Evaluation of an Of
fi
ce Protocol to Increase Exclusivity of
Breastfeeding
WHAT’S KNOWN ON THIS SUBJECT: A gap exists with lack of programs to help mothers breastfeed. The 2012 American Academy of Pediatrics’ “Policy Statement on Breastfeeding and the Use of Human Milk”re-emphasized breastfeeding as an important public health initiative rather than a lifestyle choice.
WHAT THIS STUDY ADDS: Families who receive care in a primary care setting that has implemented a“breastfeeding-friendly” office protocol may have increased rates of exclusive
breastfeeding. This study evaluated an accepted clinical protocol in a large, diverse pediatric primary care setting.
abstract
OBJECTIVE:The purpose of this study was to determine whether imple-menting a program based on a clinical protocol affects breastfeeding rates within a pediatric primary care setting. Increasing breastfeeding rates is an important public health initiative identified by multiple agencies.
METHODS:The Academy of Breastfeeding Medicine (ABM) clinical pro-tocol (“The Breastfeeding-Friendly Physician’s Office, Part 1: Optimizing Care for Infants and Children”) was used as a template for the provision of breastfeeding services within a pediatric primary care clinic. There were 757 mother–infant pairs included in the study. A retrospective before-and-after study design was used. Data collection points included the hospital stay, the newborn visit, and the 2-, 4-, and 6-month health maintenance visits. The 2 groups were compared to estimate the protocol’s effectiveness as a method of increasing breastfeeding rates.
RESULTS: The results of this evaluation were positive for exclusive breastfeeding, with group comparisons showing a statistically signif-icant increase in exclusive breastfeeding rates at all 5 time points. CONCLUSIONS:Our diverse patient population within a pediatric prac-tice had increased initiation rates and exclusive breastfeeding rates after implementation of the ABM’s breastfeeding-friendly protocol. Families who receive care in a pediatric primary care setting that has implemented the ABM clinical protocol may have increased rates of exclusive breastfeeding.Pediatrics2013;131:942–950
AUTHORS:Sharon K. Corriveau, DNP, RN, CFNP, IBCLC,a
Emily E. Drake, PhD, RN,bAnn L. Kellams, MD, IBCLC,cand
Virginia G. Rovnyak, PhDb
aLoudoun Pediatric Associates, Leesburg, Virginia;bSchool of
Nursing, University of Virginia, Charlottesville, Virginia; and
cNewborn Nursery, University of Virginia, Charlottesville, Virginia
KEY WORDS
baby-friendly, breastfeeding, breastfeeding education, breastfeeding exclusive, evidence-based health care, primary health care
ABBREVIATIONS
AAP—American Academy of Pediatrics ABM—Academy of Breastfeeding Medicine EMR—electronic medical record
IBCLC—International Board-Certified Lactation Consultant RN—registered nurse
WHO—World Health Organization
Drs Corriveau, Drake, and Kellams participated in the concept and design of the study, analysis and interpretation of data, and drafting of the manuscript; Dr Rovnyak participated in the analysis and interpretation of data; and all authors approved the manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-1310
doi:10.1542/peds.2012-1310
Accepted for publication Jan 12, 2013
Address correspondence to Sharon K. Corriveau, DNP, RN, CFNP, IBCLC, 2001 Lakeport Way, Reston, VA 20191. E-mail: sharcorr@aol. com
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have nofinancial relationships relevant to this article to disclose.
Increasing breastfeeding exclusivity and duration is an important public health initiative. The Centers for Dis-ease Control and Prevention’s 2012 Breastfeeding Report Card1 reveals 76.9% of women are initiating breast-feeding in the early postpartum period; however, exclusivity and duration of breastfeeding rapidly decline within a short time period.
The American Academy of Pediatrics (AAP),2the World Health Organization (WHO), the United Nations Children’s Fund,3and the US Department of Health and Human Services4have established increasing breastfeeding rates as im-perative.
The 2011 US Surgeon General’s Call to Action to Support Breastfeeding endorses breastfeeding as the best nutrition for infants and details action items for the health care system as a mechanism for supporting breast-feeding families. The Call to Action implementation strategy for health care specifically states“models should be established to integrate assistance with breastfeeding into routine prac-tice settings.”5
The Academy of Breastfeeding Medicine (ABM) has published a clinical protocol,
“The Breastfeeding-Friendly Physi-cian’s Office, Part 1: Optimizing Care for Infants and Children.”6 This protocol provides guidance for implementing breastfeeding support in the primary care setting and was developed based on the WHO and United Nations Child-ren’s Fund Baby-Friendly Hospital Ini-tiative.3 The literature describes this initiative as a systematic intervention providing a positive predictor of breastfeeding initiation and duration.7–16 Education of pediatricians was also identified as effective,16–18 along with lactation consultant support16,19–24and maternal self-efficacy.25–29 The ABM protocol was chosen for the current study because it includes all of these components.
Cardosa et al30 implemented the Brazilian Breastfeeding-Friendly Pri-mary Care Initiative, which is based on the WHO’s“Ten Steps to Successful Breastfeeding,” in their pediatric pri-mary care setting and found an increase in the rates of breastfeeding as well as reduced rates of disease in infants aged,1 year. The primary care setting is well situated for the extension of hospital-based breastfeeding support in combination with the established AAP’s health maintenance visits. However, there are no known studies regarding the effect of a“breastfeeding-friendly” protocol in pediatric primary care in the United States.
The goal of the current study was to determine whether the use of a breastfeeding-friendly clinical pro-tocol in a multicultural, suburban/rural US pediatric primary care setting would increase breastfeeding rates.
METHODS Design
A retrospective before-and-after design was used. Retrospective data were collected from 2 groups of patients. The preintervention group included fami-lies visiting the primary care setting with their infant for regular health maintenance visits before implementa-tion of the breastfeeding-friendly clinical protocol, and the postintervention group included those families cared for after the protocol was in place. The source of feeding was collected via record review by using 5 time points: the hospital stay, the initial outpatient newborn visit, and the 2-, 4-, and 6-month health mainte-nance visits.
For the purpose of this study, breast-feeding definitions are described as exclusive or any breastfeeding. Exclusive breastfeeding was defined as breast milk (including milk expressed) and any drops, vitamins, or medicines. It could also include solid foods if reported at
6 months but not earlier. Formula was not included. Any breastfeeding was defined as breast milk (including milk expressed) combined with any food or liquid including any non-human milk and formula.
Setting
The study was conducted within a pe-diatric primary care setting at 2 loca-tions of a single practice. Both localoca-tions are in northern Virginia, 1 in a suburban area and the other in a rural setting. The populations accessing both offices comprise a general mix of socioeco-nomic classes from upper-income families to poverty-level families. Be-cause of its proximity to the Washington, DC, metropolitan area, there is a large commuter population, and families from many ethnicities are well repre-sented. Populations accessing the rural setting also include families from West Virginia.
The clinics are staffed by 13 medical providers. The total practice population is∼13 000 patients with a patientflow of∼45 newborns entering the practice each month. The practice uses elec-tronic medical records (EMRs), and specific information regarding nutri-tion is gathered at each health main-tenance visit.
Sample
of birth, singleton birth, who entered the practice within the first week of life, remained in the practice for at least the first 6 months of age, and returned for their health maintenance visits at 2, 4, and 6 months. Exclusion criteria included infants with con-genital birth defects, preterm infants, multiple birth, infants not residing with their birth mother, who left the practice before 6 months of age, en-tered the practice at.1 week of age, had missing EMR data, or had moth-ers with a known contraindication to breastfeeding.
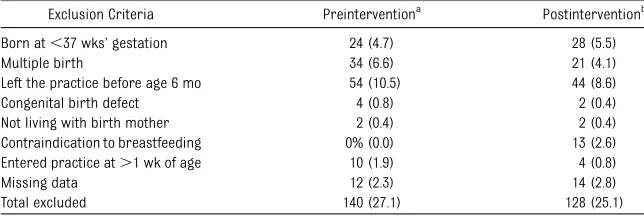
Convenience samples were obtained. For the preintervention group, all newborn records for the year 2008 were included, resulting in 516 mother– infant dyads. After applying exclusion criteria, 376 records remained for re-view. For the postintervention group, record review began in September 2010 and continued through June 2011, for a total of 509 mother–infant dyads. Once exclusion criteria were applied, 381 records remained for review. There were 140 newborns excluded from the preintervention group and 128 ex-cluded from the postintervention group. Primary reasons for exclusions were: born at ,37 weeks’ gestation, multiple births, and left the practice before 6 months of age (Table 1).
It was expected that due to the nature of EMRs and strict staff training, most data would be recorded. The University of Virginia institutional review board
approved the study as exempt before any data collection.
Intervention
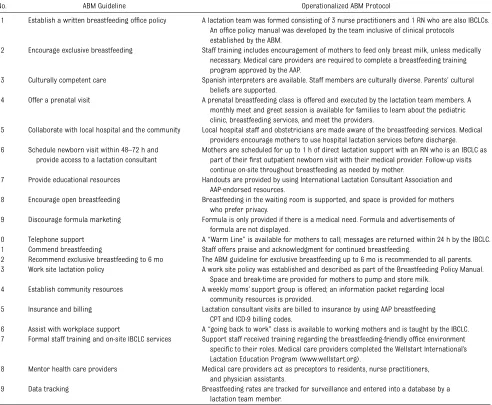
Implementation of the protocol began in December 2009 and continued for 10 months. This protocol included staff training, written policies, on-site lac-tation consultant support, community outreach, and data tracking (Table 2). Major components of this protocol in-cluded use of an AAP/WHO-approved breastfeeding curriculum for training medical staff32and direct support with an on-site International Board Certified Lactation Consultant (IBCLC) for all breastfeeding dyads. At the initial out-patient newborn visit, an EMR template was used to uncover and document indicators for professional lactation support such as excessive infant weight loss, breastfeeding concerns, or in-adequate output of stool (Table 3).33,34 Subsequent health maintenance visits include components of this template to stimulate medical providers to refer for lactation services through 6 months of age. Treatment fidelity monitoring was conducted by a committee of nurse practitioners who were also IBCLCs. They monitored staff training, audited charts for protocol adherence, tracked new-born scheduling to maintain consis-tency, and ensured integrity of data collection.
Patients enter the practice at birth from the local hospital or outlying hospitals at their initial outpatient newborn visit.
All breastfeeding dyads are scheduled with a registered nurse (RN), who is also an IBCLC, at the same time as their initial newborn appointment. This scheduling results in an extended visit allowing focused time with an IBCLC, followed by the established standard of care assessment by the medical pro-vider. Specifically, breastfeeding dyads begin their visit with the RN-IBCLC who provides up to 1 hour of breastfeeding support comprising an initial assess-ment, direct assistance, and plans for continued support. They are seen in a specially equipped room that includes a precision scale to measure milk transfer, a comfortable chair, breast-feeding pillow, and supplies that may be needed by the IBCLC. On completion of this portion of the newborn visit, the IBCLC presents her findings to the medical provider who subsequently performs a standard newborn visit. The medical provider includes In-ternational Classification of Diseases, Ninth Revision, Clinical Modification billing codes associated with newborn feeding to submit this paired encoun-ter to insurance for reimbursement.35,36 Mothers are instructed to return for additional support, as needed, through-out their breastfeeding time frame.
For all subsequent health maintenance as well as acute visits, any concerns regarding breastfeeding are expected to generate a referral for lactation services by the medical provider. Follow-up lactation visits are also scheduled for 1 hour, coupled with an examination by a medical provider, and billed to insurance.
A monthly“meet and greet”session is advertised to the community as an op-portunity for families to view the setting and meet the providers. Breastfeeding services are highlighted; a tour of the facility is provided, along with provision of information regarding a monthly pre-natal breastfeeding class and a weekly drop-in moms’support group.
TABLE 1 Excluded Mother–Infant Dyads
Exclusion Criteria Preinterventiona
Postinterventionb
Born at,37 wks’gestation 24 (4.7) 28 (5.5)
Multiple birth 34 (6.6) 21 (4.1)
Left the practice before age 6 mo 54 (10.5) 44 (8.6)
Congenital birth defect 4 (0.8) 2 (0.4)
Not living with birth mother 2 (0.4) 2 (0.4)
Contraindication to breastfeeding 0% (0.0) 13 (2.6)
Entered practice at.1 wk of age 10 (1.9) 4 (0.8)
Missing data 12 (2.3) 14 (2.8)
Total excluded 140 (27.1) 128 (25.1)
Data are presented asn(%).
Data Collection
De-identified data were collected via retrospective record review and en-tered into the SPSS version 19 program (IBM SPSS Statistics, IBM Corporation, Armonk, NY). Feeding data were recorded from the hospital, the initial newborn visit (defined as #1 week), and the 2-, 4-, and 6-month health maintenance visits. Demographic data abstracted included gender of the in-fant, birth weight, type of delivery, age of the mother, parity, and type of in-surance. Although an attempt to ob-tain race/ethnicity data was made, this
information was not routinely collected as part of the medical record, but the distribution was expected to be similar in both groups.
No feeding data were missing for the 1-week or 2-, 4-, and 6-month health maintenance visits. In-hospital new-born feeding data were missing for 23 (6.1%) of 376 infants in the pre-intervention group and 11 (2.9%) of 381 infants in the postintervention group.
Statistical Analysis
The preintervention and postinter-vention groups were compared on
demographic characteristics and on their rates of exclusive and any breast-feeding at each of the 5 time points. Comparisons used Student’st test for continuous variables andx2tests with continuity correction for categorical variables.
Logistic regression analyses were conducted on each of the 10 outcomes (exclusive breastfeeding and any breast-feeding recorded at each of the 5 time points) to determine if a bivariate in-tervention effect, if any, would persist when other risk factors were taken into account. A factor was included in TABLE 2 ABM Clinical Protocol Number 14 (Abbreviated)
No. ABM Guideline Operationalized ABM Protocol
1 Establish a written breastfeeding office policy A lactation team was formed consisting of 3 nurse practitioners and 1 RN who are also IBCLCs. An office policy manual was developed by the team inclusive of clinical protocols
established by the ABM.
2 Encourage exclusive breastfeeding Staff training includes encouragement of mothers to feed only breast milk, unless medically necessary. Medical care providers are required to complete a breastfeeding training program approved by the AAP.
3 Culturally competent care Spanish interpreters are available. Staff members are culturally diverse. Parents’cultural beliefs are supported.
4 Offer a prenatal visit A prenatal breastfeeding class is offered and executed by the lactation team members. A
monthly meet and greet session is available for families to learn about the pediatric clinic, breastfeeding services, and meet the providers.
5 Collaborate with local hospital and the community Local hospital staff and obstetricians are made aware of the breastfeeding services. Medical providers encourage mothers to use hospital lactation services before discharge. 6 Schedule newborn visit within 48–72 h and
provide access to a lactation consultant
Mothers are scheduled for up to 1 h of direct lactation support with an RN who is an IBCLC as part of theirfirst outpatient newborn visit with their medical provider. Follow-up visits continue on-site throughout breastfeeding as needed by mother.
7 Provide educational resources Handouts are provided by using International Lactation Consultant Association and AAP-endorsed resources.
8 Encourage open breastfeeding Breastfeeding in the waiting room is supported, and space is provided for mothers who prefer privacy.
9 Discourage formula marketing Formula is only provided if there is a medical need. Formula and advertisements of formula are not displayed.
10 Telephone support A“Warm Line”is available for mothers to call; messages are returned within 24 h by the IBCLC.
11 Commend breastfeeding Staff offers praise and acknowledgment for continued breastfeeding.
12 Recommend exclusive breastfeeding to 6 mo The ABM guideline for exclusive breastfeeding up to 6 mo is recommended to all parents. 13 Work site lactation policy A work site policy was established and described as part of the Breastfeeding Policy Manual.
Space and break-time are provided for mothers to pump and store milk. 14 Establish community resources A weekly moms’support group is offered; an information packet regarding local
community resources is provided.
15 Insurance and billing Lactation consultant visits are billed to insurance by using AAP breastfeeding
CPT and ICD-9 billing codes.
16 Assist with workplace support A“going back to work”class is available to working mothers and is taught by the IBCLC. 17 Formal staff training and on-site IBCLC services Support staff received training regarding the breastfeeding-friendly office environment
specific to their roles. Medical care providers completed the Wellstart International’s Lactation Education Program (www.wellstart.org).
18 Mentor health care providers Medical care providers act as preceptors to residents, nurse practitioners, and physician assistants.
19 Data tracking Breastfeeding rates are tracked for surveillance and entered into a database by a
lactation team member.
all 10 models if it was significantly dif-ferent in the preintervention and post-intervention or if it had a significant effect ata= .10 on$1 of the 10 out-comes in bivariate analyses performed on the whole sample. In all of the mod-els, the factors were entered together.
Because race/ethnicity information was not available for 58% of the records, no imputation was done and
no statistical tests were conducted on this factor.
RESULTS
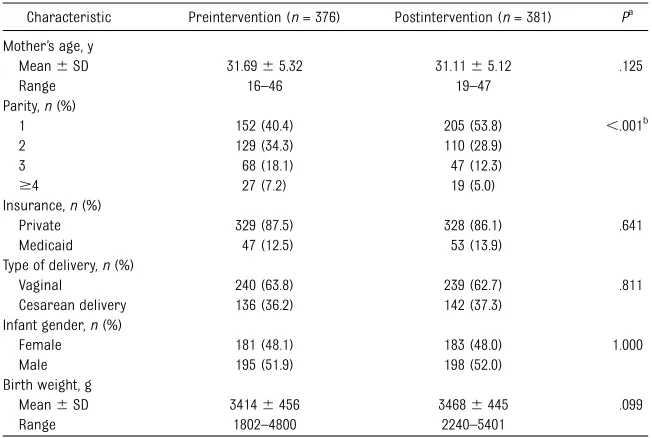
There were no significant differences between the groups for infant gender, birth weight, type of delivery, age of the mother, or type of insurance. A pre–post increase in the proportion of primipa-rous mothers from 40.4% to 53.8% (P,.001) was noted (Table 4).
Rates for exclusive breastfeeding were higher in the postintervention group than in the preintervention group at every time point, and the differences in the rates were statistically significant at all 5 time points (P,.01). Of particular note, when comparing exclusive breast-feeding rates, the postintervention group rates were at least 10 percentage points higher than those in the pre-intervention group at all 5 time points (Fig 1).
Rates for any breastfeeding were higher in the postintervention group than in the preintervention group at every time point, but the differences in the group rates were statistically
significant only at the 1-week time point (P= .021) (Fig 2).
Thefinding that the percentage offi rst-time mothers was significantly higher in the postintervention group versus the preintervention group raised the question as to whether this had an ef-fect on the results. Thex2 tests com-paring rates of exclusive breastfeeding and any breastfeeding preintervention versus postintervention, at all 5 time points, were conducted separately for primiparous and multiparous moth-ers. The results were almost the same as for the parity groups combined, the only exception being that at week 1 for the multiparous mothers, the increase in the exclusive breastfeeding rate was only 9.6 percentage points, which, with P= .059, fell just short of significance at thea=.05 level.
Logistic regression analyses were conducted on each of the 10 outcomes: exclusive breastfeeding (1 = yes, 0 = no) and any breastfeeding (1 = yes, 0 = no) recorded at each of the 5 time points. The risk factors included in each model were: group (1 = postintervention, 0 = preintervention), primiparous (1 = primiparous, 0 = multiparous), birth method (1 = cesarean delivery, 0 = spontaneous vaginal delivery), in-surance (1 = Medicaid, 0 = private), birth weight (100-g units), and mother’s age (years). The primiparous factor was included because the rates for this differed significantly between the preintervention and postintervention groups. Each of the other 5 factors had a significant effect at thea= .10 level in bivariate analyses on the whole sample for $2 of the 10 breastfeeding out-comes.
The group indicator was highly signifi -cant for exclusive breastfeeding at ev-ery time point (P , .001) but not significant for any breastfeeding ex-cept at week 1 (P= .016). The estimated odds of exclusive or any breastfeeding for those in the postintervention group TABLE 3 Indicators for Professional
Lactation Support
Weight loss since birth [ ]% [none] [gaining]
[.7%: refer to lactation within 24 h] [.10%: refer to lactation today] Feeding:“What are you feeding your infant?”
[Breast milk] [formula] [both]
Breast milk: frequency: every [2] [3] [4] h Breastfeeding quality: [good] [poor:
refer to lactation]
Breast pain/any concerns: [no] [yes: refer to lactation ] [describe]
Stool: Has your infant had,3 stools in last 24 h? [no] [yes: refer to lactation]
Quality: [greenish] [yellow, seedy] [dark/tarry on day 4 or later: refer to lactation] Urine: difficulties/concerns?
[no] [yes] [ ]: no. of wet diapers [,3 on day 3: refer to lactation]
Parameters were adapted from the Massachusetts Breast-feeding Coalition.34
TABLE 4 Demographic Characteristics of the Sample (N= 757)
Characteristic Preintervention (n= 376) Postintervention (n= 381) Pa
Mother’s age, y
Mean6SD 31.6965.32 31.1165.12 .125
Range 16–46 19–47
Parity,n(%)
1 152 (40.4) 205 (53.8) ,.001b
2 129 (34.3) 110 (28.9)
3 68 (18.1) 47 (12.3)
$4 27 (7.2) 19 (5.0)
Insurance,n(%)
Private 329 (87.5) 328 (86.1) .641
Medicaid 47 (12.5) 53 (13.9)
Type of delivery,n(%)
Vaginal 240 (63.8) 239 (62.7) .811
Cesarean delivery 136 (36.2) 142 (37.3)
Infant gender,n(%)
Female 181 (48.1) 183 (48.0) 1.000
Male 195 (51.9) 198 (52.0)
Birth weight, g
Mean6SD 34146456 34686445 .099
Range 1802–4800 2240–5401
aPvalue comparing the 2 groups by usingttests for continuous variables,x2
tests with continuity correction for di-chotomous variables, and the Pearsonx2test for the 4-level parity variable.
bP,.001 for a test of a 2-level parity variable (primiparous [yes/no]) versus group;P= .002 for a test of the 4-level parity
were higher in every case than for those in the preintervention group; odds ratios varied between 1.67 and 2.66 for the 5 exclusive breastfeeding outcomes, and they varied between 1.1 and 1.77 for the 5 any breastfeeding outcomes.
The primiparous indicator was not significant in any of the 10 regressions, withPvalues ranging from .163 to .862. However, the insurance indicator was highly significant in all 10 regressions (P,.004 in every case), with the es-timated odds of any or exclusive
breastfeeding for those receiving Med-icaid being only 28% to 47% of the odds for those with private insurance. The effect of birth weight on breastfeeding was significant at 2, 4, and 6 months after birth. At 2 and 6 months, the es-timated odds of exclusive breastfeed-ing increased by 4% to 5% with every additional 100 g of birth weight. At 2, 4, and 6 months, the estimated odds of any breastfeeding increased 4% to 6% with every additional 100 g of birth weight. The only other predictor that was significant at any time was birth method. In the hospital, the odds of exclusive breastfeeding were signifi -cantly lower for those who had a ce-sarean delivery compared with those with vaginal delivery (odds ratio: 0.51; P, .001). But birth method was not a significant predictor of exclusive breastfeeding at 1 week or at 2 and 4 months. It was significant again at 6 months (odds ratio: 0.661; P = .017). Birth method was not a significant predictor of any breastfeeding at any time point. Mother’s age was not sig-nificant in any of the 10 models, despite its effect (P,.10) on 5 of the 10 out-comes in bivariate analyses.
DISCUSSION
The x2 tests and logistic regression analyses showed that rates of exclu-sive breastfeeding were significantly higher for those in the postintervention group. Although exclusive breastfeed-ing increased significantly, the increa-ses in rates for any breastfeeding were not significant except for the 1-week time point. One possible explanation is, for mothers who were exclusively breastfeeding in the early postpartum period, breastfeeding persisted be-cause formula was not introduced. Forster et al37found a negative asso-ciation between introduction of for-mula in the hospital and breastfeeding duration. Hörnell et al38reported that the earlier an infant was given formula, FIGURE 1
Rates of exclusive breastfeeding preintervention and postintervention (may include solids if reported at 6 months; no formula). The increase in the rate of exclusive breastfeeding from preintervention to postintervention was statistically significant at all 5 time points at thea= .05 level of significance (P,
.01). **P,.001, *P,.01.
FIGURE 2
the shorter the duration of breast-feeding, while introduction of solids for the exclusively breastfed infants had no association with total breastfeeding duration.
The initiation rate for the exclusively breastfeeding postintervention group was much higher compared with the preintervention group (78% and 59%, respectively). This finding might be explained by 1 of the features of the protocol, which provides a prenatal meet and greet session to expose parents to an environment that supports breastfeed-ing mothers. Mothers who entered the practice after the breastfeeding-friendly office protocol was in place may have had increased motivation to initiate breast-feeding because they knew they would have continued support. Alternatively, it may be that mothers who were in-terested in breastfeeding sought out a supportive environment, therefore creating the potential for selection bias. Measurement of predelivery intention to breastfeed could have eliminated this as a concern.
The literature suggests primiparous women have more difficulty sustaining breastfeeding and they may breastfeed longer if they are knowledgeable and self-confident.39–41 We found similar results; when the primiparous mothers were compared preintervention and postintervention for exclusive and any
breastfeeding, both rates increased at every time point, and the pre–post increases for exclusive breastfeeding were statistically significant (P,.05) at every time point. Therefore, the ABM protocol may have had a positive effect on exclusivity for the primiparous mothers in this study.
The literature describes mothers’ pre-delivery intention to breastfeed as a strong predictor of initiating breast-feeding and continuing through early obstacles.39–44 The ABM protocol pro-vided a mechanism for extending com-ponents that support breastfeeding into the primary care setting, creating an environment that supports a mother’s intention to breastfeed. Continued lac-tation consultant support is empha-sized in the Surgeon General’s Call to Action and is called for as part of the breastfeeding-friendly office protocol. Direct support for breastfeeding dyads can be time intensive. Pairing IBCLC services with medical professionals who are also educated in breastfeeding creates a vehicle for access and re-imbursement, and it teams health pro-fessionals with shared intentions.
This study was limited by a lack of data regarding other parameters that may affect exclusivity and duration of breastfeeding such as mother’s edu-cational level, social support, smoking, work, and socioeconomic status.43,44
CONCLUSIONS
The results from this study suggest that the use of a breastfeeding-friendly clinical protocol in the primary care setting may help increase exclusive (no formula) breastfeeding rates up to 6 months of age. The risks associated with not providing breast milk are nu-merous.45–52 The ABM protocol pro-vides a template that encompasses interventions supported by the litera-ture to increase breastfeeding rates.
Although not a randomized controlled trial, implementation of the ABM clin-ical protocol with preintervention and postintervention data collection pro-vided an important evaluation of this program with useful data for clinical practice. This study provides an ex-ample of how the protocol can be operationalized. Further studies should explore use of this protocol, inclusive of patient populations and/or regions known to have low breastfeeding rates, to help expand its use and ad-dress this important public health initiative.
ACKNOWLEDGMENTS
This work was supported by Loudoun Pediatric Associates, a pediatric pri-mary care clinic that is part of Loudoun Medical Group located in Leesburg, Vir-ginia, and by the University of VirVir-ginia, Charlottesville, Virginia.
REFERENCES
1. Centers for Disease Control and Pre-vention. Breastfeeding among US children born 2000–2009, CDC national immuniza-tion survey. Atlanta, GA: Centers for Disease Control and Prevention; 2012. Available at: www.cdc.gov/breastfeeding/data/NIS_data/ index.htm. Accessed August 2012.
2. Eidelman AI, Schanler RJ, Johnston M, et al; American Academy of Pediatrics. Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics.Published February 27, 2012. Available at: http://pe-diatrics.aappublications.org/content/early/ 2012/02/22/peds.2011-3552
3. World Health Organization and United Nations Children’s Fund. Baby-Friendly Hospital Initiative revised, updated and expanded for integrated care. Published 2009. Available at: http://whqlibdoc.who.int/ publications/2009/9789241594967_eng.pdf
4. US Department of Health and Human Services. Maternal, infant, and child health. Healthy People 2020; 2010. Available at: http:// healthypeople.gov/2020/topicsobjectives2020/ overview.aspx?topicid=26
5. US Department of Health and Human Services. The Surgeon General’s Call to Action to Support Breastfeeding. Washington,
DC: US Department of Health and Human Services, Office of the Surgeon General; 2011. Available at: www.surgeongeneral. gov/topics/breastfeeding/calltoactiontosup portbreastfeeding.pdf
6. Chantry CJ, Howard CR, Lawrence RA, Powers NG; Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol #14: breastfeeding-friendly physi-cian’s office, part 1: optimizing care for infants and children.Breastfeed Med. 2006; 1(2):115–119
mothers. Cochrane Database Syst Rev. 2007;(1):CD001141
8. Braun ML, Giugliani ER, Soares ME, Giugliani C, de Oliveira AP, Danelon CM. Evaluation of the impact of the baby-friendly hos-pital initiative on rates of breastfeeding.
Am J Public Health. 2003;93(8):1277– 1279
9. Duyan Camurdan A, Ozkan S, Yüksel D, Pasli F, Sahin F, Beyazova U. The effect of the baby-friendly hospital initiative on long-term breast feeding. Int J Clin Pract. 2007;61(8):1251–1255
10. Hannula L, Kaunonen M, Tarkka MT. A sys-tematic review of professional support interventions for breastfeeding. J Clin Nurs. 2008;17(9):1132–1143
11. Kramer MS, Chalmers B, Hodnett ED, et al; PROBIT Study Group (Promotion of Breast-feeding Intervention Trial). Promotion of breastfeeding intervention trial (PROBIT): a randomized trial in the Republic of Belarus.JAMA. 2001;285(4):413–420 12. Merewood A, Philipp BL, Chawla N, Cimo S.
The baby-friendly hospital initiative increa-ses breastfeeding rates in a US neonatal intensive care unit.J Hum Lact. 2003;19(2): 166–171
13. Merewood A, Patel B, Newton KN, et al. Breastfeeding duration rates and factors affecting continued breastfeeding among infants born at an inner-city US Baby-Friendly hospital. J Hum Lact. 2007;23(2): 157–164
14. Merten S, Dratva J, Ackermann-Liebrich U. Do baby-friendly hospitals influence breastfeeding duration on a national level?
Pediatrics. 2005;116(5):e702–e708. Avail-able at: www.pediatrics.org/cgi/content/ full/116/5/e702
15. Murray EK, Ricketts S, Dellaport J. Hospital practices that increase breastfeeding du-ration: results from a population-based study.Birth. 2007;34(3):202–211
16. Chung M, Raman G, Trikalinos T, Lau J, Ip S. Interventions in primary care to promote breastfeeding: an evidence review for the US Preventive Services Task Force.Ann In-tern Med. 2008;149(8):565–582
17. Feldman-Winter L, Barone L, Milcarek B, et al. Residency curriculum improves breastfeeding care.Pediatrics. 2010;126(2): 289–297
18. Lu MC, Lange L, Slusser W, Hamilton J, Halfon N. Provider encouragement of breast-feeding: evidence from a national survey.Obstet Gynecol. 2001;97(2):290–295 19. Guise JM, Palda V, Westhoff C, Chan BK, Helfand M, Lieu TA; US Preventive Services Task Force. The effectiveness of primary care-based interventions to promote
breastfeeding: systematic evidence review and meta-analysis for the US Preventive Services Task Force.Ann Fam Med. 2003;1 (2):70–78
20. Bonuck KA, Trombley M, Freeman K, McKee D. Randomized, controlled trial of a pre-natal and postpre-natal lactation consultant intervention on duration and intensity of breastfeeding up to 12 months.Pediatrics. 2005;116(6):1413–1426
21. Gau ML. Evaluation of a lactation in-tervention program to encourage breast-feeding: a longitudinal study. Int J Nurs Stud. 2004;41(4):425–435
22. Labarere J, Gelbert-Baudino N, Ayral AS, et al. Efficacy of breastfeeding support provided by trained clinicians during an early, routine, preventive visit: a pro-spective, randomized, open trial of 226 mother-infant pairs. Pediatrics. 2005;115 (2):e139–e146. Available at: www.pediat-rics.org/cgi/content/full/115/2/e139
23. Lukac M, Riley JK, Humphrey AD. How to integrate a lactation consultant in an out-patient clinic environment. J Hum Lact. 2006;22(1):99–103
24. Thurman SE, Allen PJ. Integrating lactation consultants into primary health care ser-vices: are lactation consultants affecting breastfeeding success?Pediatr Nurs. 2008; 34(5):419–425
25. Blyth R, Creedy DK, Dennis CL, Moyle W, Pratt J, De Vries SM. Effect of maternal confidence on breastfeeding duration: an application of breastfeeding self-efficacy theory.Birth. 2002;29(4):278–284 26. Heinig MJ, Farley K. Development of
effec-tive strategies to support breastfeeding.J Hum Lact. 2001;17(4):293–294
27. Kingston D, Dennis CL, Sword W. Exploring breast-feeding self-efficacy.J Perinat Neo-natal Nurs. 2007;21(3):207–215
28. McCarter-Spaulding DE, Dennis CL. Psy-chometric testing of the breastfeeding self-efficacy scale-short form in a sample of black women in the United States.Res Nurs Health. 2010;33(2):111–119
29. Nichols J, Schutte NS, Brown RF, Dennis CL, Price I. The impact of a self-efficacy in-tervention on short-term breast-feeding outcomes. Health Educ Behav. 2009;36(2): 250–258
30. Cardosa LO, Vicente AS, Damião JJ, Rito RV. The impact of implementation of the breastfeeding friendly primary care initia-tive on the prevalence rates of breast-feeding and causes of consultations at a basic healthcare center.J Pediatr (Rio J). 2008;84(2):147–153
31. Centers for Disease Control and Pre-vention. Breastfeeding among US children
born 1999–2007, CDC national immuniza-tion survey. Atlanta, GA: Centers for Disease Control and Prevention; 2010. Available at: www.cdc.gov/breastfeeding/pdf/Breastfeeding ReportCard2010.pdf
32. Wellstart International. Wellstart’s lactation management self-study modules, level 1. 3rd ed. Available at: www.wellstart.org/
33. International Lactation Consultant Associa-tion. Clinician’s breastfeeding triage tool, 2007. Available at: www.ilca.org/files/resources/ HealthCareProviders/BREASTFEEDING%20 TRIAGE-references-Rev2.pdf
34. Massachusetts Breastfeeding Coalition. Ap-proach to early breastfeeding: a guideline for healthy term newborns, 48 hours to 2 weeks. Available at: http://massbreastfeeding. org/providers/earlyBF.html.
35. American Academy of Pediatrics. Support-ing breastfeedSupport-ing and lactation: the pri-mary care pediatrician’s guide to getting paid. Available at: http://www2.aap.org/ breastfeeding/files/pdf/coding.pdf
36. Geraghty SR, Riddle SW, Shaikh U. The breastfeeding mother and the pediatrician.
J Hum Lact. 2008;24(3):335–339
37. Forster DA, McLachlan HL, Lumley J. Fac-tors associated with breastfeeding at six months postpartum in a group of Australian women.Int Breastfeed J.2006; 1:18
38. Hörnell A, Hofvander Y, Kylberg E. Solids and formula: association with pattern and duration of breastfeeding.Pediatrics. 2001; 107(3):1–8. Available at: www.pediatrics. org/cgi/content/full/107/3/E38
39. Dewey KG, Nommsen-Rivers LA, Heinig MJ, Cohen RJ. Risk factors for suboptimal in-fant breastfeeding behavior, delayed on-set of lactation, and excess neonatal weight loss.Pediatrics. 2003;112(3 pt 1): 607–619
40. Kronborg H, Vaeth M. The influence of psychological factors on the duration of breastfeeding.Scand J Public Health. 2004; 32(3):201–216
41. McQueen KA, Dennis CL, Stremler R, Norman CD. A pilot randomized controlled trial of a breastfeeding self-efficacy intervention with primiparous mothers.J Obstet Gynecol Neo-natal Nurs. 2011;40(1):35–46
42. Declercq E, Labbok MH, Sakala C, O’Hara MA. Hospital practices and women’s likeli-hood of fulfilling their intention to exclu-sively breastfeed.Am J Public Health. 2009; 99(5):929–935
44. Thulier D, Mercer J. Variables associated with breastfeeding duration. J Obstet Gynecol Neonatal Nurs. 2009;38(3):259–268 45. Duijts L, Jaddoe VW, Hofman A, Moll HA. Prolonged and exclusive breastfeeding reduces the risk of infectious diseases in infancy.Pediatrics. 2010;126(1):18–26 46. Ip S, Chung M, Raman G, et al; Tufts-New
England Medical Center Evidence-based Practice Center. Breastfeeding and mater-nal and infant health outcomes in de-veloped countries.Evid RepTechnol. 2007; 153(153):1–186
47. Hauck FR, Thompson JM, Tanabe KO, Moon RY, Vennemann MM. Breastfeeding and
reduced risk of sudden infant death syn-drome: a meta-analysis.Pediatrics. 2011;128 (1):103–110
48. Grummer-Strawn LM, Mei Z; Centers for Disease Control and Prevention Pediat-ric Nutrition Surveillance System. Does breastfeeding protect against pediatric overweight? Analysis of longitudinal data from the Centers for Disease Control and Prevention Pediatric Nutrition Surveil-lance System. Pediatrics. 2004;113(2). Available at: www.pediatrics.org/cgi/con-tent/full/113/2/e81
49. Strathearn L, Mamun AA, Najman JM, O’Callaghan MJ. Does breastfeeding protect
against substantiated child abuse and ne-glect? A 15-year cohort study. Pediatrics. 2009;123(2):483–493
50. Bartick M, Reinhold A. The burden of sub-optimal breastfeeding in the United States: a pediatric cost analysis.Pediatrics. 2010; 125(5). Available at: www.pediatrics.org/ cgi/content/full/125/5/e1048
51. Stuebe AM, Schwarz EB. The risks and benefits of infant feeding practices for women and their children. J Perinatol. 2010;30(3):155–162
52. Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Data-base Syst Rev. 2002;(1):CD003517
HEARING LOSS AND CEREBRAL QUIET:Among the elderly, hearing loss is very common. Nearly 66% of Americans over the age of 70 are hearing impaired. New evidence indicates that hearing loss might lead to declines in other health measures. As reported by CNN (Health: January 22, 2013), a new study shows an association between hearing loss and the rate at which aging individuals ex-perience cognitive and memory decline. Researchers followed approximately 2,000 older adults with normal cognitive and memory function and performed audiometric, cognitive, and memory assessments at time of entry and then three, five, and six years later. Those with hearing impairment experienced significantly faster rates of cognitive decline. Moreover, the study showed greater cognitive and memory decline in those with increasingly severe hearing loss. Researchers theorize that the connection between hearing loss and cognitive decline may result from increased social isolation, a state associated with cognitive decline. Alternatively, there is the theory that the brain may devote additional cognitive resources in its attempt to remedy hearing loss or that the biologic mechanism of hearing loss might also be responsible for changes in cognition. Regardless of the underlying cause of this connection, further research should be done to learn if moderating hearing loss can aid in the prevention of impaired cognition.
DOI: 10.1542/peds.2012-1310 originally published online April 1, 2013;
2013;131;942
Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/131/5/942
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/131/5/942#BIBL
This article cites 37 articles, 9 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/breastfeeding_sub
Breastfeeding
http://www.aappublications.org/cgi/collection/nutrition_sub
Nutrition
http://www.aappublications.org/cgi/collection/standard_of_care_sub
Standard of Care
sub
http://www.aappublications.org/cgi/collection/quality_improvement_
Quality Improvement
e_management_sub
http://www.aappublications.org/cgi/collection/administration:practic
Administration/Practice Management
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2012-1310 originally published online April 1, 2013;
2013;131;942
Pediatrics
Sharon K. Corriveau, Emily E. Drake, Ann L. Kellams and Virginia G. Rovnyak
Evaluation of an Office Protocol to Increase Exclusivity of Breastfeeding
http://pediatrics.aappublications.org/content/131/5/942
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.