting emtricitabine-tenofovir/PrEP), 13 percent
of patients were diagnosed with a sexually transmitted infection; 77 percent of those were
asymptomatic and were diagnosed because of routine screening. After analyzing patient data
through the nine-month follow-up visit, researchers determined that following the minimum
CDC guidelines would have delayed diagnosis and treatment for 24 percent of patients,
including 40 different cases of a rectal sexually transmitted disease and three cases of syphilis
(Golub et al., 2016).
Researchers at the San Francisco Department of Public Health also evaluated sexually
transmitted infection testing frequency in a study analyzing 557 gay, bisexual, and transgender
woman patients on emtricitabine-tenofovir/PrEP between October 2012 and January 2014. In
their study, 50.9 percent of participants were diagnosed with one or more sexually transmitted
infection during the follow up period (Cohen et al., 2016). If clinicians had relied on just
semi-annual testing or based on symptomatic reporting, 34.3 percent of patients with gonorrhea,
41.0 percent of patients with chlamydia, and 20.4 percent of patients with syphilis would have
been undiagnosed, extending their period of infectivity by up to three months for each case.
These numbers lead the researchers to conclude that sexually transmitted infection testing
every three months, even in the absence of symptoms, will significantly increase detection of
19
diagnosis and treatment in sexual partners, as well as a subsequent decrease in sexually
transmitted infection prevalence (Cohen et al., 2016).
PrEP Accessibility
Cost
One of the biggest barriers to emtricitabine-tenofovir/PrEP access is its financial cost.
Without insurance, emtricitabine-tenofovir/PrEP costs approximately $2,000 for a 30-day
supply (Luthra and Gorman, 2018). To assist with the high cost, Gilead Sciences, the maker of
Truvada® (emtricitabine-tenofovir/PrEP) runs the Gilead Advancing Access Program which
provides up to $7,200 in annually in co-pay coupons to those with commercial insurance
(Gilead Sciences, 2019). The Advancing Access Program is not available for anyone who has
health insurance through a government program such Medicare Part D, Medicaid, TRICARE, or
VA-care, although Gilead will assist these patients in looking for grants and alternative funding
sources. For patients without health insurance, Gilead operates the Medication Assistance
Program which provides emtricitabine-tenofovir/PrEP at no charge to those who are eligible
(Gilead Sciences, 2019).
Primary Care Provider Awareness
Primary care providers act as the frontline for patients’ medical concerns, typically being
where patients go for annual wellness visits and health screenings, including screenings for
sexually transmitted infections. Although there has been an increase in
20
groups at higher risk for HIV acquisition, a recent study that set out to assess the comfortability
and prescribing behaviors of primary care providers in the U. S. found that just 76% reported
being aware of emtricitabine-tenofovir/PrEP. Of those, only 28% reported being somewhat or
very familiar prescribing it (Petroll et al., 2017). For primary care providers that discussed
emtricitabine-tenofovir/PrEP with at-risk patients, 60% of the conversations were initiated by
the patient, not the provider. Overall, only 17% of the sampled primary care providers reported
ever prescribing PrEP (Petroll et al., 2017). The same study showed significantly higher rates
among HIV specialists, but given the prophylactic nature of the medication, many patients
might not directly seek out an HIV specialist for treatment.
North Carolina County Public Health Agency Referrals
Mecklenburg, Edgecombe, Guilford, Bertie, Cumberland, Durham, and Pitt counties
experienced the highest average rates of new HIV infections in North Carolina from 2015 to
2017 (North Carolina Department of Health and Human Services, 2018). Of these counties, only
Mecklenburg and Durham counties advertise emtricitabine-tenofovir/PrEP referral partners to
individuals looking for a prescription who otherwise use the county health department for
various services (Mecklenburg County Health Department, 2019; Durham County Department
of Public Health, 2019). In 2018, the Mecklenburg County Health Department implemented a
emtricitabine-tenofovir/PrEP pilot project aimed at providing emtricitabine-tenofovir/PrEP to
320 high-risk uninsured individuals. This will be accomplished through the county’s contracts
21
areas with high-risk individuals. Enrollment is ongoing, and no interim results are available
currently (Mecklenburg County Health Department, 2019).
Other public health departments across the state offer emtricitabine-tenofovir/PrEP
referrals on an intermittent, inconsistent basis. Depending on the county, individuals seeking a
referral are better poised to reach out directly to their primary care provider. This would
include sexual minorities and particularly vulnerable populations. Similar barriers to accessing
overall general medical care are also applicable for those seeking a
emtricitabine-tenofovir/PrEP prescription, namely that without an established primary care provider, it is
considerably more challenging.
Telemedicine Options
Patients seeking additional confidentiality or convenience, or who lack access to a local
physician, can acquire an emtricitabine-tenofovir/PrEP prescription through telemedicine
provider PlushCare, which operates in 31 states and is the largest virtual medicine provider of
emtricitabine-tenofovir/PrEP (PlushCare, 2017). PlushCare allows patients to meet with
physicians over the phone and through video chatting. Patients seeking to participate in
PlushCare’s PrEP treatment program schedule a virtual consult with the physician who reviews
the patient’s medical history, assess risk and overall eligibility, and then coordinates HIV and
sexually transmitted infection screening at laboratories near the patients’ home, often those
operated by national companies like LabCorp and Quest Diagnostics (PlushCare, 2017). If the
patient’s tests come back negative for HIV and the patient otherwise meets the clinical criteria,
22
patient’s preferred local pharmacy. Patients are then reminded to schedule a follow-up
appointment for a prescription refill which requires another consultation with a physician, as
well as repeated testing for sexually transmitted infections (PlushCare, 2017). For patients with
commercial health insurance, consultations with a PlushCare physician are billed as a primary
care visit and typically cost less than $20 per visit, although the exact rate will depend on the
insurance plan. For those without health insurance, PlushCare charges $99 per visit (PlushCare,
2019).
Policy Considerations
Statewide Access Program
The North Carolina Department of Health and Human Services relies on local county
health departments to provide free STI and HIV prevention and control services, including
education and awareness efforts, surveillance, and epidemiology (North Carolina Department
of Health and Human Services, 2019). No statewide assistance programs for
emtricitabine-tenofovir/PrEP currently exist, although they have been piloted in other states and
municipalities and could be modeled or implemented on a smaller level within North Carolina.
California launched the AIDS PrEP Assistance Program, aimed at helping Californians
who are uninsured, insured but have high out of pocket costs, as well as those who are insured
with a high deductible plan (California Department of Public Health, n.d.). Uninsured patients
whose medication costs are covered through the Gilead Advancing Access Program still face the
challenge of paying for the required laboratory and clinical visits; in these cases, the PrEP
23
care. For those with insurance who meet eligibility requirements, the PrEP Assistance Program
will provide funding for co-pays, as well as medication costs after the $7,200 co-pay coupons
offered through the Gilead Advancing Access Program (California Department of Public Health,
n.d.). Although funding challenges and the political climate would make such a comprehensive
program challenging to implement, taking such comprehensive steps would allow North
Carolina to lead the nation in emtricitabine-tenofovir/PrEP usage, particularly in vulnerable
populations.
County-Level Education and Outreach Efforts
At the state level, North Carolina could expand its emtricitabine-tenofovir/PrEP
awareness and education outreach efforts. This could include redirecting funds towards
counties which experience the highest rates of infections, empowering those counties to direct
resources to the highest risk populations locally. As evidenced by the lack of
emtricitabine-tenofovir/PrEP referrals in five of the seven most affected counties, there is considerable room
for improvement.
Furthermore, county-wide social marketing campaigns could be set up that primarily
target increasing awareness among at-risk populations, and secondarily among physicians.
Beginning in 2014, New York City rolled out an advertising campaign for
emtricitabine-tenofovir/PrEP with slogans such as “share the night, not HIV” as well as “we play sure,
PrEP+condoms” (New York City Department of Health and Mental Hygiene, 2017). The city
placed these advertisements on subway cars, turnstiles, trash cans, and billboards, including in
24
well as the gay dating apps Grindr, Scruff, and Jack’d (New York City Department of Health and
Mental Hygiene, 2017). Counties within North Carolina could adopt a similar approach, tailoring
their advertisement mediums and locations to vulnerable populations.
Conclusion
Despite decades of progress with HIV research and prevention strategies, HIV rates
continue to increase or remain stable among various groups, emphasizing the need for current
evidence-based prevention and management strategies. The numerous studies done in recent
years, as presented here, have shown that emtricitabine-tenofovir as pre-exposure prophylaxis
is extremely effective at preventing HIV infection when taken as prescribed and will continue to
be a tool used by public health professionals and clinicians in the global fight against HIV.
Ranking among the top states in the nation by new HIV infection, North Carolina needs to
integrate emtricitabine-tenofovir/PrEP into its HIV reduction and management programs,
empowering local counties to act within at-risk communities, as well as expanding statewide
outreach and education programs, including social marketing efforts. Such action, because of
expanded use, will reduce North Carolina’s overall incidence rate of HIV and is also likely to
have a positive impact on statewide gonorrhea and chlamydia rates. Expanded use of
emtricitabine-tenofovir/PrEP will also complement efforts to mitigate HIV transmission among
25
References
Avert. (2018, November 26). History of HIV and AIDS Overview. Retrieved from https://www.avert.org/professionals/history-hiv-aids/overview
Bertozzi, S., Padian, N., & Wegbreit, J. (2006). Disease Control Priorities in Developing Countries. New York, NY: Oxford University Press.
Calabrese, S. K., & Mayer, K. H. (2019). Providers should discuss U=U with all patients living with HIV. Lancet HIV, 6(4). doi:10.1016/s2352-3018(19)30030-x
California Department of Public Health. (n.d.). California State Office of AIDS PrEP Assistance Program. Retrieved from http://www.californiaaidsresearch.org/files/PrEP-AP Info
Sheet_Final.pdf
Centers for Disease Control. (2014, June 30). Which STD Tests Should I Get? Retrieved from https://www.cdc.gov/std/prevention/screeningreccs.htm
Centers for Disease Control. (2016, May). CDC Fact Sheet: Proven HIV Prevention Methods. Retrieved from https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/hiv-proven-prevention-methods-508.pdf
Centers for Disease Control. (2017, September 27). Dear Colleague: September 27, 2017. Retrieved from https://www.cdc.gov/hiv/library/dcl/dcl/092717.html
Centers for Disease Control. (2017, February 15). Study Suggests STI Testing and Treatment as Part of PrEP Care May Reduce Bacterial STIs among Gay and Bisexual Men. Retrieved from https://www.cdc.gov/nchhstp/newsroom/2017/croi-prep-study.html
Centers for Disease Control. (2018, November). HIV Surveillance Report 2017. Retrieved from https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-report-2017-vol-29.pdf
Centers for Disease Control. (2018, November 1). HIV and Hispanics/Latinos. Retrieved from https://www.cdc.gov/hiv/group/racialethnic/hispaniclatinos/index.html
Centers for Disease Control. (2018, July). National Overview of STDs, 2017. Retrieved from https://www.cdc.gov/std/stats17/natoverview.htm
Centers for Disease Control. (2019, February 4). HIV and African Americans. Retrieved from https://www.cdc.gov/hiv/group/racialethnic/africanamericans/index.html
26
Project. Retrieved from http://www.croiconference.org/sessions/quarterly-sti-screening-optimizes-sti-detection-among-prep-users-demo-project-0
Durham County Department of Public Health. (2019). PrEP DCoDPH. Retrieved from http://dcopublichealth.org/services/std-hiv-testing/prep-dcodph
Gilead Sciences. (2018). Truvada for Pre-Exposure Prophylaxis Health Care Professional Site. Retrieved from
https://www.truvada.com/hcp/home?utm_medium=cpc&utm_campaign=2018_Truvada for PrEP HCP Branded&utm_content=Truvada - Prescribing - Broad&utm_term= truvada
prescribing&moc=5611000416&utm_source=google&gclid=Cj0KCQiAh9njBRCYARIsALJhQkG_Xv MmghaEkcClHVRMI9BKmcwzWoq-6rf99r02oqfvxBIMAPCngOMaArUgEALw_wcB&gclsrc=aw.ds
Gilead Sciences. (2019). Gilead Advancing Access Co-pay Support for the Commercially Insured. Retrieved from https://www.gileadadvancingaccess.com/hcp/financial-assistance/copay-support
Gilead Sciences. (2019). Truvada for PrEP Cost Assistance. Retrieved from https://www.truvada.com/how-to-get-truvada-for-prep/truvada-cost
Golub, S., Pena, S., Boonrai, K., Douglas, N., Hunt, M., & Radix, A. (2016, February 25). STI Data From Community-Based PrEP Implementation Suggest Changes to CDC Guidelines. Retrieved from
http://www.croiconference.org/sessions/sti-data-community-based-prep-implementation-suggest-changes-cdc-guidelines-0
Grant, R. M., Lama, J. R., Anderson, P. L., Mcmahan, V., Liu, A. Y., Vargas, L., . . . Glidden, D. V. (2010). Preexposure Chemoprophylaxis for HIV Prevention in Men Who Have Sex with Men. New England Journal of Medicine, 363(27), 2587-2599. doi:10.1056/nejmoa1011205
Holmes, K., Levine, R., & Weaver, M. (2004). Effectiveness of condoms in preventing sexually transmitted infections. Bulletin of the World Health Organization, 82(6), 454-461.
Johnson, W. D., O’Leary, A., & Flores, S. A. (2018). Per-partner condom effectiveness against HIV for men who have sex with men. AIDS, 32(11), 1499-1505.
doi:10.1097/qad.0000000000001832
Kaiser Family Foundation. (2018, July 20). Global HIV/AIDS Timeline. Retrieved from https://www.kff.org/global-health-policy/timeline/global-hivaids-timeline/
Luthra, S., & Gorman, A. (2018, July 6). Out-Of-Pocket Costs for PrEP Put the HIV Prevention Drug Out Of Reach For Many. Retrieved from
27
McCormack, S., Dunn, D., Desai, M., Dolling, D., Gafos, M., & Gilson, R. (2016). Pre-exposure prophylaxis to prevent the acquisition of HIV-1 infection (PROUD): Effectiveness results from the pilot phase of a pragmatic open-label randomised trial. Lancet, 387(10013), 53-60. doi:https://doi.org/10.1016/S0140-6736(15)00056-2
Mecklenburg County Health Department. (2019). HIV STD Surveillance PrEP. Retrieved from https://www.mecknc.gov/HealthDepartment/CDControl/HIVSTDSurveillance/Pages/PrEP.aspx
Molina, J., Capitant, C., Spire, B., Pialoux, G., Cotte, L., Charreau, I., . . . Delfraissy, J. (2015). On-Demand Preexposure Prophylaxis in Men at High Risk for HIV-1 Infection. New England Journal of Medicine, 373(23), 2237-2246. doi:10.1056/nejmoa1506273
New York City Department of Health and Mental Hygiene. (2017). Evaluating PrEP Social Marketing Campaigns: NYC ’s StaySure. Retrieved from
https://www1.nyc.gov/assets/doh/downloads/pdf/dires/evaluating-prep-social-marketing-campaigns.pdf
North Carolina Department of Health and Human Services. (2018). 2017 North Carolina HIV/STD/Hepatitis Surveillance Report. Retrieved from
https://epi.publichealth.nc.gov/cd/stds/figures/std17rpt_rev12142018.pdf
North Carolina Department of Health and Human Services. (2018, July 24). Communicable Disease Programs: HIV/STD Prevention and Care. Retrieved from
https://epi.publichealth.nc.gov/cd/stds/program.html
Pebody, R. (2015, July). PrEP Briefing Paper. Retrieved from
http://www.aidsmap.com/v635723833203470000/file/1187955/PrEP_briefing_paper.pdf
Petroll, A. E., Walsh, J. L., Owczarzak, J. L., Mcauliffe, T. L., Bogart, L. M., & Kelly, J. A. (2017). PrEP Awareness, Familiarity, Comfort, and Prescribing Experience among US Primary Care Providers and HIV Specialists. AIDS and Behavior, 21(5), 1256-1267. doi:10.1007/s10461-016-1625-1
PlushCare. (2017, November 30). PlushCare Adds PrEP Program. Retrieved from https://www.plushcare.com/blog/plushcare-launches-end-to-end-prep-treatment/
PlushCare. (2019). PrEP Online with PlushCare. Retrieved from https://prep.plushcare.com/
Smith, D. K., Herbst, J. H., Zhang, X., & Rose, C. E. (2015). Condom Effectiveness for HIV Prevention by Consistency of Use Among Men Who Have Sex With Men in the United States. JAIDS Journal of Acquired Immune Deficiency Syndromes, 68(3), 337-344.
28