I read with great interest the article by Bhandari et al,1who discuss the
feasibility of nasal intermittent positive pressure ventilation (NIPPV) to support premature infants. Their article brings forward a modality for respiratory support of premature infants that is less invasive than mechanical ventilation (MV). Although it is important to demonstrate that the avoidance of intubation and the use of NIPPV can result in less morbidity, it is important to recognize that avoidance of unneeded intermittent ventilation, whether via nasal prongs or an endotracheal tube, could be more beneficial. The use of NIPPV can be used as a second line of support to premature infants who do not respond pos-itively to less-invasive treatments.
Years ago, MV was used as the first-line, and maybe the only available, option for respiratory support of premature infants with hyaline mem-brane disease.2 Although MV has been widely used, research has
shown a clear association between MV and lung injury, also known as ventilator-induced lung injury (VILI). Two major components account for lung injury in ventilated infants: tracheal intubation and the me-chanical force on the lung during ventilation.
Tracheal intubation is a traumatic and painful procedure that a pre-mature infant can experience during his or her hospital stay. It is often performed without adequate pain management3and may be
accompa-nied by significant hemodynamic instabilities.4Once the tube is in the
trachea, it inevitably serves as a bridge between the sterile lower respiratory system of the infant and the nonsterile outside world. We recently demonstrated that within a few days, colonization of the tra-chea with bacteria occurs in⬎80% of intubated infants.5These
bacte-ria will ignite the inflammatory process, which can lead to lung injury and bronchopulmonary dysplasia.6In addition, the ciliary movement of
the cells lining the trachea is now compromised and cannot clear the mucus because of the mechanical obstruction by the tube. Secretions will accumulate in the dependent part of the lungs, causing alveoli in these areas to become full of secretions without any aeration, whereas other areas become overinflated from the increased tidal volume that they receive. Added to these drawbacks is the high resistance to air flow via the endotracheal tube, which is narrower and longer than our natural airways. This increased resistance will result in increased work of breathing. This increased work is a major obstacle for ventila-tion, even in a healthy individual. I still remember Dr Theodore Kollobow at the National Institutes of Health, who used to “treat” his visitors by offering them an endotracheal tube to place in their mouth and breathe through. Everybody will get tachypnea, begin to sweat, and feel tired within minutes. This simple exercise demonstrates the impact of intubation on ventilation in a normal healthy adult lung. What will be the effect of this exercise on a newborn with immature lungs?
The mechanical force during ventilation produces VILI via 4 pathways: barotrauma, volutrauma, atelectrauma, and biotrauma.7Barotrauma
CONTRIBUTORS:Hany Aly, MD
Department of Newborn Services, George Washington University Hospital and Children’s National Medical Center, Washington, DC
ABBREVIATIONS
NIPPV—nasal intermittent positive pressure ventilation MV—mechanical ventilation
VILI—ventilator-induced lung injury CPAP— continuous positive airway pressure www.pediatrics.org/cgi/doi/10.1542/peds.2009-0256 doi:10.1542/peds.2009-0256
Accepted for publication Mar 30, 2009
Address correspondence to Hany Aly, MD, George Washington University Hospital, Department of Newborn Services, 900 23rd St NW, Suite G2092, Washington, DC 20037. E-mail: haly@mfa. gwu.edu
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2009 by the American Academy of Pediatrics
causes air leaks when ventilating with a relatively high positive pressure.8
Vo-lutrauma causes overdistention of the alveoli.9Atelectrauma can cause
atel-ectasis of the alveoli when using low pressure.10This type of injury can
re-sult from the repeated opening and closing of lung units. Biotrauma indi-cates a mechanotransduction or con-version of the physical force on the trachea and alveoli receptors into ac-tivation of the intracellular inflamma-tory pathway, leading to capillary leaks and increased lung fluids.11This
mech-anism is responsible for increased neutrophils, hydrogen peroxide, inter-leukins, tumor necrosis factor, throm-boxane B2, and the platelet-activating factor in tracheal aspirate after MV.12,13 Intubated animals supported
with continuous positive airway pres-sure (CPAP), instead of the intermit-tent pressure, have demonstrated a significantly reduced inflammatory response.12
Injury induced by MV does not stop at the lung; it has been shown to extend to dif-ferent body organs. Multisystem organ failure and death have been observed with MV.9,14 Different mechanisms can
explain the systemic damage caused by MV. It is recognized that inflammatory mediators produced from VILI can mi-grate easily via the bloodstream. The pul-monary vasculature is also a major res-ervoir for marginated neutrophils and can harbor almost one third of all neu-trophils outside the bone marrow. Fluc-tuation and redistribution of blood flow to different organs as a result of ventila-tor pressure on cardiac output is an-other contributing factor in systemic damage. Finally, the translocation of bac-teria from inside the alveolar space to systemic circulation can occur. This has been reproduced experimentally by us-ing high transpulmonary pressure and low expiratory pressure.14,15 In
prema-ture infants, there is a strong associa-tion between MV and brain injury. In a
recent cohort study that was conducted by the National Institute for Child Health and Development, it was recognized that, for extremely low birth weight infants, each 10 days of MV was associated with a 20% increased risk for cerebral palsy.16Such association remained
sig-nificant even after controlling for possi-ble confounding factors such as intra-ventricular hemorrhage, gestational age, and sepsis. Several mechanisms that can explain the association of cere-bral palsy and MV have been proposed (Table 1).17Because of this finding,
neo-natal units try to avoid combining tra-cheal intubation and MV and use nasal CPAP instead.
The use of nasal CPAP in premature in-fants prevents alveoli from collapsing and increases the functional residual ca-pacity. It also stents the airways, im-proves the compliance, and, therefore, reduces the efforts of breathing.18CPAP
conserves surfactant by avoiding the in-flammatory component of VILI and the accumulation of mucus when the tra-chea is intubated. Apart from these “acute” effects of CPAP, the extended use of CPAP is associated with stimulation of the lung units to grow.19This makes CPAP
both a corrective and supportive ther-apy. It allows premature lungs to grow while helping the process of gas ex-change. Multiple neonatal units that al-low extended use of CPAP have reported better outcomes and a reduced inci-dence of bronchopulmonary dyspla-sia20,21; whereas when CPAP was weaned
off prematurely and replaced with nasal cannula, the advantageous effects of CPAP were not appreciable.22Infants for
whom CPAP fails are exposed to intuba-tion and MV, but ventilaintuba-tion without tra-cheal intubation can be a less-invasive approach. This approach is known as na-sal NIPPV.
The concept of ventilation without intu-bation, NIPPV, has been practiced for a long time. Mouth-to-mouth resuscitation is actually a type of NIPPV. NIPPV’s major advantage is that it avoids tracheal intu-bation for infants who are not stable on CPAP or for whom CPAP is expected to fail. It has the flexibility of alternating the mode of support to and from CPAP with-out repeated extubation/intubation at-tempts. In this capacity, NIPPV avoids 1 of the 2 “bad” components of VILI. In addi-tion, the pressure delivered by NIPPV is limited by unavoidable air leakage at the interface between the device and the na-res, or via the oropharynx if the infant’s mouth is open, and downward into the esophagus. NIPPV, therefore, may modify or put a ceiling on ventilation pressures that reach the distal alveoli. Despite these advantages, it is still a mode of de-livering positive pressure ventilation. It is a less-invasive approach than classic ventilation, but it theoretically can have similar adverse effects.
We learned from the past that unnec-essary escalation of intervention im-poses more complications and, as a result, is associated with worse
out-TABLE 1 Proposed Mechanisms That Link MV With Cerebral Palsy and Other Neurodevelopmental Risks
1. Fluctuation of cerebral blood flow: MV is associated with a cascade of increased intrathoracic pressure, impedance of venous return and decreased cardiac preload, decreased cardiac output, and compromised cerebral perfusion
2. Fluctuation of the arterial carbon dioxide tension during ventilation 3. Exposure to sedative medications that are often used during MV 4. Systemic inflammation secondary to VILI
5. Other neurodevelopmental risks
a. Frequent sleep interruption and discomfort during tracheal suctioning, heel stick, and blood draws b. Exposure to noise related to ventilator alarms
c. Loss of self-regulatory behaviors that control stress and delayed oral readiness to feed d. Maternal deprivation resulting from physical limitation
COMMENTARY
PEDIATRICS Volume 124, Number 2, August 2009 787
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
comes during the care of premature infants.23 In addition to the effects
of intermittent pressure discussed, there are also the effects of other as-sociated practices. For example, to ad-just ventilator settings while on NIPPV, blood gases need to be monitored closely, often with the use of indwelling umbilical and arterial lines. These lines are a source for bloodstream in-fections and frequent blood sampling with subsequent transfusions. There-fore, NIPPV is an excellent option when
used in the capacity as a substitute for intubation and MV. However, when used in an infant who could be man-aged adequately by a less-invasive method such as CPAP, it is an unneces-sary escalation of care.
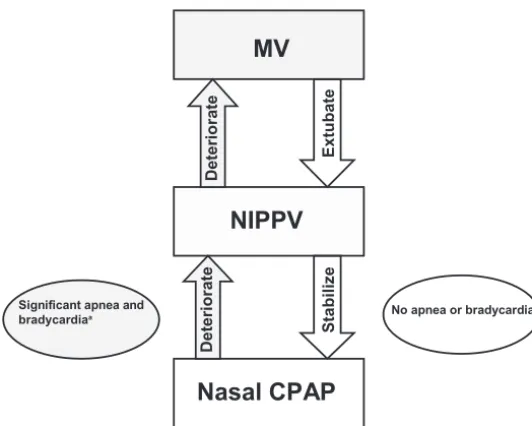
To date, there is no physiologic reason to support the use of NIPPV in infants who can otherwise be managed with CPAP. Instead, I advocate the use of NIPPV in infants for whom CPAP is likely to fail. These infants, once hemody-namically stabilized on NIPPV, can then
of this commentary is to focus our re-search on the use of NIPPV in the right direction, that is, evaluating the out-comes of infants managed with NIPPV as a second-line strategy. NIPPV can also enhance the practice of early ex-tubation in premature infants sup-ported by MV. We know that there is not a single magic bullet that can be used for the respiratory support of premature infants. Instead of trying different tools as an all-or-none modal-ity, we can introduce these tools in a practical algorithm to enhance cur-rent practices (Fig 1). Neonatal man-agement is an art of deciding when and why to use 1 tool over another. The idea that 1 method will work for all infants at all times is unrealistic. Let us stay simple and less invasive and focus our trials on protocols that have a basis in physiology, that are supported by the best available evidence, and can be translated into better clinical practice.
ACKNOWLEDGMENT
I thank Inderjeet Sandhu for help with editing this communication.
REFERENCES
1. Bhandari V, Finer NN, Ehrenkranz RA, et al; NICHD Neonatal Research Network. Synchronized nasal intermittent positive pressure ventilation and neonatal outcomes: a retrospective study. Pediat-rics.2009;124(2):517–526
2. Gedeon A.Science and Technology in Medicine: An Illustrated Account Based on Ninety-Nine Landmark Publications From Five Centuries. New York, NY: Springer Science and Business Media Inc; 2006
3. Sarkar S, Schumacher RE, Baumgart S, Donn SM. Are newborns receiving premedication before elective intubation?J Perinatol.2006;26(5):286 –289
4. Bhutada A, Sahni R, Rastogi S, Wung JT. Randomized controlled trial of thiopental for intubation in neonates.Arch Dis Child Fetal Neonatal Ed.2000;82(1):F34 –F37
5. Aly H, Badawy M, El-Kholy A, Nabil R, Mohamed A. Randomized, controlled trial on tracheal coloni-zation of ventilated infants: can gravity prevent ventilator-associated pneumonia?Pediatrics.
2008;122(4):770 –774
6. Young KC, Del moral T, Claure N, Vanbuskirk S, Bancalari E. The association between early tracheal colonization and bronchopulmonary dysplasia.J Perinatol.2005;25(6):403– 407
7. Slutsky AS. Lung injury caused by mechanical ventilation.Chest.1999;116(1 suppl):9S–15S
Nasal CPAP
NIPPV
St
abiliz
e
Deterior
ate
No apnea or bradycardia
Deterior
ate
Extu
bate
Deterior
ate
Significant apnea and bradycardiaa
FIGURE 1
8. Gammon RB, Shin MS, Buchalter SE. Pulmonary barotrauma in mechanical ventilation: patterns and risk factors.Chest.1992;102(2):568 –572
9. Kolobow T, Moretti MP, Fumagalli R, et al. Severe impairment in lung function induced by high peak airway pressure during mechanical ventilation: an experimental study.Am Rev Respir Dis.1987; 135(2):312–315
10. Muscedere JG, Mullen JB, Gan K, Slutsky AS. Tidal ventilation at low airway pressure can augment lung injury.Am J Respir Crit Care Med.1994;149(5):1327–1334
11. Wang N, Butler JP, Ingber DE. Mechanotransduction across the cell surface and through the cytoskeleton.Science.1993;260(5111):1124 –1127
12. Jobe AH, Kramer BW, Moss TJ, Newnham JP, Ikegami M. Decreased indicators of lung injury with continuous positive expiratory pressure in preterm lambs.Pediatr Res.2002;52(3):387–392 13. Imai Y, Kawano T, Miyasaka K, Takata M, Imai T, Okuyama K. Inflammatory chemical mediators
during conventional ventilation and during high frequency oscillatory ventilation.Am J Respir Crit Care Med.1994;150(6 pt 1):1550 –1554
14. Slutsky AS, Tremblay LN. Multiple system organ failure: is mechanical ventilation a contributing factor?Am J Respir Crit Care Med.1998;157(6 pt 1):1721–1725
15. Plo¨tz FB, Slutsky AS, van Vught AJ, Heijnen CJ. Ventilator-induced lung injury and multiple system organ failure: a critical review of facts and hypotheses. Intensive Care Med.2004;30(10): 1865–1872
16. Laptook AR, O’Shea TM, Shankaran S, Bhaskar B; NICHD Neonatal Network. Adverse neurodevelop-mental outcomes among extremely low birth weight infants with a normal head ultrasound: prevalence and antecedents.Pediatrics.2005;115(3):673– 680
17. Aly H. Mechanical ventilation and cerebral palsy.Pediatrics.2005;115(6):1765–1767
18. Aly H. Nasal prongs continuous positive airway pressure: a simple yet powerful tool.Pediatrics.
2001;108(3):759 –761
19. Zhang S, Garbutt V, McBride JT. Strain-induced growth of the immature lung.J Appl Physiol.
1996;81(4):1471–1476
20. Birenbaum HJ, Dentry A, Cirelli J, et al. Reduction in the incidence of chronic lung disease in very low birth weight infants: results of a quality improvement process in a tertiary level neonatal intensive care unit.Pediatrics.2009;123(1):44 –50
21. Aly H, Milner JD, Patel K, El-Mohandes AA. Does the experience with the use of nasal continuous positive airway pressure improve over time in extremely low birth weight infants?Pediatrics.
2004;114(3):697–702
22. Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB; COIN Trial Investigators. Nasal CPAP or intubation at birth for very preterm infants [published correction appears inN Engl J Med. 2008;358(14):1529].N Engl J Med.2008;358(7):700 –708
23. Walsh MC, Yao Q, Laptook A; NICHD Neonatal Research Network. Is intensity of care of neonates in first 24 hrs related to severity of illness [abstract]?Pediatr Res.2004;55:521A
COMMENTARY
PEDIATRICS Volume 124, Number 2, August 2009 789
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news
DOI: 10.1542/peds.2009-0256 originally published online July 27, 2009;
2009;124;786
Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/124/2/786
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/124/2/786#BIBL
This article cites 22 articles, 9 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/pulmonology_sub
Pulmonology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2009-0256 originally published online July 27, 2009;
2009;124;786
Pediatrics
Hany Aly
Ventilation Without Tracheal Intubation
http://pediatrics.aappublications.org/content/124/2/786
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2009 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 29, 2020
www.aappublications.org/news