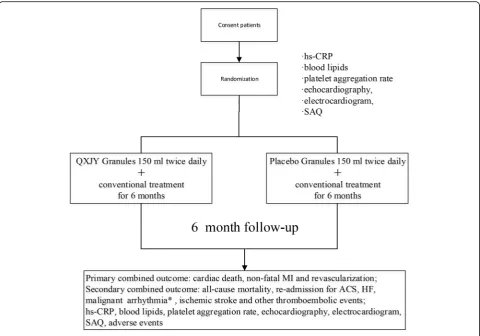
Qing Xin Jie Yu Granules in addition to conventional treatment for patients with stable coronary artery disease (QUEST Trial): study protocol for a randomized controlled trial
Full text
Figure
Related documents
We wanted to assess the real burden of IPD in children ⬍ 5 years of age in Bel- gium, compared with the existing national laboratory- based surveillance data, to calculate
Prevalence of metabolic syndrome in HIV-infected patients receiving highly active antiretroviral therapy using International Diabetes Foundation and Adult Treatment Panel III
In reply to your request that I offer some suggestions concerning measures that would improve the administration of criminal justice and reduce crime
In order to achieve maximum conversion rate (98.35%) of Ti, modeling suggested optimum values of four independent process variables, namely, temperature, KOH
The opinion is that the home should be made conducive (peaceful home) for desirable character development.. African women play vital role in this
Text document is the form of unstructured data. Most of the data that is available on web is unstructured data. The research of applying data mining techniques to unstructured data
MAbs C11-12 and E4-2 were more sensitive at detecting the rNP of JUNV, with detection limits of 7.82 and 3.91 ng/well, respectively, and these Ag capture ELISAs also detected the
