ARTICLE
Effect of a School-Entry Vaccination Requirement
on Racial and Ethnic Disparities in Hepatitis B
Immunization Coverage Levels Among
Public School Students
Julie Y. Morita, MDa, Enrique Ramirez, BAa, William E. Trick, MDb
aImmunization Program, Chicago Department of Public Health, Chicago, Illinois;bCollaborative Research Unit, Cook County Hospital, Chicago, Illinois
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVE.We evaluated the overall effect of Illinois’ school-entry mandate on hepatitis B vaccination coverage levels and racial/ethnic differences in vaccination coverage before and after the mandate.
METHODS.In 1997, the Illinois Department of Public Health mandated hepatitis B
vaccination before entry into 5th grade. We conducted a retrospective cohort study of 6 consecutive Chicago public schools’ 12th-grade classes; 4 entered 5th grade before the mandate (premandate cohorts) and 2 afterward (postmandate cohorts). We used Chicago public schools’ vaccination database and calculated annual cover-age levels for 2nd through 12th grades; the cohorts entered 12th grade during 2000 –2005. We compared hepatitis B vaccination coverage levels according to race/ethnicity and coverage levels for the premandate and postmandate cohorts.
RESULTS.We evaluated 106 541 students. The postmandate cohort had significantly
higher hepatitis B vaccination coverage levels than the premandate cohort at 5th-grade (38.2% vs 4.3%) and 9th-5th-grade (85.0% vs 37.4%) entry. For 9th-5th-grade students, compared with white students, black students were less likely to have received hepatitis B vaccination before the mandate; this disparity decreased for the first postmandate cohort. For Hispanic students, the disparity was less pronounced and also decreased after the mandate. By 9th grade in the postmandate cohorts, coverage levels for all racial/ethnic groups exceeded 80%.
CONCLUSIONS.There was a dramatic decrease in the disparity of hepatitis B vaccination coverage between white and black or Hispanic students. School-entry requirements effectively increased hepatitis B vaccination coverage levels regardless of race or ethnicity and should be considered for other recently recommended adolescent vaccines.
I
N 1994, TOreduce more rapidly the incidence of hepatitis B virus infection, the Advisory Committee on Immuni-zation Practices (ACIP), the American Academy of Pediatrics (AAP), and the American Academy of Family Physicians (AAFP) approved a recommendation to expand hepatitis B vaccination (HBV) of infants to include routine vaccination of 11- to 12-year-old adolescents.1Two years later, to increase vaccination coverage against hepatitis B, measles-mumps-rubella (MMR), and varicella infections and to provide a tetanus-diphtheria booster to adolescents, the ACIP, AAP, AAFP, and the American Medical Association recommended a routine health care visit for 11- to 12-year-old patients.2 After these recommendations, results from subsequent National Health Interview Surveys indicated that adolescent coverage levels increased but remained below theHealthy People 2010objective of 90%.3In addition to falling short of target coverage levels, there is evidence of substantial racial, ethnic, and gender differences in adolescent vaccination coverage levels.4,5State vaccination laws and regulations for kindergarten entry are effective in attaining high coverage levels (⬎90%) among school attendees and have led to a marked decline in morbidity and mortality from
vaccine-www.pediatrics.org/cgi/doi/10.1542/ peds.2007-0799
doi:10.1542/peds.2007-0799
Key Words
hepatitis B vaccine, adolescent, immunization, schools
Abbreviations
ACIP—Advisory Committee on Immunization Practices
AAP—American Academy of Pediatrics AAFP—American Academy of Family Physicians
HBV— hepatitis B vaccination MMR—measles-mumps-rubella CI— confidence interval HPV— human papillomavirus
Accepted for publication Aug 1, 2007
preventable diseases.6,7These laws also serve as an effec-tive “safety net” because they apply to all children who enter school, regardless of race, ethnicity, socioeconomic status, or insurance coverage.6,8 State laws that require proof of vaccination for entry into middle school have resulted in increased adolescent vaccination coverage levels9–11; however, the effect of middle school-entry requirements on racial and ethnic disparities is un-known.
Before the 1997 school year, the Illinois Department of Public Health approved a requirement for completion of ⱖ3 doses of hepatitis B vaccine by entry into 5th grade. We describe the effect of the requirement on racial and ethnic disparities in adolescent hepatitis B vaccine coverage levels using data from 6 cohorts of Chicago public schools students; 4 cohorts entered 5th grade before the requirement, and 2 cohorts entered 5th grade after the requirement.
METHODS
Data Source
The Chicago public school system maintains an elec-tronic health database that stores students’ records for all required vaccinations. Before entry into the database, all vaccination records must be verified and signed by either a physician or a nurse. In 2005, the Chicago Department of Public Health and Chicago public schools approved a data-sharing agreement for data residing in the Chicago public schools’ health database. In a previous study us-ing manual chart audits of school records, we found good agreement between the manual chart audit and the Chicago public schools’ electronic vaccination records.12 In addition to vaccination history, the database includes students’ date of birth and vaccination date to the level of month and year, race (self-reported as black, white, Hispanic, Asian, or Native American), gender, and med-ical or religious exemptions.
We extracted data for 6 cohorts of Chicago public schools students; each cohort was composed of students in 12th grade for 6 consecutive years, 2000 through 2005. Retrospective hepatitis B coverage levels were de-termined for each cohort back to 2nd grade. For eligibil-ity for inclusion in the cohort, we required students to be enrolled in the Chicago public schools system during 12th grade. We identify each cohort by the year that the students entered 5th grade. We evaluated 4 cohorts that entered 5th grade before the requirement (1993–1996; ie, premandate cohorts) and 2 cohorts that entered 5th grade after the requirement (1997–1998; ie, postman-date cohorts). Students were retained in the cohort to which they were assigned on the basis of entry into 12th grade regardless of whether they advanced a grade in each academic year.
State Requirement
Illinois requires that students complete the HBV series before October 15 of their 5th-grade year. After this date, students may be excluded from school if they can-not provide documentation of having completed or ini-tiated the vaccine series. Students who have medical
contraindications to vaccination (infection with hepatitis B virus or serious allergy to the vaccine or 1 of its components) or religious beliefs that do not allow them to be vaccinated are permanently exempted from vacci-nation requirements. To allow students who are in the process of completing a multiple-dose vaccination series to continue attending school, nurses and administrators are allowed to temporarily exempt students for 1 year.
Coverage-Level Determination
We calculated annual coverage levels for each cohort by determining the proportion of students who had re-ceivedⱖ3 doses of hepatitis B vaccine by October 15 of the year assessed (eg, 5th-grade students in the 1993 cohort who had receivedⱖ3 doses of hepatitis B vaccine by October 15, 1993, were considered vaccinated). We also evaluated coverage levels stratified according to racial/ethnic group. Because we were provided dates at the level of the month and year, we imputed every birth and vaccination date as the 15th of the month.
To examine the effects of the 5th-grade entry require-ment on racial and ethnic coverage levels, we compared vaccination coverage levels for the 4 premandate cohorts and the 2 postmandate cohorts. Because heterosexual or homosexual transmission accounts for⬎60% of hepati-tis B infections among adults in the United States13and because⬃25% of 9th-graders report having had vaginal sex,14we report coverage levels at entry into 9th grade for white, black, and Hispanic students. For the students who were enrolled in 5th grade 1 year before (ie, the 1996 cohort) and for 2 years after implementation of the 5th-grade vaccination requirement (ie, the 1997 and 1998 cohorts), we report the risk ratios and 95% confi-dence intervals (CIs) for completion of the hepatitis B vaccine series at 5th- and 9th-grade entry. We compared black or Hispanic students with white students (ie, the referent group). Because of the relatively small percent-age of Asian/Pacific Islander and Native American stu-dents enrolled in Chicago public schools, we limited our analyses to white, black, and Hispanic students. We compared vaccination coverage levels between white and black or Hispanic students using the2test. We used SAS 9.1.3 statistical software (SAS Institute, Inc, Cary, NC) for all statistical analyses; allPvalues were 2-sided.
RESULTS
(data not shown). For all 6 cohorts, the percentage of students who were granted medical or religious exemp-tions remained⬍3.2%.
Hepatitis B Coverage Levels
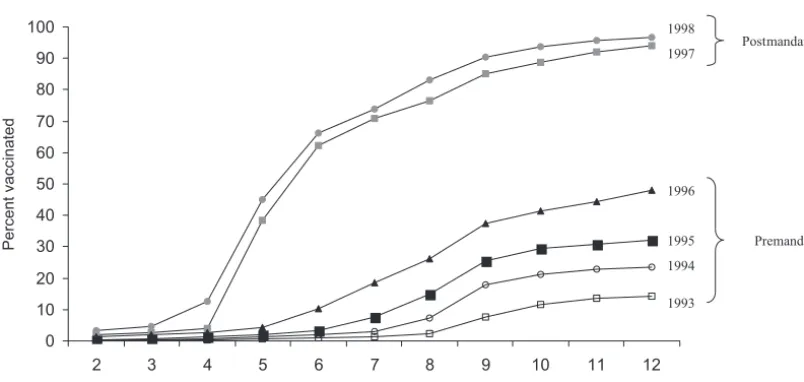
Hepatitis B vaccine coverage levels increased from 2nd through 12th grades for all cohorts (Fig 1); however, the coverage level for all premandate cohorts remained well below theHealthy People 2010goal of 90%. For the first postmandate cohort, the vaccination coverage level in-creased by 34 percentage points between the 4th and 5th grades and by 24 percentage points between the 5th and 6th grades; the increases were similar for the second postmandate cohort (Fig 1). The first postmandate co-hort had significantly higher HBV coverage levels than the final premandate cohort on entry into 5th grade (38.3% vs 4.3%; difference: 34.0%; 95% CI; 33.5%– 34.3%) and 9th grade (85.0% vs 37.4%; difference: 47.6%; 95% CI 47.4%– 47.8%;P⬍.001 for both com-parisons). The coverage levels increased even further for the second postmandate cohort for students who en-tered 5th or 9th grade (Fig 1).
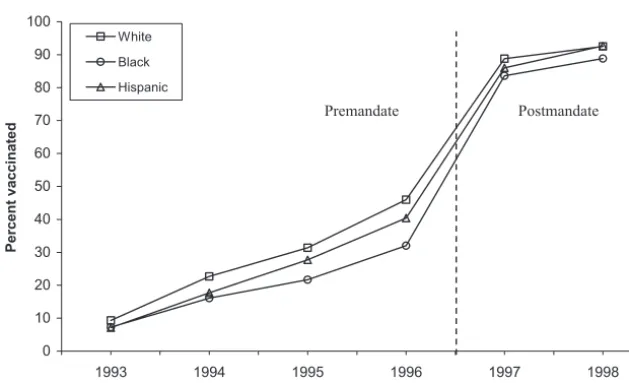
When we evaluated HBV coverage levels according to race and ethnicity, we found that before implementation of the school-entry vaccination requirement, black and Hispanic students were less likely than white students to have completed HBV by 5th and 9th grades (Table 2). For the premandate cohorts, the differences in coverage levels between white and black students were increasing (Fig 2). In contrast, for both postmandate cohorts, the differences in coverage levels between white and black or Hispanic students decreased (Fig 2). In fact, in the first postmandate cohort, Hispanic students were almost as likely as white students to have completed HBV by 5th and 9th grades (Table 2, Fig 2), and black students had similar vaccination coverage levels by 9th grade. For the second postmandate cohort, Hispanic and black students had almost achieved parity with white students by 9th grade (Table 2, Fig 2). By 12th grade, hepatitis B cover-age levels exceeded 90% for white, black, and Hispanic students (96.6%, 92.3%, and 95.6%, respectively) in the first postmandate cohort and 95% in the second post-mandate cohort (97.5%, 95.5%, and 98.1%, respec-tively).
0 10 20 30 40 50 60 70 80 90 100
2 3 4 5 6 7 8 9 10 11 12
Grade
Percent vaccinated
1998 1997
1996
1995
1994
1993
Postmandatea
Premandate
FIGURE 1
HBV coverage levels according to grade for 6 consecutive cohorts of Chicago public school students before and after the state of Illinois required vaccination.aReceipt of HBV was
required for entry into the 5th grade.
TABLE 1 Demographic Characteristics of Chicago Public School Students at Entry Into 12th Grade
Yeara N Race/Ethnicity,n(%)b Female Gender,
n(%)
Black Hispanic White Asian
Premandate cohortsc
1993 14 950 7571 (50) 4481 (30) 2001 (13) 875 (6) 8216 (55) 1994 16 733 8345 (50) 5329 (32) 2099 (13) 932 (6) 9227 (55) 1995 17 601 8812 (50) 5718 (33) 2135 (12) 899 (5) 9627 (55) 1996 18 583 9217 (50) 6152 (33) 2190 (12) 993 (5) 10 180 (55) Postmandate cohortsc
1997 18 971 9585 (51) 6234 (33) 2180 (12) 944 (5) 10 239 (54) 1998 19 703 9785 (50) 6720 (34) 2195 (11) 968 (5) 10 701 (54)
aThe year of entry for each cohort into 5th grade, the grade for which hepatitis B immunization was required. bNative American students constituted⬍0.5% in each study year.
DISCUSSION
We found that requiring completion of the HBV series by the time of 5th-grade entry dramatically reduced racial and ethnic disparities in coverage levels among adoles-cents who attended Chicago public schools. In addition to reducing disparities, by 12th grade, the school-entry mandate resulted in HBV coverage levels that exceeded theHealthy People 2010objective of 90% for all racial and ethnic categories.
The existence of racial and ethnic disparities in vac-cination coverage levels among adolescents is not sur-prising. Among preschool children, local evaluations of vaccination coverage levels in Chicago have consistently found that compared with other racial and ethnic groups, black children have the lowest vaccination cov-erage levels.12,16,17 The factors that contributed to low vaccination coverage levels among black preschool chil-dren (eg, poor access to vaccinations, suboptimal record-keeping)18are likely to persist through adolescence. In addition to the previously mentioned factors, the follow-ing adolescent-specific barriers complicate efforts to identify and vaccinate individuals who were missed at an earlier age: the nadir of medical visits occurs during 15 through 24 years of age,19and parental consent may be difficult to obtain in settings where adolescents are
unaccompanied by parents (eg, school-based vaccina-tion program).20
Although for childhood vaccinations a kindergarten school-entry requirement was considered to be a critical factor in improving coverage levels among black chil-dren,16the reduction in racial disparities occurs several years after the recommended age of vaccination, which results in a period of increased risk for disease; however, the increase in HBV coverage levels for all racial and ethnic groups occurs by 9th grade, which protects most vaccine recipients before the onset of sexual activity, the most common mode of hepatitis B transmission.13
Our findings are particularly relevant to health care providers, public health professionals, and legislators who seek strategies to achieve goals for adolescent cov-erage levels for other vaccines. For example, 6th-grade vaccination requirements for 3 recently recommended vaccinations for adolescents (Meningococcus, tetanus, diphtheria and acellular pertussis, and human papilloma-virus [HPV]) should help meet target vaccination levels while alleviating possible racial and ethnic disparities in vaccination coverage levels.
The effect of school-entry requirements on HBV lev-els is particularly relevant to the successful prevention of cervical cancer through HPV vaccination. For example, TABLE 2 Comparison of Completion of the HBV Series by Chicago Public School Students According to Race/Ethnicity Upon Entry Into 5th and
9th Grades Before and After Mandate
Yeara Fifth Grade Ninth Grade
White, %b Black Hispanic White, %b Black Hispanic
%b RR (95% CI) %b RR (95% CI) %b RR (95% CI) %b RR (95% CI)
Premandate
1996 8 (referent) 3 0.35 (0.29–0.43) 4 0.52 (0.43–0.63) 46 (referent) 32 0.70 (0.66–0.74) 40 0.88 (0.83–0.93) Postmandate
1997 46 (referent) 33 0.71 (0.68–0.75) 42 0.91 (0.86–0.96) 89 (referent) 84 0.94 (0.92–0.96) 86 0.97 (0.95–0.99) 1998 50 (referent) 39 0.78 (0.74–0.82) 51 1.0 (0.97–1.10) 93 (referent) 89 0.96 (0.95–0.97) 93 1.0 (0.99–1.00)
In 1997, the state of Illinois required receipt ofⱖ3 doses of hepatitis B vaccine before entry into the 5th grade. RR indicates relative risk.
aYear of entry into 5th grade.
bPercentage vaccinated (ie, receipt ofⱖ3 doses of hepatitis B vaccine).
0 10 20 30 40 50 60 70 80 90 100
1993 1994 1995 1996 1997 1998 Cohort year
Percent vaccinated
White
Black
Hispanic
Premandate Postmandate
FIGURE 2
both hepatitis B and HPV vaccines require 3 doses, which necessitates several visits to health care providers and monitoring the timing and number of doses admin-istered. Despite these challenges, we found that hepatitis B vaccine series completion levels by 9th grade for all racial and ethnic groups were⬎80% for the first cohort and⬎88% for the second cohort of students affected by the school-entry requirement. Because of the similarities in vaccination schedules and age of vaccination, it may be possible to extrapolate the success of the HBV re-quirement to the HPV vaccine, which likely would result in rapidly increased HPV vaccine coverage levels for all racial and ethnic groups. Acquisition of HPV infection usually occurs within the first few years after sexual initiation,21 and the percentage of people who report having vaginal sex increases from 25% in 9th grade to 75% in 12th grade.14In our study, the vaccination cov-erage levels had already increased dramatically by 9th grade; school-entry requirements for the HPV vaccine also should result in protection for the majority of ado-lescents. Because compared with white women, black and Hispanic women have a higher incidence of and mortality from cervical cancer,22it is critical that the HPV vaccine be equitably distributed to white, black, and Hispanic adolescents.
Although additional middle school vaccination re-quirements are likely to reduce substantially the mor-bidity from vaccine-preventable diseases, we have learned from the HBV school-entry requirement that several preliminary actions will facilitate public accep-tance of the requirements. Activities that improve vaccine acceptance include community and provider education, expanded access to vaccinations, provider and patient reminders, and increased use of patient-held vaccination records.23 In Illinois, the 5th-grade HBV requirement was enacted 3 years after the ACIP, AAP, and AAFP issued their recommendation for rou-tine HBV of adolescents. As a result, many programs to educate the community and health care providers and to increase access to immunizations (eg, provision of vaccine for insured, uninsured, and underinsured children; school-based vaccination drives) had been initiated before the school-entry requirement was im-plemented.
Disadvantages of premature adoption of school-entry requirements include potential opposition from health care providers and the public, who would likely have been supportive at a later time, and challenges to health care and school systems from having to vaccinate large numbers of students in a short period of time. In Chi-cago, school-entry requirements were effective in achieving high vaccination coverage levels and for elim-inating racial and ethnic disparities; however, evaluation of vaccine acceptance by physicians and the general public should be considered before additional school-entry requirements are mandated.
In our study, there was a 4-year delay (from 5th to 9th grade) in achieving hepatitis B coverage levels of ⬎80%. Although Illinois mandates that children who are out of compliance with vaccination requirements by October 15 be excluded from school, for minimization of
the negative impact on students’ educational opportuni-ties, nurses and administrators are allowed to exempt students who have initiated the 3-dose series for up to 1 year. We suspect that there may have been inconsistent enforcement of the school-entry requirement, such as extending the 1-year exemption rule. Despite the delay in vaccination, theHealthy People 2010objective of 90% coverage was achieved by 12th grade for all white, black, and Hispanic students.
The following limitations should be considered. We evaluated Chicago public schools students, most of whom are black and many of whom are of low socio-economic status; therefore, our findings may not gener-alize to other settings. Also, we required enrollment through 12th grade, and it is possible that students who left school were less likely to have been vaccinated. From 1996 through 2004, the Chicago public schools reported that the high school dropout rates ranged from 12.3% to 16.4%24; therefore, the trend for improved vaccination coverage with increasing grade may be over-estimated.
CONCLUSIONS
School mandates that required student receipt of HBV before entry into 5th grade resulted in a dramatic in-crease in vaccination coverage levels and nearly elimi-nated the difference in coverage levels between white and black or Hispanic students. School vaccination re-quirements can be an effective public health tool to prevent disease regardless of race or ethnicity. These findings are particularly relevant given the recent addi-tion of several new vaccines targeted at adolescents.
ACKNOWLEDGMENTS
We thank Susan Gerber, Chicago Department of Public Health and Robert Weinstein and Arthur Evans, Cook County Hospital, for reviewing the manuscript, and we thank Karen McMahon, Illinois Department of Public Health, for providing summaries of the hepatitis B vac-cine mandate proceedings.
REFERENCES
1. Centers for Disease Control and Prevention. Update: recom-mendations to prevent hepatitis B virus transmission—United States.MMWR Morb Mortal Wkly Rep.1995;44(30):574 –575 2. Immunization of adolescents: recommendations of the
Advi-sory Committee on Immunization Practices, the American Academy of Pediatrics, the American Academy of Family Phy-sicians, and the American Medical Association.MMWR Recomm Rep.1996;45(RR-13):1–16
3. Stokley S. Adolescent vaccination coverage levels: results from the 1997–2003 National Health Interview Survey. Paper pre-sented at: National Immunization Conference; March 6, 2006; Atlanta, GA
4. Wilson TR, Fishbein DB, Ellis PA, Edlavitch SA. The impact of a school entry law on adolescent immunization rates.J Adolesc Health.2005;37(6):511–516
5. Middleman AB. Race/ethnicity and gender disparities in the utilization of a school-based hepatitis B immunization initia-tive.J Adolesc Health.2004;34(5):414 – 419
United States: the role of school immunization laws.Vaccine.
1999;17(suppl 3):S19 –S24
7. Vaccination coverage among children entering school—United States, 2003– 04 school year. MMWR Morb Mortal Wkly Rep.
2004;53(44):1041–1044
8. Task Force on Community Preventive Services. Recommenda-tions regarding intervenRecommenda-tions to improve vaccination coverage in children, adolescents, and adults.Am J Prev Med.2000;18(1 suppl):92–96
9. Fogarty KJ, Massoudi MS, Gallo W, Averhoff FM, Yusuf H, Fishbein D. Vaccine coverage levels after implementation of a middle school vaccination requirement, Florida, 1997–2000.
Public Health Rep.2004;119(2):163–169
10. Averhoff F, Linton L, Peddecord KM, Edwards C, Wang W, Fishbein D. A middle school immunization law rapidly and substantially increases immunization coverage among adoles-cents.Am J Public Health.2004;94(6):978 –984
11. Rickert D, Deladisma A, Yusuf H, Averhoff F, Brink E, Shih S. Adolescent immunizations: are we ready for a new wave?Am J Prev Med.2004;26(1):22–28
12. Ramirez E, Bulim ID, Kraus JM, Morita J. Use of public school immunization data to determine community-level immuniza-tion coverage.Public Health Rep.2006;121(2):189 –196 13. Mast EE, Weinbaum CM, Fiore AE, et al. A comprehensive
immunization strategy to eliminate transmission of hepatitis B virus infection in the United States: recommendations of the Advisory Committee on Immunization Practices (ACIP) Part II: immunization of adults.MMWR Recomm Rep.2006;55(RR-16): 1–33; quiz CE31–CE34
14. Mosher WD, Chandra A, Jones J. Sexual behavior and selected health measures: men and women 15– 44 years of age, United States, 2002.Adv Data.2005;(362):1–55
15. US Census Bureau. American Community Survey, 2005 sum-mary tables; generated by Enrique Ramirez; using American FactFinder. Available at: http://factfinder.census.gov/servlet/ DTTable?_bm⫽y&-context⫽dt&ds_name⫽ACS_2005_EST_ G00_&-CONTEXT⫽dt&mt_name⫽ACS_2005_EST_G2000_
B01001&-tree_id⫽305&-redoLog⫽false&-geo_id⫽16000US17 14000&-search_results⫽01000US&-format⫽&-_lang⫽en. Accessed July 9, 2007
16. Dominguez SR, Parrott JS, Lauderdale DS, Daum RS. On-time immunization rates among children who enter Chicago public schools.Pediatrics.2004;114(6). Available at: www.pediatrics.org/ cgi/content/full/114/6/e741
17. Kenyon TA, Matuck MA, Stroh G. Persistent low immuniza-tion coverage among inner-city preschool children despite ac-cess to free vaccine.Pediatrics.1998;101(4 pt 1):612– 616 18. Watson JT, Ramirez E, Evens A, Bellini WJ, Johnson H, Morita
J. Measles immunization coverage determined by serology and immunization record from children in two Chicago communi-ties.Public Health Rep.2006;121(3):262–269
19. Woodwell DA, Cherry DK. National Ambulatory Medical Care Survey: 2002 summary.Adv Data.2004;(346):1– 44
20. Humiston SG, Rosenthal SL. Challenges to vaccinating adolescents: vaccine implementation issues.Pediatr Infect Dis J.
2005;24(6 suppl):S134 –S140
21. Winer RL, Lee SK, Hughes JP, Adam DE, Kiviat NB, Koutsky LA. Genital human papillomavirus infection: incidence and risk factors in a cohort of female university students [published correction appears inAm J Epidemiol. 2003;157(9):858].Am J Epidemiol.2003;157(3):218 –226
22. Ries LAG, Krapcho M, Mariotto A, et al, eds. SEER Cancer Statistics Review, 1975–2003. Bethesda, MD: National Cancer Institute; 2006
23. Briss PA, Rodewald LE, Hinman AR, et al. Reviews of evidence regarding interventions to improve vaccination coverage in children, adolescents, and adults. The Task Force on Commu-nity Preventive Services. Am J Prev Med. 2000;18(1 suppl): 97–140
DOI: 10.1542/peds.2007-0799
2008;121;e547
Pediatrics
Julie Y. Morita, Enrique Ramirez and William E. Trick
Students
Disparities in Hepatitis B Immunization Coverage Levels Among Public School
Effect of a School-Entry Vaccination Requirement on Racial and Ethnic
Services
Updated Information &
http://pediatrics.aappublications.org/content/121/3/e547
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/121/3/e547#BIBL
This article cites 17 articles, 1 of which you can access for free at:
Subspecialty Collections
_sub
http://www.aappublications.org/cgi/collection/vaccine:immunization Vaccine/Immunization
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su Infectious Disease
http://www.aappublications.org/cgi/collection/school_health_sub School Health
_sub
http://www.aappublications.org/cgi/collection/community_pediatrics Community Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2007-0799
2008;121;e547
Pediatrics
Julie Y. Morita, Enrique Ramirez and William E. Trick
Students
Disparities in Hepatitis B Immunization Coverage Levels Among Public School
Effect of a School-Entry Vaccination Requirement on Racial and Ethnic
http://pediatrics.aappublications.org/content/121/3/e547
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.