Developing Collaborative Maternal and Child Health Leaders
An Evaluation of the National Maternal and Child Health
Workforce Development Center
Alina Clarke
Undergraduate Honors Thesis
Health Policy and Management
University of North Carolina at Chapel Hill
2015-2016
Advisors:
Dr. Dorothy Cilenti
Clinical Assistant Professor
Director, National Maternal and Child Health Workforce Development Center
Department of Maternal and Child Health
Gillings School of Global Public Health
University of North Carolina at Chapel Hill
Dr. Karl Umble
Clinical Assistant Professor
Director, Bachelor of Science in Public Health Program
Department of Health Policy and Management
TABLE OF CONTENTS:
Abstract
3
Introduction
4
Evaluation Questions
5
Background
8
Methods
14
Results
17
Discussion
25
Appendix
30
ABSTRACT:
Public health agencies have invested in leadership development programs across the
local, state, and federal levels to strengthen infrastructure, programming, and outcomes by
training leaders and enhancing their relevant skillset. Collaboration is especially important to
solve systemic challenges affecting the public’s health, including maternal and child health
(MCH) populations. While there is ample literature on leadership development for MCH
professionals, few publications present evaluations of the impacts of collaborative leadership
development specific to MCH programs.
To assess the development and use of collaborative leadership practices by MCH
professionals, an evaluation of the National Maternal and Child Health Workforce Development
Center (the Center) was conducted to investigate 1) the effects of the Center’s training on the use
of collaborative leadership practices by MCH leaders, and 2) perceived barriers to collaborative
leadership for MCH leaders. This case study compared interview responses from a sample of the
Center’s participants and findings from a document review of the training curriculum with an
existing framework of collaborative leadership themes to identify gaps and opportunities for
improvement.
Key findings showed Systems Thinking and Process-based Leadership to be well covered
by the Center’s intensive cohort training, while Power Sharing emerged as a key area for
improvement. Perceived barriers to sustaining collaborative work included: 1) a tendency for
state agencies to have siloed priorities, 2) difficulty achieving a consensus to move a project
forward without individual partners disengaging, 3) strained organizational partnerships when
the individual representative leaves that partnering organization, and 4) difficulty in sustaining
INTRODUCTION:
Problem Statement
Over the past three decades, public health agencies and scholars in the United States have
focused on leadership development and training in order to strengthen leaders’ capacity to
improve public health infrastructure and health outcomes.1–3 Institutes for public health
leadership development were established throughout the local, state and federal levels over the
past 25 years, and extensive evaluation of leadership training has been highly valued.2,3
Multi-sector collaboration has emerged as a key tool to address the multifaceted,
systemic challenges that contribute to poor health.4,5 Leading by convening can be more effective
than traditional hierarchal leadership roles to manage these partnerships.4,5 Collaborative
leadership methods, such as systems thinking, vision-based leadership, collateral leadership,
power sharing, and process-based leadership, have been shown to be particularly beneficial when
implemented in health settings.4 Collaborative leaders can strengthen inter-organizational
relationships, create coalitions, foster long-term community partnerships, and ultimately impact
services, programs, policies and health outcomes.5–8
Collaborative leadership skills are also important for maternal and child health (MCH)
professionals, and are represented in the core competencies for MCH leaders.9 While there is
ample literature on leadership development for MCH professionals, few publications present
evaluations of the impacts of collaborative leadership development specific to MCH programs.10–
12 This evaluation of one aspect of the National Maternal and Child Health Workforce
Development Center at the University of North Carolina at Chapel Hill (the Center) will serve as
questions: 1) What are the effects of the Center’s leadership training and development on the use
of collaborative leadership practices by MCH leaders? 2) What are perceived barriers to
collaborative leadership for MCH leaders?
The National Maternal and Child Health Workforce Development Center (the Center)
The Maternal and Child Health Bureau (MCHB) of the Health Resources and Services
Administration funded the establishment of the Center at the University of North Carolina at
Chapel Hill, Department of Maternal and Child Health in 2013. With this program, the MCHB
sought to strengthen the capacity of the MCH workforce to respond to the current environment
of health transformation stemming from nationwide health reform and a shift in focus from
disease management to population health. The Center provides services to strengthen MCH
professionals’ skills in four critical Cores: Access to Care, Change Management, Quality
Improvement and Systems Integration. MCH program leaders that engage with the Center can
seek training in one of two ways: 1) Title V program leaders can seek the Center’s help in
developing an initial service plan for tailored assistance in one specific core area, or 2) States and
territories can join the intensive cohort training that includes personalized coaching, a quality
improvement adviser to assist in the development of a health transformation project, cohort
workshops, and collaborative learning in a shared environment. This study evaluates the use of
collaborative leadership practices by the Center’s Cohort 1 participants after undergoing
intensive cohort training.
Eight state teams were enrolled in Cohort 1. Each state team consisted of five travelling
core members that attended the in-person intensive workshop as well as additional members that
participated in the training. This program’s model required applicants to establish an
Center’s technical assistance. The Center’s coaches, who come from a wide variety of leading
organizations for public health and health transformation, provide technical assistance and
consultant services. Each state team was led by an MCH state leader and convened members
from a variety of organizations, such as Medicaid, Departments of Education, Rural Health
Associations, Local Health Departments, and parent advocacy groups. The Cohort 1 state team
applied learning, health transformation projects are as follows:
State Team Health Transformation Project
Colorado Maximize efficiency and effectiveness of care coordination delivery for Children and Youth with Special Health Care Needs population funded by state/federal care coordination resources
Georgia Develop a comprehensive work plan for implementing an intake process for the state Department of Public Health child health programs to improve efficiency of program placement of eligible children and reduce duplication of effort in obtaining family information for eligibility assessment
Hawaii Develop quality improvement processes to increase screening and referral rates of young children to improve developmental outcomes
Illinois Change focus to community-based and wellness-centered with regionalized tertiary care settings focusing on the specialized needs of high risk women and babies
Iowa Improve the MCH workforce knowledge, skills, and competencies for its role in health care reform implementation
Minnesota Reduce duplicative work by identifying key partners for joint planning of action steps for five strategies from the CYSHN strategic plan to improve access and quality of care for CYSHN and their families
Mississippi Integrate the system of care for Mississippians with special health care needs through enhanced collaboration and greater statewide partnerships
Rhode Island Develop core competencies, standardized curriculum and pathways to
The Center’s intensive cohort training model for Cohort 1 included: eight webinars that
consisted of didactic instruction, break-out sessions for discussion, and guided practice exercises,
one intensive workshop over the course of two days where state teams participated in 12
in-person sessions, peer sharing, and networking in Chapel Hill, NC, and ongoing action learning in
the implementation of projects with technical assistance from coaching and site visits. The
Center’s curriculum offered through webinars, workshop sessions, and site visits are shown
below.
Training Component Topics Covered
Webinars Health Transformation, driver diagram overview, and project focus and team selection
Quality Improvement, applying quality improvement related tools, and developing Aim Statements and Project Charters Systems Thinking and applying systems thinking tools with practice exercises
Adaptive leadership, Plan-Do-Study-Act learning cycles, and appreciative inquiry
Project measurement plans, systems mapping, causal loop mapping
Planning for sustainability, identifying problems, effective leadership strategies,
Return on investment Center support in the future
Intensive Workshop Sessions Health Transformation considerations for MCH, Impact of health reform, opportunities and challenges
Developing measures using a quality improvement approach and using logic models and aim statements to generate project measures
Updating project charters and project deliverables
Importance of root cause analysis, using tools to identify root causes, prioritize main root causes in health
transformation project and focus improvement efforts
Applying prioritization tools to develop a list of top changes for testing by state teams
Developing Plan-Do-Study-Act cycles to test change ideas Site Visits Reviewing process flow diagrams, identifying opportunities
Background
In its 1988 report, The Future of Public Health, the Institute of Medicine identified
leadership development and training as a key strategy for strengthening the capacity of the public
health infrastructure to improve health outcomes.1 Consequently, public health agencies heavily
invested in establishing leadership development training programs to build capacity for
organizational change management and effective implementation of initiatives and
programming.2,13,14 Since then, agencies continue to prioritize leadership development programs
on local, state and federal levels.2,3,13–15 Sponsors of these programs have prioritized impact
evaluations, which have emphasized the importance of “collaboration” and the related practices
of establishing coalitions, strengthening partnerships, developing communication tools, building
inter-agency teams, and enacting procedures for cooperation and collaboration.3,5,6,8
The utility of collaborative practices to address complexities of large scale social issues
has been demonstrated in the public health field.5,16 The complex, systemic nature of these
challenges demands its leaders to engage in collaborative practices such as integrating
stakeholders, creating partnerships and coalitions, and convening across sectors in order to make
significant improvements.17–20 The next section summarizes collaborative leadership practices in
the wider literature according to a five-part scheme described by Alexander et al. (2001):
systems thinking, vision-based leadership, collateral leadership, power sharing and process-based
Systems Thinking:
Systems thinking is an integral component of planning collaborative action because it
contributes to goal setting and organizational change management. 21 Leaders can use systems
thinking to map complex relationships between programs, organizations and agencies and to
identify potential partners and stakeholders associated with a complex challenge, who can then
be leveraged for collaborative support.22 The practice of systems thinking can also facilitate root
cause analyses as leaders work to identify the origins of key challenges or barriers to
organizational goals.4,21 Main outcomes of systems thinking have included comprehensive needs
assessments, identification of potential partners and leverage points, and the development of
plans for improved communication and stakeholder integration.21
Vision-based Leadership:
This practice reflects the development of actionable plans for achieving long-term
systemic goals. In the collective setting, partnerships and coalitions must align efforts and create
a shared vision in a specific direction.5 Vision-based Leadership encompasses the strategic
development of coalitions, task forces, and partnerships as well as the creation of a shared vision
for improvements among the various collaborators.4,23,24 This collaborative leadership practice
also involves effectively communicating the shared vision, and ensuring the alignment of future
efforts.5
Collateral leadership:
Collateral leadership describes the power structure often seen in public health systems.
The use of collaborative practices is particularly important for horizontal power sharing
roles.5,17,18 In this lateral power structure, leaders convene representatives of interested parties
across a system, thus creating informal leadership roles as these professionals work together
toward a common goal.5
Power Sharing:
This collaborative practice encompasses the skills necessary to effectively manage these
informal leadership roles and systems-wide relationships. Power sharing emphasizes shared
planning between partners to set priorities that address each partner’s needs and building
consensus in order to create mutually beneficial solutions in effective collaboration.4,5
Empowerment of participating partners is also generated, giving the collaboration or coalition a
greater capacity for change.5,18
Process-based Leadership:
Process-based leadership describes essential skills for collaboration throughout the
progression of efforts.4 Leaders must possess a variety of soft skills including listening, team
building, and perspective taking to facilitate collaborative work.5 Process-based leadership
outlines the fundamental practices of leaders who engage in effective collaboration.4
Collaborative Community Health Partnerships: Leadership Framework4
The five collaborative leadership themes identified by Alexander et al. (2001) were
shown to interact and overlap in practice. Systems Thinking influences Vision-based Leadership
and vice versa, and Collateral Leadership and Power Sharing also shared similar mutual
interaction.4 While there are feedback loops for these leadership themes, Systems Thinking tends
to lay the foundation for Vision-based Leadership, and Collateral Leadership is a predecessor of
as collaborative work is implemented and sustained.4 The figure below visually conveys the
interaction of these leadership themes.
Published reports of organizations, programs, and initiatives have found the use of
collaborative leadership practices beneficial to processes, outreach, and ultimately health
outcomes.5 Collaborative leadership practices have been utilized in programs spanning a variety
of specializations including cardiovascular disease, mental health, cancer, hospital mortality, and
infant mortality.5,25 These programs have cited collaborative leadership in their streamlining of
efforts across various organizations and perspectives. Collaborative leadership has been shown to
be particularly instrumental in the success of MCH programs in 90 cities across the United
States.26 The value of collaborative leadership in MCH practice is also demonstrated by the
nationally adopted core competencies for MCH leaders, which identify collaborative practices,
such as communication, conflict resolution and negotiation, and working in systems and
communities, as necessary proficiencies.9
While the aforementioned framework speaks to key facilitators of collaborative
leadership in health-related settings, research has also revealed challenges that create significant
barriers to effective and sustained collaboration. Organizations tend to struggle to work through
complexities of resource allocation, ownership and recognition, visibility, and autonomy when
collaborating with others.27 Generally, organizations do not want to give up resources for
effective communication and consensus agreement, the stronger organizations with more
resources, credit, visibility, and autonomy will tend to be less engaged than others because of a
disinclination to sacrifice their own resources and clout.27 Stronger organizations also tend to
disengage during consensus building processes and fall into absenteeism because they resent
having less decision making power in multi-partner collaborative work, especially if there is a
history of a hierarchal relationship to another organization in the coalition. Consensus building
for mutual satisfaction has been shown to be easier to achieve with fewer organizations
present.27Another challenge faced by coalitions and multi-organizational partnerships is high
member turnover and disengagement from collaborative work from losing momentum.28 Most
collaborative coalitions for public health are fueled by volunteer labor from members who must
balance professional responsibilities for their own organizations.28 Perceived effectiveness of the
coalition and sustained participation by members are correlated with their feelings of satisfaction
with solidarity, appreciation, and evidence of impact.28 Coalition members tend to feel frustrated
when planning products set vague and unrealistic expectations, such as working towards health
systems change or influencing health outcomes.28 Partners can also become frustrated when
decision-making is a slow process, which can occur when representatives at coalition meetings
have limited authority to make commitments from their organizations without review and
clearance.27 Members tend to withdraw when the costs in time and frustration outweigh the
benefits of evidence of impact.28 Planning for tangible intermediate outcomes that are
conceivable precursors to larger goals can create evident successes that keep members better
engaged.28
As leadership training programs for MCH professionals have been implemented and
development.12 One prominent MCH training program, the MCH Public Health Leadership
Institute, included the measurements of systems thinking, collaboration, creating partnerships,
and stakeholder analysis in its evaluation of perceived skill improvement experienced by
trainees.11
Although the use of collaborative practices is widely viewed as a key skill for MCH
leaders and an integral component of MCH programming, few publications evaluate the impacts
of related leadership development training on MCH professionals’ use of collaborative
practices.29 This study will contribute to this knowledge base by evaluating the use of
collaborative practices by the Center’s cohort 1 participants after undergoing the intensive cohort
METHODS: Study Design
This case study evaluates the Center’s approaches to fostering collaborative practices for
MCH professionals using qualitative methods.30 Case study methodology is particularly useful in
evaluating programs, such as the Center’s training, in bounded settings where the behavior of
those involved in the study cannot be manipulated.30
Data Collection: Key Informant Interviews
The evaluator conducted key informant interviews by telephone with the Center’s Cohort
1 participants approximately one year after their formal completion of the intensive training
program.30–32 Key informant interviews are used to provide detailed information regarding
experiences, opinions, perspectives, and impressions about a localized phenomenon. Two levels
of purposeful sampling were used to select key informants for this study. First, the evaluator
decided to only study the Center’s Cohort 1 participants in order have one full year of related
experience post-training available for analysis. There were eight state teams in Cohort 1, with
approximately five members per team. Out of the total 40 participants, eight were selected for
interview. One representative from each state team was identified as a key informant for
interview based on the following criteria: participated in the Center’s Cohort 1 intensive training
program as a co-lead of a state team, or identified by a co-lead as a suitable representative of the
state team. This sampling was also on the selection process for the Center’s evaluation conducted
six months after the formal completion of the intensive training program, where the same
co-leads were interviewed at that time. Each key informant received verbal confirmation of the
with one state team leader, and no adjustments were deemed necessary before widespread use.
This pilot interview was included in data analysis.
Data Analysis
The principal dataset consists of eight transcribed interviews that was managed and
analyzed using Atlas.ti software. Data was also collected in a document review of the Center’s
Cohort 1 training curriculum for analysis. A preliminary codebook was created before the
completion of the data collection process for anticipated themes based on the evaluator’s
literature review. This codebook was updated throughout data collection and analysis to capture
emergent themes, which were marked as subcodes and then linked and grouped according to the
five-part collaborative leadership framework by Alexander et al.33 In this inductive strategy, each
data code was captured by one of the five themes in the framework: Systems Thinking,
Vision-based Leadership, Collateral Leadership, Power Sharing or Process-Vision-based Leadership. Findings
from the key informant interviews and document review were then compared in a matrix against
the five-part framework to identify strengths and gaps in the Center’s training.4,34 A network
diagram was developed to map the process of collaborative work described by participants of
this study.
Validity and Reliability
A triangulation strategy was implemented in this study to source data from more than one
method.30,35 To capture different dimensions of collaborative leadership training and practices for
the Center’s Cohort 1 participants, the data collected in key informant interviews were
Generalizability in a qualitative case study is difficult to scope, but this study’s 100% response
rate from each sampled team has represented the span of perspectives across all state teams.
Ethical Considerations
The Institutional Review Board at the University of North Carolina at Chapel Hill
deemed this study exempt from review. All participants were former participants of the Center’s
intensive training cohort and were made aware of the voluntary nature of this study. All
interviewees were given an opportunity to refuse participation in the interview or refuse
recording. No published findings link to any specific participant, state team, or identifying
RESULTS:
Systems thinking and Vision-based Leadership practices tended to be mentioned
together, with Systems Thinking acting as a predecessor for actions related to Vision-based
Leadership. Collateral leadership and Power Sharing tended to be similarly paired, and
Process-based Leadership components were mentioned as overarching practices. Key informants also
described several barriers and facilitators to sustaining partnerships for effective collaboration.
Leadership Practices by Collaborative Community Health Partnerships Theme:
The significant findings from eight total key informant interviews were organized based
on relevance to each leadership theme in the Alexander et al. framework. Findings were deemed
significant if the practice was independently mentioned by more than one participant, or
mentioned at least three times throughout the course of one interview. Findings were then
compared to the Center’s curriculum to identify gaps and areas for improvement.
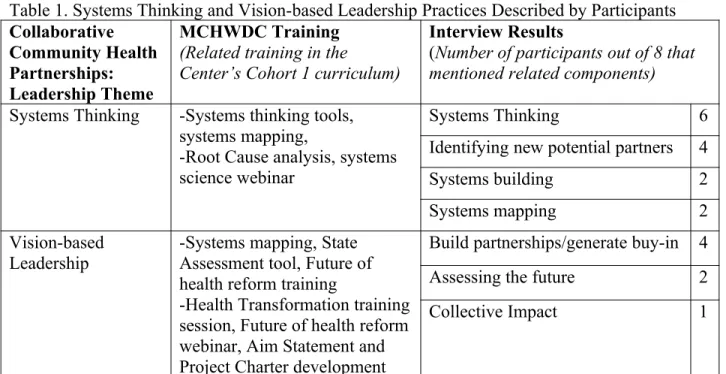
Table 1. Systems Thinking and Vision-based Leadership Practices Described by Participants
Collaborative Community Health Partnerships: Leadership Theme
MCHWDC Training
(Related training in the Center’s Cohort 1 curriculum)
Interview Results
(Number of participants out of 8 that mentioned related components)
Systems Thinking -Systems thinking tools, systems mapping,
-Root Cause analysis, systems science webinar
Systems Thinking 6 Identifying new potential partners 4 Systems building 2
Systems mapping 2
Vision-based Leadership
-Systems mapping, State Assessment tool, Future of health reform training
-Health Transformation training session, Future of health reform webinar, Aim Statement and Project Charter development
Build partnerships/generate buy-in 4
Assessing the future 2
Four interviewees described ways in which Systems Thinking practices laid the
foundation for Vision-based Leadership and further collaborative work by generating buy-in for
partners. Systems Thinking was the only collaborative leadership theme that was explicitly
mentioned by key informants in these interviews. Systems Thinking practices played a key role
in identifying new potential partners that were stakeholders in a systems-wide approach for four
teams’ project with the Center. Interviewees described perceived benefits from guided practice
with the systems thinking tools, systems mapping, and systems building that were provided by
the Center during training. For example, one key informant stated, “I think the tools around
systems thinking were the most useful for what our project was focused on and what we
needed.” Additionally, the Center provided tools and didactic instruction on root cause analyses
in systems-wide approaches as well as a systems science training document; however, these
training components were only found in the document review and not mentioned by key
informants in the interviews.
In addition to using systems thinking tools to generate buy-in across partnerships, key
informants also mentioned the Vision-based Leadership practices used to create a shared vision
of project aims with stakeholders and partners. Two interviewees found it useful to assess the
future of healthcare reform with their partners in order to align efforts moving forward. One key
informant interview specifically stated that they adapted the Center’s intensive workshop session
on the future of healthcare reform and brought it to their partners and stakeholders for a relevant
project. Document review of the Center’s Cohort 1 curriculum identified a training session on
assessing health transformation and the impacts on participants’ states, as well as an introductory
interviewees also mentioned similar adaptation and use for the State Health Assessment tool,
which was introduced to state teams in the Center’s intensive cohort training.
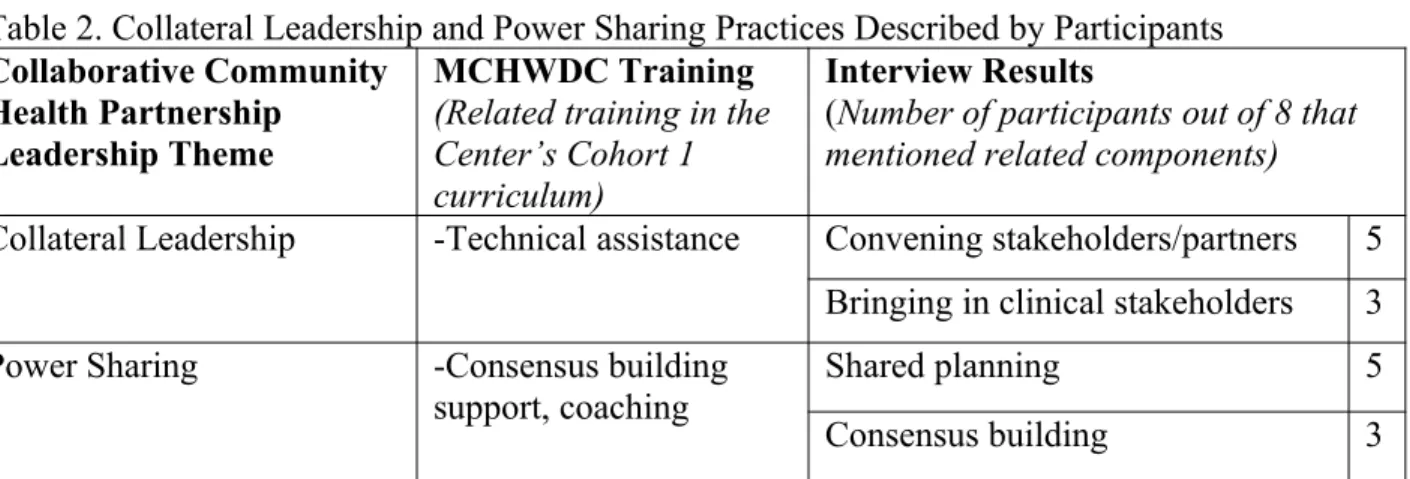
Table 2. Collateral Leadership and Power SharingPractices Described by Participants
Collaborative Community Health Partnership
Leadership Theme
MCHWDC Training
(Related training in the Center’s Cohort 1 curriculum)
Interview Results
(Number of participants out of 8 that mentioned related components)
Collateral Leadership -Technical assistance Convening stakeholders/partners 5 Bringing in clinical stakeholders 3 Power Sharing -Consensus building
support, coaching Shared planning 5 Consensus building 3
Five interviewees described significant support and opportunities provided by the Center
to convene stakeholders and partners for their projects, and mentioned carrying this experience
forward in their work since training. For example, one key informant said,
“We brought together a pretty wide stakeholder group for our group for the cohort
[training] including Medicaid, primary care physicians, local MCH agencies...this
[project] helped us bring that group of diverse stakeholders together to work on
workforce development issues as they relate to Title V.”
The Center’s technical assistance and coaching for state teams was designed to support the
individual needs of each group, which included engaging and convening the necessary
stakeholders and partners identified in systems thinking exercises. In fact, one key informant
stated, “Through the technical assistance, we had increased our partnerships [more] than what
our original intention of the project was going to be.” Three teams described particular success in
convening stakeholders from the provider perspective for their projects. Two of these teams
expressed feelings of accomplishment for successfully engaging clinical partners. While key
interviewees viewed the Center’s training as an overall facilitator in building these partnerships
by providing an opportunity to convene stakeholders and partners for the Center’s required
application-based project.
The two main practices related to Power Sharing mentioned by key informants were
shared planning and consensus building. Five interviewees mentioned engaging stakeholders and
partners in the planning process of their projects, and three mentioned consensus-building
practices. For example, one interviewee said,
“Our project was actually bringing together [a] variety of stakeholders, and through the
consensus building activities we were able to find more, -- we were able to move forward
even though it wasn’t 100% agreement, and so I think that this is the first time that I’ve
been in that kind of an environment where it was very clear that we were going to go on a
consensus path.”
Those three interviewees identified consensus building as one of the most necessary practices to
sustaining partnerships, and two found consensus building to be one of the most difficult
concepts to effectively implement in practice. For example, when asked about an area of
collaborative leadership the key informant wished they learned more about in the Center’s
training, one interviewee responded, “The consensus building, because that’s always the toughest
one to get through.”The usefulness of the Center’s coaching and training sessions on consensus
building were mentioned by all three interviewees, and two also mentioned they wish more time
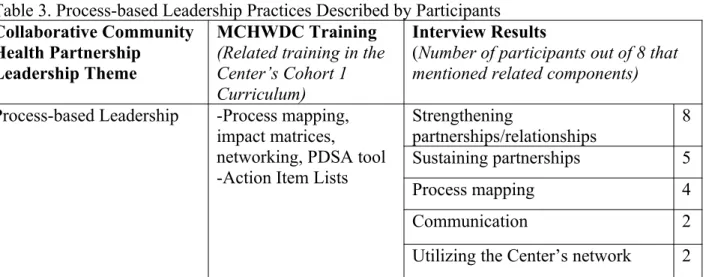
Table 3. Process-based Leadership Practices Described by Participants
Collaborative Community Health Partnership
Leadership Theme
MCHWDC Training
(Related training in the Center’s Cohort 1 Curriculum)
Interview Results
(Number of participants out of 8 that mentioned related components)
Process-based Leadership -Process mapping, impact matrices, networking, PDSA tool -Action Item Lists
Strengthening
partnerships/relationships 8 Sustaining partnerships 5
Process mapping 4
Communication 2
Utilizing the Center’s network 2
Interviewees tended to mention Process-based Leadership components as practices that
they felt they the Center has helped them improve. All eight key informants felt that their state
team was able to strengthen a partnership, interagency relationship or coalition in some way
since undergoing the Center’s intensive cohort training. Five interviewees mentioned sustaining
long-term partnerships is particularly difficult in their work, but the Center provided support for
engaging partners throughout the duration of the project. There was also an identified need for
more related training, with one key informant stating, “If I had to guess of what we would want
to learn more about is that is once you build [teams and partnerships], how do you keep them?”
Communication was seen as a key facilitator for collaborative work for two interviewees, who
described an observed need and challenge to continuously keep partners updated on progress to
maintain their engagement. Process mapping training, impact matrix tools and
Plan-Do-Study-Act cycles were all mentioned by interviewees as useful components of the Center’s curriculum
for integrating partners into the planning and implementation of collaborative work. Document
review identified Action Item Lists as another related tool that ties actions/suggestions to
responsibilities for each partner and provides a structured format for effective communication
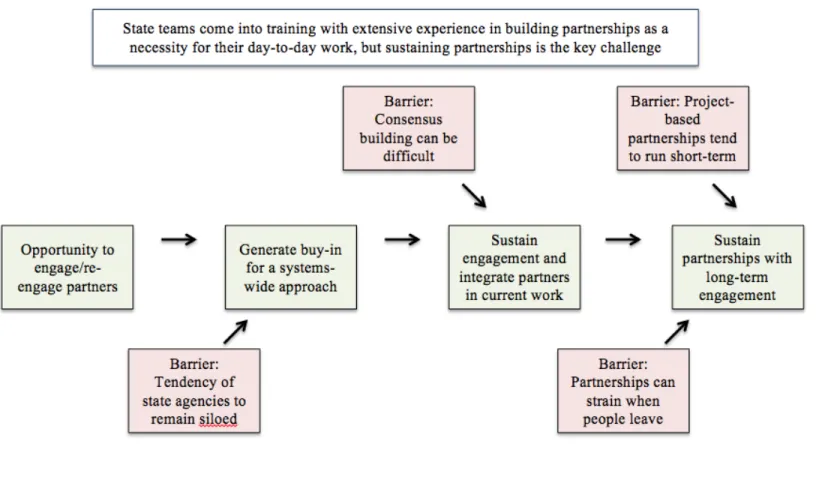
Barriers to Collaborative Leadership for Participants:
This case study found four key barriers to sustained collaborative work with partnerships
for the Center’s Cohort 1 participants: 1) a tendency for state agencies to have siloed priorities,
2) difficulty achieving a consensus to move a project forward without individual partners
disengaging, 3) strained organizational partnerships when the individual representative leaves
that partnering organization, and 4) difficulty in sustaining project-based partnerships past the
short term. The process of sustaining long-term collaboration with key barriers as described by
Cohort 1 key informants is shown in Figure 1.
Cohort 1 key informants reported that participants generally come into the Center’s
intensive cohort training with extensive experience in building inter-agency partnerships as a
result of the nature of their work. It has been said that they felt comfortable establishing
partnerships, but the Center was influential in learning how to strengthen and sustain
partnerships. Document review of the state teams’ aim statements found four health
transformation projects that identify improving collaboration and coordination with partners as
explicit goals. Several key informants particularly valued the way that the inter-agency team
structure provided an opportunity for them to engage the stakeholders with whom they wanted to
build new partnerships or re-engage existing partners to further integrate them into collective
work. Six key informants stated that most of their collaborative work is executed with partners
that they have worked with before on another project.
Systems Thinking was an essential takeaway for the majority of key informants in
identifying stakeholders and other potential partners to convene. Systems Thinking practices
have also been used to demonstrate each partners’ role in the collective work, with aims to
they have identified stakeholders that would be beneficial partners, two key informants have
found a tendency for state organizations to work more independently. This culture of siloed
priorities was highlighted as a barrier to sustaining collaboration with partners. As described, the
continued struggle is to break individual organizations from a “what’s in it for me?” mentality in
order to take a more comprehensive, systems approach.
When convening the right partners and stakeholders for collaborative work, three state
teams mentioned consensus building as one of the most difficult practices to effectively
implement, as well as one of the most useful aspects of the Center’s training. One key informant
described the necessity of consensus building practices to sustain the engagement of a coalition’s
members in order to promote timely progress without unanimous agreement while still valuing
the present perspectives. This key informant had prior experience of partners disengaging as a
result of a consensus building process that required concessions and expressed feelings of
surprise as a result of this recent successful practice.
Each participant described difficulty in sustaining long-term active partnerships. Even
though six state teams mentioned working with current partners before, three mentioned that
these efforts are largely project-based. These three teams found that their collaborative
relationships with partnering agencies generally waned at the conclusion of a specific project,
until a different endeavor surfaced. Two state teams described the difficulty of sustaining
partnerships with an agency when a previous individual collaborator/contact has left the position.
One key informant is the only team member still working in her state system since the end of the
intensive cohort training, including external partners. She is currently facing significant
challenges in garnering support and buy-in from these new contacts, who have not worked with
Figure 1. Process Map of Sustaining Long-term Partnerships for Cohort 1 Participants
DISCUSSION:
This study evaluates the use of collaborative leadership practices by MCH leaders after
undergoing the Center’s leadership development training. The key findings of this study address
two evaluation questions: 1) What are the effects of the Center’s leadership training and
development on the use of collaborative leadership practices by MCH leaders? 2) What are
perceived barriers to collaborative leadership practices for MCH leaders?
Responses from the eight total key informant interviews aligned with the structure of the
key collaborative leadership themes framework by Alexander et al. (2001). In this study, key
informants tended to mention Systems Thinking and Vision-based Leadership practices together,
and also paired Collateral Leadership and Power Sharing practices when describing their
experiences. Process-based Leadership actions for sustaining partnerships and working
collaboratively were mentioned as overarching facilitators encompassing softer skills, such as
effective communication, to maintain engagement. Systems Thinking was the only collaborative
leadership theme from the framework that was explicitly mentioned by interviewees. It is
important to note that the Center does not train on Alexander et al. framework explicitly; this
collaborative leadership framework was utilized for analysis purposes only. While the purpose of
the Center’s training does not intentionally address all of these leadership themes, this analysis
does provide the Center with opportunities to improve identified gaps.
Key informants describe using Systems Thinking practices to identify necessary partners
and stakeholders, and then implementing Vision-based Leadership to generate buy-in for
collaborative work with those potential partners. Alexander et al. (2001) described a similar
chronology in their framework where leaders create a framework for action through systems
Leadership practices are mentioned by key informants as a predecessor to Power Sharing in this
study, as key informants describe convening stakeholders and ensuring the right partners were
assembled for an effective systems-based solution and then discuss the necessity and difficulty of
effective consensus building practices and shared planning. Similarly, Alexander et al. (2001)
describe convening processes in which a group of necessary core partners are represented for
collaboration and the subsequent need to share power among the different organizational partners
in order to create a sense of shared ownership and mutual accountability.4 Finally, this study also
aligns with the Alexander et al. (2001) framework findings that show Process-based Leadership
practices crosscutting across all of the other themes to facilitate the growth and sustainment of
collaboration.
The Center’s training related to collaborative leadership seems to be strongest in Systems
Thinking and Process-based Leadership. Overall, interviewees felt that they received the most
training related to collaborative leadership in Systems Thinking. The key informants’ significant
recollection of specific systems thinking tools, systems mapping, and support in identifying
partners for the health transformation projects indicate the Center’s focus on earlier stages of
project development, planning and implementation in the intensive cohort training. The only
component of collaborative leadership that all eight key informants answered similarly was
related to Process-based Leadership. Each interviewee felt that they were able to strengthen a
partnership or organizational relationship as a result of either working with that partner on their
inter-agency state team or working with that partner in the continuation of the health
transformation project after the formal close of the intensive cohort training. The health
transformation project seems to have the most significant role in Process-based Leadership
additional exposure and support. Power Sharing is the collaborative leadership theme that
demonstrates the Center’s most significant need for strengthening training components. Power
Sharing was also identified as the most difficult leadership theme for individuals to master by
Alexander et al. (2001).4 Interviewees only mentioned two specific examples of Power Sharing:
shared planning and consensus building. Interviewees expressed an observed need for more
support in consensus building. The key informants who discussed the difficulty of implementing
consensus-based decision-making mentioned that they wished more time was spent on this topic
in the Center’s training. This highlights a need to provide additional support for consensus
building in didactic instruction with guided practice to prepare participants for related challenges
that may arise in the future. If health transformation projects are in the earlier stages of
development, difficult decisions that require a tumultuous consensus building process may not be
necessary to make as yet. Preemptively preparing MCH leaders for future consensus building
processes could mitigate some of the challenges faced later on.
Even though one of the Center’s strongest collaborative leadership training areas is
Process-based Leadership, Cohort 1 participants still describe facing challenges in sustaining
partnerships and keeping partners engaged, which is a key component of this theme. In this
study, MCH leaders mention the challenge of bringing other agencies into collaborative work,
because of an observed organizational tendency to remain focused on internal projects. Green
(2000) describes this in the context of most organizations’ tendency to resist giving up resources
to invest in shared work.27 To work through the complexities of resource allocation, ownership
and recognition, key recommendations include effective communication and consensus
agreement 4,27 Consensus building is another challenge for MCH leaders in this study, who find
consensus building for mutual satisfaction is easier to achieve with fewer organizations present
and attending representatives with enough clout for decision-making without organizational
review.27 MCH leaders in this study ultimately describe an observed challenge in sustaining
long-term engagement from partners. Green (2000) attributes this disengagement to the partners’
frustration due to a lack of satisfaction which include feelings of solidarity, appreciation, and
evidence of impact, and similar findings are described by Kreuter (2000) and Alexander et al
(2001).4,27,28 Partnering members tend to feel particularly frustrated when group aims set vague
and unrealistic expectations, such as working towards health systems change or influencing
health outcomes.28 While participants generally feel that their work with the Center has provided
significant improvement in their perceived skillset in sustaining partnerships, they still describe
challenges that prevent effective implementation in practice. It would be advantageous to
participants if the Center strengthens training components to help MCH leaders anticipate these
barriers in their work to address how these barriers could be lessened in the participants’ future
work.
Limitations
One limitation of this study was the use of single-coder for data analysis, but two
methodological strategies mitigated the effects of this limitation. The evaluator used a published
framework as a structured reference for analysis, which addressed the potential for bias from the
single-coder evaluation. The triangulation strategy implemented in data collection also provides
additional validity and reliability to this study and mitigates effects from potential biases, as the
Center’s goals and the interviewees’ comments frequently aligned. Another limitation of this
leaders who volunteered to participate in the Center’s intensive cohort training to improve their
leadership skills, who may have different perspectives and experiences than the larger population
of MCH leaders.
Conclusion
In the current environment of health reform and a shifted focus from disease management
to population health, effective collaboration with partnering organizations is necessary for MCH
leaders to address the systemic issues that affect of their target populations. Effective leadership
is crucial to convene and engage necessary stakeholders for a systems approach to solving MCH
issues and then sustain this collaborative work. The findings in this study suggest that investment
in leadership development training for MCH professionals, such as the Center, can improve
participants’ perceived skill in collaborative leadership practices. Further research and evaluation
should be done to investigate key collaborative leadership competencies for MCH professionals
and barriers to sustaining collaboration in order to strengthen leadership development training
APPENDIX:
Interview Guide
Introduction: My name is Alina Clarke and I am working with the National Maternal and Child Health Workforce Development Center at UNC Chapel Hill Gillings School of Global Public Health to collect data for my senior thesis. For this research, I am interviewing participants in the intensive leadership cohort about leveraging partnerships, creating coalitions, systems thinking, building a shared vision, navigating interagency relationships and convening across stakeholders. This interview will be recorded for data quality assurance.
1. The Center provided training and tools in several areas: establishing new and/or strengthening partnerships, team-building with interdisciplinary or interagency team members, consensus building and systems thinking.
a. In which of these areas did you learn the most about?
b. Which do you wish you spent more time learning about?
c. Which do you find most useful and applicable to your work?
2. Would you please provide an example of how you have applied some of these skills and techniques since the training?
3. Would you please provide an update on your team’s health transformation project now at one year after your formal relationship with the Center?
a. Are you still working with any of your new partners identified in the development of your health transformation project?
b. How were you able to sustain these partnerships?
c. Have these partnerships expanded?
d. Have you formed any new partnerships since the formal close of your relationship with the Center?
4. Were you able to experience successes or achieve goals as a result of enhanced collaboration with partners?
REFERENCES:
1. Institute of Medicine. The future of public health. 1988.
2. Woltring C. Does leadership training make a difference? The CDC/UC public health leadership institute: 1991–1999. J Public Heal. 2003.
3. Baker E, Umble K, Frederick S, Woltring C. A brief history of formal public health leadership development in the United States since 1988: lessons learned and future needs.
Leadersh Public Heal. 2008.
4. Alexander J, Comfort M. Leadership in collaborative community health partnerships.
Nonprofit Manag. 2001.
5. Larson C, Sweeny C, Christian A, Olson L. Collaborative leadership and health: A review of the literature. Excell Collab Turn Point. 2002.
6. Stoto M, Abel C, Dievler A. Healthy Communities: New Partnerships for the Future of Public Health.; 1996.
7. Umble K, Steffen D. The National Public Health Leadership Institute: evaluation of a team-based approach to developing collaborative public health leaders. Public Heal. 2005. 8. Umble K, Baker E, Diehl S. An evaluation of the National Public Health Leadership
Institute–1991-2006: part II. Strengthening public health leadership networks, systems, and infrastructure. J Public. 2011.
9. Association of Maternal and Child Health Programs. Maternal and Child Health Competencies Version 3.0.; 2009.
10. Kroelinger C, Kasehagen L, Barradas D. Building leadership skills and promoting workforce development: evaluation data collected from public health professionals in the field of maternal and child health. Matern child Heal. 2012.
11. Fernandez C, Noble C. Moving the needle: A retrospective pre-and post-analysis of improving perceived abilities across 20 leadership skills. Matern child Heal. 2015. 12. Dodds J, Vann W, Lee J. The UNC-CH MCH leadership training consortium: Building
the capacity to develop interdisciplinary MCH leaders. Matern Child. 2010.
13. Kimbrell J, Witmer A, Flaherty P. The Louisiana Public Health Institute: A Cross‐Sector
Approach for Improving the Public’s Health. J Public Heal. 2002.
14. Saleh S. Evaluating the effectiveness of public health leadership training: the NEPHLI experience. Am J. 2004.
15. Reynolds M, Leahy E. Developing a public health training institute through public health improvement efforts: Montana’s story. J Public Heal Manag Pract. 2002.
16. Kania J, Kramer M. Collective impact. 2011.
17. Avery C. All power to you: Collaborative leadership works. J Qual Particip. 1999. 18. Fawcett S. Using empowerment theory in collaborative partnerships for community health
and development. Am J. 1995.
19. Lovelace K. Multidisciplinary top management teamwork: Effects on local health department performance. J Public Heal Manag Pract. 2001.
20. Nowell B, Harrison L. Leading change through collaborative partnerships: A profile of leadership and capacity among local public health leaders. J Prev Interv. 2010.
21. Leischow S, Best A, Trochim W. Systems thinking to improve the public’s health. Am J.
2008.
tobacco control. 2007.
23. Chrislip D, Larson C. Collaborative leadership: How citizens and civic leaders can make a difference. 1994.
24. Carr A. Leadership and Community Participation: Four Case Studies. J Curric Superv. 1997.
25. Versteeg M, Laurant M, Franx G. Factors associated with the impact of quality
improvement collaboratives in mental healthcare: an exploratory study. Implement …. 2012.
26. Peck M, Fitzgerald M. Lessons Learned, 1997: Profiles of Leading Urban Health
Department Initiatives in Maternal and Child Health. Highlights of the CityMatCH Urban Maternal and Child. 1998.
27. Green L. Caveats on coalitions: in praise of partnerships. Health Promot Pract. 2000. 28. Kreuter M, Lezin N, Young L. Evaluating community-based collaborative mechanisms:
Implications for practitioners. Health Promot Pract. 2000.
29. Mouradian W, Huebner C. Future directions in leadership training of MCH professionals: Cross-cutting MCH leadership competencies. Matern Child Health J. 2007.
30. Merriam S, Tisdell E. Qualitative Research: A Guide to Design and Implementation.; 2015.
31. Boyce C, Neale P. Conducting in-Depth Interviews: A Guide for Designing and Conducting in-Depth Interviews for Evaluation Input.; 2006.
32. Tremblay M. The key informant technique: A nonethnographic application. Am Anthropol. 1957.
33. Boyatzis R. Transforming Qualitative Information: Thematic Analysis and Code Development.; 1998.
34. Miles M, Huberman A, Saldana J. Qualitative Data Analysis: A Methods Sourcebook.; 2013.