Positive
Family
Functioning
29 September 2010
Final
Report
by
Access
Economics
Pty
Limited
for
Department of Families, Housing, Community
Services and Indigenous Affairs
© Access Economics Pty Limited
This work is copyright. The Copyright Act 1968 permits fair dealing for study, research, news reporting, criticism or review. Selected passages, tables or diagrams may be reproduced for such purposes provided acknowledgment of the source is included. Permission for any more extensive reproduction must be obtained from Access Economics Pty Limited through the contact officer listed for this report.
Disclaimer
While every effort has been made to ensure the accuracy of this document and any attachments, the uncertain nature of economic data, forecasting and analysis means that Access Economics Pty Limited is unable to make any warranties in relation to the information contained herein. Access Economics Pty Limited, its employees and agents disclaim liability for any loss or damage which may arise as a consequence of any person relying on the information contained in this document and any attachments.
Access Economics Pty Limited ABN 82 113 621 361 www.AccessEconomics.com.au
CANBERRA MELBOURNE SYDNEY
Level 1 9 Sydney Avenue Barton ACT 2600 Level 27 150 Lonsdale Street Melbourne VIC 3000 Suite 1401, Level 14 68 Pitt Street Sydney NSW 2000 T: +61 2 6175 2000 F: +61 2 6175 2001 T: +61 3 9659 8300 F: +61 3 9659 8301 T: +61 2 9376 2500 F: +61 2 9376 2501 For information on this report please contact Lynne Pezzullo T: 61‐2‐6175 2000 E: [email protected] Report prepared by Lynne Pezzullo Penny Taylor Scott Mitchell Laze Pejoski Khoa Le Anam Bilgrami
Contents
Acknowledgements...i
Glossary ii Executive Summary ...i
1 Introduction ... 5
2 Methodological overview ... 6
2.1 Definition of family functioning and the outcomes of interest ... 6
2.2 Data review... 7
2.3 Literature review... 10
2.4 Concepts and data underlying lifetime costing ... 10
2.5 Model construction... 11
2.6 Cost benefit/cost effectiveness analysis (CBA/CEA) and the process for selecting interventions for analysis... 18
3 Findings from the LSAC data investigation ... 21
3.1 LSAC variables ... 21
3.2 LSAC analysis... 24
4 Findings from the ATP data investigation... 31
4.1 ATP variables... 31
4.2 ATP analysis ... 34
5 The costing model... 38
5.1 Health outcomes... 38
5.2 Productivity outcomes ... 44
5.3 Criminality outcomes ... 45
5.4 Lifetime costing framework ... 49
6 Cost benefit analysis ... 52
6.1 Communities for children (CfC)... 52
6.2 Positive Parenting Program (PPP) ... 56
6.3 Reconnect ... 62
6.4 Shocking all variables – the value of PFF ... 69
7 Conclusions ... 71
References... 77
Appendix A : LSAC children and future addictive behaviours ... 85
Appendix B : Literature review sources, ATP ... 88
Appendix C : LSAC regression outcomes ... 91
Appendix D : LSAC variable specification ... 104
Appendix E : Mean and standard deviation of LSAC variables... 108
Appendix F : ATP variable interpretation... 111
Appendix H : Mean and standard deviation of ATP variables... 128
Appendix I : Detailed costing methodology and tables ... 133
Charts
Chart 3.1 : Explanatory power of regressions, by age... 26
Chart A.1 : Differences in cognitive development by socio‐economic status... 86
Tables
Table 2.1 : Characteristics of family functioning domains ... 6
Table 2.2 : FF variables used for each intervention ... 16
Table 3.1 : Regression constructs in LSAC ... 23
Table 4.1 : Regression constructs... 32
Table 5.1 : Summary of total costs of obesity (2010)... 39
Table 5.2 : Summary of total costs of anxiety and depression (2010) ... 41
Table 5.3 : Summary of total costs of daily smoking (2010) ... 42
Table 5.4 : Summary of total costs of alcohol abuse (2010) ... 43
Table 5.5 : Summary of total costs of illicit drug use (2010)... 44
Table 5.6 : Estimated effects* (%) of year 12 and undergraduate completion* on probability of participation and average earnings ... 45
Table 5.7 : Social costs of crime by cost type (2010) ... 46
Table 5.8 : Net recurrent expenditure on criminal courts (2008‐09) and % criminal court finalisations by court type ... 47
Table 5.9 : Total real net operating expenditure on prisons and community corrections in Australia in 2008‐09... 48
Table 5.10 : Discounted lifetime costs of adverse health outcomes (a) (2010 dollars)... 49
Table 5.11 : Discounted lifetime costs of adverse productivity outcomes (a) (2010 dollars).... 50
Table 5.12 : Discounted lifetime costs of criminality outcomes (a) (2010 dollars)... 51
Table 6.1 : Communities for Children target areas and related LSAC variables ... 54
Table 6.2 : Outcomes of Communities for Children variables used in this report... 55
Table 6.3 : Outcomes of CfC as delivered over 2004‐05 to 2007‐08 ... 56
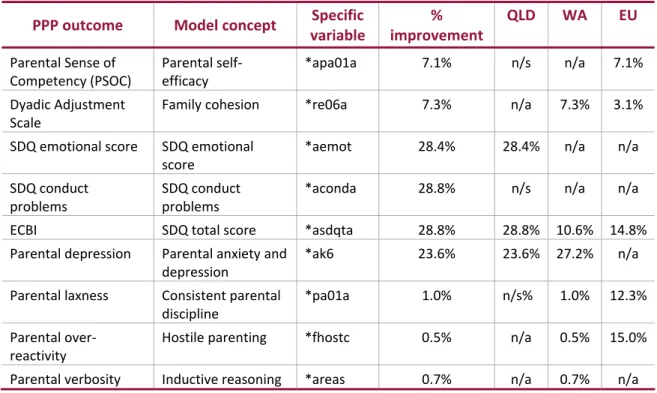
Table 6.4 : PPP target areas and LSAC variables ... 58
Table 6.5 : Impact of large scale Queensland PPP trial ... 58
Table 6.6 : Impact of large scale Western Australian PPP trial ... 59
Table 6.7 : Improvement in means scores of European PPP trial ... 60
Table 6.9 : PPP costs ($US) ... 61
Table 6.10 : Outcomes of PPP as delivered over 2004‐05 to 2007‐08 in Queensland... 61
Table 6.11 : ATP variables associated with the Reconnect Program ... 66
Table 6.12 : Estimate of effect size — young person’s perception of their ability to manage family conflict before Reconnect and now... 67
Table 6.13 : Estimate of effect size — young person’s perception of their family’s ability to manage family conflict before Reconnect and now ... 68
Table 6.14 : Outcomes of the Reconnect Program, as delivered over 2004‐05 to 2008‐09... 69
Table 6.15 : The value of PFF... 69
Table 7.1 : Summary of costs and benefits of modelled interventions ... 72
Table B.1 : Antisocial behaviour ... 88
Table B.2 : Anxiety and depression ... 88
Table B.3 : Smoking ... 89
Table B.4 : Alcohol... 89
Table B.5 : Illicit drug use ... 89
Table B.6 : Productivity ... 90
Table B.7 : Overweight/obesity... 90
Table C.1 : Obesity B1 (ahs23c2) ... 91
Table C.2 : Obesity B2 (bcbmi) ... 92
Table C.3 : Obesity B3 (ccbmi)... 92
Table C.4 : Obesity K2 (dcbmi) ... 93
Table C.5 : Obesity K3 (ecbmi)... 93
Table C.6 : Productivity B1 (awlrnoi) ... 94
Table C.7 : Productivity B2 (bwlrnoi)... 94
Table C.8 : Productivity B3 (cwlrnoi) ... 95
Table C.9 : Productivity K2 (dwlrnoi)... 95
Table C.10 : Productivity K3 (ewlrnoi) ... 96
Table C.11 : Anxiety and depression B1 (apedsgc)... 96
Table C.12 : Anxiety and depression B2 (bpedsef)... 97
Table C.13 : Anxiety and depression B3 (cpedsef) ... 97
Table C.14 : Anxiety and depression K2 (daemot) ... 98
Table C.15 : Anxiety and depression K3 (eaemot) ... 98
Table C.16 : Antisocial B1 (apedsgc)... 99
Table C.17 : Antisocial B2 (babitp) ... 99
Table C.19 : Antisocial K2 (daconda) ... 100
Table C.20 : Antisocial K3 (eaconda) ... 101
Table C.21 : Addictions B1 (apedsgc) ... 101
Table C.22 : Addictions B2 (babitp) ... 102
Table C.23 : Addictions B3 (casdqta) ... 102
Table C.24 : Addictions K2 (dasdqta)... 103
Table C.25 : Addictions K3 (easdqta)... 103
Table D.1 : Standard LSAC variables... 104
Table D.2 : Combinations of LSAC variables... 106
Illustrative distribution of categorical variables... 109
Table G.1 : Underengagement predictor variables... 118
Table G.2 : Completion of high school(a)(b) ... 118
Table G.3 : Completion of high school (only) v University degree(a)(b) ... 119
Table G.4 : Body mass index at 23‐24 years(a)(b)... 120
Table G.5 : ATP anxiety/depression 2002 crosstabulation ... 122
Table G.6 : Logistic regression results — child age 19‐20 years (year 2002)(a)(b) ... 122
Table G.7 : Logistic regression results — child age 19‐20 years (year 2002)(a)(b) ... 124
Table I.1 : Obesity prevalence rates and estimated obese people (number) in 2010 ... 136
Table I.2 : Anxiety and depression prevalence rates and estimated people with anxiety and depression (number) in 2010 ... 136
Table I.3 : Smoking prevalence rates and estimated current daily smokers in 2010... 137
Table I.4 : Prevalence rates for tobacco‐caused diseases and conditions(a)... 138
Table I.5 : Prevalence rates ‐ drinking at risky‐high risk(a) levels of long term health harm and estimated risky‐high risk drinkers in 2010... 138
Table I.6 : Prevalence rates for recent use(a) of illicit drugs and estimated recent users in 2010139 Table I.7 : Offender age‐gender prevalence profile and estimated offenders in 2008‐09 ... 139
Table I.8 : Prisoner age‐gender prevalence rates and estimated prisoners in 2009 ... 140
Table I.9 : Annual per‐person costs of obesity ‐ males (in 2010 dollars) ... 140
Table I.10 : Annual per‐person costs of obesity ‐ females (in 2010 dollars) ... 141
Table I.11 : Annual per‐person costs of anxiety and depression ‐ males (in 2010 dollars)... 142
Table I.12 : Annual per‐person costs of anxiety and depression ‐ females (in 2010 dollars) .. 142
Table I.13 : Annual per‐person costs of current daily smoking ‐ males (in 2010 dollars) ... 143
Table I.14 : Annual per‐person costs of current daily smoking ‐ females (in 2010 dollars)... 143
Table I.15 : Annual per‐person costs of alcohol abuse ‐ males (in 2010 dollars)... 144
Table I.17 : Annual per‐person costs of illicit drug abuse ‐ males (in 2010 dollars)... 145
Table I.18 : Annual per‐person costs of illicit drug abuse ‐ females (in 2010 dollars) ... 145
Table I.19 : Age‐gender employment in the general population ... 146
Table I.20 : Age‐gender average weekly earnings(a) for the general population ($) ... 146
Table I.21 : Annual costs of year 12 non‐completion ($ 2010) ... 147
Table I.22 : Annual costs of undergraduate degree non‐completion ($ 2010)... 147
Table I.23 : Age‐specific undergraduate non‐completion rates in 2007... 148
Table I.24 : Annual policing cost per offender ($) ... 149
Table I.25 : Annual court system cost per offender ($)... 149
Table I.26 : Annual prison system cost per prisoner ($)... 149
Table I.27 : Annual per‐person societal costs of crime for males ($)... 150
Table I.28 : Annual per‐person societal costs of crime for females ($)... 150
Table I.29 : Crime under‐reporting multipliers and derived probabilities ... 151
Table I.30 : Probabilities of court action on reported crimes ... 152
Table I.31 : Court finalisation outcome probabilities... 153
Table I.32 : Custodial sentence probabilities in guilty verdict court cases ... 153
Figures
Figure 2.1 : Approximate age of study cohorts and bridging the current information gap... 8
Figure 2.2 : Diagram of data map... 9
Figure 2.3 : Conceptual map for valuing costs of NFF... 10
Figure 2.4 : Incidence versus prevalence approach ... 10
Figure 2.5 : Cost effectiveness analysis model map... 17
Figure 2.6 : CEA model pathway for interventions ... 18
Acknowledgements
Access Economics would like to acknowledge with gratitude the expert knowledge and inputs
provided by members of the Expert Reference Group for this project.
Professor Ann Sanson
Department of Paediatrics, University of Melbourne, ARC/NHMRC Research Network
Coordinator, Australian Research Alliance for Children and Youth
Brian Babington
Chief Executive Officer, Families Australia
Carol Ey
Branch Manager, Research and Analysis Branch, Department of Families, Housing, Community
Services and Indigenous Affairs
Dr Lance Emerson
Chief Executive Officer, Australian Research Alliance for Children and Youth (ARACY)
Dr Marian Esler
Section Manager, Research Section, Family and Child Support Policy Branch, Department of
Families, Housing, Community Services and Indigenous Affairs
Dr Matthew Gray
Deputy Director, Australian Institute of Family Studies
Megan Shipley
Research Section, Family and Child Support Policy Branch, Department of Families, Housing,
Community Services and Indigenous Affairs
Paula Mance
Research Projects and Publications Section, Department of Families, Housing, Community
Services and Indigenous Affairs
Rachel Henry
Research Section, Family and Child Support Policy Branch, Department of Families, Housing,
Community Services and Indigenous Affairs
Professor Stephen Zubrick
Co‐Director for Developmental Health, Curtin University of Technology
Access Economics would like to acknowledge in particular the staff of the Australian Institute
of Family Studies (AIFS), who analysed the Australian Temperament Project (ATP) data and
modelled those regressions. Apart from Dr Gray, particular thanks go to Dr Ben Edwards and
Glossary
ABS Australian Bureau of Statistics
AE‐DEM Access Economics Demographic Model
AEM Access Economics Macroeconomics Model
AIFS Australian Institute of Family Studies
AIHW Australian Institute of Health and Welfare
AWE average weekly earnings
ATP Australian Temperament Project
B1, B2, B3 Baby cohort, waves 1, 2 and 3 in LSAC
BOD burden of disease
CALD Culturally and Linguistically Diverse
CBA cost benefit analysis
CEA cost effectiveness analysis
CFC Communities for Children
DALY disability adjusted life year
DCBA disease cost‐burden analysis
DEEWR Department of Education, Employment and Workplace Relations
DOFD Department of Finance and Deregulation
DSM Diagnostic and Statistical Manual
DSP Disability Support Pension
DWL deadweight loss
FAHCSIA Australian Government Department of Families, Housing, Community
Services and Indigenous Affairs
FF family functioning
FRS family relationship services
GP general practitioner
HILDA Household Income and Labour Dynamics in Australia
International Classification of Diseases (10th revision)
ICD‐10
K1, K2, K3 Kindy cohort, waves 1, 2 and 3 in LSAC
LSAC Longitudinal Study of Australian Children
LSAY Longitudinal Study of Australian Youth
NHS National Health Survey
NDHS National Drug Strategy Household Survey
NSA Newstart Allowance
NFF negative family functioning
MBS Medicare Benefits Schedule
OLS Ordinary Least Squares
PBS Pharmaceutical Benefits Scheme
PC Productivity Commission
PFF positive family functioning
PPP Postive Parenting Program
PS Parenting Scale
PSOC Parental Sense of Competency
PUP Parents under Pressure
QOL quality of life
REACH Responding Early Assisting Children
SCRGSP Steering Committee for the Review of Government Service Provision
SDAC Survey of Disability, Ageing and Carers (ABS)
SDQ Strengths and Difficulties Questionnaire
SES socioeconomic status
SFCS Stronger Families and Communities Strategy
TILA Transition to Independent Living Allowance
VSLY value of a statistical life year
WHO World Health Organization
W1,2,3 waves 1,2,3 of LSAC
YLD year(s) of healthy life lost due to disability
Executive
Summary
Access Economics was commissioned by the Australian Government Department of Families,
Housing, Community Services and Indigenous Affairs (FaHCSIA) to quantify, in economic terms,
the value of ‘goods and services’ provided by positive family functioning (PFF) and to conduct a
cost benefit analysis (CBA) to establish the returns to government and society for investments
made in supporting family functioning (FF). This report follows a scoping study, also conducted
by Access Economics, to establish the methodology for the project. The scoping study explains
the equivalence of measuring the value of PFF as the costs of negative family functioning
(NFF). This study was overseen by a panel of experts.
Methods
FF is defined through a variety of domains – emotional, governance, cognitive, physical, intra‐
familial and social (Table 2.1). Literature review revealed three broad areas of outcomes
associated with FF.
■
Health outcomes were observed through the occurrence of anxiety and depression,obesity and substance abuse (smoking, alcohol and drug abuse) later in life. These are
associated with health expenditures, productivity losses (through lower workforce
participation and premature death), other financial costs, and loss of quality of life (QoL)
(measured in disability adjusted life years or DALYs).
■
Productivity outcomes were reflected in secondary and tertiary educationalachievement completion, flowing on to impact lifetime earnings.
■
Social outcomes were primarily measured through negative manifestations – antisocialbehaviour such as delinquency and crime, resulting in criminal justice system costs.
Two longitudinal studies — the Longitudinal study of Australian Children (LSAC) aged up to 9
years and the Australian Temperament Project (ATP) for older children were selected to
analyse the relationship between FF and child outcomes. Regression analysis was conducted
to establish relationships between ‘transition’ health, productivity and social outcome
variables in LSAC and FF variables. The latter were selected on the basis of literature evidence,
after controlling for other factors such as socioeconomic status (SES). Transition variables
were carefully selected to match similar or identical ATP variables. Further regression analysis
was undertaken using the transition variables, together with ATP FF and control independent
variables, to establish relationships with ATP ‘interim’ health, productivity and social outcomes
in early adulthood. The interim outcomes were then used to predict lifetime health,
productivity and social costs, based on an extensive costing process utilising multiple data
sources (Chapter 5).
Findings
The net present value (NPV) of benefits from intervening in childhood and adolescence to
prevent poor outcomes later in life are substantial, despite the fact that such intervention
incurs costs today but discounted benefits are realised a long time into the future.
In total, the potential NPV of benefits to be realised is in the order of $5.4 billion per
annum in 2010 dollars. This can be considered the cost of NFF currently, or the value of
PFF gains possible. Over half these gains (53% or $2.9 billion) are productivity gains,
with a further 22% ($1.2 billion) of the benefits deriving from savings from fewer
addictions. Fewer cases of anxiety and depression would save $0.6 billion (11%), while
lower rates of criminality and antisocial behaviour would accrue $0.5 billion (10%). A
reduction in obesity would save $0.3 billion per annum (5% of the total) ‐ Figure i. Figure i: Value of PFF by benefit type, 2010 (total $5.4 billion), $bn and % total 261 , 5% 2,882 , 53% 581 , 11% 547 , 10% 1,176 , 22%
Obesity Productivity Anxiety and depression Anti‐social Addictions
Source: Access Economics calculations. Note: Shares may not sum to 100% due to rounding.
is has focused on three interventions selected on ba
■
efit:cost ratio
tio
benefit:cost ratio for this return on investment.
Costs and benefits are summarised in Table ii.
There are also marked social and economic benefits if cost effective prevention programs can
be identified and implemented. This analys the ses of a range of criteria (section 2.6)
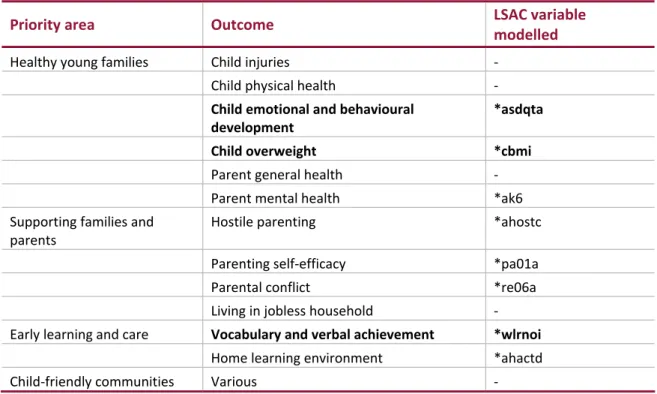
The Communities for Children program, targeting pre‐school and primary school aged
children, is one of the major Australian Government investments in families. The
program improves outcomes in various FF areas including hostile parenting, parenting
self‐efficacy, parent mental health, quality of the home learning environment, parental
relationship conflict, child total emotional and behavioural problems, childhood
overweight, receptive vocabulary achievement and verbal ability. The ben for this program was estimated as 4.8:1, a 377% return on investment.
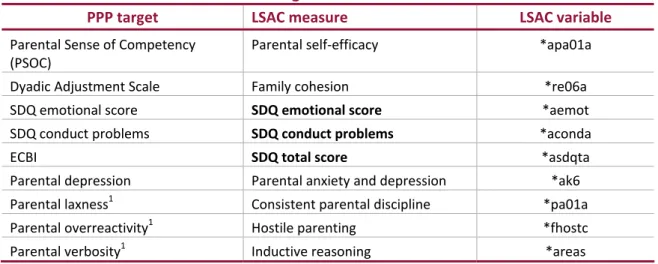
■
The Positive Parenting Program is one of the best evaluated FF programs for youngerchildren. The program improves FF outcomes in parental sense of competency, the
dyadic adjustment scale, the Strengths and Difficulties Questionnaire (SDQ) emotional
and conduct scales, the Eyberg Child Behaviour Intensity score, parental depression,
parental laxness, parental over‐reactivity, and parental verbosity. The benefit:cost ra for this program was estimated as 13.8:1, a substantial 1,283% return on investment.
■
The Reconnect program targets an older cohort of children and was found to improveoutcomes in school bonding and conflictual relationships, with proxied effect sizes
estimated for attachment to parents and harsh parenting. The
Table ii: Summary of costs and benefits of modelled interventions
CfC PPP Reconnect
Program cost ($m)* 113.6 19.7 112.1
Unit cost ($) 840/child aged 0‐5 34/child aged 2‐12 3,800/person aged 12‐21
Benefit ($m, lifetime NPV) 541.4 272.4 202.8
Benefit:cost ratio 4.76 13.82 1.81
Source: Access Economics calculations. * Costs estimated over 2004‐05 to 2007‐08 except for Reconnect which extends to 2008‐09.
Many of the family ‘inputs’ incorporated in the analysis were found to be statistically
significant explanators of child outcomes with the relationship consistent with that predicted
by the literature.
■
Obesity was explained by key drivers such as previous obesity, parental obesity, lack ofchild persistence, and parent‐child conflict.
■
Anxiety and depression were dependent on previous emotional problems, difficulttemperament, lower socioeconomic status (SES), harsh discipline, parental
anxiety/depression, alienation from parents and lack of child persistence.
■
Smoking in young adulthood (19‐20 years) was determined by previous smoking inadolescence, parental permission to smoke at home and a conflictual parent‐teenager
relationship. Alcohol abuse (binge drinking) in young adulthood was dependent on teen
bingeing, lack of parental monitoring, father drinking and initiating drinking at an older
age (over 15 compared to 14 or younger). Illicit drug use in 23‐24 year olds was
dependent on the child’s temperament, lack of parental monitoring, and mother
smoking.
■
Predisposition to smoking, alcohol abuse and illicit drug use was established in earlyyears by parental smoking, temperament, harsh and/or inconsistent discipline, poor
nce,
king and low
SES, along with parental anxiety/depression and the child’s temperament.
te these
findings internationally as well as continue to enhance the evidence base in Australia. Access Economics
family cohesion and parental anxiety depression.
■
Productivity was driven by previous learning outcomes, consistent discipline,temperament, socioeconomic status, parent education and, in adolescence, persiste relationship quality/warmth, parental monitoring and a positive attitude to school.
■
Antisocial behaviour and outcomes were determined by child lack of persistence,previous social/conduct problems and, importantly, were largely influenced by early life
FF variables such as poor family cohesion, harsh discipline, parental smo
The greatest value in this project has been primarily to showcase how a broad, quantitative
approach to social policy evaluation can work. With better quality data in the future, there is
scope to refine and continue to develop the modelling and elaborate on findings further. The
scope of this project has been both ambitious and challenging but, we believe, the methods
developed and many findings and insights are of global significance. The novelty of the
1
Introduction
Access Economics was commissioned by the Australian Government Department of Families,
Housing, Community Services and Indigenous Affairs (FaHCSIA) to quantify, in economic terms,
the value of ‘goods and services’ provided by positive family functioning (PFF) and to conduct a
cost benefit analysis (CBA) and/or cost effectiveness analysis (CEA) to establish the returns to
government and society for investments made in supporting family functioning.
This report follows a scoping study, also conducted by Access Economics. The scoping study in
2009 determined:
■
the feasibility of quantifying, in economic terms, the value of ‘goods and services’provided by PFF;
■
a method for measuring the benefits of PFF; and■
a method to conduct CBA and CEA of interventions to improve FF.The methods developed in the scoping study form the basis for the analysis in this report. The
scoping study explains the equivalence of measuring the value of PFF as the costs of negative
family functioning (NFF).
Both the scoping study and this full study were overseen by a panel of experts, as listed in the
acknowledgements section of each report. In addition, this study was undertaken with
assistance from the Australian Institute of Family Studies (AIFS), which analysed the Australian
Temperament Project (ATP) data.
The structure of this report is as follows.
■
The methodology is explained in chapter 2.■
The findings from the investigation of the Longitudinal Survey of Australian Childrenf the ATP are detailed in chapter 4.
nd the CEA results are explained.
etailed information is provided in the Appendices in relation to the methods, LSAC and
ATP investigations, and the costing model.
(LSAC) are outlined in chapter 3.
■
The findings from the investigation o■
The costing model is described in 5.■
In chapter 6, the interventions analysed a■
Conclusions are elaborated in chapter 7.2
Methodological
overview
2.1
Definition
of
family
functioning
and
the
outcomes
of
interest
The focus of the scoping study was on the outcomes of family functioning for the child,
without pursuing any family ‘ideal’ or promoting any specific type of family structure. Children
are not able to explicitly control their family environment and they are often viewed as the
main victims of NFF.
The scoping study identified that while no simple definition of PFF exists, consistent themes (or
‘domains’) of FF emerged from the literature. These were developed and agreed, in
consultation with the Expert Reference Group for the scoping study and with FaHCSIA. These
domains provide an overarching definition of the FF environment. A summary is provided
below.
Family functioning (FF) – positive and negative – is defined through a variety of emotional attributes, family governance frameworks, cognitive engagement and development characteristics, physical health habits, intra‐familial relationships and social connectedness. PFF is characterised by emotional closeness, warmth, support and security; well‐communicated and consistently applied age‐ appropriate expectations; stimulating and educational interactions; the cultivation and modelling of physical health promotion strategies; high quality relationships between all family members; and involvement of family members in community activities.
The domains of FF are not mutually exclusive, but interact, complement each other and co‐
exist.
Table 2.1: Characteristics of family functioning domains Domain Characteristics / Proxies
Emotional Closeness of parent‐child relationships, warmth, responsiveness,
sensitivity, perceived parental and family support as well as healthy
open communication, and security/safety.
Governance Establishment of age‐appropriate rules, expectations and consistency
Engagement and cognitive
development
Reading and verbal engagement, quality time fostering the development of educational, language and interaction skills. Physical health
Healthy/unhealthy physical activities or environments as well as access – including in‐utero – to specific products (e.g. fruit and vegetables, cigarettes and alcohol).
Intra‐familial relationships (dyadic family relationships)
Quality of relationships between all members of the family. For example sibling rivalries, parent‐child relationships as well as the health of the parents’ relationship.
Social connectivity Involvement of parents and children in activities outside of the family
unit (e.g. school, community service, volunteer work). Also includes relationships with extended family and work/life balance.
The literature review for the scoping study revealed three broad areas of outcomes associated
with FF.
■
Health outcomes were mostly observed through the occurrence of mental illnesses suchas anxiety and depression later in life, but also included eating disorders, health
behaviours (e.g. unsafe sex, physical inactivity, overweight and obesity) and substance
abuse (e.g. smoking, alcohol and drug abuse), with the consequent physical impacts of
these risk factors on morbidity and mortality outcomes.
■
Productivity outcomes were reflected in rates of labour force participation,employment and hourly wage rates, with a number of intermediate measures reported
in the literature, such as reduced levels of literacy and numeracy and other measures of
educational achievement.
■
Social outcomes were measured primarily through their negative manifestations – involvement in antisocial behaviour such as delinquency, and the probability of criminalbehaviour during youth and later in life. In contrast it was harder to quantitatively
associate PFF with positive manifestations such as the quality of inter‐personal
relationships and future community contributions.
The criteria used to select the specific outcomes for analysis in this report were:
■
each outcome domain was covered (health, productivity and social);■
outcomes were associated with high economic and social costs, including burden ofwere able to be measured by the data sets used as the basis for analysis
(see below).
this
ree);
sion, obesity, smoking, drinking, illicit drug use); and
ile
aic of
thy study timeframes. For example, intermediate outcomes
y and literacy cannot easily be converted into specific types of jobs and streams.
investigated but the LSAY did not
disease (BoD), based on prevalence and/or existing studies of costs and BoD;
■
the outcomesIn report, the correlation between FF is thus examined for the following outcomes:
■
productivity (school completion and completion of an undergraduate university deg■
health (anxiety and/or depres■
social (antisocial behaviour).Wh the literature provided valuable insights into potential linkages between FF and child
outcomes, the following cautions apply.
■
Many of the concepts are difficult to capture and measure and there is a mos different and overlapping instruments and metrics.■
Statistical techniques can be used to determine correlation rather than causation.■
While measures of intermediate outcomes are available, it is difficult to convert these tofinal outcomes without leng such as numerac
lifetime earnings
2.2
Data
review
Two longitudinal studies — the Longitudinal study of Australian Children (LSAC) and the
Australian Temperament Project (ATP) were selected to analyse the correlation between FF
and child outcomes. The Longitudinal Survey of Australian Youth (LSAY) and the Household,
col t information on FF variables and HILDA is limited to relationships between the family
nment and parent’s participation in the labour force.
LSAC has the advantage of containing a breadth of data, valuable for testing
confo lec enviro
■
unding factors. However, a disadvantage is the relatively short timeframe of data
years. However, measures
gers
du ,
however, eptual consistencies in measurement of FF between the two data sets.
collection as the eldest participants from the child cohorts are currently 10‐11 years of
age.
■
ATP is currently the only study in Australia that allows the determination of long termimpacts of FF on health, economic and social outcomes as the most recent data for
participants in this study were collected at the age of 23‐24
of FF and parenting have only been recorded since the participants were in their early
teens, with no measures during infancy or early childhood.
Variables from the ATP and LSAC within each of FF domains were mapped to the specific
outcomes selected for analysis so that the likelihood of one of the events of interest occurring
could be established across different age groups (Figure 2.1) and linked with outcomes. The
ability to join information from LSAC and ATP is limited by slightly different methods in each
data set of measuring FF and differences in the generations (ATP children were teena ring the 1990s, whereas LSAC children are growing up during the new century). There are
conc
Figure 2.1: Approximate age of study cohorts and bridging the current information gap
LSAC (1)
LSAC (2) Current Age Cohort Data Gap
ATP
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Approximate Age of Cohort in 2009
LSAC (1) is the Birth cohort and LSAC (2) is the Kindy cohort.
Ideally, one or two more waves of information from the LSAC is required to successfully bridge
the gap in ages between the two studies, to enable mapping outcomes for children aged
analys
■
observations in the oldest groupsi.e. the third wave of the Kindy cohort in LSAC. Early and mid‐period FF and control
P
ep analys
9 years to those aged 13 years. This approach is considered acceptable, given the alternative is
to wait some years for additional study waves to be completed.
Figure 2.2 shows how LSAC provides the dependent (end‐period ‘transition’) variables and
independent (early and mid‐period family functioning and control) variables in regression
is of children aged up to 9 years.
End‐period transition variables are those that relate to
variables relate to observations in all the other age groups (the first and second wave
observations and the third wave for the birth cohort).
AT data then provide the dependent (end‐period ‘interim outcome’) variables and
ind endent (early and mid‐period family functioning and control) variables in regression
■
ion completed, illicit drug use and body mass index were assessed at age
23‐24 years, while other variables (completing year 12, smoking, binge drinking,
n be modelled by ‘shocking’ the LSAC variables, while
adolescent interventions1 can by ‘shocking’ the ATP variables. ‘Shocking’ the
model refers to changing inpu simulating the effects of
an intervention, and then observing the consequent change in model outputs (health,
End‐period interim outcome variables are those that relate to observations in the oldest
groups of ATP relevant to the cost data and the circumstance. For example, highest
level of educat
anxiety/depression, and anti‐social behaviour) were assessed at adulthood (18‐19
years). Early and mid‐period FF and control variables relate to younger age
observations.
The interim outcomes can then be used to predict, in an Excel model, lifetime health costs,
lifetime productivity losses, social costs of crime and disability adjusted life years (DALYs). The
impact of childhood programs ca
be modelled
t parameters from one level to another, productivity and social outcomes).
Figure 2.2: Diagram of data map
LSAC ‐ early and mid‐period
CfC, PPP shock FF variables
control variables (confounding) Regression analysis
LSAC ‐ end‐period ATP ‐ early and mid‐period
Transition variables FF variables shock Reconnect
control variables (confounding) Regression analysis ATP ‐ end‐period
Interim outcomes Excel model Lieftime health costs Productivity (lifetime earnings) Social (lifetime costs of crime) DALYs
In laymen’s terms, LSAC was used to establish the impact of FF on children up to the age of
9 years, at which age transitional outcomes from childhood were spliced into the ATP analysis
by matching this set of transitional outcomes across the two datasets. Health, productivity
ng adequate data to establish
hip between family functioning and outcomes, collaborative relationships were
chers and FaHCSIA data specialists. Both were important
participants in the project. Furthermore, AIFS currently manages the ATP data set and access
and social interim outcomes in early adulthood thus depended on FF during adolescence as
well as the transitional outcomes from childhood. From the interim outcomes in early
adulthood, lifetime cost impacts were predicted using a variety of other datasets.
Given the identification of the ATP and LSAC databases as providi the relations
established with AIFS resear
arrangements require that AIFS undertake any in depth analysis.
1
The Communities for Children (CfC) and Positive Parenting Program (PPP) were selected for younger children, while the Reconnect program was selected for adolescents (see Section 2.6).
2.3
Literature
review
Evidence from the literature was used to edify the selection of family functioning inputs from
es. The findings are briefly
outlined in chapter 3, and chapter 4, and evidence is summarised in Appendix A and Appendix
2.4
Concepts
a
the ATP and LSAC that would be likely to be correlated with outcom B.
nd
data
underlying
lifetime
costing
Costs were attached to each outcome as depicted in Figure 2.3.
Figure 2.3: Conceptual map for valuing costs of NFF
Emotional Health Health system expenditures Governance Productivity losses
Cognitive Productivity Criminality costs Physical Social/criminality DWLs
Intra‐familial Other financial impacts Social Burden of disease
Source: Access Economics. Blue – health impacts. Red – productivity impacts. Green – Social/criminality impacts.
An incidence or ‘life aetiology of lagged
outcomes – i.e. ‘lifetime’ costs (hazard model). An incidence approach is distinguished from a
time’ costing approach was adopted in line with the prevalence approach in Figure 2.4.
Figure 2.4: Incidence versus prevalence approach
2000
2009
2018
A*
A
B*
B
B**
C
C*
Incidence
costs
(2009)
=
C
+
present
value
of
C*
Prevalence
costs
(2009)
=
A
+
B
+
C
The lif diseas
■
Cost Data Collection
(Department of Health and Ageing), the Pharmaceutical Benefits Scheme (PBS), the Note: The years are illustrative and do not relate to this analysis.
etime costs associated with each outcome include the standard cost categories for
e cost burden analysis from the health economics literature:
Direct health costs – estimated with cost data sourced primarily from the Australian
Medicare Benefits Schedule (MBS) and epidemiological data sourced from the Australian
Bureau of Statistics (ABS) National Health Survey (NHS), AIHW and other specific
epidemiological studies reported in the peer reviewed literature.
re
(unpaid care provided by family and friends), health aids and appliances, deadweight
sources of these estimates are previous studies by Access Economics, and the ABS
and Carers (SDAC) (ABS, 2004), and Lattimore et al (1997).
is s
the co lected for analysis. The net
se
■
nt a direct input into the cost benefit analysis.
analyses) change as a result of the intervention
pact of a 'shock' to consistent
■
Costs of crime – estimated with data primarily from the Steering Committee for theReview of Government Service Provision (SCRGSP) Report on Government Services, and
reports from the Australian Institute of Criminology and ABS. .
■
Productivity costs – are estimated using the human capital approach and reflectreduced labour force participation and absenteeism due to the outcomes selected.
Parameters and labour force data were drawn primarily from the ABS and reports by the
Productivity Commission (PC), as well as peer reviewed literature.
■
Burden of disease (BoD) – was estimated using DALYs and determined using the samedisability weights and methodology used by the AIHW (Begg et al, 2007). Monetary
values were estimated for the BoD using the value of a statistical life year from DOFD
(2009).
■
Other financial costs – include costs associated with the provision of informal ca losses (DWLs) (efficiency losses which arise due to transfer payments). The main Survey of Disability, AgeingFurther detail on costing methods, cost categories and data sources is provided in Appendix I.
2.5
Model
construction
Th ection provides an outline of the model developed to investigate the benefits of PFF and
sts and benefits of the three family functioning programs se
benefits for each program were derived under a scenario with the intervention compared to a
‘ba case’ without the intervention.
The costs for the CfC program, PPP and Reconnect programs are reported in chapter 6
and represe
■
The benefits are based on the extent to which each intervention improves FF andreduces its associated costs. The effectiveness of each intervention is reported in
chapter 6 while the associated costs (health, productivity and social) are detailed in
chapter 5.
The underlying principle of the model (developed in Microsoft Excel 2007) is that outcomes
(dependent variables in the regression
affecting early and mid‐period family functioning (independent) variables in the regression.
The size of the intervention is a direct function of the effectiveness of the program on
impacted functioning variables (chapter 6) and the size of the coefficients derived in the
regressions (Appendix C and Appendix G).
A simple example illustrates the model construction using the im
discipline on anxiety in children aged 4‐5 (so the analysis starts with the B3 cohort of this age –
incidentally the same age as the K1 cohort). The ‘shock’ in this example was derived from PPP
improvements in ‘parental laxness’ and mapped directly to parental consistent discipline as
The 'shock' can be viewed as changing the input parameters (e.g. parental consistent
discipline) from one level to another, simulated by the effects of an intervention. Before the
shock, the multivariate regressions for anxiety are given below for age group 4‐5 (B3), 6‐7 (K2)
and 8
anxiet child, and discipline is towards that child).
‐9 (K3), respectively. In each case, i represents the observational child in the dataset (so
y is that of the
Where:
B3 = Cohort of children aged 4‐5 in the ("Baby") group B2 = Cohort of children aged 2‐3 in the ("Baby") group
= Beta coefficient for 'Anxiety' in group B2
= Beta coefficient for 'Consistent discipline' in group B3 = Regression error term
Where:
K2 = Cohort of children aged 6‐7 in the ("Kindergarten") group B3 = Cohort of children aged 4‐5 in the ("Baby") group
= Beta coefficient for 'Anxiety' in group B3
= Beta coefficient for 'Consistent discipline' in group K2 = Regression error term
Where:
K3 = Cohort of children aged 8‐9 in the ("Kindergarten") group K2 = Cohort of children aged 6‐7 in the ("Kindergarten") group
= Beta coefficient for 'Anxiety' in group K2
= Beta coefficient for 'Consistent discipline' in group K3 = Regression error term
As a result of the intervention, the new level of childhood anxiety for children aged 4‐5
includes changes in parental consistent discipline. The change in parental consistent discipline
from the shock was calculated by multiplying the effectiveness of the program by the average
onsistent discipline value for children aged 4‐5.
c
Where:
= New 'Anxiety' value after intervention
= (mean consistent discipline x effectiveness of
program)
= Beta coefficient for 'Anxiety' in group B2
= Beta coefficient for 'Consistent discipline' in group B3 B3 = Cohort of children aged 4‐5 in the ("Baby") group
B2 = Cohort of children aged 2‐3 in the ("Baby") group = Regression error term
As a result of the shock, the consequent change in the model output (Anxiety') is given by a
ercentage change. p Where:
= Percentage change in 'Anxiety' = New 'Anxiety' value after intervention = Baseline 'Anxiety' value
B3 = Cohort of children aged 4‐5 in the ("Baby") group B2 = Cohort of children aged 2‐3 in the ("Baby") group
Consequently, the direct percentage change in anxiety levels for children in the 4‐5 age group
is captured through to the next LSAC age group (6‐7 year group) through the use of the lagged
ependent variable changing by the intervention effectiveness.
Where:
= Percentage change in 'Anxiety' = New 'Anxiety' value after intervention
= Baseline 'Anxiety' mean value B3 = Cohort of children aged 4‐5 in the ("Baby") group B2 = Cohort of children aged 2‐3 in the ("Baby") group
Where:
= New 'Anxiety' value after intervention in the previous age group = New 'Anxiety' lagged dependent variable = as above
= Beta coefficient for 'Anxiety' in group B2
= Beta coefficient for 'Consistent discipline' in group B3 K2 = Cohort of children aged 6‐7 in the ("Kindergarten") group B3 = Cohort of children aged 4‐5 in the ("Baby") group
= Regression error term
Following this pattern, Anxiety’’K2,i and Anxiety’K3,i are similarly calculated. The change in the
final period of LSAC compared with the actual outcome is then included in the ATP multinomial
logit regression i.e. the new anxiety levels for K3 children aged 9 (the final regression in the
Where:
= New 'Anxiety' value in children aged 8‐9 in the ("Kindergarten") group = Base 'Anxiety' value in children aged 8‐9 in the ("Kindergarten") group
This effectively assumes that no change occurs in outcomes between the ages of 10 to 12. As
mentioned before, this approach is considered acceptable, given the alternative is to wait
some years for additional study waves to be completed.
The multinomial logit regression models were used to analyse the impact of an intervention on
the probability of each family functioning outcome for children aged 13‐23 years. Unlike the
multivariate linear regressions, the results presented in the logit regression represent the
probability of an outcome for a person with ‘average’ attributes. Like the LSAC multivariate
linear regressions, the interventions were modelled as a deviation from the mean of a
particular explanatory variable (e.g. anxiety). The baseline logistic regression is given below,
where e is a mathematical constant, i is again each child observed (in ATP this time), βs are
again coefficients, and
ε
s are again error terms. X is the sample mean.
After the percentage change from anxiety in the 8‐9 year old age group, the new logistic
regression is given, with changes to the lagged dependent variable.
In using the multinomial logit model, coefficient estimates are not directly interpretable so do
not provide the same type of information as coefficients from an Ordinary Least Squares (OLS)
model. A more natural way of interpreting results from a multinomial logit model is to
determine the impact on the probability of an outcome by changing the variables that would
be impacted by the intervention while holding all others constant. The impact of the
intervention on the probability can therefore be represented by:
The impact of the intervention was therefore measured as the difference between the
probability of an outcome for an average person with and without the intervention. As such,
the model projects the probabilistic change in the outcome as a result of the intervention and
between the scenario and the ‘base case’ (no intervention) can therefore be evaluated to
determine the intervention’s overall return on investment using a dollar value.
Table 2.2 summarises all the FF variables in the model for each intervention modelled
(i.e. found to be significant in the regression analysis reported later on). A conceptual map of
the model is provided in Figure 2.5.
Table 2.2: FF variables used for each intervention
CfC PPP Reconnect
Hostile parenting Hostile parenting Harsh parenting
Parenting self‐efficacy Parental self‐efficacy
Consistent parental discipline
Attachment to parents
Parental warmth*
Parental relationship conflict Family cohesion Conflictual relationships
Parent mental health Parental anxiety and depression
Child total emotional and behavioural
problems (SDQ)
SDQ total score, SDQ emotional score, SDQ conduct problems
Quality of the home learning
environment
Home learning environment*
Receptive vocabulary achievement
and verbal ability
Inductive reasoning School bonding (positive affect
towards school); Under‐engagement
(not in education or training and not
employed)*
Child overweight
Source: Access Economics (2010). Note: See Chapters 3, 4 and 6 for derivation. * These variables are in the Reconnect model but the effect size was estimated as zero.
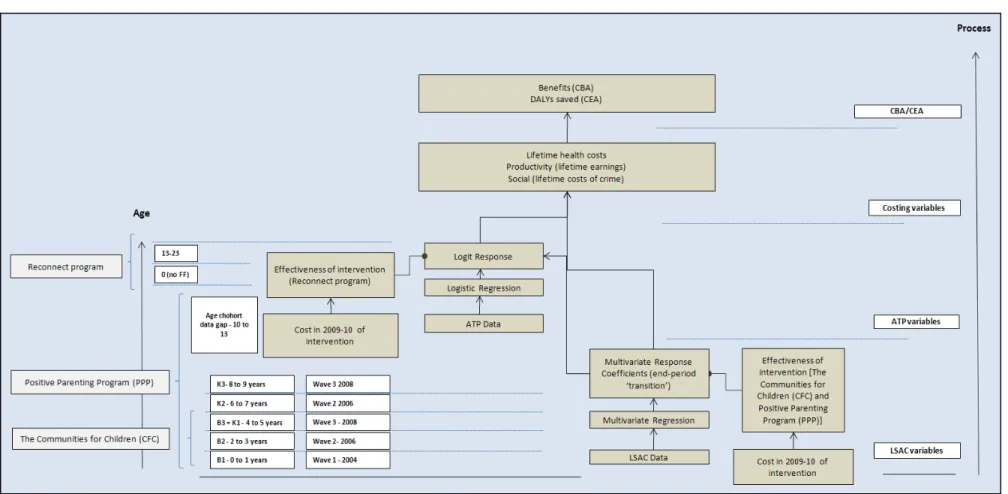
Figure 2.5: Cost effectiveness analysis model map
Source: Access Economics (2010)
2.6
Cost
benefit/cost
effectiveness
analysis
(CBA/CEA)
and
the
process
for
selecting
interventions
for
analysis
The concept of CEA modelling of FF interventions is outlined in Figure 2.6. All analyses
compare the outcomes for children with the interventions, against outcomes for children
without the intervention. The efficacy of a selected intervention in improving FF is derived
from previous evaluations of the programs. The Excel model is then used to explore how this
improvement in FF (the ‘shock’) reduces lifetime costs (in dollars and DALYs). These lifetime
benefits can then be compared with the intervention costs, in net present value (NPV) terms. Figure 2.6: CEA model pathway for interventions
Intervention
Improvement in family functioning in
Yr x (efficacy)
Reduces lifetime costs (NPV in Yr x, discounted
DALYs saved )
Cost in 09‐10$ Benefit in 09‐10$ CBA $:$ Benefit:Cost ratio
DALYs saved CEA $/DALY saved
As noted in Section 2.2, ‘shocking’ the model for CBA and CEA involves comparing what
happens in the absence of an intervention (the status quo), with what would happen if a
particular target population received an intervention. The intervention improves FF based on
evaluated effectiveness of the program, which in turn improves transition and/or interim
outcomes (based on the coefficients derived from the modelling). Better outcomes are
associated with lower costs, so the NPV of the benefits (lower costs of NFF) can then be
compared with the costs of the intervention. Benefits minus costs provide the ‘net benefit’ in
dollars, while benefits divided by costs provide the ‘benefit:cost ratio’.
The process of selecting appropriate FF interventions commenced in the scoping study, when a
preliminary assessment was undertaken of 12 types of interventions:
1. family assistance and income support payments;
2. family relationship services (FRS);
3. Stronger Families and Communities Strategy, including Communities for Children and
Invest to Grow;
4. Positive Parenting Program (PPP);
5. Early childhood education;
6. Peel Child Health Survey;
7. Responding Early Assisting Children (REACh);
8. Reconnect;
9. Youthlinx;
10. Transition to Independent Living Allowance (TILA);
11. SureStart; and
For this full study, criteria were established in the first Reference Group meeting for assessing
appropriate interventions for CEA. These four criteria were:
1. Model data: the LSAC and ATP datasets will be able to accommodate ‘shocks’ to the
intervention;
2. Target age: the interventions will target different age groups (e.g. pre‐school, primary
school, youth)
3. Reach: the interventions have ‘reach’ i.e. they effectively target relevant
(disadvantaged) groups; and
4. Efficacy data: adequate information is available from Australian (preferably) or
international sources in order to provide an indication of the efficacy of interventions.
A follow‐up meeting with Steve Zubrick identified three further criteria.
5. Specificity: Interventions specifically target family functioning, rather than indirectly
affect it (e.g. income supplementation can assist with FF, but is in essence a poverty
alleviation method).
6. Sustainability: Interventions are current, and likely to continue into the future.
7. Relevance: Interventions have strong connections to or relevance for FaHCSIA.
We also reviewed literature provided by the Reference Group – Karoly et al (2007) and Wise et
al (2005). The interventions selected from this process are summarised below.
2.6.2
Communities
for
children
(CfC)
CfC meets all criteria for the CEA.
1. Model data: LSAC FF data can be linked with CfC interventions.
2. Target age: CfC is targeted to pre‐school and primary school age children.
3. Reach: CfC targets all Australian population sub‐groups.
4. Efficacy data: CfC has been evaluated with efficacy outcomes that can be imputed to
the Excel model.
5. Specificity: CfC aims to improve family functioning and outcomes for children.
6. Sustainability: The CfC program has forward funding.
7. Relevance: CfC is a FaHCSIA program.
Conclusion: CfC is one of the major Australian Government investments in
families. It has already been shown to be efficacious, and the CEA evaluation can
also determine at what cost its effective outcomes are achieved.
2.6.3
Positive
Parenting
Program
PPP meets all criteria for the CEA.
1. Model data: LSAC FF data can be linked with PPP interventions.
2. Target age: PPP is targeted to pre‐school and primary school age children.
3. Reach: PPP targets all Australian population sub‐groups.
4. Efficacy data: PPP has been evaluated with efficacy outcomes that can be imputed to
5. Specificity: PPP aims to improve family functioning and outcomes for children.
6. Sustainability: The PPP program is successful and growing.
7. Relevance: PPP is a program relevant to FaHCSIA core business.
Conclusion: PPP is one of the best evaluated programs targeted at improving
family functioning and outcomes for younger children. While its efficacy is well‐
proven, there are fewer studies on its cost effectiveness and this CEA can also act
as a tool to test/triangulate the power of the model.
2.6.4
Reconnect
In the Scoping Study Reference Group and in the 13 January Reference Group meeting the
Reconnect program was identified as being a good candidate for CEA. Again it meets all
criteria for the CEA.
1. Model data: ATP FF data can be linked with Reconnect interventions.
2. Target age: Reconnect targets youth aged 12‐18 (who are homeless or at risk of
homelessness) and their families.
3. Reach: Reconnect targets all Australian population sub‐groups.2
4. Efficacy data: Reconnect has been evaluated with efficacy outcomes that can be
imputed to the Excel model (based on two longitudinal studies).
5. Specificity: Reconnect aims to improve family functioning and outcomes for high school
aged children.
6. Sustainability: The Reconnect program is funded into the future.
7. Relevance: Reconnect is a FaHCSIA program.
Conclusion: Reconnect provides a complementary intervention targeted at an the
older cohort of children, which has been evaluated as effective, but where
nothing is yet known regard cost effectiveness.
2
Indigenous youth comprised 9% of the respondents to the longitudinal survey that formed a key element of the 2003 evaluation by the Australian Government Department of Family and Community Services (FACS, 2003:34) and ‘No differences exist between entering and exiting clients in relation to country of birth or language background’ (FACS, 2003:35). Youth were represented from all jurisdictions, from both sexes and with varying levels of case
3
Findings
from
the
LSAC
data
investigation
LSAC consists of two cohorts ‘B’ (for Baby) and ‘K’ (for Kindergarten). Each of these cohorts
has three sets of time data ‐‘waves’ of survey data taken at two yearly intervals. Information is
collected through self‐reporting and also observational measures (such as parent‐child
interactions). Child outcomes are measured as: behavioural and emotional adjustment;
language and cognitive development; and social competence.
LSAC contains specific research questions. One question focuses particularly on the impacts of
family relationships, composition and dynamics on child outcomes, and changes to these over
time. The question includes the analysis of:
■
the size and make‐up of family;■
the involvement of extended family;■
roles of family members;■
character of parental relationships and level of conflict in the family;ies, particularly in times of stress.
to represent
se
Appendix D provides a detailed description of each individual variable.
Cases
■
lationships between children and parents. In
■
parenting practices;■
child’s temperament;■
impact of family break‐up and re‐formation; and■
family coping strateg3.1
LSAC
variables
Evidence from the literature was used to edify the selection of family functioning inputs from
the ATP and LSAC that would be likely to be correlated with outcomes. The evidence is in Appendix B. In most cases, the choice of relevant LSAC variables
summarised
the general literature categories in the model is fairly straightforward. �