Predoctoral Dental Education
Complementary and Alternative Medicine
in Predoctoral Dental Curricula: An
Exploratory Survey of U.S. Dental Schools
Michael L. Spector, D.M.D., M.S.; Colleen M. Kummet, M.S.;
David C. Holmes, D.D.S., M.S.
Abstract: The purpose of this study was to identify the prevalence of complementary and alternative medicine (CAM) education in U.S. dental schools. A survey was administered via e-mail to each U.S. dental school’s academic dean, and data were col-lected from respondents in a fillable PDF form submitted electronically to the study investigators. The survey asked respondents whether CAM was taught at the institution; if the response was yes, information was requested regarding the CAM therapies included, credentials of the instructor, number of hours taught, reason for teaching CAM, and format in which CAM was taught. Of the sixty dental schools contacted, twenty-two responded to the survey (37 percent response rate). Of these respondents, ten (45.5 percent) reported offering instruction in CAM as part of their predoctoral curricula. Herb/drug interactions were found to be taught with more frequency than any other CAM topic (in six out of the ten institutions). Limitations of the study are discussed, and suggestions for future studies are made.
Dr. Spector is Assistant Professor, Department of Family Dentistry, College of Dentistry, University of Iowa; Ms. Kummet is Biostatistician, Dows Institute for Dental Research, College of Dentistry, University of Iowa; and Dr. Holmes is Professor and Head, Department of Family Dentistry, College of Dentistry, University of Iowa. Direct correspondence and requests for reprints to Dr. Michael L. Spector, Department of Family Dentistry, College of Dentistry, University of Iowa, 313 Dental Science Build-ing South, Iowa City, IA 52242-1001; 319-335-7322; [email protected].
Keywords: complementary therapies, alternative medicine, dental curriculum, dental education
Submitted for publication 12/12/12; accepted 2/5/13
C
omplementary and alternative medicine(CAM) was defined by Barnes et al.1 as “a group of diverse medical and health care systems, therapies, and products that are not presently considered to be conventional medicine.” Examples of more common CAM therapies include, but are not limited to, the following: acupuncture, Ayurvedic medicine, homeopathy, naturopathy, megavitamin therapy, chiropractic therapy, herbal medicines, massage therapy, biofeedback, hypnosis, meditation, deep breathing exercises, yoga, Tai Chi, prayer for healing, and Reiki. A review of the classifications and definitions of CAM therapies is found in the 2007 National Health Statistics Report by Barnes et al.2
The use of CAM in the U.S. population has risen in the past twenty years. Estimates of the gen-eral population’s use of some type of CAM modality within the past year have ranged from approximately 30 to 60 percent.1-5 In 1991, Eisenberg et al.3 studied CAM usage in the general population, focusing on sixteen categories of therapies the authors considered
complementary or alternative in nature. This study reported that 34 percent of the population used at least one of the above-mentioned CAM therapies within the past year. A subsequent survey conducted by the same group in 19974 found that 42 percent of the population had used a CAM therapy in the past year. More recent data from the 2002 National Health Interview Survey (NHIS),1 conducted by the Centers for Disease Control and Prevention (CDC), showed that 62 percent of the population used a CAM therapy including prayer within the past year. Excluding prayer, the survey found that 36 percent of the population used some form of CAM within the past year. Data from a CDC survey in 20072 revealed that almost 40 percent of those surveyed had used some form of CAM within the past twelve months. In a pilot study examining CAM usage by patients in one dental school clinic, the investigators reported that 67 percent of those patients had used a CAM therapy within the past twelve months (excluding prayer).6 About one in ten of these dental school
tems Inc., San Jose, CA), submitted electronically to the investigators.
We searched for a validated instrument to use in this study, but because no articles had been published on this topic, creation of a questionnaire was necessary. Drawing on our experience in CAM and curriculum management, we composed a draft survey instrument. Following iterative review and input from other faculty members at our home in-stitution with similar experience and expertise in these areas, the final version of the questionnaire was accepted. The final survey briefly described CAM to the participants and then asked seven questions about the incorporation of CAM in the respondent’s predoctoral curriculum (contact the corresponding author for a copy of the survey).
The survey first asked if the respondent’s in-stitution incorporated CAM subject material into the predoctoral curriculum. If the answer was “no,” the survey was then complete. If the answer was “yes,” the respondent was asked six questions: 1) Which CAM topics are being taught? (a check-off list of CAM therapies was provided, along with space for “other therapies not listed”); 2) Who is teaching CAM material, and what are their credentials? (a check-off list of provider types was provided, along with space for “other provider” not listed); 3) How many hours of CAM material are taught in each year?; 4) What format is the CAM material presented to pred-octoral students? (a check-off list of lecture, PBL, Web-based, invited lecture outside curriculum was provided, along with space for “other” not listed); 5) Why is CAM taught to the predoctoral students (a check-off list of reasons was provided, along with space for “other reasons” not listed); and 6) an open-ended comments section about CAM curriculum at their institution.
If the academic dean did not respond to the first e-mail, a follow up e-mail was sent four weeks later. If the academic dean still did not respond, a follow-up phone call was made (by the first author, MS) two weeks after the last e-mail to request participation. If no response was obtained after these three attempts, we considered the institution to be a non-responder. All academic deans were able to opt out by replying to the initial e-mail and telling the research team they did not wish to participate. The research team then respected the individual’s wishes and did not contact that institution further. Data were then imported from the PDF data repository to SAS 9.3 (SAS Institute Inc., Cary, NC) for analysis.
clinic patients used topical herbal oral products to treat dental conditions.
These reports of CAM usage across different studies must be interpreted with caution because the studies did not use uniform taxonomy and classifica-tion systems; thus, comparison of CAM therapies across studies may not have ideal scientific validity. An excellent discussion of classification criteria and a proposed new classification system can be found in Kristoffersen et al.’s 2008 article.7 Although it may be difficult to provide a precise percentage of CAM usage in the general population, it is clear that usage is relatively widespread. As such, it can be expected that dentists will see patients in their practice who are using some form of CAM therapies.
The role of predoctoral dental educators in teaching procedural CAM therapies to our students can be debated. However, a strong case can be made that we should prepare future dentists to responsibly treat patients who are already using these therapies. This would support the current movement toward developing and training our graduates to be part of collaborative health care teams.8,9 It also appears that the preponderance of patients using CAM are doing so in conjunction with allopathic (conventional) medicine; thus, they are not abandoning allopathic medicine, only complementing it with CAM thera-pies.4,10,11 The interprofessional health care team may have an allopathic physician or CAM therapist pre-scribing CAM therapies to the patients that current and future practicing dentists are treating.
To date, no data have been published about the specific educational training given to U.S. dental students with respect to complementary and alterna-tive medicine. The aim of our study was therefore to investigate the CAM education being provided in U.S. predoctoral dental curricula.
Methods
The study was approved by the University of Iowa’s Institutional Review Board (#201201765). Assistant/associate deans for academic affairs or deans for curriculum (known informally as academic deans) were identified for the then-sixty U.S. dental schools as listed in the 2010-11 ADEA Directory of Institutional Members and Association Officers.12 An electronic survey regarding CAM in dental school curricula was administered via e-mail to each of these individuals. Data were collected from respondents through the use of a fillable PDF form (Adobe
Sys-included were those with a medical degree (M.D.), speech pathology training, nutrition, adult nurse prac-titioner (ANP), psychologist, behavioral scientist, and biomedical scientist.
Hours of CAM Instruction
These respondents reported that CAM instruc-tion was most commonly provided to second-year dental students, with six schools (60 percent) pro-viding at least one credit hour in the second year. Instruction in CAM therapies was said to be least often provided to fourth-year dental students, with only two schools (20 percent) providing any credit hours to fourth-year students. The mean number of credit hours provided in each year is summarized in Table 2.
Respondents from five schools (50 percent) reported providing no instruction in the first year of dental school, while two schools (20 percent) offered one credit hour to first-year dental students. Three schools offered more than one credit, with two, three, and 4.5 credits of CAM instruction being offered in the first year. Respondents from four schools (40 percent) said the curriculum provided no instruction in the second year of dental school, while two schools (20 percent) offered one credit hour to second-year dental students. Three schools offered two credits of CAM instruction, and one school offered three credits to second-year students. Six schools (60 percent) provided no instruction in the third year of dental school. One, 1.5, two, and 7.5 credits were provided by the four schools that taught CAM in the third year. Eight schools (80 percent) provided no instruction
Results
Of the sixty dental schools contacted, twenty-two responded to the survey (37 percent response rate). Of the twenty-two respondents, ten (45.5 percent) responded that their institution provided instruction in CAM as part of their predoctoral cur-ricula. The following is a descriptive analysis of responses from the ten responding institutions.
Types of CAM Taught and
Instructors’ Credentials
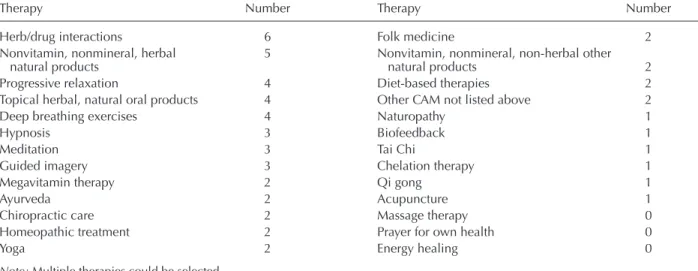
The survey asked respondents to specify which CAM therapies were addressed in their curricula. Table 1 shows the number of institutions (out of ten) that indicated they provided instruction in each CAM category. Respondents could mark as many catego-ries as were applicable. The number of CAM thera-pies included ranged from one to seventeen, with a mean of 5.6 therapies per institution (median=4.0). The most commonly reported number of therapies being taught was four.
Half of the institutions that were teaching CAM therapies (five schools, 50 percent) indicated that the courses were taught by Pharm.D. or pharmacology faculty members. In two schools (20 percent), faculty members with D.D.S. degrees and special training in a CAM field taught the CAM therapies, and two schools (20 percent) indicated that faculty members or invited speakers with a CAM degree were teach-ing that subject. Five schools (50 percent) reported having CAM instructors with other qualifications;
Table 1. Number of institutions providing instruction in each CAM therapy out of the ten that reported teaching CAM
Therapy Number Therapy Number
Herb/drug interactions 6 Folk medicine 2 Nonvitamin, nonmineral, herbal 5 Nonvitamin, nonmineral, non-herbal other natural products natural products 2 Progressive relaxation 4 Diet-based therapies 2 Topical herbal, natural oral products 4 Other CAM not listed above 2 Deep breathing exercises 4 Naturopathy 1
Hypnosis 3 Biofeedback 1
Meditation 3 Tai Chi 1
Guided imagery 3 Chelation therapy 1 Megavitamin therapy 2 Qi gong 1
Ayurveda 2 Acupuncture 1
Chiropractic care 2 Massage therapy 0 Homeopathic treatment 2 Prayer for own health 0
Yoga 2 Energy healing 0
dentists are seeing and will continue to see patients who are using CAM therapies. Understanding these therapies and their implications for patients’ oral and systemic health is a critical component in providing optimal care. Our purpose for this study was to fill a void in the literature about how CAM is being taught to predoctoral students in U.S. dental schools.
The fact that only twenty-two of the sixty (37 percent) academic deans responded to this survey may lead one to believe that there is a low level of interest in this topic in the dental school community. We believe this to be the case to a certain extent. CAM instruction may not be a high priority for the academic deans for many reasons. We speculate that if the topic related to an accreditation standard, then perhaps the response rate may have been higher. We also feel that the topic of complementary and alter-native medicine may have a negative connotation considered non-scientific subject matter and thus this survey might not have occupied a high priority in the respondents’ busy schedules.
This study may also have faced limitations because of its methodology, so we would like to elaborate on possible future strategies for eliciting a better response rate in subsequent surveys. It has in the final year of dental school. Courses in CAM
of one and three credits were offered at the only two schools providing CAM education to fourth-year dental students. One school provided three credit hours of CAM education in addition to the curricula for other dental school years.
Reasons and Format for Teaching
CAM
Respondents to the survey were asked to report the reasons that CAM was taught to their predoctoral students; multiple reasons could be selected (Table 3). Respondents from four institutions (40 percent) indicated that their students requested the informa-tion, and respondents from three schools (30 percent) indicated that either the faculty or the institution was interested in providing instruction. Respondents from two schools said they provided instruction in CAM to better prepare students, and respondents from two other schools indicated that the reason for teach-ing CAM was the widespread use of CAM among patients. One school provided CAM instructions to help students manage stress, and one indicated that the instruction was provided to make students aware of patients’ personal, religious, and health beliefs and traditions so that the student-practitioners avoid offending their patients.
Respondents from nine schools (90 percent) indicated that CAM instruction was provided to predoctoral students in lecture format, while re-spondents from two schools (20 percent) indicated that PBL or invited lectures were used. One school provided instruction in CAM as part of a hospital clerkship rotation.
Discussion
As current and future dental students embark on their paths towards treating the public’s oral health needs, it is the role of dental educators to prepare stu-dents to the best of our abilities. There is no doubt that
Table 2. Credits of CAM instruction offered by school and year
Year 1 Year 2 Year 3 Year 4 Other
Number of schools 5 6 4 2 1
Mean credit hours 1.30 1.83 3.00 2.00 3.00 Range 1 to 4.5 1 to 3 1 to 7.5 1 to 3 3
Table 3. Reasons respondents gave for why CAM is taught to predoctoral students at their institution
Reason Number Students demand the information 4 ADA recommendations 0 Accreditation recommendations 0
Other 9
Faculty interest 2 Institution desires to expose students 1 Students’ own stress management 1 Make students aware of personal, religious, 1 health beliefs, and traditions, and avoid offending patients
Prepare students to become better providers 2 Widespread use and impact on dental care 2
and appreciate the rationale and value for teaching these subjects.
This study found that herb/drug interactions were being taught with more frequency than any other CAM topic (in six out of the ten institutions) and the subject of non-vitamin, non-mineral, herbal natural products was also being taught with high frequency (in five out of the ten institutions). It is im-perative that practicing dentists be familiar with herb/ drug interactions since a large number of patients may be using herbal remedies, which can interact with the drugs dentists use and prescribe. Little provides a review of the subject with respect to dentistry;16 he describes the various complementary and alternative therapies and provides a detailed discussion of drug/ herb interactions.
As we reviewed the data regarding other thera-pies being taught with higher frequencies, possible patterns emerged. Progressive relaxation (four out of ten schools), deep breathing exercises (four out of ten), hypnosis (three out of ten), meditation (three out of ten), and guided imagery (three out of ten) are all associated with easing patient anxiety associated with dental visits. The institutions teaching these therapies evidently place value on introducing or teaching these CAM modalities, and it may be worth the consideration of other institutions interested in incorporating CAM.
With regard to who is teaching the CAM sub-jects to predoctoral students, we observed that half of the institutions responding (five schools, 50 percent) indicated that CAM courses were taught by Pharm.D. or pharmacology faculty members. In two schools (20 percent), faculty members with D.D.S. degrees and special training in a CAM field taught the CAM courses, and two other schools (20 percent) indicated that faculty members or invited speakers with a CAM degree were teaching this subject. These results may be encouraging to administrators as they can see that it may be quite possible to incorporate CAM thera-pies into the predoctoral curriculum without hiring additional faculty members. Our findings seem to indicate that CAM is being taught to predoctoral students by faculty members already at the dental schools or by inviting them to lecture on the topic on an ad hoc basis.
Dental educators contemplating incorporation of CAM into their curricula can see from the results of our study that CAM can be placed anywhere in a four-year program, although CAM instruction was most commonly provided to second-year students (with 60 percent of the ten schools providing at least been reported that an Internet survey like the one
we used may generate lower response rates than a survey using traditional mail.13-15 We concur with the recommendation of Krause et al.14 that, in future survey-based studies with dental schools, the inves-tigators may want to consider using an approach that combines e-mail and a paper survey. Another possible way to increase the response rate for future studies would be to contact the deans of the schools, rather than the academic deans. While we assumed that the names we chose were the appropriate con-tacts (as identified in the 2010-11 ADEA Directory of Institutional Members and Association Officers), they may not have been the correct person to contact for this purpose, and this may have had a negative influence on response rate. Perhaps the dean may have been able to more accurately direct the survey to the appropriate school representative, thus possibly increasing the response rate.
In addition to improvements in the survey de-livery for future studies, we envision some potential refinements to the instrument. It would be interesting, for example, to ask whether the schools who do not have CAM instruction at present are considering it in the future. Further, in order to elicit more useful responses to question #5 (“Why is CAM taught to predoctoral students? What is the objective of teach-ing CAM material?”), it might be more productive to include more response choices or to leave the question open-ended.
In an effort to keep the questionnaire brief, we elected to not include definitions of the individual CAM therapies on the instrument. We presumed that respondents would recognize the therapies being taught at their school and that if they did not recog-nize a therapy on the list, the school was not teaching it. Most of the CAM therapies on the questionnaire are well known or self-explanatory, but others, such as Ayurveda (an ancient Indian system of medicine) and Qi gong (an ancient Chinese healing discipline), are more obscure. For future studies, it might be worthwhile to include a glossary or appendix of definitions with the survey instrument.
Even with the low response rate, we do feel the information collected is valuable and warrants dissemination. Not only will the data serve as a starting point for future work, but it may also serve as a roadmap for dental schools considering add-ing a CAM component. An institution plannadd-ing to incorporate information on CAM therapies can look at the data presented with respect to the CAM top-ics being taught at the ten institutions reported here
ternative medicine use among adults and children: United States, 2007. Natl Health Stat Report 2008;12:1-23. 3. Eisenberg DM, Kessler RC, Foster C, et al.
Unconven-tional medicine in the United States: prevalence, costs, and patterns of use. N Engl J Med 1993;328(4):246-52. 4. Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alter-native medicine use in the United States, 1990-97: results of a follow-up national survey. JAMA 1998;280(18): 1569-75.
5. Astin JA. Why patients use alternative medicine: results of a national study. JAMA 1998;279(19):1548-53. 6. Spector ML, Fischer M, Dawson DV, et al.
Complemen-tary and alternative medicine usage by patients of a dental school clinic. Spec Care Dent 2012;32(5):177-83. 7. Kristoffersen AE, Fønnebø V, Norheim AJ. Use of
complementary and alternative medicine among patients: classification criteria determine level of use. J Altern Complement Med 2008;14(8):911-9.
8. Polverini PJ. A curriculum for the new dental practitio-ner: preparing dentists for a prospective oral health care environment. Am J Public Health 2012;102(2):e1-3. 9. Schmitt M, Blue A, Aschenbrener CA, Viggiano TR. Core
competencies for interprofessional collaborative practice: reforming health care by transforming health profession-als’ education. Acad Med 2011;86(11):1351.
10. Astin JA. Why patients use alternative medicine: results of a national study. JAMA 1998;279(19):1548-53. 11. Druss BG, Rosenheck RA. Association between use
of unconventional therapies and conventional medical services. JAMA 1999;282(7):651-6.
12. American Dental Education Association. 2010-11 direc-tory of institutional members and association officers. Washington, DC: American Dental Education Association, 2010.
13. Leece P, Bhandari M, Sprague S, et al. Internet versus mailed questionnaires: a controlled comparison. J Med Internet Res 2004;6(4):e39.
14. Krause M, Vainio L, Zwetchkenbaum S, Inglehart M. Dental education about patients with special needs: a survey of U.S. and Canadian dental schools. J Dent Educ 2010;74(11):1179-89.
15. Raziano DB, Jayadevappa R, Valenzula D, et al. E-mail versus conventional postal mail survey of geriatric chiefs. Gerontologist 2001;41(6):799-804.
16. Little JW. Complementary and alternative medicine: im-pact on dentistry. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98(2):137-45.
one credit hour in the second year). With respect to format, it appears that lectures were being used most often in most programs teaching CAM therapies (90 percent of the ten schools). However, other formats are also possible, and indeed PBL format and hospital clerkship rotations in CAM were reported as well. It is interesting to note that 40 percent of the responding schools reported that their students requested expo-sure to complementary and alternative medicine. This suggests that faculty at those universities recognize the value of students’ opinions and that they consider this input seriously in curricular decisions.
Twelve of the twenty-two schools that respond-ed to this survey reportrespond-ed not having specific courses about complementary and alternative medicine in their curricula. It should be noted that this does not mean that CAM principles and therapies are not being taught at these institutions since CAM content may be embedded within other courses. It is also possible that questions about CAM are included in the dental school clinic’s patient health history forms. The am-biguity on this point is another limitation of our sur-vey, and other researchers should consider clarifying these points in future surveys. This limitation of our instrument suggests that students’ exposure to CAM therapies may be underrepresented in our study.
Despite its limitations, this study was the first to explore the integration of CAM into predoctoral dental curricula in the United States and as such serves to establish preliminary data and begin a dialogue on the subject. We hope that future studies provide more data that will enable researchers to begin to make recommendations about the amount and content of CAM therapies taught to predoctoral dental students in order to help them become better prepared practitioners.
REFERENCES
1. Barnes PM, Powell-Griner E, McFann K, Nahin RL. Complementary and alternative medicine use among adults: United States, 2002. Adv Data 2004;343:1-19. 2. Barnes PM, Bloom B, Nahin RL. Complementary and