International Journal Advances in Social Science and Humanities
Available online at: www.ijassh.com
RESEARCH ARTICLE
Validating the Integrated Person-Centered and Existential Therapy
Model (IPCE) for the Treatment of Combat Veterans with Posttraumatic
Stress Disorder
Venter Henry J*
Psychological Department, National University, California.
*Corresponding Author: Email: [email protected]
Abstract
The findings and results of various studies on the prevalence and treatment of mental health disorders among US military and veteran populations, particularly Posttraumatic Stress Disorder (PTSD), indicated a need to focus on Person-Centered and Existential Treatment modalities to address the issues of moral injury and dysfunctional meaning ascribed to war trauma. Preliminary data will be presented to statistically show the effectiveness of a treatment the Integrated Person-Centered and Existential (IPCE) model developed to address the underlying existential issues of wartrauma such as loss of meaning and purpose among veterans diagnosed with PTSD. The IPCE model effectively translates the tenets of Existential Theory and Person-Centered therapy into a counseling process that is more readily accessible to practitioners and a model that can provide a measurable impact on outcomes and is replicable.Since the IPCE five-phase model lends itself to be quantifiable and measurable it is suitable for qualitative research that can provide evidence-based information of Existential therapy outcomes in the treatment of veterans with PTSD. The aim of this pilot study is to determine the effectiveness of a newly developed psychotherapy model using Person-Centered and Existential Theory for the treatment of veterans with PTSD.
Keywords: Posttraumatic stress disorder, Combat veterans, Person-Centered therapy, Logotherapy, Existential
therapy.
Introduction
The last ten years have been marked by a surge in United States (US) military personnel and veterans seeking treatment for service connected psychological and mental health issues following several military operations. In 2004, 15.6% to 17.1% of soldiers returning from Iraq and Afghanistan reported with symptoms of PTSD, depression, and general anxiety with 35% of Iraq war veterans requiring mental health care in the first year after deployment. In 2007, 20.3% active duty and 42.4% reservists screened positive for mental health disorders; in 2008 18.5% of Iraq and Afghanistan veterans reported depression and PTSD [1]. Of the 289,328 veterans seeking health care for the first time, 36.9% received one or more mental health diagnoses; 21.8% (60,000 plus) had PTSD and 17.4% depression [2]. Not only is the alarming high amount of veterans seeking help a problem, but providing effective therapy or high-quality care - defined by the Institute of Medicine (IOM) in their 2012 study as safe, effective, patient-centered, timely, efficient, and equitable treatment of any physiological or psychological problem - is equally a challenge.
Historically,Person-Centered, existential and experiential treatment modalities did not lend itself to psychometric research to render statistical analysis of its significance due to being too abstract and not focused on diagnosis. This research project developed a treatment approach using the theory and principles of Person-Centered, existential and experiential treatment modalities structured in five phases with specific goals and outcomes in each phase that can be measured with pre- and post-testing and statistically analyzed for effectives.
Literature Review
The returning veteran is not only suffering from symptoms of the PTSD syndrome, but is suffering loss on a larger metaphysical scale including the loss of the world as they once knew it – the world now suddenly has little meaning or sense after returning from war to civilian life. This kind of metaphysical loss cannot be cured by drugs, catharsis, deconditioning, or support alone [4]. Greening [4] stated that for most humans, the meaning of illness, any illness or disorder, begins with the loss of a world. It is vital to help reconstruct this world when providing counseling to populations such as the combat veteran suffering from PTSD. Recent studies confirmed the effectiveness of humanistic and existential therapeutic approaches to addressthis metaphysical problem including the loss of meaning and purpose [5-7]. Logotherapy is a distinct branch of the Humanistic/Existential School of Psychotherapy with a focus on the meaning of human existence as well as man’s search for such a meaning developed by Viktor Frankl [8-10]. What sets Frankl apart is his unconditional affirmation of life’s meaning. The Greek word Logos can mean “the word”, “the will of God”, “the controlling principles of the universe” or “meaning.”Frankl translated logos as meaning and called his approach Logotherapy [8,9]. Therefore, Logotherapy means healing and health through finding meaning in life. The main objective of Logotherapy is to address the existential crisis a person experiences due to a loss of meaning in life and facilitate his or her quest to find meaning in any circumstance or event, thereby empowering them to live meaningfully and responsibly regardless of their life circumstances. Recent empirical investigation of Frankl’s Logotherapy has been proven effective in addressing issues of meaning and purpose [11]. Logotherapy was put to a severe test in a very personal way between 1942 and 1945, when Frankl was committed to Nazi concentration camps. His experience and observation about that period supported the main thesis of Logotherapy:
“This was the lesson I had to learn in three years spent in Auschwitz and Dachau: those most apt to survive the camps were those oriented toward the future, toward a meaning to be fulfilled by them in the future” [9].
The humanistic and specifically the Person-Centered approach to counseling developed by Carl Rogers have been proven to be effective regardless of which theoretical approach it is integrated with. Person-Centered therapy has recently been effectively integrated by various therapeutic approaches including with cognitive therapy treating anxiety; with prolonged exposure in mediating PTSD symptoms reduction [12]; and Cognitive Remediation Therapy in the Whole Psychosocial Rehabilitation Process in an evidence-Based approach [13]. The fluidity of Existential therapy makes it an ideal foundation for an integrative approach to therapy [14]. The three pillars of Person-Centered therapy, empathy, congruence and unconditional positive regard enables the therapist to create a safe and trusting environment in which clients can explore their lives and consider change [15-17]. One of the tenets of Person-Centered therapy is to help the person discover incongruence in their lives, which withholds them from being authentic and free people who lives in the present [15-17]. One of the incongruences is the loss of meaning and purpose experienced by the combat veteran returning from war and suffering from PTSD. Therefore, Person-Centered Theory is a natural fit to integrate with Existential Theory when pursuing metaphysical loss and moral injury.
Person-Centered and existential psychotherapeutic approaches, especially treating serious psychological disorders such as veterans with combat-related PTSD. For this reason there is a need for more refined models of treatment which specifically focus on the underlying issues behind symptoms.
The Present Study
In light of the observed shortcomings of existing treatment models the researcher developed a psychotherapeutic treatment model consisting of a five-phase integrated Person-Centered and Existential Treatment program for veterans with combat related PTSD based on the tenets of Victor Frank’s Logotherapy [8] and Carl Rogers’ Person-Centered therapy [15-17]. The treatment model is called Integrative Person-Centered and Existential Therapy (IPCE) with five phases in the treatment process: Impact, Meaning, Process, Action, and Continuity (IMPAC). It is based on the core set of Person-Centered therapy, which focuses on creating a safe, unconditional environment and Existential Theory with a focus on the loss of meaning. This model effectively translates the tenets of ExistentialTheory and Person-Centered therapy into a measurable counseling process that is more readily accessible to practitioners and one that can provide a measurable impact on counseling outcomes. Since the five-phase model lends itself to be quantifiable and measurable it is suitable for qualitative research that can provide much needed evidence of Existential treatment outcomes in the treatment of serious psychological disorders. Treatment Philosophy of Integrated
Person-Centered and Existential Therapy (IPCE) The treatment philosophy of the newly developed
treatment program is unique in that it goes beyond symptom reduction and focuses on the whole person. The purpose is to process the root of anxiety and create new meaning of life thereby fostering connectedness to life and to others. The root of Existential therapy is that people cannot begin to heal from their experiences of trauma unless they are supported as whole beings and provided a safe conduit to explore their world and reconnect with themselves and others [8].
The treatment will focus on developing an understanding of the veteran in his or her world, their capacities to be in the world, and the barriers or incongruences that are preventing them from fully experiencing those capacities [15-17]. The treatment program will address the issues behind the trauma including guilt, responsibility, despair, and loss. Itwill specifically focus on the meaning the veteran is ascribing to
his or her trauma and the world he or she is in now, because when people encounter traumatic events their ability to make sense of the senseless is not only thwarted by the overwhelming traumatic experiences, but also altered in a way that gives traumatic experiences power over their world. The model specifically focuses on: Developing an understanding of the veteran in his or her world; their capacities to be in the world; the barriers that are preventing them from fully experiencing those capacities; the existential issues behind the trauma including guilt, responsibility, despair, and loss; and the meaning the veteran is ascribing to his or her trauma and the world he or she is in now. When encountering traumatic events peoples’ ability to make sense of the senseless is not only thwarted by the overwhelming traumatic experiences, but also altered in a way that gives experiences power over their world. Without addressing these underlying causes of trauma, life becomes a day-to-day struggle to survive the intrusive, the horrific, and the paralyzing world that has the traumatized veteran feeling there is no exit or escape [4,18].
Description of Integrated Person-Centered and Existential Therapy (IPCE)
The treatment model is called Integrative Person-Centered and Existential Therapy (IPCE) with five phases in the treatment process namely: Impact, Meaning, Processing, Action, and Continued Growth (IMPAC). IPCE is based on the core set of ExistentialTheory with a focus on the loss of meaning or dysfunctional meaning ascribed to traumatic events. This model effectively translates the tenets of Existential Theory and Person-Centered therapy into a measurable counseling process that is more readily accessible to practitioners and a model that can provide a measurable impact on counseling outcomes and is replicable. Since the five-phase model lends itself to be quantifiable and measurable it is suitable for qualitative research that can provide much needed evidence of experiential treatment outcomes in the treatment of serious psychological disorders such as combat-related PTSD. The therapist moves to the next phase when he or she is certain that the goals of the phase have been accomplished. The five phases cover the following:
and trusting environment using the three pillars of Person-Centered therapy, empathy, congruence and unconditional positive regard [15-17]. The veteran is helped to reflect on the history of the trauma, what happened during the trauma, with focus on how it changed or affected his or her life instead of only focusing on what is wrong with the veteran, for example just talking about symptoms. In this phase it is important that the person receives the message that he or she is more than just the sum of the symptoms making up PTSD. Every person is unique and in some way each person’s PTSD will manifest in a different manner. The premise of IPCE is that trauma gains a hold over people and keeps them trapped in the past, but in the process the person is not aware of what it is that is keeping him or her trapped. This phase gives the therapist a window into the person’s past and present and helps the therapist to develop an idea of how it must be to be the veteran, which is the cornerstone of empathy. Empathy is both a counseling technique and a way of being with the veteran which conveys the notion that they are completely understood and accepted regardless of what happened to them, what they did, and how it affected them.
Phase 2: Meaning - discovering the meaning ascribed to the trauma: The essential question of this phase to the client is: “Why do you think the event that cause your trauma happened to you and what is the meaning you ascribed to it and your life?” The focus of this phase is helping the veteran discover the dysfunctional and negative meaning they ascribed to the trauma, themselves, and their lives. This is the point in therapy where it is explored with the client that the loss of meaning and purpose they are experiencing in the present are trapping them in the consequences of the past and therefore keeping them chained to the pain of the trauma. Examples of dysfunctional meaning includes self-statements such as: I can never trust people again; I can never get close to someone else (when they lost buddies); my life is over; I don’t deserve to be alive; I don’t deserve happiness; I need to suffer for what I’ve done. Each person ascribes something unique to themselves and the trauma and it is often this ascribed meaning that can keep a person trapped in their trauma and the past. This phase takes the veteran further than just telling the story as in Phase 1 and explores possible dysfunctional meanings or loss of meaning the veteran experiences. One of the tenets of Person-Centered therapy is to help the person discover incongruence in their lives, which withholds them from being authentic and free
people who lives in the present [28, 29, 30]. Attentive listening during the first phase would have given the therapist an idea of how the veteran views the trauma of the past or if meaning is absent in their lives.
Phase 3: Processing - processing the effects of dysfunctional meaning: The essential question in this phase to the client is: “How can you view what happened to you differently?” Now that the therapist has a better understanding of the veteran’s past and what happened to him or her and a clear idea has been formed of the meaning ascribed to the trauma and the past, the veteran can be assisted in brainstorming how they can view the past differently. In IPCE therapy, according to the principles of Person-Centered and ExistentialTheory, solutions are not prescribed to the person [8,10, 15,16,17]. Every person is unique and will take more or less time to explore how they can view the past differently. With the help of the new perspective developed during the first two phases the veteran is encouraged to explore different views or interpretations of the past with new self-statements such as: “I did not betray my friends by surviving the war and coming back alive”; “I’m not a criminal that should be punished because I killed someone in war”; “my life is not over”. Taking personal responsibility is a major tenet of Person-Centered and ExistentialTheory and, therefore it is important that the veteran is empowered during this phase to take responsibility for changing their way of thinking. The idea during this phase is not to make any major life changesyet but simply to reflect on how
the past could be viewed differently.
past. Memorializing is one of the techniques used in this phase and, for instance, the veteran may decide to write a letter to his or her deceased friends to share whatever thoughts they want to, which often includes asking forgiveness. Often they write a statement to themselves for forgiveness and to let go of the past. They may also write poems or make a painting or a collage. These acts of memorializing are also called anchors. The focus is to not simply let them make a decision about the future but to anchor it in an action they can remember or to memorialize the decision in a way they can vividly recall. Veterans who have lived isolated lives or lives focused only on themselves and their problems, often decide to join a group or start doing volunteer work to break the pattern of egocentric isolation.
Phase 5: Continued - planning for future growth: The essential question of this phase to the client is: “How do you plan to continue growing and healing?” This phase focuses on cementing the new decision veterans made in the previous phase. If a veteran for instance decided to start volunteering it will not be easy to find the right place or group. This phase focuses on assisting them in implementing changes and keeping with their decisions. During this phase the first four phases must be summarized and reviewed to ensure that the veteran maintains their new perspective. At the same time this phase focuses on the future to ensure that the veteran implements changes they made during the therapy. This is also the time where the veteran is helped to decide if they should pursue further therapy, such as joining a group. The notion is conveyed to the veteran that healing is a process and a journey and often not accomplished in one therapy approach. As such, many veterans will benefit from joining a group therapy with other veterans, joining a symptom-focused therapy approach to deal for instance with ongoing symptoms of anxiety, joining a therapy approach to develop interpersonal skillsor access couples therapy with their spouses. Depending on the unique circumstances of each individual the therapist will help them make a plan to facilitate future and ongoing growth and healing.
Objectives
The aim of this pilot study is to determine the effectiveness of a newly developed psychotherapy IPCE model using Person-Centered and ExistentialTheory. The following research question will be answered: Will the newly developed treatment IPCE modelrender statistically significant differences in pre- and post-test results that would show it is potentially
effective in treating veterans with combat-related PTSD?
Method
Procedure
One male veteran who has been previously diagnosed with PTSD at the VA and awarded a 100% service connected rating for PTSD has been selected to participate in the pilot study. Prior to participating in the newly developed psychotherapy model, the veteran completed three psychometric pre-tests, two measuring PTSD symptoms and one measuring purpose in life including: the PTSD Checklist (PCL-5) for American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) [19,20];Purpose in Life Test (PIL) [21]; and the Mississippi Scale for Combat-Related PTSD (M-PTSD) [22]. Following completion of the therapy, which consisted of 10-20 therapy sessions of 1 hour each once per week, the veteran completed the same three post-tests. Results from the pre- and post-tests were then statistically analyzed to determine possible significance using the Statistical Package for the Social Sciences (SPSS) using paired t-Tests [23]. Design
This type of research design using one subject with measure prior and after anintervention is called a one-group pretest-posttest design. The one-group pretest-posttest design involves collecting information on the status of subjects prior to and following implementation of an intervention such as psychotherapy treatment. This involves pre-testing (e.g., symptoms) and subsequent measurement (post-testing) of the variables of interest after implementation.
Testing
Scale for Combat-Related PTSD (M-PTSD) and also correlates moderately with level of combat exposure with correlations reported as 0.929 and diagnostic efficiency was 0.900 [20]. Examination of the individual items showed wide ranging values of individual item correlations ranging from 0.386 to 0.788, and with diagnostic efficiencies of 0.700 or better for symptoms [24].
(2) Mississippi Scale for Combat-Related PTSD (M-PTSD): The M-PTSDis a 35-item self-report measure that assesses combat-related PTSD in veteran populations. Items sample DSM-5 symptoms of PTSD and frequently observed associated features (substance abuse, suicidality, and depression). Respondents are asked to rate how they feel about each item using 5-point, Likert-style response categories.
Ten positively framed items are reversed scored and then responses are summed to provide an index of PTSD symptom severity which can range from 35-175. Cutoff scores for a probable PTSD diagnosis have been validated for some populations, but may not generalize to other populations. In a study to validate the M-PTSD findings support the construct validity (sensitivity) of this scale in the immediate and longitudinal measurement of relatively non-pathological degrees of war-related stress in reservists not involved in direct fighting [19,22]. Initial level of PTSD symptomatology upon returning from a war zone was predictive of M-PTSD-DS scores 3 years later. This scale was shown effective in detecting varying degrees of war-related stress in this self-selected group of reservists [25].
(3) Purpose in Life Test (PIL): Meaning in life has been a popular topic of philosophy and study, and the perceived presence of meaning in one's life has been associated with many positive psychological variables (e.g., life satisfaction), while the perceived absence of meaning has been associated
with negative variables (e.g., depression). The Purpose in Life test (PIL) was developed in order to assess the amount of perceived meaning in a person's life. The Purpose in Life (PIL) test is the earliest and most widely studied of the well-known Logo therapy psychometric instruments and is the primary Logo therapy measure of the degree to which an individual experiences a sense of personal life meaning [6, 7]. The PIL has been psychometrically reviewed in a number of sources [26, 27-32]. With regard to validity, the PIL, as is expected, correlates positively with constructs such as happiness, emotional stability, and extroversion, and negatively with constructs such as boredom proneness, anxiety, and depression [29, 30, 32, 33, 34, 35]. Such correlations are consistent with Logo therapy conceptualizations and research studies that demonstrate the relationship between meaning and well-being [30, 32, 36].
Results
The Results for PTSD Checklist (PCL-5) The results for the PTSD Checklist (PCL-5) indicate that the mean value of the PCL-5pretest and PCL-5posttest for 20 questions is 3.60 and 1.95 respectively at a standard deviation of 0.681 and 1.191 respectively. The correlation between the variables are 0.419 at the significance level of 0.059 (which is greater than 0.05). So there is no significant correlation between PCL pre-test and PCL post-test. However, the t-Test value is 6.773 at the significance level of 0.000 (which is less than 0.05). So there is a statistically significant difference between the PCL pre-test and PCL post-test (at the significance level 0.05). The researcher concludes, on the basis of the results, that there is a statistically significant reduction in symptoms of PTSD and it can be concluded that this reduction is due to the effect of the treatment program (see Table 1 to 3).
Table 1: The results for PTSD checklist (PCL-5)
Paired Samples Statistics
Mean N Std. Deviation Std. Error Mean
Pair 1 PCL Posttest PCL Pretest 3.60 1.95 20 20 1.191 .681 .152 .266
Table 2: Paired samples correlations
N Correlation Sig.
Table 3: Paired samples test
Paired Samples Test
Paired Differences T df Sig.
(2-tailed)
Mean Std.
Deviation Std. Error Mean 95% Confidence Interval of the Difference
Lower Upper
Pair 1 PCL Pretest – PCL Posttest 1.650 1.089 .244 1.140 2.160 6.773 19 .000
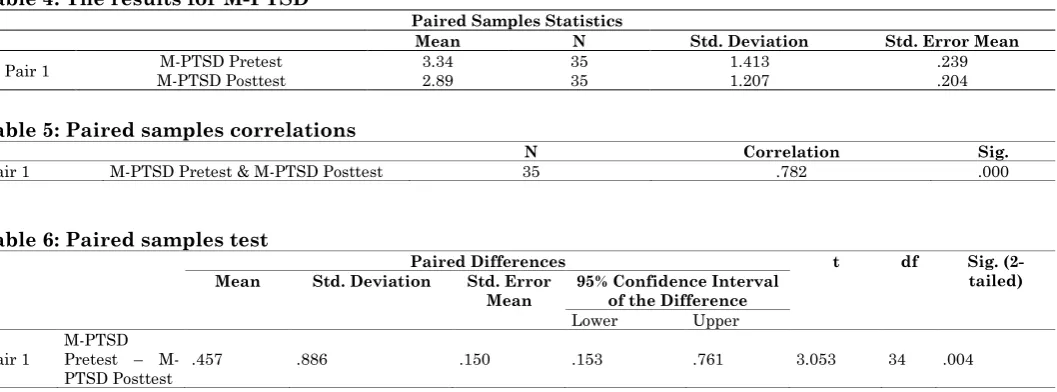
The Results for M-PTSD
The results for Mississippi Scale for Combat-Related PTSD (M-PTSD) indicate that the mean values of the M-PTSD pre-test and M-PTSD post-test for 35 questions are 3.34 and 2.89 respectively at a standard deviation of 1.413 and 1.207 respectively. The correlation between the variables is 0.782 at the significance level of 0.000 (which is less than 0.05). So there is significant correlation between M-PTSD pre-test and M-
PTSD post-test. The t-Test value is 3.053 at the significance level of 0.004 (which is less than 0.05) indicating a statistically significant difference between the M-PTSD pre-test and M-PTSD post-test (at the significance level 0.05). It can therefore be concluded that the reduction in PTSD symptomatology as measured by the M-PTSD is not due to chance but due to the effects of the therapeutic intervention (see Table 4 to 6).
Table 4: The results for M-PTSD
Paired Samples Statistics
Mean N Std. Deviation Std. Error Mean
Pair 1 M-PTSD Pretest 3.34 35 1.413 .239
M-PTSD Posttest 2.89 35 1.207 .204
Table 5: Paired samples correlations
N Correlation Sig.
Pair 1 M-PTSD Pretest & M-PTSD Posttest 35 .782 .000
Table 6: Paired samples test
Paired Differences t df Sig.
(2-tailed)
Mean Std. Deviation Std. Error
Mean
95% Confidence Interval of the Difference
Lower Upper
Pair 1
M-PTSD Pretest –
M-PTSD Posttest .457 .886 .150 .153 .761 3.053 34 .004
The Results for Purpose in Life Test (PIL)
The results for Purpose in Life Test (PIL) indicate that the mean values of PIL pre-test and PIL post-test for 20 questions are 2.35 and 3.70 respectively at a standard deviation of 0.813 and 0.657 respectively. The correlation between the variables are 0.306 at the significance level of 0.190 (which is greater than 0.05). So there is no significant correlation between PIL pre-test and PIL post-test. The t-Test value is 6.899 at the
significance level of 0.000 (which is less than 0.05) and therefore there is a statistically significant difference between the PIL pre-test and PIL post-test (at the significance level 0.05). Therefore a significant increase is noted in the perceived meaning reported by the subject, which is due to the effect of the treatment program and not to chance (see Table t to 9].
Table 7: The results for purpose in life test (PIL)
Paired Samples Statistics
Mean N Std. Deviation Std. Error Mean
Pair 1 PIL Pretest 2.35 20 .813 .182
PIL Posttest 3.70 20 .657 .147
Table 8: Paired samples correlations
N Correlation Sig.
Table 9: Paired samples test
Paired Differences T df Sig.
(2-tailed)
Mean Std.
Deviation Std. Error Mean 95% Confidence Interval of the Difference
Lower Upper
Pair 1 PIL Pretest – PIL Posttest -1.350 .875 .196 -1.760 -.940 -6.899 19 .000
Discussion
This study started with the research question: Will the newly developed treatment model render statistically significant differences at the significance level 0.05 in pre- and post-test results that would show it is potentially effective in treating veterans with combat-related PTSD? The conclusion is that the newly developed integrated Person-Centered and Existential treatment model for use with combat veterans with PTSD has proven effective in a one subject one-group pretest-posttest design based on the statistical analysis of the pre- and post-test data.
The three instruments used, the PTSD Checklist (PCL-5), Purpose in Life Test (PIL), and the Mississippi Scale for Combat-Related PTSD (M-PTSD) rendered statistically significant data indicating that the change in the pre-test and post-test data was not due to chance, but as a result of the effect of the therapeutic intervention utilized in this study as indicated in Tables 1-3. The results of the PCL and the M-PTSD indicate that PTSD symptoms as measured by these reliable and valid instruments significantly decreased after the therapeutic intervention. These two testing instruments are frequently used by other evidence-based treatment modalities such as cognitive behavioral therapy and exposure therapy to determine effectiveness. The fact that the newly developed Experiential and Existential treatment model rendered statistically significant results of change using the same instruments confirms that it has promise for future inclusion as an evidence-based treatment in future.
The results of the pre-test and post-test data of the PIL indicate that the subject’s perception of purpose and meaning in life increased significantly at the significance level 0.05 after the intervention. This instrument is frequently used by Existential therapists and meaning centered approaches to measure the change in meaning among clients. The fact that the newly developed therapeutic IPCE approach rendered statistically significant results using the PIL shows that it has promise in effecting existential issues, such as meaning and purpose in life.
Limitations
This is a pilot study and a first attempt to systematically evaluate the effectiveness of the newly developed treatment IPCE model and this can be seen as strength. Problematic is that the type of design using one subject called a one-group pretest-posttest design has limitations. Although this design provides a significant improvement over the one-shot study measuring only post-test results the design suffers from weaknesses because it cannot allow the researcher to rule out the possibility that some alternate factor (besides the treatment) or extraneous variable has contributed to change. Another limitation is that the study could not be designed as a true randomized control trial since no control group could be included and the subject was not randomly assigned to the treatment. Suggestions for Future Research
This issue of the one-group pretest-posttest design using only one subject could be addressed in future and the statistical data improved by including more subjects into future research projects using the newly developed treatment model. The issue of the lack of randomization can be addressed in future by including more subjects in future research studies and allow some to be randomly assigned to a no-treatment, waiting list control group and others to be randomly assigned to treatment. The researcher plans to expand the study in future and to include the above suggestions in order to determine if the effectiveness shown in this study cross over to larger samples.
Conclusion
subject. However, it does show that the newly
developed treatment model has promise for the future.
References
1. Marmar CR (2009) Mental health impact of Afghanistan and
Iraq deployment: Meeting the challenge of a new generation of veterans. Depression and Anxiety, 26:493-497.
2. Institute of Medicine (IOM) (2012) Treatment for posttraumatic
stress disorder in military and veteran populations: Initial assessment. Committee on the Assessment of Ongoing Effects in the Treatment of Posttraumatic Stress Disorder. Washington, DC: The National Academies Press. Study supported by the National Academy of Sciences and the Department of Defense.
3. Venter HJ (2014) Barriers to psychiatric care among military
and veteran populations in the US: The effect of stigma and prejudice on psychological and pharmacological treatment. International Journal of Advances in Psychology, 3(1):1-9.
4. Greening T Post-traumatic stress disorder: An existential
humanistic perspective. In Krippner, S. & Powers, S. M., editors (1997) Broken images, broken selves: Dissociative narratives in clinical practice.125‐135. New York: Brunner/Mazel.
5. Hoffman L, Vallejos L, Heatherlyn P, Cleare-Hoffman HP, Rubin
S (2015) Emotion, relationship, and meaning as core existential practice: Evidence-based foundations. Journal Contemp Psychotherapy, 45:11-20.
6. Vos J, Cooper M, Correria E, Craig M (2015). Existential
therapies: A review of their scientific foundations and efficacy. Existential Analysis, 26(1):49-69.
7. Vos J, Cooper M, Craig M (2014) Existential therapies: A
meta-analysis of their effects on psychological outcomes. Journal of Counseling and Clinical Psychology, 83(1):115-128.
8. Frankl VE (1946).Man’s search for meaning. Boston: Beacon
Press.
9. Frankl VE (1985) The unconscious god: Psychotherapy and
theology. New York: Simon & Schuster.
10.Frankl VE (2010) The Feeling of Meaninglessness: A challenge to
psychotherapy and philosophy. A. Battyany. Milwaukee, WI: Marquette University Press.
11.Joshi C, Marszalek JM, Berkel LA, Hisnhaw AB (2014) An
empirical investigation of Viktor Frankl’slogotherapeutic model. Journal of Humanistic Psychology, 54(2):227-253.
12.Mclean CP, Yeh R, Rosenfield D, Foa EB (2015) Changes in
negative cognitions mediate PTSD symptom reductions during client-centered therapy and prolonged exposure for adolescents. Behaviour Research and Therapy, 68:64-66.
13.Penadés R, Catalán R, Pujol N, Masana G, García-Rizo C,
Bernardo M (2012) The integration of cognitive remediation therapy into the whole psychosocial rehabilitation process: An evidence-based and person-centered approach. Rehabilitation Research and Practice. Volume 2012: Article ID 386895, 8.
14.Hoffman L (2009) Knowing and the unknown: An existential
epistemology in a postmodern context. Humana, Mente, 11: 97-110.
15.Rogers CR (1951) Client-centered therapy. New York, NY:
Houghton-Mifflin Company.
16.Rogers CR (1961) On becoming a person: a therapist’s view of psychotherapy. Boston, MA: Houghton-Mifflin Company.
17.Rogers CR (1980) A way of being. New York, NY:
Houghton-Mifflin Company.
18.Brown LS (2008) Feminist therapy as a meaning-making
practice: Where there is no power, where is the meaning? In K.J.
Schneider (Ed.), Existential-integrative psychotherapy:
Guidepost to the core of practice (pp. 130-140). New York: Routledge.
19.American Psychiatric Association (2013) Diagnostic and
statistical manual of mental disorders (5thed.). Arlington, VA:
American Psychiatric Association.
20.Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP,
Schnurr PP (2013). The PTSD checklist for DSM-5 (PCL-5).Scale available from the National Center for PTSD at www.ptsd.va.gov.
21.Crumbaugh JC, Maholick LT (1964) An experimental study in existentialism: The psychometric approach to Frankl’s concepts of noogenic neurosis. Journal of Clinical Psychology, 20:200-207.
22.Keane, T. M., Caddell, J. M., & Taylor, K. L. (1988). Mississippi Scale for combat-related Posttraumatic Stress Disorder: Three studies in reliability and validity.Journal of Consulting and Clinical Psychology, 56: 85-90.
23.IBM Corp. (Released 2013) IBM SPSS statistics for Windows,
Version 22.0. Armonk, NY: IBM Corp.
24.Blanchard E.B., Jones-Alexander J., Buckley .TC.,&Forneris, C.A. (1996). Psychometric properties of the PTSD checklist (PCL).Behaviour Research and Therapy. Aug; 34(8):669-73.
25.Sloan P, Arsenault L, Hilsenroth MJ (1998) A longitudinal
evaluation of the Mississippi Scale for combat-related PTSD in detecting war-related stress symptomatology. Journal Clinical Psychology, 54(8):1085-90).
26.Charlesworth G, Sadek S, Schepers A, Spector A (2015)
Cognitive behavior therapy for anxiety in people with dementia: A clinician guideline for a person-centered approach. Behavior Modification, 39(3):390-412.
27.Crumbaugh JC, Maholick LT (1969) Manual of instruction for the Purpose in Life test. Abilene, TX: V. Frankl Institute of Logotherapy.
28.Crumbaugh JC, Henrion R (1988) The PIL test: Administration,
interpretation, uses, theory and critique. The International Forum for Logotherapy, 11:76-88.
29.Hutzell RR (1987a) Purpose-in-life (PIL) test. In D. J. Keyser and
R. C. Sweetland (Eds.), Test critiques: VI: 437-446. Kansas City, MO: Test Corporation of America.
30.Hutzell, RR (1988) A review of the purpose in life test. The International forum for Logotherapy, 11:89-101.
31.Melton AMA, Schulenberg SE (2008) On the measurement of
meaning: Logotherapy’s empirical contributions of humanistic psychology. The Humanistic Psychologist, 36:1-14.
32.Reker GT (2000) Manual of the life attitude profile-revised. Peterborough, Ontario: Student Psychologists Pr
33.Schulenberg SE (2004) A psychometric investigation of
logtherapy measures and the outcome questionnaire (OQ-45.2). North American Journal of Psychology, 6:477-492.
34.Hutzell RR (1989) Life purpose questionnaire overview sheet. Berkeley, CA: Institute of Logotherapy Press.
35.Melton, A.M.A.,&Schulenberg, S.E. (2007). On the relationship between meaning in life and boredom proneness: Examining a logotherapy postulate. Psychological Reports, 101: 1016-1022.
36.Robak RW, Griffin PW (2000) Purpose in life: What is its