Somatosensory Evoked Potentials in Very Preterm Infants in Relation to
L
-Thyroxine Supplementation
Bert J. Smit, MD*; Joke H. Kok, MD, PhD*; Linda S. de Vries, MD, PhD‡; Aleid G. van Wassenaer, MD, PhD*; Friedo W. Dekker, MD, PhD§;
and Bram W. Ongerboer de Visser, MD, PhDi
ABSTRACT. Objective. To study the effect of L
-thy-roxine supplementation on neurologic maturation in very preterm infants with transient hypothyroxinemia.
Design. Randomized, double-blind,
placebo-con-trolled,L-thyroxine supplementation trial.
Setting. Level III neonatal intensive care unit.
Subjects. A total of 200 infants<30 weeks’ gestational age.
Intervention. Subjects were randomly assigned to re-ceive L-thyroxine (8 mg/kg birth weight per day) or a
placebo during the first 6 weeks of life.
Methods. Median nerve somatosensory evoked
po-tentials were recorded, measuring cortical N1 peak
la-tency at 2 weeks of age, at term, and at 6 months (correct-ed) age.
Results. Cortical N1 peak latency was not decreased
significantly in theL-thyroxine group compared with the
placebo group throughout the study period.
Conclusion. L-Thyroxine supplementation during the
first 6 weeks of life did not decrease cortical N1 peak
latency in infants of <30 weeks’ gestational age.
Pediatrics 1998;101:865– 869; electrophysiology, evoked potentials, hypothyroidism, hypothyroxinemia, preterm infant, somatosensory, thyroxine.
ABBREVIATIONS. SEP, somatosensory evoked potential; PMA, postmenstrual age; ms, millisecond.
T
hyroid hormones are essential for normal brain development.1A shortage of thyroid hormonesduring brain development, as in congenital hy-pothyroidism, can cause subsequent problems in motor and cognitive development.2,3Transient
hypo-thyroxinemia is common in preterm infants and has been associated with an increased risk of neurode-velopmental dysfunction.4 – 6 It is still unknown
whether transient hypothyroxinemia in preterm in-fants causes a shortage of thyroid hormone at the cellular level in the nervous system, as is the case in congenital hypothyroidism, and thus requiresl
-thy-roxine supplementation.7–9In patients with
congeni-tal hypothyroidism, a delay in neurologic maturation is determined by measurement of prolonged laten-cies in somatosensory evoked potentials (SEPs).10 –13
Likewise, in preterm infants with transient hypothy-roxinemia, recording SEPs could provide new in-sight into the effects of low plasma T4on neurologic
maturation at an early stage. We were the first to record SEPs in a randomized, double-blind, placebo-controlled trial of l-thyroxine supplementation in 200 infants of ,30 weeks’ gestational age.14 We
hy-pothesized that byl-thyroxine supplementation, cor-tical N1 peak latency in median nerve SEPs would
decrease.
PATIENTS AND METHODS
We enrolled 200 infants between January 1991 and July 1993. The patient size of 200 infants was based on the primary endpoint of developmental outcome at 24 months.14 The study was
ap-proved by the Research and Ethics Committee of the Academic Medical Center in Amsterdam, The Netherlands. Inclusion criteria were gestational age between 25 and 30 weeks and admission to our neonatal intensive care unit within the first 24 hours after birth. Exclusion criteria were severe congenital malformations, maternal endocrine disease, and maternal illicit drug dependency. After informed consent of at least one parent, the infants were randomly and blindly assigned to receive either l-thyroxine (8
mg/kg birth weight) or a placebo. Trial medication was adminis-tered 12 to 24 hours after birth once daily during the first 6 weeks of life, initially by intravenous injection as long as parenteral nutrition was given and orally thereafter. In a preliminary study, we found that with this dose, a physiologic replacement therapy is achieved.15
Measurement of SEPs
In each patient, SEPs were obtained at 2 weeks of age (14 to 17 days), at term age (37 to 43 weeks’ postmenstrual age [PMA]), and at 6 months (corrected) age (63 to 69 weeks’ PMA). PMA is defined as gestational age at birth plus postnatal age. Corrected age is defined as age corrected for preterm birth, ie, age from the ex-pected date of birth. SEPs were recorded with a mobile SEP recording machine (Neuropack Four Mini, model MEB-5304K, Nihon Kohden, Tokyo, Japan). Electrical pulses of 0.1 millisecond (ms) duration were delivered at a rate of 1 per 2 seconds. A hand-held device was placed on the ventral wrist overlying the median nerve. The intensity of stimulation used was that which was necessary to produce a minimal thumb twitch. The skin temperature was guaranteed.36.5°C. Recordings were obtained from the left somatosensory cortex after stimulation of the right median nerve.
In case of an infusion line in the right arm or unilateral brain lesions on the left side, recordings were obtained from the right somatosensory cortex, after stimulation of the left median nerve. Recording was performed with silver–silverchloride disk elec-trodes (diameter, 10 mm). The negative electrode was placed over the primary somatosensory area for the upper extremities (C39/ From the Departments of *Neonatology, §Clinical Epidemiology and
Bio-statistics, andiClinical Neurophysiology, Emma Children’s Hospital AMC, University of Amsterdam, Amsterdam, The Netherlands; and the ‡Depart-ment of Neonatology, Wilhelmina Children’s Hospital, University of Utrecht, Utrecht, The Netherlands.
Received for publication Jun 6, 1997; accepted Sep 9, 1997.
Reprint requests to (B.J.S.) Academic Medical Center, University of Amster-dam, Emma Children’s Hospital AMC, Department of Neonatology, H3N-148, Box 22700, 1100 DE Amsterdam, The Netherlands.
C49, ie, 2 cm posterior to C3/C4, according to the international 10-to 20-electrode system). The reference electrode was placed in the midfrontal position (Fz), and one electrode was placed on the lower arm as ground. The skin– electrode resistance was usually kept,2Vand never.5V. The analysis time was 200 ms. Thirty to 50 responses were averaged through a bandpass of 2 to 100 Hz. Each recording was duplicated to show reproducibility. After stimulation of the median nerve, the latency to the peak of the first negative wave (which signals the arrival of the afferent impulse at the cerebral cortex), recorded as cortical N1 peak latency, was
measured according to the criteria of Desmedt et al.16If a bilobed
N1-wave was present, the latency to the first prominent peak was
determined. All infants were tested without sedation. At 2 weeks of age, the infant’s behavioral state during recording was noted according to Prechtl.17At term and at 6 months (corrected) age, the
behavioral state was classified as awake or asleep. Furthermore, actual medication was recorded. Each SEP recording took about 45 minutes to complete. All potentials were stored on a disk. Later they were reassessed and classified for quality according to pre-defined criteria regarding configuration and reproducibility. If both configuration and reproducibility were good, the quality was considered good.
If the configuration was good, but lacked good reproducibility, ie, two cortical N1peak latencies with a difference of.10% of the
largest value, the quality was considered moderate. In cases of good or moderate quality, the mean value of the two cortical N1
peak latencies was used for the analysis.
If neither configuration nor reproducibility were good, the quality of the potentials was considered poor. Potentials of poor quality were excluded from statistical analysis.
Cranial Ultrasonography
We performed sequential cranial ultrasonography of all infants using a mechanical sector scanner (ATL Ultramark 4) with a 7.5-MHz transducer. Ultrasonography was performed before trial medication commenced and on days 5, 14, 28, and 42, or more often if clinically indicated. We classified hemorrhage according to Volpe,18and periventricular leucomalacia according to De Vries et
al.19Unilateral hemorrhagic parenchymal involvement evolving in
porencephalic cysts were classified as parenchymal hemorrhages. For the classification of ventriculomegaly, we followed Levene.20
Statistical Analysis
Categorical data were analyzed using thex2test for two and
multiway tables (BMDP 4F, BMDP Statistical Software, Inc, Los Angeles, CA). Continuous data were analyzed using the student’s ttest (BMDP 3D). Linear regression analysis (BMDP 1R) was used to study the relationship between l-thyroxine supplementation and cortical N1peak latency at three time points. Possible
con-founding factors included in the linear regression analysis were infants’ sex, weight class for gestational age,21ethnic origin of the
mother, antenatal steroids, asphyxia, cranial ultrasound findings (before trial medication), behavioral state, and PMA. Interaction analysis was performed on every confounding factor with l -thyroxine supplementation. The distribution of residuals was checked for skewness. If appropriate, logarithmic transformation was applied.
RESULTS Patient Population
We enrolled 100 infants each in the l-thyroxine group and the placebo group. Seven infants were withdrawn from the study; 4 because of severe con-genital malformations diagnosed after study entry and 3 because of parental discomfort about the study.14The data collected from these patients were
not excluded from the statistical analysis. On the three consecutive SEP recordings (14 to 17 days after birth, and 37 to 43 weeks’ and 63 to 69 weeks’ PMA) the initial group of 200 infants was reduced by mor-talities (n529, 33, 35, respectively) and poor clinical condition (n5 8, 4, 2, respectively), or for practical reasons (n513, 29, 56, respectively). The main
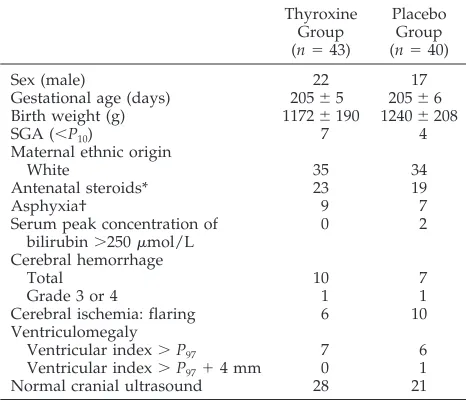
prac-tical reason at 37 to 43 and 63 to 69 weeks’ PMA was parental discomfort with the time-consuming aspect of the SEP recording. We could only obtain record-able SEPs from a few infants of ,30 weeks’ PMA. Therefore, at 2 weeks of age, data of infants ,30 weeks’ PMA (n567) were excluded. At the first SEP recording (14 to 17 days after birth), thel-thyroxine group and the placebo group were comparable with respect to baseline characteristics (Table 1). This was the case for all three time points.
SEPs
Only SEP recordings of good or moderate quality were analyzed. Causes for a poor quality included unstable clinical condition and local factors as edema, especially during intensive care. Data reduc-tion amounted to 40% (n533) at 2 weeks of age, 7% (n 5 9) at term age, and 5% (n 5 5) at 6 months’ (corrected) age.
After this data reduction, the number of SEP re-cordings and the baseline characteristics of corre-sponding patients remained comparable in the
l-thyroxine group and the placebo group at the three time points.
Cortical N1Peak Latency in Relation toL-Thyroxine
Supplementation
For N1latency at 2 weeks of age (14 to 17 days; 30
to 32 weeks’ PMA), at term age (37 to 43 weeks’ PMA), and at 6 months (corrected) age (63 to 69 weeks’ PMA), we found no statistically significant difference between the l-thyroxine group and the placebo group (Table 2).
Cortical N1Peak Latency in Relation toL-thyroxine
Supplementation and PMA
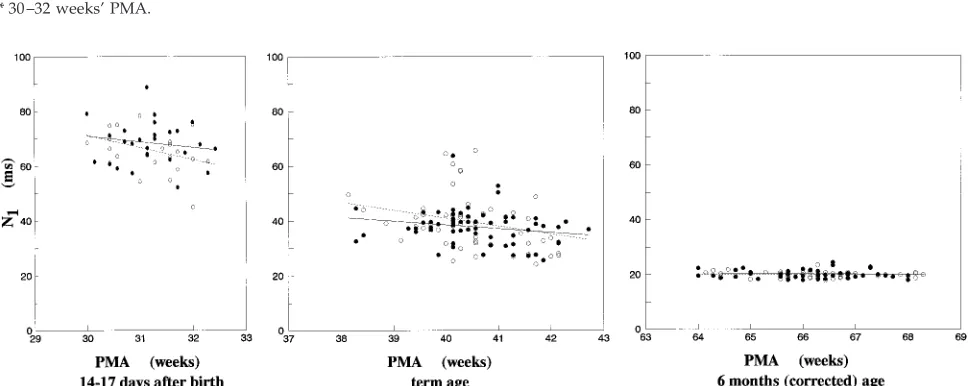
The Figure shows N1latency in relation to PMA at
time of SEP recording in both the l-thyroxine and placebo groups at three time points. N1 latency
de-TABLE 1. Baseline Characteristics at First SEP Measurement 14 –17 Days After Birth
Thyroxine Group (n543)
Placebo Group (n540)
Sex (male) 22 17
Gestational age (days) 20565 20566 Birth weight (g) 11726190 12406208
SGA (,P10) 7 4
Maternal ethnic origin
White 35 34
Antenatal steroids* 23 19
Asphyxia† 9 7
Serum peak concentration of bilirubin.250mmol/L
0 2
Cerebral hemorrhage
Total 10 7
Grade 3 or 4 1 1
Cerebral ischemia: flaring 6 10
Ventriculomegaly
Ventricular index.P97 7 6
Ventricular index.P9714 mm 0 1
Normal cranial ultrasound 28 21
creased with the increment of PMA from a mean value of 67 ms at 2 weeks of age to 38 ms at term age and 20 ms at 6 months’ (corrected) age. No signifi-cant effect of l-thyroxine supplementation was found at any of the three time points (Figure).
Cortical N1Peak Latency in Relation toL-Thyroxine
Supplementation, PMA, and Possible Confounding Factors
After adjusting for possible confounding factors, linear regression analysis gave no additional support for an effect of l-thyroxine supplementation on N1
latency at any of the three time points (Table 2). We found no significant interactions between possible confounding factors and l-thyroxine supplementa-tion. We discarded hyperbilirubinemia as a con-founding factor. There was no correlation between the serum peak concentration of bilirubin and N1
latency at 2 weeks of age, nor did inclusion or exclu-sion of the patients with a serum peak concentration .250 mmol/L (n 5 2, both in the placebo group) change the results of the analyses. Actual medication also was discarded as confounding factor, because in this respect thel-thyroxine and placebo groups were completely similar. We treated all patients with caf-feine at the age of 2 weeks. Throughout the study, no SEP recordings were made during anticonvulsive therapy. Cranial ultrasound findings (before trial medication) were used as confounding factors. How-ever, we did diagnose more hemorrhages (grade 3 or 4:n59), periventricular leucomalacia (grade 2 or 3: n 5 3), and ventriculomegaly (ventricular index .P97:n5 3) later on in the neonatal period. If
ultra-sound findings present at 2 weeks of age or the final
summary of ultrasound findings on day 42 were used in the respective analyses, the results remained unchanged. Also, including or excluding behavioral state as a confounding factor, which could be related tol-thyroxine supplementation, had no effect on the results. Finally, logarithmic transformation was ap-plied because of a moderate skewness and different variances of N1latency at the three time points. This
had no effect on the results.
Subgroup Analysis in SEP Recordings With Good Quality
If we also excluded SEP recordings of moderate quality, a subgroup analysis of the remaining good-quality SEPs revealed a prolonged N1latency in the l-thyroxine group (69.365.0 ms;n512) at 2 weeks of age, compared with the placebo group (63.265.0 ms; n 5 9. Difference between means, adjusted for covariates: 4.6 ms; 95% confidence interval: 0.1–9.2). At term age, N1latency was similar in thel
-thyrox-ine group (37.8 6 6.6 ms; n 5 56) and the placebo group (37.668.4 ms;n544). This also was the case at 6 months’ (corrected) age (20.061.3 ms;n549 vs 20.06 1.1 ms;n5 48).
DISCUSSION
This study demonstrated thatl-thyroxine supple-mentation during the first 6 weeks of life did not decrease cortical N1peak latency in infants of ,30
weeks’ gestational age.
This finding can be explained by the transient and, for some infants, mild character of the hypothyrox-inemia. Moreover, transient hypothyroxinemia does not necessarily cause hypothyroidism at the cellular
TABLE 2. Cortical N1Peak Latency (ms) in Median Nerve SEP in Relation tol-Thyroxine Supplementation
Univariate Analysis Adjusted for
Covariates
l-Thyroxine Group Placebo Group D D 95% CI
14–17 days after birth* 68.367.8 (n527) 66.168.5 (n523) 12.2 11.0 23.925.8 37–43 weeks’ PMA 37.566.4 (n567) 38.869.7 (n558) 21.3 21.0 23.621.7 63–69 weeks’ PMA 20.161.5 (n552) 20.161.1 (n550) 0 20.1 20.620.4
Values are mean6SD;Dl-thyroxine2placebo. * 30 –32 weeks’ PMA.
Figure. Relation between cortical N1peak latency in SEPs and PMA at three time points. Solid circles indicatel-thyroxine group; open
level of the nervous system. Intracellular mecha-nisms such as elevated type II deiodinase activity and increased binding capacity of T3receptors may
protect the cell from hypothyroidism.22,23Our finding
can be regarded as being in agreement with the finding of Van Wassenaer et al thatl-thyroxine sup-plementation does not improve neurologic develop-ment at the age of 2 years.14
If, at 2 weeks of age, only SEPs with good config-uration and reproducibility were analyzed, we found a prolonged N1 latency in the l-thyroxine group
compared with the placebo group. At 2 weeks of age, only data of infants of.30 weeks’ PMA were used for the analysis. Consequently, these infants were .28 weeks’ gestational age. This is of special interest in relation to the finding of Van Wassenaer et al: in infants of .27 weeks’ gestation, the mental– devel-opmental score of the l-thyroxine group is lower than that of the placebo group.14 If the result of our
subgroup analysis (only good-quality SEPs) is re-garded as more reliable than that of the general analysis, then this could support the hypothesis that
l-thyroxine supplementation in infants of .27 weeks’ gestation may be harmful.
First, the dose ofl-thyroxine could have been too high for some infants, resulting in intracellular hy-perthyroidism.
Second,l-thyroxine supplementation may lead to elevated type III deiodinase activity24 and
subse-quent conversion of T4 to reverse T3 (a nonactive
metabolite of T4) instead of T3, which results in an
inadvertent decrease of intracellular T3. Both
hyper-thyroidism and hypohyper-thyroidism may interfere with synaptogenesis.25
It is important to note that abnormal latencies in median nerve SEPs, established in patients with con-genital hypothyroidism,10 –13 are much more striking
than our current findings in very preterm infants with transient hypothyroxinemia. In congenital hy-pothyroidism, especially in patients with a total de-ficient thyroxine production despite early initiation of l-thyroxine therapy, the extent and duration of decreased thyroxine levels are generally more seri-ous than in transient hypothyroxinemia in preterm infants. In this study at 2 weeks after birth, plasma thyroxine levels in the placebo group andl -thyrox-ine group were 89.8632.3 pmol/L and 121.5629.3 pmol/L, respectively.14Furthermore, synaptogenesis
and myelinization within the central nervous system progress most rapidly near term and after term age, respectively.26 This could explain the difference in
impact of decreased plasma (free) thyroxine levels between term and preterm infants. It is of interest that also in patients with primary congenital hypo-thyroidism, overtreatment, like initial undertreat-ment, may lead to delayed maturation of the SEP and seems to be harmful.13
Median nerve SEPs have been studied extensively during the neonatal period.27–38The short-latency N
1
component, regarded to reflect the maturation of the nervous system, can be affected by many factors. As described in the literature, these include behavioral state,30 medication,31 cranial ultrasound
abnormali-ties,32–34hyperbilirubinemia,35low birth weight,36
ad-aptation to extrauterine life,37and prenatal exposure
to betamethasone/thyrotropin-releasing factor.38
Our study is the first randomized controlled trial in which cortical N1 peak latency of median nerve
SEP was measured in a large group of very preterm infants and analyzed all these factors as well. N1
latency values at 2 weeks of age (30 to 32 weeks’ PMA) and at term age were in agreement with those given in the literature.27,28 At 6 months’ (corrected)
age, N1latency reached a mean value of 20.1 ms. The
slight variance and stability of N1 latency with
in-creasing age suggest full maturation of the somato-sensory nervous pathway by the age of 6 months.
We considered the effect of methodologic errors or selection bias. Measuring N1latency of median nerve
SEP in very preterm infants has its limitations owing to unstable clinical condition and adverse circum-stances. Therefore, we excluded SEP recordings of poor quality. Data reduction was the same in both study groups. A larger study group would have decreased the width of confidence intervals, result-ing in a more precise estimation of latencies. How-ever, this would not have lead to other conclusions. Recently, we reported that l-thyroxine supple-mentation during the first 6 weeks of life does not increase motor nerve conduction velocity in the ul-nar and posterior tibial nerve in infants of ,30 weeks’ gestational age.39 In the present study, we
demonstrated thatl-thyroxine supplementation did not cause cortical N1 peak latency of median nerve
SEP to decrease. In both studies, maturational pro-cesses such as myelinization and synaptogenesis are not accelerated by l-thyroxine supplementation. Both neurophysiologic studies gave us the opportu-nity to assess the functional impact of l-thyroxine supplementation on the developing nervous system of very preterm infants with transient hypothyrox-inemia. More studies are needed to unravel the miss-ing link between transient hypothyroxinemia and subsequent neurodevelopmental dysfunction.
CONCLUSION
l-Thyroxine supplementation during the first 6 weeks of life did not decrease cortical N1 peak
la-tency in infants of,30 weeks’ gestational age.
ACKNOWLEDGMENTS
This work was supported by the Praeventiefonds, the Hague (grant 28-2051), The Netherlands.
We would like to thank the participating children and their parents and the medical and nursing staff of our neonatal depart-ment for their cooperation. We are grateful to A. A. Boode, Dr T. Brantsma-van Wulfften Palthe, G. J. van Bruggen, Ir A. A. M. Hart, Dr Ir F. H. C. de Jongh, Dr F. E. P. Meyjes, and Prof Dr J. J. M. de Vijlder for their enthusiastic support.
REFERENCES
1. Timiras PS, Nzekwe EU. Thyroid hormones and nervous system devel-opment.Biol Neonate.1989;55:376 –385
2. Kooistra L, Laane C, Vulsma T, Schellekens JMH, Van Der Meere JJ, Kalverboer AF. Motor and cognitive development in children with congenital hypothyroidism: a long-term evaluation of the effects of neonatal treatment.J Pediatr.1994;124:903–909
3. Simons WF, Fuggle PW, Grant DB, Smith I. Intellectual development at 10 years in early treated congenital hypothyroidism.Arch Dis Child.
1994;71:232–234
Tran-sient hypothyroxinaemia associated with developmental delay in very preterm infants.Arch Dis Child.1992;67:944 –947
5. Den Ouden AL, Kok JH, Verkerk PH, Brand R, Verloove-Vanhorick SP. The relation between neonatal thyroxine levels and neurodevelopmen-tal outcome at age 5 and 9 years in a national cohort of very preterm and/or very low birth weight infants.Pediatr Res.1996;39:142–145 6. Reuss ML, Paneth N, Pinto-Martin JA, Lorenz JM, Susser M. The
rela-tion of transient hypothyroxinemia in preterm infants to neurologic development at two years of age.N Engl J Med.1996;334:821– 827 7. Lucas A, Morley R, Fewtrell MS. Low triiodothyronine concentrations
in preterm infants and subsequent intelligence quotient (IQ) at 8 years follow up.Br Med J,1996;312:1132–1133
8. Brook CGD. Do preterm infants need thyroxine replacement?Br Med J.
1996;312:1133–1134. Commentary
9. Vulsma T, Kok JH. Prematurity-associated neurologic and developmen-tal abnormalities and neonadevelopmen-tal thyroid functions.N Engl J Med.1996; 334:857– 858
10. Laureau E, Vanasse M, Hebert R, et al. Somatosensory evoked poten-tials and auditory brain-stem responses in congenital hypothyroidism. I. A longitudinal study before and after treatment in six infants detected in the neonatal period. Electroencephalogr Clin Neurophysiol. 1986;64: 501–510
11. Norcross-Nechay K, Richards GE, Cavallo A. Evoked potentials show early and delayed abnormalities in children with congenital hypothy-roidism.Neuropediatrics.1989;20:158 –163
12. Bongers-Schokking CT, Colon EJ, Hoogland RA, De Groot CJ, Van Den Brande JL. Somatosensory evoked potentials in neonates with primary congenital hypothyroidism during the first week of therapy.Pediatr Res.
1991;30:34 –39
13. Bongers-Schokking CT, Colon EJ, Mulder PGH, Hoogland RA, De Groot CJ, Van Den Brande JL. Influence of treatment on the maturation of the somesthetic pathway in infants with primary congenital hypo-thyroidism during the first year of life.Pediatr Res.1993;34:73–78 14. Van Wassenaer AG, Kok JH, De Vijlder JJM, et al. Effects of thyroxine
supplementation on neurologic development in infants born at less than 30 weeks’ gestation.N Engl J Med.1997;336:21–26
15. Van Wassenaer AG, Kok JH, Endert E, Vulsma T, De Vijlder JJM. Thyroxine administration to infants of less than 30 weeks’ gestational age does not increase plasma triiodothyronine concentrations.Acta Endocrinol.1993;129:139 –146
16. Desmedt JE, Brunko E, Debecker J. Maturation of the somatosensory evoked potentials in normal infants and children with special reference to the early N1component.Electroencephalogr Clin Neurophysiol.1976;40:
43–58
17. Prechtl HFR. The behavioural states of the newborn infant (a review).
Brain Res.1974;76:185–212
18. Volpe JJ.Neurology of the Newborn. 2nd ed. Philadelphia, PA: WB Saun-ders Company; 1987:331
19. De Vries LS, Eken P, Dubowitz LMS. The spectrum of leucomalacia using cranial ultrasound.Behav Brain Res.1992;49:1– 6
20. Levene MI. Measurement of the growth of the lateral ventricles in preterm infants with real-time ultrasound.Arch Dis Child. 1981;56: 900 –904
21. Kloosterman GJ. On intrauterine growth.Int J Gynaecol Obstet.1970;8: 895–912
22. Silva JE, Matthews PS. Production rates and turnover of triiodothyro-nine in rat developing cerebral cortex and cerebellum. Responses to hypothyroidism.J Clin Invest.1984;74:1035–1049
23. Bellabarda D, Fortier S, Belisle S, Lehoux JG. Triiodothyronine nuclear receptors in liver, brain and lung of neonatal rats. Effect of hypothy-roidism and thyroid replacement therapy.Biol Neonate.1984;45:41– 48 24. Fisher DA, Polk DH, WU SY. Fetal thyroid metabolism: a plaralistic
system.Thyroid.1994;4:367–371
25. Nicholson JL, Altman J. Synaptogenesis in the rat cerebellum: effects of early hypo- and hyperthyroidism.Science.1972;176:530 –532
26. Volpe JJ. Neuronal proliferation, migration, organization, and myelin-ization. In:Neurology of the Newborn. 3rd ed. Philadelphia, PA: WB Saunders Company; 1995:43–92
27. Klimach VJ, Cooke RWI. Maturation of the neonatal somatosensory evoked response in preterm infants.Dev Med Child Neurol.1988;30: 208 –214
28. Taylor MJ, Boor R, Ekert PG. Preterm maturation of the somatosensory evoked potential.Electroencephalogr Clin Neurophysiol.1996;100:448 – 452 29. Bongers-Schokking CJ, Colon EJ, Hoogland RA, Van Den Brande JL, De Groot CJ. The somatosensory evoked potentials of normal infants: in-fluence of filter bandpass, arousal state and number of stimuli.Brain Dev.1989;11:33–39
30. Desmedt JE, Manil J. Somatosensory evoked potentials of the normal human neonate in REM sleep, in slow wave sleep and in waking.
Electroencephalogr Clin Neurophysiol.1970;29:113–126
31. Saletu B. Cerebral evoked potentials in psychopharmacology. In: Desmedt JE, ed.Auditory Evoked Potentials in Man. Psychopharmacology Correlates of Evoked Potentials. Basel, Switzerland: S Karger; 1977:175–207 32. Willis J, Duncan MC, Bell R, Pappas F, Moniz M. Somatosensory evoked potentials predict neuromotor outcome after periventricular hemor-rhage.Dev Med Child Neurol.1989;31:435– 439
33. De Vries LS, Pierrat V, Minami T, Smet M, Casaer P. The role of short latency somatosensory evoked responses in infants with rapidly pro-gressive ventricular dilatation.Neuropediatrics.1990;21:136 –139 34. Pierrat V, Eken P, Duquennoy C, Rousseau S, De Vries LS. Prognostic
value of early somatosensory evoked potentials in neonates with cystic leukomalacia.Dev Med Child Neurol.1993;35:683– 690
35. Bongers-Schokking CT, Colon EJ, Hoogland RA, Van Den Brande JL, De Groot CJ. Somatosensory evoked potentials in neonatal jaundice.Acta Paediatr Scand.1990;79:149 –155
36. Pierrat V, Eken P, Truffert P, Duquennoy C, De Vries LS. Somatosen-sory evoked potentials in preterm infants with intrauterine growth retardation.Early Hum Dev.1996;44:17–25
37. Pierrat V, De Vries LS, Minami T, Casaer P. Somatosensory evoked potentials and adaptation to extrauterine life: a longitudinal study.
Brain Dev.1990;12:376 –379
38. De Zegher F, De Vries LS, Pierrat P, et al. Effect of prenatal betamethasone/thyrotropin releasing hormone treatment on somato-sensory evoked potentials in preterm newborns.Pediatr Res.1992;32: 212–214
DOI: 10.1542/peds.101.5.865
1998;101;865
Pediatrics
Dekker and Bram W. Ongerboer de Visser
Bert J. Smit, Joke H. Kok, Linda S. de Vries, Aleid G. van Wassenaer, Friedo W.
l-Thyroxine Supplementation
Somatosensory Evoked Potentials in Very Preterm Infants in Relation to
Services
Updated Information &
http://pediatrics.aappublications.org/content/101/5/865
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/101/5/865#BIBL
This article cites 35 articles, 6 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/neonatology_sub
Neonatology
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
http://www.aappublications.org/cgi/collection/endocrinology_sub
Endocrinology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.101.5.865
1998;101;865
Pediatrics
Dekker and Bram W. Ongerboer de Visser
Bert J. Smit, Joke H. Kok, Linda S. de Vries, Aleid G. van Wassenaer, Friedo W.
l-Thyroxine Supplementation
Somatosensory Evoked Potentials in Very Preterm Infants in Relation to
http://pediatrics.aappublications.org/content/101/5/865
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.