Infant Sleep Problems and Postnatal Depression:
A Community-Based Study
Harriet Hiscock, FRACP, and Melissa Wake, FRACP, MD
ABSTRACT. Objectives. To describe infant sleep pat-terns and investigate relationships between infant sleep problems and maternal well-being in the community setting.
Design. Cross-sectional community survey.
Setting. Maternal and Child Health Centers in 3 mid-dle-class local government areas in Melbourne, Austra-lia.
Participants. Mothers of infants 6 to 12 months of age.
Main Outcome Measures. Maternal well-being (Edin-burgh Postnatal Depression Scale) and infant sleep prob-lems (standardized maternal questionnaire).
Results. The survey was completed by 738 mothers (94% response rate), of whom 46% reported their infant’s sleep as a problem. In the univariate analyses, sleep patterns characterizing a sleep problem included the in-fant sleeping in the parent’s bed, being nursed to sleep, taking longer to fall asleep, waking more often and for longer periods overnight, and taking shorter naps. The same sleep patterns were associated with high depres-sion scores and tended to increase as depresdepres-sion scores increased.
Because of positive skew, the Edinburgh Postnatal De-pression Score was analyzed in 3 categories (<10, 10 –12, and>12) using validated cutoff scores from community and clinical studies. Fifteen percent of mothers scored above 12 on the depression scale, indicating probable clinical depression, and 18% scored between 10 and 12, indicating possible clinical depression. After adjusting for potential confounders and factors significant in the univariate analyses, maternal report of an infant sleep problem remained a significant predictor of a depression score >12 (odds ratio: 2.13; 95% confidence interval: 1.27,3.56) and>10 (odds ratio: 2.88; 95% confidence inter-val: 1.93,4.31). However, mothers reporting good sleep quality, despite an infant sleep problem, were not more likely to suffer depression.
Conclusions. Maternal report of infant sleep prob-lems and depression symptoms are common in middle-class Australian communities. There is a strong associa-tion between the 2, even when known depression risk factors are taken into account. Maternal report of good sleep quality attenuates this relationship. Appropriate anticipatory guidance addressing infant sleep could po-tentially decrease maternal report of depressive symp-toms.Pediatrics2001;107:1317–1322;infant sleep, postna-tal depression, community sample.
ABBREVIATIONS. PND, postnatal depression; EPDS, Edinburgh Postnatal Depression Scale; SD, standard deviation; OR, odds ratio; CI, confidence interval.
I
nfant sleep problems and postnatal depression (PND) are important, not only because of their high prevalence, but also because of their adverse sequelae. In Australia, more than one third of parents report problems with their infant’s sleep.1Estimates of the prevalence of PND range between 10% and 15% in the general population,2with an even higher proportion reporting problems that, although less severe, still significantly reduce maternal well-be-ing.3Infant sleep problems and PND can both impact adversely and in apparently similar ways on the mother, the infant, and the mother–infant relation-ship.2,4 Infant sleep disruption can lead to maternal sleep disruption, resulting in adverse effects on mood, cognition, and motor function,5similar symp-toms to those reported by mothers suffering from PND.2Infants with sleep problems are more likely to be tired, inattentive, and irritable and have difficulty modulating their impulses and emotions.6Children of depressed mothers experience similar problems as well as attachment difficulties and poorer cognitive and behavioral outcomes.7,8
How infant sleep problems and PND are related (and, in particular, whether 1 causes the other) is yet to be established. Case– control studies consistently report more depressive symptoms in mothers of poor sleepers than in mothers of good sleepers,9,10 regardless of social class.11 Maternal depressed mood predicts both the presence of sleep problems9 and their persistence.12 In 1 sample of consecutive mothers attending a pediatric sleep outpatient clinic, 40% reported symptoms of PND.13 Uncontrolled sleep intervention studies have demonstrated signif-icant reductions in maternal depression scores after treatment of the child’s sleep problem.13,14
We investigated the relationship between maternal depression and sleep problems for 3 reasons. First, important questions remain unanswered. What sleep behaviors do mothers consider problematic? Do de-pressed mothers differ from nondede-pressed mothers in reporting their infant’s sleep behaviors? Are de-pressed mothers characterized by a cluster of mater-nal, infant, and demographic variables, possibly in-cluding perceived infant sleep problems? Second, there are few good data describing the relationship between maternal depression symptoms and infant
From the Centre for Community Child Health, Royal Children’s Hospital, Melbourne, Australia.
Received for publication Jan 3, 2000; accepted Sep 26, 2000.
Reprint requests to (H.H.) Centre for Community Child Health, Royal Children’s Hospital, Parkville VIC 3052, Melbourne, Australia. E-mail: [email protected]
sleep problems in the community setting. Third, pre-vious studies have tended to use nonvalidated de-pression measures or measures containing items about somatic symptoms that are normal changes in the postnatal setting. In addition, small sample sizes, poor response rates, and researcher-imposed defini-tions of sleep problems have reduced the validity and generalizability of the data.
This survey addressed these issues. We examined the relationship between PND and infant sleep prob-lems in a large Australian community sample. We used a well-validated PND screening scale and stan-dard definitions of parent-reported infant sleep problems.
METHODS
Between May 1998 and April 1999, mothers attending routine hearing testing sessions at participating Maternal and Child Health Centers in 3 statistical local government areas in suburban Melbourne, Australia, were invited to take part. The areas chosen represented predominantly middle-class mothers who were deemed likely to participate in a second study involving a com-munity-based treatment of infant sleep problems. The Maternal and Child Health service is provided free to all children in the state of Victoria 0 to 6 years of age, and⬃90% of children are known to attend the hearing sessions offered to all infants 7 to 9 months of age.
After giving verbal consent to the principal investigator, moth-ers completed a 48-item survey while waiting for their infant’s appointment or were provided with a reply paid envelope if they chose to take the survey home. The survey asked for details of the infant’s sleep over the previous 2 weeks and whether the mother considered her infant’s sleep to be a problem. If the infant’s sleep was a problem, mothers were asked to rate its severity on a 7-point visual analog scale designed for the study. Maternal well-being was assessed by the Edinburgh Postnatal Depression Scale (EPDS),15a 10-item scale with scores ranging from 0 to 30. Scores
⬎10 and 12 indicate probable depression in community and clin-ical samples, respectively.16,17Mothers were also asked whether they had been previously diagnosed with depression. Infant fac-tors (sex, birth weight, gestation, delivery type, health, ordinal number, breastfeeding status, and use of childcare) and sociode-mographic factors (maternal and paternal education, employment status, occupational prestige for current or most recent occupation [ANU3 Occupational Prestige Scale],18country of birth, maternal age, and marital status) were sought.
An item regarding maternal sleep quality19was added for the final 305 questionnaires because maternal comments indicated that this might be an important intermediary between infant sleep and maternal well-being.
Ethics approval was obtained from the Ethics in Human Re-search Committee of the Royal Children’s Hospital, Melbourne, Australia.
Analyses
Because of positive skew, the EPDS score was analyzed in 3 categories using cutoff scores recommended in clinical and com-munity studies (⬍10, 10 –12, and⬎12). Univariate analyses were conducted to characterize: 1) sleep problems and 2) the relation-ship among infant, maternal, and sociodemographic variables and the 3 EPDS categories. Means and standard deviations (SDs) are reported for continuous variables that were approximately nor-mally distributed, and medians and ranges for those that were not. Pearson’s2analyses were used for categorical variables. Two-samplettests and analysis of variance were used to test differ-ences in means of continuous parametric variables, while Wil-coxon rank-sum tests were used for nonparametric variables.
For the multivariate analyses, the EPDS score was dichoto-mized in 2 ways: 1) using a cutoff score of 10 or more16and 2) using a cutoff score of 12.17The resulting binary variables were analyzed with logistic regression models to explore the association with infant sleep problems. The final models included risk factors that held an association with the dichotomized EPDS scores and variables that confounded the EPDS–sleep problem association.
Data were analyzed with Stata, Version 6 (Stata Corp, College Station, TX).
RESULTS
Of 815 eligible mothers, 674 (86%) completed the survey at the session; 110 (13%) took the survey home and 67 (8%) returned it; 1 declined to complete the survey and 30 (4%) left before being approached. The response rate from those approached was 94% (n⫽ 738).
Population Characteristics
Table 1 shows the characteristics of the sample. As expected from the geographical areas sampled, mothers were in general well-educated (62% tertiary degree), Australian born (75%), and married to em-ployed partners (96%).
Sleep Patterns
Sleep disruption was prevalent. Fifty-nine percent of infants were reported to wake 4 or more nights per week (with 37% of the total sample waking every
TABLE 1. Infant and Demographic Characteristics of the Sur-vey Population
Variable
Infant Age (mo)
Mean (SD) 8.7 (1.1)
Range 6.2–12.9
Gender (%)
Male 54.1
Female 45.9
First-born child (%) 49.3
Gestation (%)
ⱕ32 wk 0.8
33–36 wk 5.4
37–41 wk 80.1
ⱖ42 wk 13.7
Current breastfeeding practices (%)
Exclusively breastfeeding 34.0 Breast and formula feeding 21.8 Was breastfed, now formula only 37.8
Never breastfed 6.4
Demographic Maternal age (y)
Mean (SD) 33.6 (4.1)
Born in Australia (%)
Mothers 74.8
Fathers 74.6
Language spoken at home (%)
English 95.5
Marital status (%)
Single 1.4
Divorced/separated 1.1
Married/defacto 97.5
University education (%)
Mothers 61.8
Fathers 61.6
Maternal employment status (%)
Employed 31.5
Home duties/unemployed 68.5
Paternal employment status (%)
Employed 96.1
Unemployed 3.9
Maternal occupational prestige (ANU 3)
Mean (SD) 48.5 (18.4)
Range 3.7–100
Paternal occupational prestige (ANU 3)
Mean (SD) 53.5 (20.3)
night); only 13% were not reported to wake over-night. The average child in the sample went to bed at 8 pm, woke once overnight, rose at 7:30 am,and had 2 naps per day lasting 75 minutes.
Forty-two percent of mothers reported unusual events that they perceived had affected their child’s sleep over the previous 2 weeks. These included illness (reported by 26% of all mothers), teething (15%), travel (9%), guests (7%), and other (9%). Factors Associated With Report of Sleep Problems
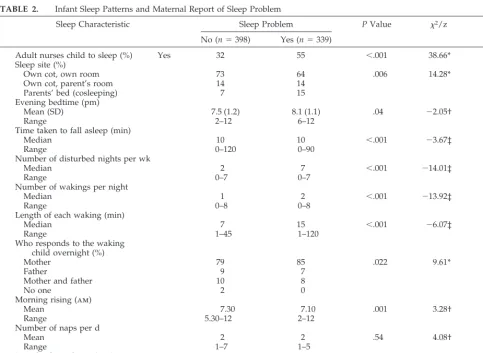
Forty-six percent of mothers reported their infant’s sleep as a problem, of whom⬎40% rated the severity of the problem asⱖ5 of a possible 7. Sleep patterns were significantly different for those reporting a sleep problem (Table 2). In particular, infants with a sleep problem were more likely to sleep in the par-ent’s bed, be nursed to sleep, take longer to fall asleep, wake more often and for longer periods over-night, and take shorter naps (all P ⬍ .01). Mothers who were exclusively breastfeeding were more likely to report a sleep problem (2⫽ 16.12; df⫽ 1; P ⬍ .001), compared with nonbreastfeeding mothers or those who gave their infant both formula and breast milk. Mean maternal occupational prestige scores were lower for those reporting sleep problems (55.2
vs 28.6;t⫽2.6;P⫽.02), but other infant and socio-demographic factors did not differ.
Factors Associated With Maternal Well-Being
The median EPDS score was 7 (mean: 7.6; SD: 4.2; range: 0 –25). Table 3 outlines sleep and nonsleep characteristics by EPDS category. Of the sleep char-acteristics, maternal report of an infant sleep prob-lem was most strongly associated with EPDS cate-gory (P ⬍ .001). EPDS scores increased with sleep problem severity (P⬍ .001). Mothers with a higher EPDS score were more likely to sleep with their child, nurse them to sleep, and report more night-time wakings more nights per week (allP⬍ .02).
A number of nonsleep characteristics were associ-ated with a high EPDS score (Table 3). These in-cluded a past history of maternal depression,being divorced, and having a partner born overseas. Logistic Regression Analyses
Many individual sleep patterns were strongly as-sociated with maternal report of a sleep problem. Because of this high collinearity, only 2 sleep pat-terns continued to be independently associated with high EPDS scores (duration of night waking and infant sleeping in the parents’ bed) over and above
TABLE 2. Infant Sleep Patterns and Maternal Report of Sleep Problem
Sleep Characteristic Sleep Problem PValue 2/z df
No (n⫽398) Yes (n⫽339)
Adult nurses child to sleep (%) Yes 32 55 ⬍.001 38.66* 1
Sleep site (%)
Own cot, own room 73 64 .006 14.28* 3
Own cot, parent’s room 14 14
Parents’ bed (cosleeping) 7 15
Evening bedtime (pm)
Mean (SD) 7.5 (1.2) 8.1 (1.1) .04 ⫺2.05† –
Range 2–12 6–12
Time taken to fall asleep (min)
Median 10 10 ⬍.001 ⫺3.67‡ –
Range 0–120 0–90
Number of disturbed nights per wk
Median 2 7 ⬍.001 ⫺14.01‡ –
Range 0–7 0–7
Number of wakings per night
Median 1 2 ⬍.001 ⫺13.92‡ –
Range 0–8 0–8
Length of each waking (min)
Median 7 15 ⬍.001 ⫺6.07‡ –
Range 1–45 1–120
Who responds to the waking child overnight (%)
Mother 79 85 .022 9.61* 3
Father 9 7
Mother and father 10 8
No one 2 0
Morning rising (am)
Mean 7.30 7.10 .001 3.28† –
Range 5.30–12 2–12
Number of naps per d
Mean 2 2 .54 4.08† –
Range 1–7 1–5
Length of usual nap (min)
Mean (SD) 78 (1.6) 72 (1.6) .009 2.63† –
Range 3–180 1–180
maternal report of a sleep problem. The final model, therefore, included maternal report of a sleep prob-lem, duration of night waking, infant sleeping in the parents’ bed, history of maternal depression, and marital status/partner born overseas (both predic-tive of depression in the univariate analyses). In this model, maternal report of a sleep problem continued to be strongly associated with EPDS scores greater
than both 10 and 12 (Table 4). Mothers with a history of depression were also more likely to have high EPDS scores. Mothers whose partners were born overseas were more likely to score⬎10 on the EPDS (odds ratio [OR]: 1.91;P⫽.003) and a similar effect was observed for those scoring over 12 (OR: 1.59;P⫽ .08).
For the subgroup of mothers (42%) with sleep
TABLE 3. Association Between Independent Variables and Maternal Well-Being (EPDS Score)
By EPDS Category PValue 2/F df
⬍10 (n⫽493)
10–12 (n⫽134)
⬎12 (n⫽111) Sleep characteristic
Sleep problem present (%) Yes 36 62 68 ⬍.001 51.75* 2
Severity of sleep problem (n⫽339) Mean (SD) 3.6 (1.4) 4.3 (1.5) 4.8 (1.4) ⬍.001 42.19† —
Adult nurses child to sleep (%) Yes 39 46 53 .02 7.81* 2
Sleep site (%)
Own cot, own room 72 63 61 .01 19.27* 6
Own cot, parent’s room 13 14 15
Parent’s bed (cosleeping) 8 17 15
Other 7 6 8
Time taken to fall asleep (min) Mean (SD) 12 (11.8) 15 (13.8) 16 (14) ⬍.001 11.23† — Number of waking nights/wk Mean (SD) 3.9 (2.7) 4.6 (2.5) 5.1 (2.4) .002 34.90† — Number of wakings/night
Median 1.4 1.7 2.2 ⬍.001 49.13‡ —
Range 0–8 0–5 0–6
Length of each waking (min)
Median 10 10 15 ⬍.001 14.87‡ —
Range 1–90 1–90 1–120
Who attends the night waking (%)
Mother 81 83 87 .6 4.56* 6
Father 8 9 6
No one/other 11 8 7
Nonsleep characteristic
Past history of depression (%) Yes 8 11 20 .001 14.75* 2
Marital status (%)
Married 91 95 83 .007 17.65* 6
Defacto 7 4 11
Single 1 0 3
Divorced 1 2 4
Mother born overseas (%) Yes 23 27 32 .12 4.17* 2
Partner born overseas (%) Yes 23 34 32 ⬍.01 6.87* 2
Assisted delivery (forceps, vacuum, cesarean) (%)
Yes 40 43 59 .64 0.89* 2
*2analysis. † Student’sttest. ‡ Mann-WhitneyUtest.
TABLE 4. ORs for EPDS Score as a Function of Report of Sleep Problem Adjusted for Other Variables
Variable EPDSⱖ10 (n⫽245) EPDS⬎12 (n⫽111)
n Unadjusted OR (95% CI)
Adjusted* OR (95% CI)
n Unadjusted OR (95% CI)
Adjusted* OR (95% CI)
Sleep problem 158 3.14 (2.28, 4.32) 2.88 (1.93, 4.31) 75 2.87 (1.87, 4.40) 2.13 (1.27, 3.56) History of depression 37 2.13 (1.32, 3.45) 2.18 (1.20, 3.96) 22 2.67 (1.56, 4.62) 2.65 (1.40, 5.01) Partner born overseas 82 1.73 (1.23, 2.43) 1.91 (1.25, 2.94) 36 1.44 (0.93, 2.22) 1.59 (0.95, 2.66) Marital status
Married† 219 1 (⫺) 1 (⫺) 92 1 (⫺) 1 (⫺)
Defacto 17 1.20 (0.28, 5.25) 1.52 (0.27, 8.54) 12 0.77 (0.16, 3.30) 0.66 (0.12, 3.56) Single 3 1.13 (0.29, 4.42) 1.27 (0.26, 6.19) 3 0.37 (0.09, 1.46) 0.33 (0.07, 1.54) Divorced/separated 6 7.48 (0.86, 56.89) 13.77 (0.88, 214.38) 4 2.33 (0.35, 16.12) 1.86 (0.19, 18.14) Duration of night waking 1.02 (1.01, 1.03) 1.02 (1.00, 1.03) 1.02 (1.01, 1.04) 1.02 (1.00, 1.03) Place of sleep
Own cot, own room† 152 1 (⫺) 1 (⫺) 68 1 (⫺) 1 (⫺)
Own cot, parent’s room 36 1.20 (0.74, 1.96) 1.39 (0.81, 2.37) 17 1.29 (0.72, 2.31) 1.32 (0.69, 2.55) Parent’s bed 40 2.20 (1.34, 3.63) 1.99 (1.13, 3.52) 17 1.80 (0.99, 3.27) 1.50 (0.76, 2.96) Sibling’s room 13 0.78 (0.33, 1.82) 1.54 (0.67, 3.51) 5 1.01 (0.38, 2.68) 1.38 (0.49, 3.92) Other 4 1.49 (0.45, 4.91) 1.36 (0.38, 4.88) 4 2.88 (0.86, 9.60) 3.78 (1.03, 13.84)
quality data available, logistic regression analyses were repeated with this predictor variable included. These mothers did not differ from other mothers in terms of marital status, past history of depression, education level, partner born overseas, or report of sleep problem. After controlling for sleep quality as good or very good, the presence of an infant sleep problem no longer predicted an EPDS score above 10 (OR: 1.22; 95% confidence interval [CI]: 0.64 –2.35) or above 12 (OR: 1. 27; 95% CI: 0.59 –2.72). Infants whose mothers reported good sleep quality were more likely to sleep in their own bed, wake less often, and settle themselves to sleep.
DISCUSSION
Infant sleep problems were reported by almost one half of the mothers in our study. Infants reported to have a sleep problem were significantly more likely to wake frequently and for longer periods, sleep in their parent’s bed, and need an adult to settle them to sleep. These behaviors are usually learnt and, as such, are amenable to change through behavior mod-ification.20 If parents could be helped to teach their infant to settle independently, mothers would not need to attend night wakings. Because these night wakings were also associated with a high EPDS score, this might decrease maternal report of depres-sion symptoms.
Depressed mothers were more likely to report the cluster of sleep patterns that characterized an infant sleep problem than nondepressed mothers. There could be several reasons for this. Depressed mothers may sleep poorly and may be more aware of their infant’s night wakings than nondepressed mothers who sleep through the night. Infants of depressed mothers may be more difficult to settle and may wake more frequently. Depressed mothers may be biased in their report of sleep problems, an issue that has not been addressed in the literature. Alterna-tively, infants who have not learnt to settle indepen-dently may disrupt their mother’s sleep resulting in maternal sleep deprivation and report of symptoms similar to depression. Because this study was cross-sectional, we cannot define causality. However, it is clear that depressed mothers perceive their infant’s sleep patterns quite differently from nondepressed mothers.
Our results confirm previous findings that child sleep problems and maternal report of depression symptoms are common in middle-class Australian communities.1,21 A strong relationship exists be-tween the 2, even when established risk factors for PND, such as a past history of depression, are taken into account. Maternal sleep quality may be an im-portant mediator in the relationship between depres-sion and infant sleep problems because mothers who reported their sleep quality as good or very good were less likely to report depressive symptoms, even when they perceived their infant’s sleep to be a prob-lem. This suggests that other factors are operating to promote good maternal sleep quality and protect mothers from depressive symptoms in the presence of an infant sleep problem.
The high response rate (94%) in our study suggests
that our results are likely to be representative of middle-class Australian populations. Prevalences of sleep problems and PND in this study were similar to Australian studies using the same measures across broader sociodemographic strata,1,21suggesting that our results may, in fact, generalize beyond a middle-class sample. Given that both PND and sleep prob-lems occur across all socioeconomic classes, it is un-likely that mothers from lower classes will be suffering less than are mothers in our sample.
Subjective report of an infant sleep problem, and its severity if present, was the principal variable against which we assessed reports of depression symptoms. Several more objective parent report measures have been proposed, usually requiring a certain number of wakings for a certain duration occurring a certain number of nights per week.10,22 Such definitions may severely underestimate the im-pact of sleep disruption experienced by families. For example, in the study by Morrell23 only 17.3% of infants met Richman’s criteria, but 35% had a sleep problem defined by the mother. From a clinical point of view, parent report may provide the most relevant and useful measure of a sleep problem. Furthermore, there is good evidence that mothers of poor sleepers report their child’s sleep patterns more accurately than mothers of good sleepers, compared with over-night video recording,24and in this study, objective indicators of disturbed infant sleep were strongly related to maternal reporting of a sleep problem.
CONCLUSION
Infant sleep problems are common and should be taken seriously. Many mothers reporting sleep prob-lems are experiencing symptoms of depression, even if they do not reach a cutoff score for clinical depres-sion. Many of the sleep patterns perceived by moth-ers as sleep problems are amenable to change, and much of this change could potentially be imple-mented in the primary care setting. Controlled trials are required to establish whether treatment of infant sleep problems can improve maternal well-being.
Randomized, controlled trials have demonstrated that with appropriate anticipatory guidance, prob-lem sleep patterns are preventable.25,26 Future re-search needs to examine whether such guidance can reduce the incidence of maternal report of depres-sion symptoms. In the interim, practitioners should be aware that a mother who reports infant sleep problems is likely to be experiencing emotional dif-ficulties. Attending to the sleep problem may not only improve the infant’s sleep, but may also have significant ramifications for the well-being of the mother, her infant, and her family.
ACKNOWLEDGMENTS
This project was funded by the Research Institute, Royal Chil-dren’s Hospital, Melbourne, and a Public Health Postgraduate National Health and Medical Research Council Scholarship.
REFERENCES
1. Armstrong KL, Quin RA, Dadds MR. The sleep patterns of normal children.Med J Aust. 1994;161:202–206
3. Brown S, Lumley J. Maternal health after childbirth: results of an Australian population based survey. Br J Obstet Gynaecol. 1998;105: 156 –161
4. Kerr SM, Jowett SA. Sleep problems in pre-school children: a review of the literature.Child Care Health Dev. 1994;20:379 –391
5. Pilcher JJ, Huffcutt AI. Effects of sleep deprivation on performance: a meta-analysis.Sleep. 1996;19:318 –326
6. Lavigne JV, Arend R, Rosenbaum D, et al. Sleep and behavior problems among preschoolers.Dev Behav Pediatr. 1999;20:164 –169
7. Beck CT. The effects of postpartum depression on child development: a meta-analysis.Arch Psychiatr Nurs. 1998;12:12–20
8. Murray L, Hipwell A, Hooper R. The cognitive development of 5-year-old children of postnatally depressed mothers.J Child Psychol Psychiatry. 1996;37:927–935
9. Lozoff B, Wolf AW, Davis N. Sleep problems seen in pediatric practice.
Pediatrics. 1985;75:477– 483
10. Richman N. A community survey of characteristics of one- to two-year-olds with sleep disruptions.Am Acad Child Psychiatry. 1981;20:281–291 11. Scott G, Richards MPM. Night waking in 1-year-old children in
En-gland.Child Care Health Dev. 1990;16:283–302
12. Zuckerman B, Stevenson J, Bailey V. Sleep problems in early childhood: continuities, predictive factors and behavioral correlates. Pediatrics. 1987;80:664 – 671
13. Armstrong KL, Van Haeringen AR, Dadds MR, Cash R. Sleep depriva-tion or postnatal depression in later infancy: separating the chicken from the egg.J Paediatr Child Health. 1998;34:260 –262
14. Leeson R, Barbour J, Ray KL, Warr R. Management of infant sleep problems in a residential unit.Child Care Health Dev. 1994;20:89 –100 15. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression:
development of a 10-item Edinburgh Postnatal Depression Scale.Br J Psychiatry. 1987;150:782–786
16. Murray L, Carothers AD. The validation of the Edinburgh Postnatal Depression Scale on a community sample. Br J Psychiatry. 1990;157: 288 –290
17. Boyce P, Stubbs J, Todd A. The Edinburgh Postnatal Depression Scale: validation for an Australian sample.Aust N Z J Psychiatry. 1993;27: 472– 476
18. Jones FL. Occupational prestige in Australia: a new scale.Aust N Z J Soc. 1989;25:187–199
19. Buysse D, Reynolds C, Monk T, Berman S, Kupfer D. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research.Psychiatry Res. 1988;28:193–213
20. Ferber R. Sleeplessness in children. In: Ferber R, Kryger M, eds. Princi-ples and Practice of Sleep Medicine in the Child. Philadelphia, PA: WB Saunders Company; 1995:79 – 89
21. Astbury J, Brown S, Lumley J, Small R. Birth events, birth experiences and social differences in postnatal depression. Aust J Public Health. 1994;18:176 –184
22. Moore T, Ucko LE. Night waking in early infancy.Arch Dis Child. 1957;32:333–342
23. Morrell JMB. The role of maternal cognitions in infant sleep problems as assessed by a new instrument, the Maternal Cognitions About Infant Sleep Questionnaire.J Child Psychol Psychiatry. 1999;40:247–248 24. Minde K, Popiel K, Leos N, Falkner S, Parker K, Handley-Derry M. The
evaluation and treatment of sleep disturbances in young children.
J Child Psychol Psychiatry. 1993;34:521–533
25. Kerr SM, Powett SA, Smith LN. Preventing sleep problems in infants: a randomized controlled trial.J Adv Nurs. 1996;24:938 –942
26. Adair R, Zuckerman B, Bauchner H, Philipp B, Levenson S. Reducing night waking in infancy: a primary care intervention.Pediatrics. 1992; 89:585–588
FIRST WORLD CONGRESS: UPDATE IN ANDROGEN DISORDERS, SEPTEMBER 12–15, 2001, GUBBIO, ITALY
Genetics, Pathophysiology, Clinical Management and Outcome in Steroidal Enzymatic Pathway Disorders, and Pathologies of Androgen-Responsive Cells
The First World Congress is sponsored by the Faculty of Medicine of the University of Rome “Tor Vergata,” Rome, Italy, and Weill Medical College of Cornell University, New York, New York.
For the first time, an international panel will bring together leaders in the fields of androgen research. The conference will address several topics including: currently debated intersex issues, hirsutism and baldness, and hormone effects on prostate cancer. In addition, the meeting will summarize the efforts of the last 2 decades in research on the biological basis of the effect of hormones on sexual development and cancer. The conference is pioneering because gender outcome of patients born with androgen excess will be reported together with the thorny problem of sex assignment of newborns with ambiguous genitalia. The study of hormones has demonstrated a much broader clinical importance than previ-ously recognized, and this program will also provide a forum for discussing the future of androgen research.
Invited lectures include: genetics of sex, gender assignment in the newborn, management of patients with ambiguous genitalia and outcome studies, prenatal therapy in congenital adrenal hyperplasia, genetic analysis of male pattern baldness and 5␣-reductase genes, androgen and estrogen receptors and prostatic cancer, gene therapy, and prostate cancer.
For Congress registration and scientific information, please contact:
USA—Maria New, MD
Professor and Chairman, Department of Pediatrics New York Presbyterian Hospital
Weill Medical College, Cornell University 525 E. 68th Street
New York, NY 10021
E-mail: [email protected]
Europe—Gaetano Frajese, MD
Professor and Chairman, Department of Internal Medicine and Endocrinology Faculty of Medicine
University of Rome “Tor Vergata” Via di Porta Pinciana, 4
00187 Rome ITALY E-mail: [email protected]
Local Organizing Committee
Professor A. Fabbri and Professor C. Moretti
Department of Internal Medicine, Faculty of Medicine University of Rome “Tor Vergata”
DOI: 10.1542/peds.107.6.1317
2001;107;1317
Pediatrics
Harriet Hiscock and Melissa Wake
Infant Sleep Problems and Postnatal Depression: A Community-Based Study
Services
Updated Information &
http://pediatrics.aappublications.org/content/107/6/1317 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/107/6/1317#BIBL This article cites 25 articles, 6 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.107.6.1317
2001;107;1317
Pediatrics
Harriet Hiscock and Melissa Wake
Infant Sleep Problems and Postnatal Depression: A Community-Based Study
http://pediatrics.aappublications.org/content/107/6/1317
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.