P. Anitha, et al. J Sci Res Pharm, 2019;8(3):16-21 World Inventia Publishers
Journal of Scientific Research in Pharmacy
http://www.jsrponline.com/Vol. 8, Issue 3, 2019 ISSN: 2277-9469 USA CODEN: JSRPCJ
Research Article
A NEW STABILITY-INDICATING UPLC METHOD DEVELOPMENT AND VALIDATION FOR DETERMINATION OF SOFOSBUVIR AND SIMEPREVIR IN BULK AND PHARMACEUTICAL DOSAGE FORM
P. Anitha *, K. Suhita Sindu, V. Amitha, Jane Violet Parnell, A. Vamshi Krishna, Dr. J.V.C. Sharma Department of Pharmaceutical Analysis, Joginpally B.R. Pharmacy College, Moinabad, Rangareddy, Telangana, INDIA.
Received on: 28-02-2019; Revised and Accepted on: 15-03-2019
ABSTRACT
A
simple, specific, accurate and economic stability indicating Ultra Performance Liquid Chromatography method was developed and validated for the combination therapy which is used in the treatment of hepatitis C named Sofosbuvir and Simeprevir. The method has shown adequate separation of Sofosbuvir and Simeprevir from their degradation products. The separation was achieved on a Hibar C18, 100 × 2.1 mm, 1.7µm column. In UPLC, the sample analyte was resolved by taking the mobile phase as a mixture of 0.1% Formic acid: Acetonitrile (70:30 v/v) in isocratic mode of elution and the flow rate is set to 0.3ml/min and the column oven temperature is maintained at 30oC. The detection was carried out at 260 nm. The retention time of Sofosbuvir and Simeprevirwere found to be 1.282 min and 0.550 min respectively. The developed UPLC method was validated according to the current International Conference on Harmonization (ICH) guidelines for specificity, LOD, LOQ, linearity, accuracy, precision, intermediate precision and robustness. The results of the study showed that the proposed UPLC method is simple, rapid, precise and accurate, which is useful for the routine analysis of Simeprevir and Sofosbuvir in bulk drug and in its pharmaceutical dosage form.
KEYWORDS: Stability Study, UPLC, Method Development, Validation, Sofosbuvir and Simeprevir.
INTRODUCTION
H
epatitis C virus was found to be a commonly attacking disease to human beings and was increased day by day. The literature reveals that 72% of the patients were suffered from chronic HCV. In early stage 75% to 85% of the liver is persisted with the virus. These defects have been treated by use of an oral form of these combinational drugs respectively. The United States Food & Drug Administration has approved the combination of Simeprevir and Sofosbuvir for the treatment of hepatitis C.Sofosbuvir is a nucleotide analog and it works by inhibiting the enzyme NS5B polymerase viral protein which is responsible for RNA polymerase that performs the replication process and hence it works by preventing hepatitis C virus (HCV) to replicate itself by inhibiting the RNA polymerase which is used for treating the chronic hepatitis C infection as a combination therapy. The IUPAC name of Sofosbuvir is S)-Isopropyl-2-((S)-(((2R,3R,4R,5R)-5-(2,4-dioxo-3,4-dihydro
*Corresponding author: P. Anitha
Department of Pharmaceutical Analysis, Joginpally B.R. Pharmacy College,
Moinabad, Rangareddy, Telangana, INDIA. * E-Mail: [email protected]
DOI: https://doi.org/10.5281/zenodo.2594759
pyrimidin-1(2H)-yl)-4-fluoro-3-hydroxy-4-methyl tetrahydro furan-2-yl) methoxy)- (phenoxy)phosphorylamino)propanoate with molecular formula of C22H29FN3O9P and its molecular
weight is 529.45.
Simeprevir is a direct acting anti-viral agent which inhibits NS3/4A protease, thus preventing viral maturation through inhibition of protein synthesis, Genotype 1, most prevailing form of hepatitis C virus (HCV) which includes peg interferon-alfa and ribavirin. The IUPAC name of Simeprevir is (1R,4R,6R,7Z,15R)-N-(cyclopropanesulfonyl)-17-({7-methoxy-8 methyl2[4(propan2yl)1,3thiazol2yl]quinolin4yl}oxy) -13-methyl-2,14-dioxo-3,13diazatricyclooctadec-7-ene-4-carbox amide. It contains a molecular formula of C38H47N5O7S2 and with
molecular weight 749.942g/mol.
Fig. 1: Structure of Sofosbuvir
Fig. 2: Structure of Simeprevir
EXPERIMENTAL WORK
Reagents and Chemicals Used:
The Sofosbuvir and Simeprevir pure drugs (API) were obtained as gift samples and the combination Sofosbuvir and Simeprevir tablets (Olysio and Sovaldi) were purchased from the local pharmacy, distilled Water, Acetonitrile, formic acid.
Instruments used:
Electronics Balance-Denver, pH meter-BVK
enterprises, India, Ultrasonicator-BVK enterprises, Acquity UPLC SYSTEM equipped with quaternary pumps, ACQUITY TUV detector and Auto sampler integrated with Empower 2 Software.UV-VIS spectrophotometer PG Instruments T60 with special bandwidth of 2 mm and 10mm and matched quartz cells integrated with UV win 6 Software was used for measuring absorbances of Simeprevir and Sofosbuvir solutions.
Solution preparations:
Diluent: Based up on the solubility of the drugs, diluent was
selected, Acetonitrile and Water taken in the ratio of 50:50
Preparation of Standard stock solutions: Accurately weighed
15 mg of Simeprevir, 40 mg of Sofosbuvir and transferred to individual 25 ml volumetric flasks separately. 3/4th of diluents was added to both of these flasks and sonicated for 10 minutes. Flasks were made up with diluents and labeled as Standard stock solution 1and 2 (600µg/ml of Simeprevir and 1600µg/ml of Sofosbuvir).
Preparation of Standard working solutions (100% solution):
1ml from each stock solution was pipetted out and taken into a 10ml volumetric flask and made up with diluent (60µg/ml Simeprevir of and 160µg/ml of Sofosbuvir).
Preparation of Sample stock solutions: 20 tablets were
weighed and the average weight of each tablet was calculated, then the weight equivalent to 1 tablet was transferred into a 100 ml volumetric flask, 50ml of diluents was added and
sonicated for 25 min, further the volume was made up with diluent and filtered (1500µg/ml of Simeprevir and 4000µg/ml of Sofosbuvir).
Preparation of Sample working solutions (100% solution):
0.4ml of filtered sample stock solution was transferred to 10ml volumetric flask and made up with diluent. (60µg/ml of Simeprevir and 160µg/ml of Sofosbuvir).
Preparation of Mobile phase: Prepare a degassed mixture of
1% Formic acid and acetonitrile in the ratio of 70:30 v/v.
UPLC Method Development:
The UPLC method of Sofosbuvir and Simeprevir was performed by several trials for various parameters like different columns, flow rates, and mobile phases, finally the following Chromatographic conditions were set and method was optimized.
Chromatographic conditions: Hibar C18 (2.1 x 100mm, 1.7µm
particle size) was used as a stationary phase maintained at 30°C. The mobile phase involved a variable composition of % Formic acid and Acetonitrile in the ratio of 70:30, delivered at a flow rate of 0.3mL/min. The optimum wavelength selected was 260 nm which represents the wavelength of maximum response for determination of combinational drugs Simeprevir and Sofosbuvir. The stressed samples were analyzed using a PDA detector covering the range of 200-400nm. Refer Table-1
Validation Parameters: System suitability:
The system suitability parameters were determined by preparing standard solutions of Simeprevir (60ppm) and Sofosbuvir (160ppm) and the solutions were injected six times and the parameters like peak tailing, resolution and USP plate count were determined. Refer Table-2
Acceptance criteria: The % RSD for the area of six standard
injections results should not be more than 2%.
Linearity:
Accurately weighed 15 mg of Simeprevir, 40 mg of Sofosbuvir and transferred to individual 25 ml volumetric flasks separately. 3/4 th of diluents was added to both of these flasks and sonicated for 10 minutes. Flasks were made up with diluents and labeled as Standard stock solution 1and 2. (600µg/ml of Simeprevir and 1600µg/ml of Sofosbuvir). From the standard stock solutions different concentrations were prepared accordingly for Simeprevir 15-90µg/ml and 40-240µg/ml for Sofosbuvir. Refer Table-3 and Fig 3-4.
Acceptance criteria: Correlation coefficient r2 ≥ 0.999.
Accuracy:
Accuracy is the method which can be determined by Recovery studies. Assay of drug was conducted in triplicate as per test method with equal amount of Sofosbuvir and Simeprevir into each volumetric flask for each spiked level to obtain the concentrations of 50%, 100%, 150% of the labelled amount. Refer Table 4-5.
Acceptance criteria: The %Recovery of Sofosbuvir and
Precision:
Precision can be defined as “The degree of agreement among individual test results when the procedure is applied repeatedly to multiple samplings of a homogenous sample”. Accurately weighed 15 mg of Simeprevir, 40 mg of Sofosbuvir and transferred to individual 25 ml volumetric flasks separately. 3/4 th of diluents was added to both of these flasks and sonicated for 10 minutes. Flasks were made up with diluents and labeled as Standard stock solution 1 and 2 (600µg/ml of Simeprevir and 1600µg/ml of Sofosbuvir). Refer Table-6.
Limit of Detection:
The detection limit of an individual analytical procedure is the lowest amount of analyte in a sample which can be detected but not necessarily quantitated as an exact value. 0.25ml each from two standard stock solutions was pipetted out and transferred to two separate 10ml volumetric flasks and made up with diluents. From the above solutions 0.1ml each of Simeprevir and Sofosbuvir solutions respectively were transferred to 10ml volumetric flasks and made up with the same diluents. Refer Table-6
Limit of Quantitation:
The quantitation limit of an individual analytical procedure is the lowest amount of analyte in a sample which can be quantitatively determined. 0.25ml each from two standard stock solutions was pipetted out and transferred to two separate 10ml volumetric flask and made up with diluent. From the above solutions 0.3ml each of Simeprevir, Sofosbuvir, and solutions respectively were transferred to 10ml volumetric flasks and made up with the same diluent. Refer Table-6-8
Robustness:
The concept of robustness of an analytical procedure has been defined by the ICH as “a measure of its capacity to remain unaffected by small, but deliberate variations in method parameters”. The robustness of the assay method was established by introducing small changes in the chromatographic condition which included wavelength (225 nm–229 nm), flow rate (0.8 and 1.2 mL/min) and organic phase (+5% to −5%). The results were tabulated in Table 9.
Forced degradation/ stability studies:
Forced degradation studies include the degradation of drug substance and drug product at conditions more severe than accelerated conditions. These studies illustrate the chemical stability of the molecule which further facilitates the development of stable formulation with suitable storage conditions. Multiple stressed samples were prepared as indicated below. They were chromatographed along with a non-stressed sample. Hydrolytic conditions: acid, base, peroxide, thermal, photolytic and humidity induced degradation. For stress degradation analysis, Simeprevir and of Sofosbuvir was treated with 0.05M HCl (acid stress), 0.05M NaOH (alkaline stress) for 5 min on bench top, 1% v/v Hydrogen peroxide (oxidative stress), 85o C for 24 h (thermal stress). Samples for
photolytic stress are placed in white fluorescent light, 1.2 million Lux hours and UV light, 200 watt-hours for 24 h and finally for 90% RH at 25o c at 72 hours . Samples are then
injected for analysis. The results of analysis are then compared with similarly prepared fresh samples. The results were tabulated in Table 10.
RESULTS AND DISCUSSION
Optimized method:
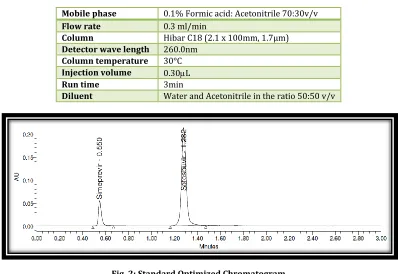
Table No. 1: Chromatographic conditions
Mobile phase 0.1% Formic acid: Acetonitrile 70:30v/v
Flow rate 0.3ml/min
Column Hibar C18 (2.1 x 100mm, 1.7µm)
Detector wave length 260.0nm
Column temperature 30°C
Injection volume 0.30L
Run time 3min
Diluent Water and Acetonitrile in the ratio 50:50 v/v
Fig. 2: Standard Optimized Chromatogram
Observation: Sofosbuvir and Simeprevir were eluted at 0.550 min and 1.282 min respectively with good resolution. Plate count and tailing factor was very
Table No. 2: System suitability parameters for Simeprevir and Sofosbuvir
S. No. Simeprevir Sofosbuvir
Inj RT (min) USP Plate Count Tailing RT (min) USP Plate Count Tailing
1 0.548 2315 1.37 1.273 5507 1.07
2 0.549 2297 1.39 1.278 5536 1.07
3 0.550 2269 1.39 1.278 5570 1.08
4 0.550 2303 1.40 1.279 5467 1.08
5 0.550 2270 1.42 1.279 5563 1.09
6 0.550 2298 1.39 1.282 5491 1.07
Observation: According to ICH guidelines plate count should be more than 2000, tailing factor should be less than 2 and resolution must be more than 2.
All the system suitable parameters were passed and were within the limits.
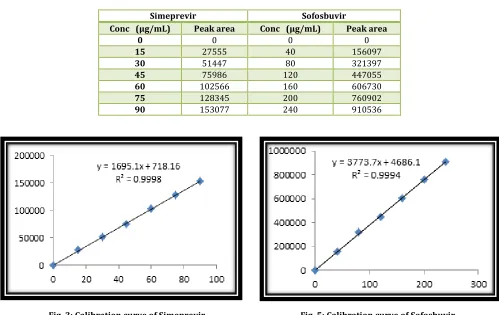
Table No. 3: Linearity table for Simeprevir and Sofosbuvir
Simeprevir Sofosbuvir
Conc (μg/mL) Peak area Conc (μg/mL) Peak area
0 0 0 0
15 27555 40 156097
30 51447 80 321397
45 75986 120 447055
60 102566 160 606730
75 128345 200 760902
90 153077 240 910536
Fig. 3: Calibration curve of Simeprevir Fig. 5: Calibration curve of Sofosbuvir
Discussion: Six linear concentrations of Simeprevir (15-90µg/ml) and Sofosbuvir (40-240µg/ml) were injected in a duplicate manner. Average areas were
mentioned above and linearity equations obtained for Simeprevir was y = 1695.x + 718.1 and of Sofosbuvir was y = 3773.x + 4686. Correlation coefficient obtained was 0.999 for the two drugs.
Table No. 4: Accuracy table of Simeprevir
% Level Amount Spiked(μg/mL) Amount recovered(μg/mL) % Recovery Mean %Recovery
50% 30 29.92 99.72
99.66%
30 30.23 100.78
30 29.96 99.88
100% 60 60 59.91 59.46 99.85 99.09
60 59.19 98.64
150% 90 90 89.51 89.23 99.46 99.14
Table No. 5: Accuracy table of Sofosbuvir
% Level Amount Spiked(μg/mL) Amount recovered(μg/mL) % Recovery Mean %Recovery
50% 80 79.93 99.91
99.55%
80 79.87 99.84
80 79.26 99.08
100% 160 160 158.67 158.54 99.17 99.09
160 159.05 99.41
150% 240 240 236.78 242.08 100.87 98.66
240 239.93 99.97
Table No 6: System precision table of Sofosbuvir and Simeprevir
S. No Area of Simeprevir Area of Sofosbuvir
1. 101411 592840
2. 100585 596467
3. 101740 594175
4. 101133 594387
5. 101227 597835
6. 100568 598851
Mean 101111 595759
S.D 462.8 2336.0
%RSD 0.5 0.4
Table No. 7: Intermediate precision table of Sofosbuvir and Simeprevir
S. No Area of Simeprevir Area of Sofosbuvir
1. 101056 601898
2. 100392 593257
3. 99932 596199
4. 100926 595076
5. 100748 593463
6. 100818 596795
Mean 100645 596115
S.D 414.9 3168.4
%RSD 0.4 0.5
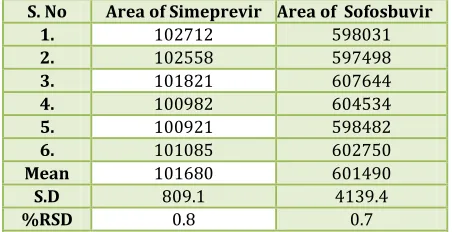
Table No. 8: Repeatability table of Sofosbuvir and Simeprevir
S. No Area of Simeprevir Area of Sofosbuvir
1. 102712 598031
2. 102558 597498
3. 101821 607644
4. 100982 604534
5. 100921 598482
6. 101085 602750
Mean 101680 601490
S.D 809.1 4139.4
%RSD 0.8 0.7
Table No. 9:Robustness data for Sofosbuvir and Simeprevir
S. No. Condition %RSD of Simeprevir %RSD of Sofosbuvir
1 Flow rate (-) 0.2ml/min 1.8 0.2
2 Flow rate (+) 0.4ml/min 1.2 0.1
3 Mobile phase (-) 55B:45A 1.1 0.1
4 Mobile phase (+) 45B:55A 0.4 0.5
5 Temperature (-) 25°C 1.5 0.3
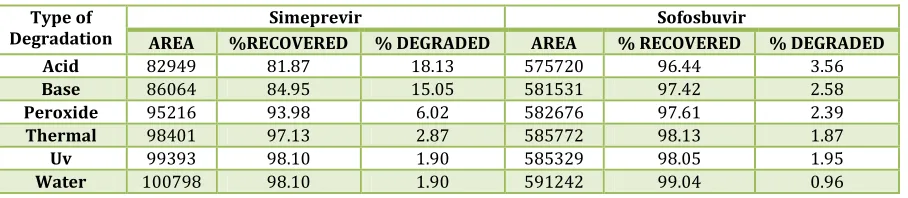
Table 10: Degradation data
Type of
Degradation AREA %RECOVERED Simeprevir % DEGRADED AREA % RECOVERED Sofosbuvir % DEGRADED
Acid 82949 81.87 18.13 575720 96.44 3.56
Base 86064 84.95 15.05 581531 97.42 2.58
Peroxide 95216 93.98 6.02 582676 97.61 2.39
Thermal 98401 97.13 2.87 585772 98.13 1.87
Uv 99393 98.10 1.90 585329 98.05 1.95
Water 100798 98.10 1.90 591242 99.04 0.96
CONCLUSION
A
simple, Accurate, precise method was developed for the simultaneous estimation of the Simeprevir and Sofosbuvir in Tablet dosage form. Retention time of Simeprevir and Sofosbuvir were found to be 0.550min and 1.282min. %RSD of the Simeprevir and Sofosbuvir were and found to be 0.5 and 0.4 respectively. %Recovery was obtained as 99.66% and 99.55% for Simeprevir and Sofosbuvir respectively. LOD, LOQ values obtained from regression equations of Simeprevir and Sofosbuvir were 0.42, 1.27 and 0.07, 0.21 respectively. Regression equation of Simeprevir is y = 1695.x + 718.1, and y = 3773.x + 4686. of Sofosbuvir. Retention times were decreased and that run time was decreased, so the method developed was simple and economical that can be adopted in regular Quality control test in Industries.ACKNOWLEDGEMENT
W
e are very much thankful to Joginpally B.R. Pharmacy College, Hyderabad, for giving permission to carry out our research work.REFERENCES:
1. Sofosbuvir: https://www.drugbank.ca/drugs/DB08934. 2. Simeprevir: https://www.drugbank.ca/drugs/DB06290. 3. International Conference on Harmonization (1994)
Validation of analytical procedures, text and methodology Q2 (R1), November 2005.
4. ICH. Stability testing of new drug substances and products Q1A (R2), IFPMA, Geneva, Switzerland, 2003. 5. S. Roopa Rani, Dr. S. Shobha rani. J Pharm Res
2017;6(2):70-76.
6. B. Raj Kumar, Dr. KV. Subrahmanyam. Indo Am J Pharm Res 2016;6(02).
7. Khedkar PM, Mhajan PM, Sawant SD. Int J Pharm Res Rev
2017;6(3):1-4.
8. Hamd MA, Marzouk AA. J App Pharm Sci 2017 ;2:114-119.
9. Mansour FR. Spectrochim Acta A Mol Biomol Spectrosc
2018;188:626-632.
10. Mohan VP, Satyanarayana T. J Global Trends Pharm Sci
2016;7(1):3013-3015.
11. Khalid AM, Attia Nasar M. El-Abasawi, Ahmed El-Olemy, Ahmed Serag. Anal Chem lett 2017;7(1):43-51.
How to cite this article:
P. Anitha et al. A NEW STABILITY-INDICATING UPLC METHOD DEVELOPMENT AND VALIDATION FOR DETERMINATION OF SOFOSBUVIR AND SIMEPREVIR IN BULK AND PHARMACEUTICAL DOSAGE FORM. J Sci Res Pharm 2019;8(3):16-21.
DOI: https://doi.org/10.5281/zenodo.2594759
Conflict of interest: The authors have declared that no conflict of interest exists.