Evaluation of the Accelerate Pheno
System for Fast Identification and
Antimicrobial Susceptibility Testing from
Positive Blood Cultures in Bloodstream
Infections Caused by Gram-Negative
Pathogens
Matthias Marschal,a,bJohanna Bachmaier,aIngo Autenrieth,a,b Philipp Oberhettinger,a,bMatthias Willmann,a,bSilke Petera,b
Institute of Medical Microbiology and Hygiene, University of Tübingen, Tübingen, Germanya; German Center for Infection Research (DZIF), Partner Site Tübingen, Tübingen, Germanyb
ABSTRACT Bloodstream infections (BSI) are an important cause of morbidity and mortality. Increasing rates of antimicrobial-resistant pathogens limit treatment op-tions, prompting an empirical use of broad-range antibiotics. Fast and reliable diag-nostic tools are needed to provide adequate therapy in a timely manner and to enable a de-escalation of treatment. The Accelerate Pheno system (Accelerate Diag-nostics, USA) is a fully automated test system that performs both identification and antimicrobial susceptibility testing (AST) directly from positive blood cultures within approximately 7 h. In total, 115 episodes of BSI with Gram-negative bacteria were included in our study and compared to conventional culture-based methods. The Accelerate Pheno system correctly identified 88.7% (102 of 115) of all BSI episodes and 97.1% (102 of 105) of isolates that are covered by the system’s identification panel. The Accelerate Pheno system generated an AST result for 91.3% (95 of 104) samples in which the Accelerate Pheno system identified a Gram-negative pathogen. The overall category agreement between the Accelerate Pheno system and culture-based AST was 96.4%, the rates for minor discrepancies 1.4%, major dis-crepancies 2.3%, and very major disdis-crepancies 1.0%. Of note, ceftriaxone, piperacillin-tazobactam, and carbapenem resistance was correctly detected in blood culture speci-mens with extended-spectrum beta-lactamase-producing Escherichia coli (n ⫽ 7) and multidrug-resistantPseudomonas aeruginosa(n⫽3) strains. The utilization of the Accel-erate Pheno system reduced the time to result for identification by 27.49 h (P⬍0.0001) and for AST by 40.39 h (P⬍0.0001) compared to culture-based methods in our labora-tory setting. In conclusion, the Accelerate Pheno system provided fast, reliable results while significantly improving turnaround time in blood culture diagnostics of Gram-negative BSI.
KEYWORDS antimicrobial susceptibility testing, bloodstream infections, rapid tests
B
loodstream infections (BSI) are an important cause of morbidity and mortality, associated with prolonged hospital stays, as well as high costs for health care systems (1–3). Increasing rates of antimicrobial-resistant pathogens, in particular Gram-negative bacteria, limit treatment options, often prompting the empirical use of broad-range antibiotics. Therefore, we need fast and reliable diagnostic tools to speed up both identification (ID) and antimicrobial susceptibility testing (AST) from blood cultures in order to provide adequate therapy in a timely manner and to enable effective antibiotic stewardship interventions (4).Received7 February 2017Returned for
modification8 March 2017Accepted20
April 2017
Accepted manuscript posted online26
April 2017
CitationMarschal M, Bachmaier J, Autenrieth
I, Oberhettinger P, Willmann M, Peter S. 2017. Evaluation of the Accelerate Pheno system for fast identification and antimicrobial susceptibility testing from positive blood cultures in bloodstream infections caused by gram-negative pathogens. J Clin Microbiol 55:2116 –2126.https://doi.org/10.1128/JCM .00181-17.
EditorAlexander J. McAdam, Boston Children's
Hospital
Copyright© 2017 American Society for
Microbiology.All Rights Reserved. Address correspondence to Silke Peter, [email protected].
crossm
on May 16, 2020 by guest
http://jcm.asm.org/
Current laboratory ID and AST are based primarily on bacterial culture and are usually completed in 2 days or more (5). Some authors have described direct identifi-cation based on matrix-assisted laser desorption ionization–time of flight mass spec-trometry (MALDI-TOF MS) (6–9) and molecular detection assays for pathogen identifi-cation from positive blood culture bottles (8, 10–14). While assays such as the BioFire FilmArray blood culture identification panel (BioFire; bioMérieux SA, USA) and the Verigene blood culture assays (Nanosphere, USA) have been shown to enable fast pathogen identification and detection of a few antimicrobial resistance genes, pheno-typic AST is not provided.
The Accelerate Pheno system (Accelerate Diagnostics, USA) is a fully automated test system capable of performing identification and AST directly from positive blood cultures within approximately 7 h. The system combines gel electrofiltration and fluorescence in situ hybridization for bacterial identification, as well as automated microscopy for analyzing bacterial growth rates and for extrapolating MIC values.
In the following study, we provide a prospective evaluation of the Accelerate Pheno system in comparison to conventional culture-based identification and AST in BSI with Gram-negative bacteria. As the rates of resistant Gram-positive organisms such as vancomycin-resistant enterococci and methicillin-resistant staphylococci are currently below 1% in our hospital, we decided to focus our evaluation of the Accelerate Pheno system on Gram-negative BSI.
RESULTS
The performance of the Accelerate Pheno system for the direct detection of Gram-negative bacteria from positive blood culture samples was evaluated on a total of 115 episodes of Gram-negative BSI infections over 6 months. These included 105 mono-microbial infections with Escherichia coli (n ⫽ 58), Klebsiella pneumoniae (n ⫽ 14),
Klebsiella oxytoca (n ⫽ 2), Pseudomonas aeruginosa (n ⫽ 8), Enterobacter cloacae
complex(n⫽ 6),Serratia marcescens(n⫽ 3),Proteus mirabilis(n⫽ 2),Acinetobacter
baumanniicomplex (n ⫽ 1),Citrobacter freundii(n⫽ 1),Bacteroides fragilis(n ⫽3),
Morganella morganii(n⫽1),Acinetobacter radioresistens(n⫽1),Hafnia alvei(n⫽1),
Sphingomonas paucimobilis(n⫽1),Moraxella nonliquefaciens(n⫽1),Serratia rubidaea
(n⫽1), andRhizobium radiobacter(n⫽1). In addition, 10 polymicrobial BSI episodes occurred during the study period.
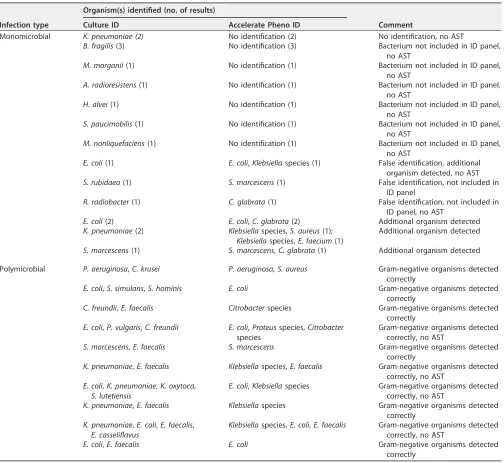
Identification of Gram-negative BSI pathogens.Correct identification of Gram-negative bacteria was achieved in 102 of 115 samples (88.7%), including 10 polymicrobial BSI. Discrepant results and polymicrobial BSI samples are summarized in Table 1.
In 13 specimens, the Accelerate Pheno system could not provide identification or, if so, only incorrectly. Identification could not be obtained in eight specimens with organisms not covered in the Accelerate Pheno system identification panel, including
B. fragilis (n ⫽ 3),M. morganii(n ⫽1),A. radioresistens(n ⫽ 1),H. alvei (n ⫽ 1),S.
paucimobilis(n⫽1), andM. nonliquefaciens(n⫽1). With regard to isolates covered by
the Accelerate Pheno system identification panel, 102 of 105 Gram-negative isolates were correctly identified (97.1%) (Table 1).
Identification was not provided in twoK. pneumoniaeisolates. In three isolates, we observed a false identification result:Serratia rubidaeawas identified asSerratia
marc-escens;Rhizobium radiobacterwas identified asC. glabrata; and in another sample with
E. coli, the identification result was E. coli and K. pneumoniae, which was the only
Gram-negative organism identified as false positive by the Accelerate Pheno system test.
The Accelerate Pheno system identified an additional organism in six infections classified as monomicrobial by culture. In polymicrobial infections, the Accelerate Pheno system identified all Gram-negative organisms correctly.
Accelerate Pheno system AST results for Gram-negative bacteria.The Acceler-ate Pheno system only produced AST results if identification was provided for an organism and if the number and growth of detected organisms in the growth control
on May 16, 2020 by guest
http://jcm.asm.org/
channel was considered sufficient for the analysis. In our study, a Gram-negative bacterium was reported in 104 of the 105 samples with an identification result. In one specimen containing Rhizobium radiobacter, C. glabrata was reported only by the Accelerate Pheno system. Overall, in 95 (91.3%) of these 104 samples AST results were reported. AST data were not generated by the Accelerate Pheno system in the follow-ing cases: 10 unidentified specimens, two isolate misidentifications, four polymicrobial specimens with mixed Gram-negative infections, and four monomicrobial blood culture specimens (Table 1).
[image:3.585.42.546.80.543.2]A total of 987 AST results were produced and compared to the culture-based AST results of Vitek 2 and Etest. For 11 (1.1%) AST measurements, a discordant result between the Vitek 2 and the Etest could not be resolved by repeating the tests, and
TABLE 1Overview of discrepant identification results and polymicrobial BSI infectionsa
Infection type
Organism(s) identified (no. of results)
Comment
Culture ID Accelerate Pheno ID
Monomicrobial K. pneumoniae (2) No identification (2) No identification, no AST
B. fragilis(3) No identification (3) Bacterium not included in ID panel, no AST
M. morganii(1) No identification (1) Bacterium not included in ID panel, no AST
A. radioresistens(1) No identification (1) Bacterium not included in ID panel, no AST
H. alvei(1) No identification (1) Bacterium not included in ID panel, no AST
S. paucimobilis(1) No identification (1) Bacterium not included in ID panel, no AST
M. nonliquefaciens(1) No identification (1) Bacterium not included in ID panel, no AST
E. coli(1) E. coli,Klebsiellaspecies (1) False identification, additional organism detected, no AST S. rubidaea(1) S. marcescens(1) False identification, not included in
ID panel
R. radiobacter(1) C. glabrata(1) False identification, not included in ID panel, no AST
E. coli(2) E. coli,C. glabrata(2) Additional organism detected K. pneumoniae(2) Klebsiellaspecies,S. aureus(1);
Klebsiellaspecies,E. faecium(1)
Additional organism detected
S. marcescens(1) S. marcescens,C. glabrata(1) Additional organism detected
Polymicrobial P. aeruginosa,C. krusei P. aeruginosa,S. aureus Gram-negative organisms detected correctly
E. coli,S. simulans,S. hominis E. coli Gram-negative organisms detected correctly
C. freundii,E. faecalis Citrobacterspecies Gram-negative organisms detected correctly
E. coli,P. vulgaris,C. freundii E. coli,Proteusspecies,Citrobacter species
Gram-negative organisms detected correctly, no AST
S. marcescens,E. faecalis S. marcescens Gram-negative organisms detected correctly
K. pneumoniae,E. faecalis Klebsiellaspecies,E. faecalis Gram-negative organisms detected correctly, no AST
E. coli,K. pneumoniae,K. oxytoca, S. lutetiensis
E. coli,Klebsiellaspecies Gram-negative organisms detected correctly, no AST
K. pneumoniae,E. faecalis Klebsiellaspecies Gram-negative organisms detected correctly
K. pneumoniae,E. coli,E. faecalis, E. casseliflavus
Klebsiellaspecies,E. coli,E. faecalis Gram-negative organisms detected correctly, no AST
E. coli,E. faecalis E. coli Gram-negative organisms detected correctly
aThe Accelerate Pheno system correctly identified 102 of 115 (88.7%) blood culture specimens with Gram-negative organisms. No identification (ID) was achieved in
10 specimens, and a false identification was made for three samples. In six of the monomicrobial BSI an additional organism was identified by the Accelerate Pheno system. In the polymicrobial BSI, all Gram-negative organisms were correctly identified. Overall, AST data were generated by the Accelerate Pheno system in 95 of 115 (82.6%) specimens included in the study. No AST result was generated in 20 samples, including 10 samples without pathogen ID, two falsely identified samples, four polymicrobial specimens, and four monomicrobial blood culture samples.
on May 16, 2020 by guest
http://jcm.asm.org/
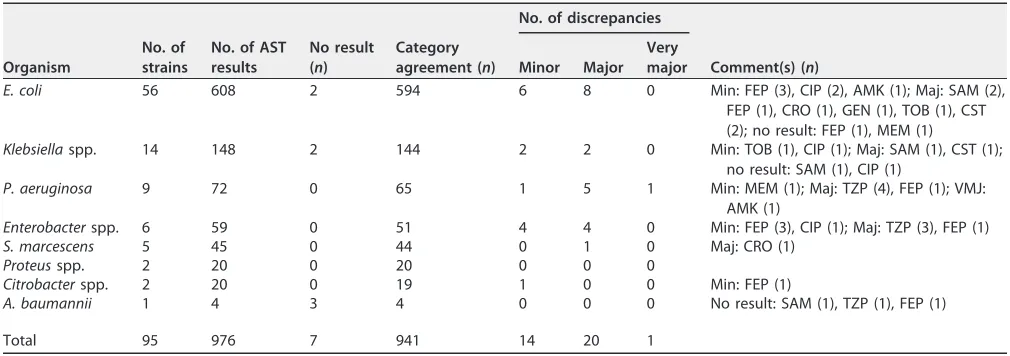
thus no gold standard AST result was determined. These measurements were excluded from the analysis, resulting in 976 AST measurements available for evaluation. Detailed results are displayed in Tables 2 and 3.
The overall category agreement (CA) between the Accelerate Pheno system and culture-based AST was 96.4%, the rate for minor discrepancies 1.4%, major discrepan-cies 2.3%, and very major discrepandiscrepan-cies 1.0%. The highest CA was observed for ertapenem (100%), followed by meropenem (98.9%) and gentamicin (98.9%). A low CA was detected for cefepime (88.9%) and piperacillin-tazobactam (92.3%). Most major discrepancies were detected for beta-lactam antibiotics, with ampicillin-sulbactam and piperacillin-tazobactam having the highest rates with 8.8 and 8.2%, respectively (Table 2). The major errors for ampicillin-sulbactam occurred in E. coli(n⫽2) andK.
pneu-moniae(n⫽1), whereas the major errors for piperacillin-tazobactam were observed in
Enterobacterspp. (n⫽3) andP. aeruginosa(n⫽4). Only one very major discrepancy
[image:4.585.42.550.83.262.2]was observed for amikacin in a bloodstream infection withP. aeruginosa. The Acceler-ate Pheno system did not provide AST results for 7 (0.7%) AST measurements, although
TABLE 2AST results of the Accelerate Pheno system compared to culture-based ASTa
Antimicrobial agent
Accelerate Pheno system AST Culture-based AST (no.)
No. of AST results
No. (%) of category agreements
No. (%) of minor discrepancies
No. (%) of major discrepancies
No. (%) of very major
discrepancies Susceptible Resistant
S R/I Total
SAM 66 31 32 63 (95.5) 0 (0) 3 (8.8) 0 (0) 34 32
TZP 91 78 6 84 (92.3) 0 (0) 7 (8.2) 0 (0) 85 6
FEP 90 73 6/1* 80 (88.9) 7 (7.8) 3 (3.6) 0 (0) 83 6/1*
CRO 85 75 8 83 (97.6) 0 (0) 2 (2.6) 0 (0) 77 8
ETP 85 85 0 85 (100) 0 (0) 0 (0) 0 (0) 85 0
MEM 94 91 2 93 (98.9) 1 (1.1) 0 (0) 0 (0) 91 3
AMK 95 91 2 93 (97.9) 1 (1.1) 0 (0) 1 (33.3) 92 3
GEN 94 84 9 93 (98.9) 0 (0) 1 (1.2) 0 (0) 85 9
TOB 94 82 10 92 (97.9) 1 (1.1) 1 (1.2) 0 (0) 84 10
CIP 94 69 21 90 (95.7) 4 (4.3) 0 (0) 0 (0) 73 21
CST 88 85 0 85 (96.6) 0 (0) 3 (3.4) 0 (0) 88 0
Total 976 844 97 941 (96.4) 14 (1.4) 20 (2.3) 1 (1.0) 876 100
aThe overall category agreement was 96.4%. Minor discrepancies, major discrepancies, and very major discrepancies were detected in 1.4, 2.3, and 1.0%, respectively. *, One strain showed an intermediate result for FEP in the Accelerate Pheno system and culture-based ASTs. AMK, amikacin; SAM, ampicillin-sulbactam; FEP, cefepime; CRO, ceftriaxone; CIP, ciprofloxacin; GEN, gentamicin; MEM, meropenem; TZP, piperacillin-tazobactam; TOB, tobramycin; CST, colistin; ETP, ertapenem. S, susceptible; R/I, resistant/intermediate.
TABLE 3AST results of the Accelerate Pheno system compared to culture-based AST for 95 Gram-negative pathogens included in the
studya
Organism
No. of strains
No. of AST results
No result (n)
Category agreement (n)
No. of discrepancies
Comment(s) (n)
Minor Major
Very major
E. coli 56 608 2 594 6 8 0 Min: FEP (3), CIP (2), AMK (1); Maj: SAM (2), FEP (1), CRO (1), GEN (1), TOB (1), CST (2); no result: FEP (1), MEM (1)
Klebsiellaspp. 14 148 2 144 2 2 0 Min: TOB (1), CIP (1); Maj: SAM (1), CST (1); no result: SAM (1), CIP (1)
P. aeruginosa 9 72 0 65 1 5 1 Min: MEM (1); Maj: TZP (4), FEP (1); VMJ: AMK (1)
Enterobacterspp. 6 59 0 51 4 4 0 Min: FEP (3), CIP (1); Maj: TZP (3), FEP (1) S. marcescens 5 45 0 44 0 1 0 Maj: CRO (1)
Proteusspp. 2 20 0 20 0 0 0
Citrobacterspp. 2 20 0 19 1 0 0 Min: FEP (1)
A. baumannii 1 4 3 4 0 0 0 No result: SAM (1), TZP (1), FEP (1)
Total 95 976 7 941 14 20 1
aAMK, amikacin; SAM, ampicillin-sulbactam; FEP, cefepime; CRO, ceftriaxone; CIP, ciprofloxacin; GEN, gentamicin; MEM, meropenem; TZP, piperacillin-tazobactam; TOB,
tobramycin; CST, colistin; ETP, ertapenem. Maj, major discrepancy; Min, minor discrepancy; VMJ, very major discrepancy.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:4.585.40.545.544.722.2]other AST measurements of other antibiotics were successfully accomplished in these specimens (Table 3).
The study included a total of 13 strains resistant either to piperacillin-tazobactam, ceftriaxone or carbapenems, including 7 extended-spectrum beta-lactamase (ESBL)-positive strains and three multidrug-resistantP. aeruginosaisolates. For these antibi-otics, the Accelerate Pheno system correctly detected resistant phenotype in all iso-lates, as summarized in Table 4. However, in two specimens with pathogens harboring chromosomal AmpC beta-lactamases (M. morganii andH. alvei), no ASTs were con-ducted since the species are not included in the identification panel of the Accelerate Pheno system.
Comparison of time to result between Accelerate Pheno system and culture-based diagnostics.During the study period, two Accelerate Pheno system modules were available, allowing us to test two samples at a time. The Accelerate Pheno system was started with median times of 8.13 h (interquartile range [IQR]⫽2.63 to 13.38 h) after the blood culture was flagged positive in the blood culture incubator and 2.23 h (IQR ⫽ 1.42 to 3.02 h) after the start of processing the positive blood culture. No negative impact on identification and AST was observed for samples that were ana-lyzed in the Accelerate Pheno system later than 8 h after the blood culture was flagged positive (results summarized in Table S1 in the supplemental material).
Identification.The calculation of median time starting with initial processing of the positive blood culture to identification results was available in 95 samples excluding polymicrobial BSI infections. After the start of processing the positive-flagged blood culture, median time to Gram stain results was 1.53 h (IQR⫽0.97 to 2.12 h), while the median time to the Accelerate Pheno system identification results was 3.58 h (IQR⫽ 2.75 to 4.38 h) and the median time to the identification results of the grown bacterial culture was 31.07 h (IQR⫽28.82 to 46.55 h). The median run time of the Accelerate Pheno system for identification was 1.35 h (IQR⫽1.35 to 1.35 h). In comparing median time to identification, we found that the Accelerate Pheno system enabled pathogen identification 27.49 h (P⬍0.0001) before culture-based identification.
Antimicrobial susceptibility testing.The calculation of the time to result for AST is based on 89 specimens and refers to the Vitek 2 AST results obtained in the routine diagnostics workflow not including E-Tests for amikacin, ceftriaxone, ertapenem, and colistin. Median time to AST results with the Accelerate Pheno system was 8.88 h (IQR⫽ 8.10 to 9.67 h) after the start of positive blood culture processing compared to the median time to the culture-based AST of 49.27 h (IQR⫽46.00 to 49.80 h). The median duration of the Accelerate Pheno system test run was 6.65 h (IQR⫽6.63 to 6.67 h) for both identification and AST. In summary, the application of the Accelerate Pheno system made AST results available 40.39 h (P⬍0.0001) earlier compared to conven-tional culture-based AST.
DISCUSSION
Our results represent one of the first studies to evaluate the performance of the Accelerate Pheno system for identification and AST directly from positive blood culture bottles in a routine diagnostic setting.
Identification of Gram-negative organisms was successfully achieved in 102 of 115 (88.7%) blood cultures, including 10 polymicrobial BSI. Considering only BSI episodes with organisms covered by the identification panel, successful identification was ob-tained in 102 of 105 (97.1%) positive blood cultures. Only one false-positive Gram-negative organism was detected in anE. coliBSI, in which the Accelerate Pheno system additionally reportedKlebsiellaspecies. The sensitivity values are comparable to pub-lished performance data for the molecular Verigene Gram-negative blood culture assay (Nanosphere, IL) (14–19), as well as the BioFire FilmArray blood culture identification panel (BioFire; bioMérieux SA, USA) for the detection of Gram-negative, Gram-positive, and fungal pathogens (11, 12, 20–24).
In total, 10 polymicrobial BSI were included in our study, in which the Accelerate Pheno system could correctly identify all Gram-negative organisms in a single sample.
on May 16, 2020 by guest
http://jcm.asm.org/
TABLE 4 Overview of MIC results of the Accelerate Pheno system and the Etests in isolates resistant to piperacillin-tazobactam, ceftriaxone, ertapenem, or meropenem a Isolate ( n ⴝ 13) Test b MIC ( g/ml) c Comment SAM TZP FEP CRO ETP MEM AMK GEN TOB CIP CST C. freundii (1) ACC – 128 (R) ⱕ 1 (S) ⱖ 8 (R) 0.25 (S) ⱕ 0.25 (S) ⱕ 4 (S) ⱕ 1 (S) ⱕ 1 (S) ⱕ 0.25 (S) ⱕ 0.5 (S) AmpC positive Etest ND ⬎ 256 (R) 1 (S) ⬎ 32 (R) 0.094 (S) 0.047 (S) 1.5 (S) 0.25 (S) 1 (S) 0.047 (S) 1.5 (S) E. coli (2) ACC 4 (S) ⱕ 4 (S) ⱕ 1 (S) ⱖ 8 (R) 0.25 (S) ⱕ 0.25 (S) ⱕ 4 (S) ⱕ 1 (S) ⱕ 1 (S) ⱕ 0.25 (S) ⱕ 0.5 (S) ESBL positive Etest 6 (S) 0.75 (S) * ⬎ 32 (R) 0.012 (S) 0.032 (S) 2 (S) 0.5 (S) 0.75 (S) 0.5 (S) 1 (S) E. coli (3) ACC ⱖ 64 (R) ⱕ 4 (S) 16 (R) ⱖ 8 (R) ⱕ 0.125 (S) ⱕ 0.25 (S) ⱕ 4 (S) 16 (R) 16 (R) ⱖ 8 (R) ⱕ 0.5 (S) ESBL positive Etest 24 (R) 2 (S) * ⬎ 32 (R) 0.012 (S) 0.023 (S) 4 (S) 24 (R) 24 (R) ⬎ 32 (R) 0.75 (S) E. coli (4) ACC ⱖ 64 (R) ⱕ 4 (S) 2 (I) ⱖ 8 (R) 0.25 (S) ⱕ 0.25 (S) ⱕ 4 (S) ⱕ 1 (S) ⱕ 1 (S) ⱖ 8 (R) 2 (S) ESBL positive Etest 24 (R) 0.5 (S) 4 (I) ⬎ 32 (R) 0.008 (S) 0.016 (S) 2 (S) 0.75 (S) 0.75 (S) ⬎ 32 (R) 1 (S) E. coli (5) ACC ⱖ 64 (R) 128 (R) ⱕ 1 (S) 0.5 (S) 0.25 (S) ⱕ 0.25 (S) ⱕ 4 (S) ⱕ 1 (S) ⱕ 1 (S) ⱖ 8 (R) ⱕ 0.5 (S) CAZ, CTX susceptible Etest ⬎ 256 (R) ⬎ 256 (R) 0.38 (S) 0.125 (S) 0.012 (S) 0.032 (S) 2 (S) 0.5 (S) 0.75 (S) ⬎ 32 (R) 2 (S) E. coli (6) ACC ⱖ 64 (R) ⱕ 4 (S) ⱖ 32 (R) ⱖ 8 (R) 0.25 (S) ⱕ 0.25 (S) 16 (I) 2 (S) ⱖ 32 (R) ⱖ 8 (R) 2 (S) ESBL positive Etest 64 (R) 4 (S) 12 (R) ⬎ 32 (R) 0.012 (S) 0.023 (S) 8 (S) 0.5 (S) 16 (R) ⬎ 32 (R) 1.5 (S) E. coli (7) ACC ⱖ 64 (R) 128 (R) ⱕ 1 (S) ⱕ 0.25 (S) ⱕ 0.125 (S) ⱕ 0.25 (S) ⱕ 4 (S) 16 (R) 16 (R) ⱖ 8 (R) ⱕ 0.5 (S) CAZ, CTX susceptible Etest ⬎ 256 (R) 64 (R) 1 (S) 0.094 (S) 0.008 (S) 0.016 (S) 1 (S) 12 (R) 16 (R) ⬎ 32 (R) 1 (S) E. coli (8) ACC 16 (R) ⱕ 4 (S) ⱕ 1 (S) ⱖ 8 (R) 0.25 (S) ⱕ 0.25 (S) ⱕ 4 (S) 2 (S) ⱕ 1 (S) ⱖ 8 (R) ⱕ 0.5 (S) ESBL positive Etest * 0.38 (S) * ⬎ 32 (R) 0.006 (S) 0.012 (S) 1 (S) 0.38 (S) 0.75 (S) ⬎ 32 (R) 0.75 (S) E. coli (9) ACC 32 (R) ⱕ 4 (S) 16 (R) ⱖ 8 (R) 0.25 (S) ⱕ 0.25 (S) ⱕ 4 (S) ⱕ 1 (S) ⱕ 1 (S) ⱕ 0.25 (S) ⱕ 0.5 (S) ESBL positive Etest 16 (R) 0.5 (S) 6 (R) ⬎ 32 (R) 0.012 (S) 0.016 (S) 0.75 (S) 0.25 (S) 0.5 (S) 0.094 (S) 1 (S) E. coli (10) ACC ⱖ 64 (R) ⱕ 4 (S) ⱖ 32 (R) ⱖ 8 (R) 0.25 (S) ⱕ 0.25 (S) ⱕ 4 (S) 16 (R) 8 (R) ⱖ 8 (R) 2 (S) ESBL positive Etest 64 (R) 0.75 (S) 16 (R) ⬎ 32 (R) 0.023 (S) 0.032 (S) 1.5 (S) 0.5 (S) 1 (S) ⬎ 32 (R) 1 (S) P. aeruginosa (11) ACC – 128 (R) 32 (R) – – ⱖ 16 (R) ⱖ 128 (R) ⱖ 32 (R) ⱖ 32 (R) ⱖ 8 (R) ⱕ 0.5 (S) MDR phenotype Etest ND ⬎ 256 (R) 96 (R) ND ND ⬎ 32 (R) 24 (R) ⬎ 256 (R) ⬎ 256 (R) ⬎ 32 (R) 2 (S) P. aeruginosa (12) ACC – 128 (R) 32 (R) – – 4 (I) ⱕ 4 (S) 16 (R) 16 (R) ⱖ 8 (R) ⱕ 0.5 (S) MDR phenotype Etest ND ⬎ 256 (R) ⬎ 256 (R) ND ND ⬎ 32 (R) 16 (I) ⬎ 256 (R) ⬎ 256 (R) ⬎ 32 (R) 1.5 (S) P. aeruginosa (13) ACC – 128 (R) 32 (R) – – ⱖ 16 (R) ⱖ 128 (R) 16 (R) ⱖ 32 (R) ⱖ 8 (R) ⱕ 0.5 (S) MDR phenotype Etest ND 12 (S) 24 (R) ND ND ⬎ 32 (R) 24 (R) 16 (R) 24 (R) ⬎ 32 (R) 0.75 (S) a In all, seven E. coli isolates were third-generation cephalosporin-resistant ESBL producers, and three P. aeruginosa isolates had a multidrug-resistant phenotype. The nonsusceptible phenotype was correctly detected by the Accelerate Pheno system for piperacillin-tazobactam, ceftriaxone, and meropenem in all 13 isolates (identified parenthetically as isolates 1 to 13 in column 1). b ACC, Accelerate Pheno. c Isolates are identified parenthetically as resistant (R), susceptible (S), or intermediate (I). * , Discrepant result between the Vitek 2 and the Etest were excluded from the evaluation study. –, The AST measurement was not performed by the Accelerate Pheno system for the antibiotic-pathogen combination. MDR, multidrug resistant; ND, not done; AMK, amikacin; CAZ, ceft azidime; CIP, ciprofloxacin; CRO, ceftriaxone; CST, colistin; CTX, cefotaxime; ETP, ertapenem; FEP, cefepime; GEN, gentamicin; MEM, meropenem; SAM, ampicillin-sulbactam; TOB, tobramycin; TZP, piperacillin-taz obactam.
on May 16, 2020 by guest
http://jcm.asm.org/
[image:6.585.58.374.75.736.2]However, in seven of these samples, cultivated Gram-positive organisms were not detected. Of note, the Accelerate Pheno system detected two or more organisms in six monomicrobial BSI infections, namely,C. glabrata(n⫽3),S. aureus(n⫽1),
Enterococ-cus faecium(n⫽1), andKlebsiellaspecies (n⫽1). This emphasizes the need for further
evaluation of the system, in particular for Gram-positive and fungal BSI, applying the newly released software version 1.2, including an optimized identification algorithm. A total of 10 specimens yielded no identification at all, of which 8 were not covered by the Accelerate PhenoTest BC kit identification panel. However, some of these organ-isms, e.g.,Bacteroidesspecies, might be of clinical importance. Anaerobic bacteria have been reported to be isolated from up to 4.1% of positive blood culture samples (25). Members of theBacteroides fragilisgroup are the most prevalent anaerobic pathogens recovered with 45% (25) and are associated with a high mortality rate up to 25% (26). Anaerobic incubation and growth rates usually prolong time to identification by conventional methods, with 45.13 h for the three isolates in this study compared to a median time to identification of 31.07 h (IQR ⫽ 28.82 to 46.55 h). H. alvei and M.
morganiiare also not covered by the Accelerate PhenoTest BC kit identification panel.
Both species were detected in one blood culture, each corresponding to 1.8% of the BSI episodes included in the study. AlthoughH. alveiandM. morganiihave been reported as rare causes of sepsis (27, 28), both species harbor a chromosomal AmpC beta-lactamase (29).H. alveiandM. morganiiare considered to be intrinsically resistant to ampicillin, amoxicillin-clavulanic acid, and ampicillin-sulbactam, and the use of cefo-taxime, ceftriaxone, or ceftazidime as monotherapy is discouraged againstM. morganii
due to the risk of selecting derepressed AmpC-resistant populations (30). In addition,M.
morganii is considered intrinsically resistant to colistin and, as for H. alvei, a high
percentage of colistin resistance has been described in wild-type isolates (30, 31). AST data were generated in 95 of the 104 (91.3%) specimens in which the Accelerate Pheno system identified a Gram-negative organism. The system was not able to perform AST in four polymicrobial infections (3.8%), one misidentified specimen (1.0%), and four monobacterial infections (3.8%). The monobacterial infections included three
E. coliand oneK. pneumoniaeinfections, all without a special growth morphology or
resistance phenotype. In addition, the time period from the positive flagged bottle to starting the Accelerate Pheno system was not prolonged in these isolates (8.95, 7.97, 4.98, and 6.13 h) compared to a median starting time of 8.13 h (IQR⫽2.63 to 13.38 h). The overall category agreement of the 976 AST results was 96.4% with minor, major, and very major discrepancies occurring at a rate of 1.4, 2.3, and 1.0%, respectively. Major error discrepancies for piperacillin-tazobactam (n ⫽ 7) were observed for P.
aeruginosaandEnterobacterspp. The AST for piperacillin-tazobactam andP. aeruginosa
has been optimized in the newly released software version 1.2.
In the study, seven ESBL-producingE. coliand three MDRP. aeruginosaisolates were included. Notably, the Accelerate Pheno system correctly detected resistances to piperacillin-tazobactam, ceftriaxone and carbapenems, while not generating false-susceptible AST results in these strains (Table 4). This clearly demonstrates the potential of the Accelerate Pheno system to detect MDR phenotypes in a timely manner in order to enable adequate patient therapy as quickly as possible. This is important in our hospital setting, since mortality rates caused byP. aeruginosaBSI ranged between 34 and 61% for non-metallo-beta-lactamase (MBL) producers and MBL-positiveP. aerugi-nosa strains, respectively (32). The Accelerate PhenoTest BC kit AST panel has been extended in software version 1.2 by ceftazidime and aztreonam after this study cohort was finalized, introducing two more important antibiotics for ESBL screening and the treatment of Gram-negative infections (33). However, more studies involving a larger proportion of MDR and XDR organisms, including colistin-resistant isolates, are needed to further evaluate the system performance on these organisms.
We observed that the Accelerate Pheno system rapidly increased identification by 27.49 h in comparison to culture-based identification in our setting. The culture-based AST results were available approximately 49.27 h (IQR ⫽ 46.00 to 49.80 h) after processing began for positive blood cultures. In contrast, the Accelerate Pheno system
on May 16, 2020 by guest
http://jcm.asm.org/
AST results were available within approximately 8.88 h (IQR⫽8.10 to 9.67 h), which is 40.39 h faster than the culture results. This reduction in time to result for blood culture diagnostics is particularly evident in the setting of our academic microbiology labora-tory, with reduced operating hours during the night. Although the trend is moving toward a 24/7 model (34), limited service during night shifts represents the reality for many academic microbiology departments in various countries, often due to the lack of automation and trained personnel (34–36).
The availability of rapid identification and AST results in Gram-negative bloodstream infections has a great impact on patient outcome and length of hospital stay, as well as on the effectiveness of antibiotic stewardship programs. Various studies have addressed these aspects to optimize patient management and outcome. It was previ-ously shown that during empirical treatment up to 58% of the patients were found to receive inadequate therapy (37), which was associated with increased mortality (37, 38) and a prolonged hospital stay after Gram-negative BSI (39). Thus, faster identification of blood culture pathogens was associated with a shorter time for adequate therapy (40) and decreased mortality in combination with antibiotic stewardship programs (ASP) (41). In addition, another study showed that the introduction of PCR-based blood culture identification in combination with ASP enabled an earlier de-escalation of antibiotic therapy compared to ASP alone (23). However, comparison of these studies remains difficult, since the real impact of rapid diagnostic tool depends on various factors (e.g., patient characteristics, local therapeutic guidelines, and laboratory service hours) and needs to be determined in the local setting.
Usually, treatment escalation and de-escalation strategies based only on identifica-tion results rely on the retrospective antimicrobial susceptibility data of a particular epidemiological setting that run the risk of individual patients receiving inappropriately narrow or broad antibiotic therapy. Therefore, a rapid assay capable of generating fast identification and AST results has the potential for allowing faster adequate therapy, as well as targeted ASP measures, most likely reducing the risk of inappropriate therapy in the individual case. However, to determine the specific additional impact of the rapid AST of the Accelerate Pheno system on clinical decisions and outcomes, larger clinical trials in various epidemiological settings will still be needed, including trials comparing the system to rapid ID-only strategies as a baseline, provided by systems such as the BioFire FilmArray blood culture identification panel and the Verigene blood culture assays. One limitation is that the Accelerate Pheno system can currently only process one sample at a time per system module. The system can be set up with four to eight modules and is not as yet suitable for large-scale sample processing. Also, the deploy-ment of selection and stratification algorithms adapted to the epidemiological situation and patient population is recommended in order to utilize the system in producing fast results for patients with the greatest need.
In conclusion, the Accelerate Pheno system was shown to produce good results in terms of identification and AST of Gram-negative organisms from positive blood cultures. In our setting, the identification results and AST results were available ap-proximately 27.49 and 40.39 h faster, respectively, compared to culture-based diagnos-tics. We therefore find the Accelerate Pheno system to be a valuable tool in improving the turnaround time in blood culture diagnostics, which could prove significant in therapeutic management, especially in high-risk patients.
MATERIALS AND METHODS
Study, samples, and laboratory settings.The study was performed from April 2016 to October 2016 at a tertiary university hospital in Southern Germany in accordance with the local ethics committee (no. 139/2016BO2). The patient cohort comprised inpatients and patients presenting at the emergency department of a 1,500-bed tertiary university hospital and a 340-bed trauma clinic located on same campus. Our laboratory received 12,779 aerobic blood culture bottles in 2016, of which 1,304 (10.2%) were positive.
The first positive blood culture of each patient with Gram-negative rods in the initial Gram stain was included in the study. Specimens with Gram-positive organisms or fungi in the initial Gram-stain of the positive blood culture bottle were not included in the study. Laboratory operation hours are weekdays
on May 16, 2020 by guest
http://jcm.asm.org/
from 7:30 a.m. to 5:30 p.m. and weekends from 7:30 a.m. to 3 p.m. Blood cultures are processed every morning and during the operating hours as soon as they are flagged positive.
Blood culture diagnostics.Blood culture bottles were incubated in the Bactec 9240 blood culture instrument (BD Diagnostic Systems, Franklin Lakes, NJ). The routine diagnostic workflow included subcultures of the positive blood culture bottles, followed by MALDI-TOF MS (Microflex LT; Bruker Daltonics, Germany) and supplemented, when necessary, by the Vitek 2 identification system (bioMéri-eux SA, France) to achieve identification on the species level.
AST was performed using the Vitek 2 (AST N232 card; bioMérieux, SA, France). All bacterial isolates
were stored at⫺80°C for further analysis. During the study period, the initial routine Vitek 2 AST was
repeated and confirmed by Etest MIC determination (Liofilchem s.r.l., Italy) for all reported antibiotics. Since amikacin, ceftriaxone, ertapenem, and colistin were not included in the routine diagnostic Vitek 2 AST card, MICs were exclusively determined by Etest. Results were interpreted according to the guidelines
set by the European Committee on Antimicrobial Susceptibility Testing (EUCAST;http://www.eucast.org/
fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_6.0_Breakpoint_table.pdf).
We ran the Accelerate PhenoTest BC kit (Accelerate Diagnostics, USA) on the Accelerate Pheno system on blood culture bottles flagged positive after first obtaining the Gram stain result. According to the manufacturer’s instructions, it is recommended to apply the Accelerate Pheno system within 8 h after the blood culture bottle is flagged positive. However, due to our operating hours we extended this time period and accepted samples that we could process within 24 h after the positive signal in the blood culture incubator. According to the manufacturer’s instructions, 5-ml portions from the blood culture bottle were transferred into the sample vial. The test system was then started, lasting a total of approximately 2 min in hands-on time. Two Accelerate Pheno system modules were available for the study period, allowing for the processing of two samples at a time. The analysis software, Accelerate Diagnostics Host applications, version 1.1.0.69, generated a report of the findings automatically. The
Accelerate Pheno system identified the following Gram-negative organisms:Escherichia coli,Klebsiella
spp.,Enterobacterspp.,Proteusspp.,Citrobacterspp.,Serratia marcescens,Acinetobacter baumannii, and
Pseudomonas aeruginosa. AST was performed for ampicillin-sulbactam (E. coli,Klebsiellaspp.,Proteusspp.,
and A. baumannii), piperacillin-tazobactam, ceftriaxone (not for P. aeruginosa and A. baumannii),
cefepime, ertapenem (not forP. aeruginosaandA. baumannii), meropenem, amikacin, gentamicin (not
forA. baumannii), tobramycin (not forA. baumannii), ciprofloxacin, and colistin (not forProteusspp. and
S. marcescens).
Gold standard definition.The culture-based identification was defined as the gold standard for bacterial identification. For antimicrobials included in the AST Vitek 2 card, the Vitek 2 AST results and the Etest results for these antimicrobials were evaluated. The consensus result of the Vitek 2 and the Etest was considered the gold standard for AST. In case no category agreement was obtained in the initially performed Vitek 2 and the subsequently performed Etest, both tests were repeated to resolve the discrepancy. If a concordant result (S, I, or R) was obtained in three of the four test results, this was considered correct. For antimicrobials not included in the Vitek 2 AST (amikacin, ceftriaxone, ertapenem, and colistin) the Etest result was considered the gold standard. In case a discrepancy from the Accelerate
Pheno system result was observed for these four antimicrobials (n⫽5), the Etest was repeated twice to
rule out a mistake in the laboratory. If a concordant result (S, I, or R) was obtained in two of the three test results, this was considered correct.
Data analysis.The Accelerate Pheno system identification results were compared against results from culture-based identification. The identification was considered correct if the Gram-negative organ-ism yielded the same results in both methods, with no additional Gram-negative organorgan-isms detected or failing to be detected. Fungi and Gram-positive identification results were not taken into account.
The Accelerate Pheno system AST results were compared to the culture-based gold standard, which consists of the Vitek 2 and Etest result (see above). The total category agreement (CA) was determined, and the discrepant results were categorized as follows: very major discrepancy (false susceptibility), major discrepancy (false resistance), or minor discrepancy (intermediate versus susceptible or resistant). The rate of very major discrepancies (VMJ) was calculated by dividing the number of very major discrepancies by the number of resistant strains tested and multiplied by 100, while the rate of major discrepancies (Maj) was calculated by dividing the number of major discrepancies by the number of susceptible strains tested and multiplied by 100. The rate of minor discrepancies (Min) was calculated by dividing the number of minor discrepancies by the total number of strains tested multiplied by 100. The three rates have units in percent (%).
D’Agostino’s K-squared test was used to check for normality. Skewed data were presented in medians and IQRs. The presence of equal variances between groups was examined by using a Bartlett’s test. In the case of a positive Bartlett’s test result, hypothesis testing was carried out using the Wilcoxon rank sum
test; otherwise, a pairedttest was used. All analyses were performed using Stata version 12.1 (Stat Corp.,
College Station, TX).
SUPPLEMENTAL MATERIAL
Supplemental material for this article may be found athttps://doi.org/10.1128/JCM
.00181-17.
SUPPLEMENTAL FILE 1,PDF file, 0.3 MB.
on May 16, 2020 by guest
http://jcm.asm.org/
ACKNOWLEDGMENTS
The study was funded in part by the Institute of Medical Microbiology and Hygiene, Medical Faculty, University of Tübingen, Tübingen, Germany.
We thank the team of diagnostic technicians for their expert technical assistance. Two Accelerate Pheno system modules and the test reagents were provided by Accelerate Diagnostics, Inc., Tucson, AZ, for the study period. Accelerate Diagnostics had no role in study design, data collection and interpretation, or the decision to submit the work for publication.
We have no conflict of interest to disclose.
REFERENCES
1. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. 2001. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 29:
1303–1310.https://doi.org/10.1097/00003246-200107000-00002.
2. Mayr FB, Yende S, Angus DC. 2014. Epidemiology of severe sepsis.
Virulence 5:4 –11.https://doi.org/10.4161/viru.27372.
3. Pittet D, Tarara D, Wenzel RP. 1994. Nosocomial bloodstream infection in critically ill patients: excess length of stay, extra costs, and attributable
mortality. JAMA 271:1598 –1601. https://doi.org/10.1001/jama.1994
.03510440058033.
4. Bauer KA, Perez KK, Forrest GN, Goff DA. 2014. Review of rapid diagnostic tests used by antimicrobial stewardship programs. Clin Infect Dis
59(Suppl 3):S134 –S145.https://doi.org/10.1093/cid/ciu547.
5. Savinelli T, Parenteau S, Mermel LA. 2004. What happens when auto-mated blood culture instrument detect growth but there are no tech-nologists in the microbiology laboratory? Diagn Microbiol Infect Dis
48:173–174.https://doi.org/10.1016/j.diagmicrobio.2003.10.001.
6. Clerc O, Prod’hom G, Vogne C, Bizzini A, Calandra T, Greub G. 2013. Impact of matrix-assisted laser desorption ionization time-of-flight mass spectrometry on the clinical management of patients with Gram-negative bacteremia: a prospective observational study. Clin Infect Dis
56:1101–1107.https://doi.org/10.1093/cid/cis1204.
7. La Scola B, Raoult D. 2009. Direct identification of bacteria in positive blood culture bottles by matrix-assisted laser desorption ionization
time-of-flight mass spectrometry. PLoS One 4:e8041.https://doi.org/10.1371/
journal.pone.0008041.
8. Fiori B, D’Inzeo T, Giaquinto A, Menchinelli G, Liotti FM, de Maio F, De Angelis G, Quaranta G, Nagel D, Tumbarello M, Posteraro B, Sanguinetti M, Spanu T. 2016. Optimized use of the MALDI BioTyper system and the FilmArray BCID panel for direct identification of microbial pathogens
from positive blood cultures. J Clin Microbiol 54:576 –584.https://doi
.org/10.1128/JCM.02590-15.
9. Vlek AL, Bonten MJ, Boel CH. 2012. Direct matrix-assisted laser desorp-tion ionizadesorp-tion time-of-flight mass spectrometry improves
appropriate-ness of antibiotic treatment of bacteremia. PLoS One 7:e32589.https://
doi.org/10.1371/journal.pone.0032589.
10. Salimnia H, Fairfax MR, Lephart PR, Schreckenberger P, DesJarlais SM, Johnson JK, Robinson G, Carroll KC, Greer A, Morgan M, Chan R, Loef-felholz M, Valencia-Shelton F, Jenkins S, Schuetz AN, Daly JA, Barney T, Hemmert A, Kanack KJ. 2016. Evaluation of the FilmArray blood culture identification panel: results of a multicenter controlled trial. J Clin
Mi-crobiol 54:687– 698.https://doi.org/10.1128/JCM.01679-15.
11. Ward C, Stocker K, Begum J, Wade P, Ebrahimsa U, Goldenberg SD. 2015.
Performance evaluation of the Verigene®(Nanosphere) and FilmArray®
(BioFire®) molecular assays for identification of causative organisms in bacterial bloodstream infections. Eur J Clin Microbiol Infect Dis 34:
487– 496.https://doi.org/10.1007/s10096-014-2252-2.
12. Altun O, Almuhayawi M, Ullberg M, Ozenci V. 2013. Clinical evaluation of the FilmArray blood culture identification panel in identification of bacteria and yeasts from positive blood culture bottles. J Clin Microbiol
51:4130 – 4136.https://doi.org/10.1128/JCM.01835-13.
13. Walker T, Dumadag S, Lee CJ, Lee SH, Bender JM, Cupo Abbott J, She RC. 2016. Clinical impact of laboratory implementation of Verigene BC-GN microarray-based assay for detection of gram-negative bacteria in
pos-itive blood cultures. J Clin Microbiol 54:1789 –1796.https://doi.org/10
.1128/JCM.00376-16.
14. Ledeboer NA, Lopansri BK, Dhiman N, Cavagnolo R, Carroll KC, Granato P, Thomson R, Jr, Butler-Wu SM, Berger H, Samuel L, Pancholi P, Swyers
L, Hansen GT, Tran NK, Polage CR, Thomson KS, Hanson ND, Winegar R, Buchan BW. 2015. Identification of Gram-negative bacteria and genetic resistance determinants from positive blood culture broths by use of the Verigene Gram-negative blood culture multiplex microarray-based
mo-lecular assay. J Clin Microbiol 53:2460 –2472.https://doi.org/10.1128/
JCM.00581-15.
15. Sullivan KV, Deburger B, Roundtree SS, Ventrola CA, Blecker-Shelly DL, Mortensen JE. 2014. Pediatric multicenter evaluation of the Verigene gram-negative blood culture test for rapid detection of inpatient bac-teremia involving gram-negative organisms, extended-spectrum beta-lactamases, and carbapenemases. J Clin Microbiol 52:2416 –2421. https://doi.org/10.1128/JCM.00737-14.
16. Dodemont M, De Mendonca R, Nonhoff C, Roisin S, Denis O. 2014. Performance of the Verigene Gram-negative blood culture assay for rapid detection of bacteria and resistance determinants. J Clin Microbiol
52:3085–3087.https://doi.org/10.1128/JCM.01099-14.
17. Mancini N, Infurnari L, Ghidoli N, Valzano G, Clementi N, Burioni R, Clementi M. 2014. Potential impact of a microarray-based nucleic acid assay for rapid detection of Gram-negative bacteria and resistance markers in positive blood cultures. J Clin Microbiol 52:1242–1245. https://doi.org/10.1128/JCM.00142-14.
18. Tojo M, Fujita T, Ainoda Y, Nagamatsu M, Hayakawa K, Mezaki K, Sakurai A, Masui Y, Yazaki H, Takahashi H, Miyoshi-Akiyama T, Totsuka K, Kirikae T, Ohmagari N. 2014. Evaluation of an automated rapid diagnostic assay for detection of Gram-negative bacteria and their drug-resistance genes
in positive blood cultures. PLoS One 9:e94064.https://doi.org/10.1371/
journal.pone.0094064.
19. Hill JT, Tran KD, Barton KL, Labreche MJ, Sharp SE. 2014. Evaluation of the Nanosphere Verigene BC-GN assay for direct identification of gram-negative bacilli and antibiotic resistance markers from positive blood cultures and potential impact for more-rapid antibiotic interventions. J
Clin Microbiol 52:3805–3807.https://doi.org/10.1128/JCM.01537-14.
20. Rand KH, Delano JP. 2014. Direct identification of bacteria in positive blood cultures: comparison of two rapid methods, FilmArray and mass
spectrometry. Diagn Microbiol Infect Dis 79:293–297.https://doi.org/10
.1016/j.diagmicrobio.2014.03.014.
21. Blaschke AJ, Heyrend C, Byington CL, Fisher MA, Barker E, Garrone NF, Thatcher SA, Pavia AT, Barney T, Alger GD, Daly JA, Ririe KM, Ota I, Poritz MA. 2012. Rapid identification of pathogens from positive blood cultures by multiplex polymerase chain reaction using the FilmArray system.
Diagn Microbiol Infect Dis 74:349 –355. https://doi.org/10.1016/j
.diagmicrobio.2012.08.013.
22. Southern TR, VanSchooneveld TC, Bannister DL, Brown TL, Crismon AS, Buss SN, Iwen PC, Fey PD. 2015. Implementation and performance of the
BioFire FilmArray®blood culture identification panel with antimicrobial
treatment recommendations for bloodstream infections at a midwestern
academic tertiary hospital. Diagn Microbiol Infect Dis 81:96 –101.https://
doi.org/10.1016/j.diagmicrobio.2014.11.004.
23. MacVane SH, Nolte FS. 2016. Benefits of adding a rapid PCR-based blood culture identification panel to an established antimicrobial stewardship
program. J Clin Microbiol 54:2455–2463. https://doi.org/10.1128/JCM
.00996-16.
24. Banerjee R, Teng CB, Cunningham SA, Ihde SM, Steckelberg JM, Moriarty JP, Shah ND, Mandrekar JN, Patel R. 2015. Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification
and susceptibility testing. Clin Infect Dis 61:1071–1080.https://doi.org/
10.1093/cid/civ447.
on May 16, 2020 by guest
http://jcm.asm.org/
25. Ng LS, Kwang LL, Rao S, Tan TY. 2015. Anaerobic bacteraemia revisited: species and susceptibilities. Ann Acad Med Singapore 44:13–18. 26. Tan TY, Ng LS, Kwang LL, Rao S, Eng LC. 2016. Clinical characteristics and
antimicrobial susceptibilities of anaerobic bacteremia in an acute care
hospital. Anaerobe 43:69 –74. https://doi.org/10.1016/j.anaerobe.2016
.11.009.
27. Gunthard H, Pennekamp A. 1996. Clinical significance of extraintestinal
Hafnia alveiisolates from 61 patients and review of the literature. Clin
Infect Dis 22:1040 –1045.https://doi.org/10.1093/clinids/22.6.1040.
28. Diekema DJ, Pfaller MA, Jones RN, Doern GV, Kugler KC, Beach ML, Sader HS. 2000. Trends in antimicrobial susceptibility of bacterial pathogens isolated from patients with bloodstream infections in the USA, Canada, and Latin America. SENTRY Participants Group. Int J Antimicrob Agents
13:257–271.https://doi.org/10.1016/S0924-8579(99)00131-4.
29. Jacoby GA. 2009. AmpC-lactamases. Clin Microbiol Rev 22:161–182.
https://doi.org/10.1128/CMR.00036-08.
30. Leclercq R, Canton R, Brown DF, Giske CG, Heisig P, MacGowan AP, Mouton JW, Nordmann P, Rodloff AC, Rossolini GM, Soussy CJ, Steinbakk M, Winstanley TG, Kahlmeter G. 2013. EUCAST expert rules in
antimicro-bial susceptibility testing. Clin Microbiol Infect 19:141–160.https://doi
.org/10.1111/j.1469-0691.2011.03703.x.
31. Abbott SL, Moler S, Green N, Tran RK, Wainwright K, Janda JM. 2011. Clinical and laboratory diagnostic characteristics and cytotoxigenic
po-tential ofHafnia alveiandHafnia paralveistrains. J Clin Microbiol 49:
3122–3126.https://doi.org/10.1128/JCM.00866-11.
32. Willmann M, Kuebart I, Marschal M, Schroppel K, Vogel W, Flesch I,
Markert U, Autenrieth IB, Holzl F, Peter S. 2013. Effect of metallo-
-lactamase production and multidrug resistance on clinical outcomes in
patients withPseudomonas aeruginosabloodstream infection: a
retro-spective cohort study. BMC Infect Dis 13:515.https://doi.org/10.1186/
1471-2334-13-515.
33. Kanj SS, Kanafani ZA. 2011. Current concepts in antimicrobial therapy against resistant gram-negative organisms: extended-spectrum
beta-lactamase-producingEnterobacteriaceae, carbapenem-resistant
Entero-bacteriaceae, and multidrug-resistant Pseudomonas aeruginosa. Mayo
Clin Proc 86:250 –259.https://doi.org/10.4065/mcp.2010.0674.
34. Dauwalder O, Vandenesch F. 2014. Clinical microbiology laboratory: from the Pasteur model to the 24/7 clinical chemistry concept. Clin
Microbiol Infect 20:O593–O594. https://doi.org/10.1111/1469-0691
.12692.
35. Bourbeau PP, Ledeboer NA. 2013. Automation in clinical microbiology. J
Clin Microbiol 51:1658 –1665.https://doi.org/10.1128/JCM.00301-13.
36. Ledeboer NA, Dallas SD. 2014. The automated clinical microbiology
laboratory: fact or fantasy? J Clin Microbiol 52:3140 –3146.https://doi
.org/10.1128/JCM.00686-14.
37. Bouza E, Sousa D, Munoz P, Rodriguez-Creixems M, Fron C, Lechuz JG. 2004. Bloodstream infections: a trial of the impact of different methods of reporting positive blood culture results. Clin Infect Dis 39:1161–1169. https://doi.org/10.1086/424520.
38. Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, Gurka D, Kumar A, Cheang M. 2006. Duration of hypotension before initiation of effective antimicrobial ther-apy is the critical determinant of survival in human septic shock. Crit
Care Med 34:1589 –1596. https://doi.org/10.1097/01.CCM.0000217961
.75225.E9.
39. Battle SE, Bookstaver PB, Justo JA, Kohn J, Albrecht H, Al-Hasan MN. 2017. Association between inappropriate empirical antimicrobial ther-apy and hospital length of stay in Gram-negative bloodstream infections: stratification by prognosis. J Antimicrob Chemother 72:
299 –304.https://doi.org/10.1093/jac/dkw402.
40. Sango A, McCarter YS, Johnson D, Ferreira J, Guzman N, Jankowski CA. 2013. Stewardship approach for optimizing antimicrobial therapy through use of a rapid microarray assay on blood cultures positive for
Enterococcus species. J Clin Microbiol 51:4008 – 4011.https://doi.org/10
.1128/JCM.01951-13.
41. Perez KK, Olsen RJ, Musick WL, Cernoch PL, Davis JR, Peterson LE, Musser JM. 2014. Integrating rapid diagnostics and antimicrobial stewardship im-proves outcomes in patients with antibiotic-resistant Gram-negative
bacte-remia. J Infect 69:216 –225.https://doi.org/10.1016/j.jinf.2014.05.005.