Introduction
The pastO
ver the past five decades, improvements in the sensitivity and specificity of thyroid test methodologies have dramatically impacted the clinical strategies for detecting and treating thyroid disorders. In the 1950s, only one thyroid test was available - an indirect estimate of the serum total (free + protein-bound) thyroxine (TT4) concentration, using the protein bound iodine (PBI) technique. Since 1970, technological advances in radioimmunoassay (rIA) and immunometric assay (IMA) methodologies have progressively improved the specificity and sensitivity of the methods.The present scenario
Currently, thyroid testing is performed on serum specimens
using either manual or automated methods employing specific
antibodies. Methodology is still evolving as performance standards are established by the professional organizations and new technology and instruments are developed by manufacturers. A multitude of tests are currently available for testing thyroid function:
• Serum-based methods are available for measuring both total
(TT4 and TT3) and free (FT4 and FT3) thyroid hormone concentrations.
• In addition, measurements can be made of the thyroid
hormone binding proteins, Thyroxine Binding globulin (TBG), Transthyretin (TTR)/Prealbumin (TBPA) and Albumin, as well as for the pituitary thyroid stimulator, thyrotropin (thyroid stimulating hormone, TSH) and the thyroid hormone precursor protein, Thyroglobulin (Tg).
• The recognition of autoimmunity as the leading cause
of thyroid dysfunction, has led to the development and incorporation of tests to determine thyroid autoantibodies – thyroid peroxidise antibodies (TPOAb), thyroglobulin antibodies (TgAb), and TSH receptor antibodies (TRAb). The current review will cover the current status and limitations of the thyroid testing methods most commonly
used in clinical practice and as recommended by the global and Indian guidelines.1
The Value of Laboratory Testing in
Thyroid Diseases
The value of clinical diagnosis in thyroid dysfunction is limited because clinical manifestations of the disease vary considerably; patients may present with diverse characteristics of
the disease along with differing severity levels and non-specific
signs and symptoms. Physicians do consider and rule out thyroid dysfunction more frequently than they establish a diagnosis of thyroid disorder. Considering this scenario, many patients with thyroid disorders will remain undiagnosed if laboratory evaluation of only those patients with clearly suggestive signs and symptoms of thyroid dysfunction is performed. It, therefore, becomes imperative to implement routine laboratory screening to identify such patients, so that appropriate treatment for thyroid disorders can be instituted or conservative monitoring carried out to anticipate potential future consequences. Reference values of laboratory tests of thyroid function (Table 1).
The enhanced sensitivity and specificity of TSH assays have
greatly improved the assessment of thyroid function tests. Since TSH levels change dynamically in response to the alterations of T3 and T4, the approach to evaluate whether the patient has
thyroid disorder is to test the TSH levels first. The sensitive
immunoradiometric assays (IRMA) for TSH are sensitive enough to distinguish between the lower limit of the reference range or suppressed values of TSH that are seen in thyrotoxicosis. Extremely sensitive TSH assays are now available; the 4th/5th generation assays can detect TSH levels as low as 0≤0.004mU/L. However, for practical purposes, TSH values of ≤ 0.1mU/L are considered sufficient. If TSH levels are found to be abnormal,
then circulating T3 and T4 levels should be estimated. Although radioimmuno assays are widely available to measure total T3 and T4, these are highly protein bound and several factors can
influence their levels. Hence it is important to measure free or
unbound T3 and T4 levels. Testing for thyroid dysfunction
TSH is the first test to perform serum TSH level remains the
single best test of thyroid function. Thyroid-stimulating hormone testing is the preferred approach because:
1. TSH is central to the negative-feedback system
2. Small changes in serum thyroid function cause logarithmic
amplification in TSH secretion
3. The most advanced (third-generation) chemiluminescent
TSH assays can now detect both elevation and significant
lowering of TSH levels, and are capable of reliably measuring values <0.1mU/L, thus aiding detection of subclinical thyrotoxicosis.
A normal TSH value is a sufficient indicator to stop further
testing of thyroid function in most cases. However, in cases suggestive of possible hypothalamic pituitary disease (central), a free-T4 level estimation is desirable. In such patients, TSH levels may not reliably indicate the regulation of T4 replacement, and,
Laboratory Evaluation of Thyroid Function
Shashank R Joshi
Department of Endocrinology, Grant Medical College and Sir JJ Group of Hospitals, Endocrinologist, Lilavati and Bhatia Hospital, Mumbai.
Table 1 : Reference values of thyroid function test
Test Range TSH 0.5 -4.7mU/L T3 0.92-2.78nmol/L FT3 0.22-6.78 pmol/L T4 58-140 nmol/L FT4 10.3-35pmol/L Note
• Where possible manufacturers reference ranges should be confirmed locally using an adequate population size of at least 120 ambulatory subjects.
• For TSH, reference ranges should be established using specimens collected between 0800h and 1800h and using 95% confidence limits from log transformed data.
• Since TSH, free and total thyroid hormones change during pregnancy, trimester related reference ranges should be available with data generated locally or contrywise.2
therefore, may require estimation of free T4 levels. 1
TSH testing should be commonly carried out in the following
settings:
• In patients presenting with suspected goitres: Serum TSH levels must be measured.
• As screening for congenital hypothyroidism: A heel-prick blood specimen is used for determining serum TSH levels. This is an established screening test for congenital hypothyroidism and has been adopted as a routine screening measure in many countries. The practice of routine screening for congenital hypothyroidism by the TSH test should be more
widely adopted and continued. The low cost filterpaper TSH
methods will be available in India soon.
• In patients with atrial fibrillation, dyslipidaemia, osteoporosis, and infertility: Serum TSH levels should be measured at presentation.
As screening for thyroid disorders in patients with unclear diagnoses: Serum TSH test should be carried out in all patients
who have non-specific manifestations, are asymptomatic, and
in whom the diagnosis is not clear. The high-sensitivity TSH test should be performed in such cases (where there’s a low pre-test probability of the disease). The advantage of this test is that its negative predictive value is very high and a vast majority of the results come out negative. Measurement of serum TSH
alone can suffice during sequential follow-up visits (after the first investigation has been carried out) in patients who have
not received treatment for thyroid disorders and for those who may be at risk of developing thyroid dysfunction.
Important considerations for the clinician if TSH is abnormal (Table 2)
• In patients with abnormal TSH concentrations, a focused
history, physical examination (in particular thyroid gland examination), repeat TSH test, serum T3 and T4 level determination and occasionally imaging studies need to be carried out.
• It is not uncommon to see that many patients with high
TSH values are informed that they need to take thyroid medication life-long and after having been prescribed T4, no further workup or explanation is undertaken.
• In patients with goitrous changes or the presence of thyroid
nodules, TSH concentration may be in the normal range because of an unaltered thyroid function. This warrants
complete patient evaluation including testing for
anti-thyroid antibodies, imaging ultrasound and fine-needle
aspiration cytology.
• In patients whose TSH levels are abnormal, T3 and T4 levels should be determined. Free T3 and T4 level estimation is preferred over total T3 and T4 estimation because these hormones are extensively (>99%) bound to plasma proteins and only the unbound forms are active. 3
Inappropriate TSH
This is a biochemical diagnosis in which elevation in circulating FT4 and/or FT3 is associated with an “inappropriately” detectable or elevated serum TSH concentration. If this biochemical picture is observed then assay artefact/laboratory error should
be considered first.Once the laboratory has excluded such explanations then the cause of “true” inappropriate TSH should
be considered. The differential diagnosis are a TSH secreting
pituitary tumour (TSH-oma) or a syndrome of thyroid hormone resistance. The finding of an elevated serum sex hormone binding globulin (SHBG) and circulating free a subunit may
support the diagnosis of TSH-oma, as may the finding of hyper
or hypo-secretion of other pituitary hormones. Pituitary imaging
usually confirms the diagnosis but should not be undertaken until the appropriate biochemical confirmation has been made. A syndrome of thyroid hormone resistance can be confirmed by
family history; sequencing of the β thyroid hormone receptor
confirms the diagnosis. When an ‘inappropriately’ detectable
or elevated serum TSH is found in association with elevated circulating free T3 and/or T4 concentrations, the TSH is termed
‘inappropriate’. Such cases may occur due to assay artefacts or laboratory errors and this should be considered first. However,
if on repeat determination, TSH is still found to be inappropriate, other common explanations for apparent elevation of FT4 should be considered. These include the presence of binding protein abnormalities (such as familial dysalbuminaemic hyperthyroxinaemia) or assay dependent antibody interference in the measurements of FT4, FT3 or TSH. To distinguish between TSHomas and thyroid hormone resistance, estimations of SHBG,
a subunit and other anterior pituitary hormones may be carried out.
Total T4
Several laboratories measure the total T4 and total T3 which Table 2 : Some causes of abnormal serum TSH concentrations
TSH below normal TSH above normal
• Primary hyperthyroidism • Primary hypothyroidism
• Pituitary/hypothalamic disease with central hypothyroidism (TSH
unreliable) • Pituitary thyrotroph adenoma; Pituitary resistance to thyroid hormone (central hyperthyroidism) TSH, unreliable. • Generalized thyroid hormone resistance
• Prolonged thyrotroph cell suppression after recent hyperthyroidism
in euthyroid or hypothyroid patient • Thyrotoxicosis from overly rapid correction of severe hypothyroidism with parenteral T4
• Old age • Old age
• Drugs, e.g., glucocorticoids, dopamine • Drugs, e.g., amiodarone • Problems with T4 treatment : Overdosage in treatment for fatigue or
overweight, Altered gastrointestinal absorption because of drugs or disease, Altered T4 clearance because of drugs, Patient compliance problems, Prescription error, Testing too soon after T4 dose decrease
• Problems with T4 treatment : Underdosage based on misleadingly high total T4, Altered gastrointestinal absorption because of drugs or disease, Altered T4 clearance because of drugs, Patient compliance problems, Prescription error, Testing too soon after T4 dose increase • Many severe systemic illnesses (Sick Enthyrid State) • Recovery phase after severe systemic illness (Sick Enthyrid State) • Combination of pulsatile TSH secretion and analytical precision limits• Combination of pulsatile TSH secretion and analytical precision limits
Antibody in patient serum against antibody in TSH assay, causing analytical artefact
is not a true reflection of the thyroid status of an individual.
This is because thyroid hormones circulate in the body largely in the inactive form, bound to carrier proteins (thyroid binding globulin (TBG), transthyretin and albumin) while only the small unbound fraction is metabolically active. Moreover, in some clinical conditions, particularly those in which there is an alteration of the amount of carrier proteins, the total T3 and total T4 may be elevated while the thyroid functional state (free T3 and T4 levels) may be normal. Such conditions include:
1. Hereditary abnormalities of binding proteins: These include
TBG deficiency or TBG excess, abnormal albumin levels and
abnormal transthyretin levels.
2. Acquired deficiency of binding proteins: Conditions such
as nephrotic syndrome may cause protein loss from the body. In severe liver disease, there’s impaired production of proteins, and therapy with androgens or anabolic steroids may alter the levels of carrier proteins.
3. Drug-induced alterations in T4 binding to TBG: Therapy with salicylates, phenytoin, phenylbutazone may alter T4-TBG binding.
4. Presence of T4 antibodies.
The development of newer immunoassay methods for determining free T3 and T4 has overcome many of these problems. Radioimmunoassay measurement of total serum T4
levels is highly sensitive in reflecting the hyperthyroid (85-95%)
and the hypothyroid status (80-90%) of patients.
Total T3
Currently routine measurement of serum T3 is not carried out (only T4 is measured) in patients suspected of having thyroid disorders. About 25% of patients with hypothyroidism have low normal T3 values. Free T3/ total T3 measurements, however,
should be performed in the following settings:
1. In patients suspected of having T3 thyrotoxicosis.
2. In patients taking drugs that inhibit the peripheral conversion of T4 to T3 (such as dexamethasone, propranolol, propylthiouracil, amiodarone, and iodine-containing contrast media).5
Testing both TSH and FT4
There are certain clinical situations where TSH testing must be coupled with testing the FT4 levels. Clinical situations where measurement of both serum TSH and FT4 is required are principally disorders where the pituitary-thyroid axis is not intact or is unstable. These situations include:
• Optimising thyroxine therapy in newly diagnosed patients
with hypothyroidism.
• Diagnosing and monitoring thyroid disorders in pregnancy. • Monitoring patients with hyperthyroidism in the early
months after treatment.
• Diagnosis and monitoring treatment for central
hypothyroidism.
• End-organ thyroid hormone resistance. • Sick Euthyroid State.
• TSH-secreting pituitary adenomas.
• Women with type I diabetes should have their thyroid
function, including serum TSH, FT4 and thyroid peroxidase antibody status, established preconception, at booking when pregnant and at 3 months post-partum.
• Possible subclinical hypothyroidism: If screening is
performed, and a high serum TSH concentration is found, and the FT4 is normal, the measurement should be repeated 3-6 months later, along with measurement of serum FT4, after excluding non-thyroidal illness and drug interference.
• Overtly hypothyroid patients (who have serum TSH greater
than 10 mU/L and low FT4 concentrations) should be treated with thyroxine.
In patients with a high serum TSH level and normal FT4 concentrations (possible subclinical hypothyroidism), TSH measurements and FT4 should be repeated 3 to 6 months later, after precluding non-thyroid disorders and drug interference. In cases of doubt in identifying specimens in which both serum TSH and FT4 should be carried out, it is prudent to test all specimens for TSH and FT4, rather than test for TSH alone.6
Testing TSH and FT4 and FT3
In hospital inpatient ICU: In the absence of an abnormal thyroid gland by careful physical examination, a hospital inpatient with a mild or moderate (<20mIU/L) increase in serum TSH and an estimated free T4 (by either a free-T4 test or a free-T4 index) within the health-related reference interval can usually be followed without treatment and re-evaluated later. The same holds true for a patient with a subnormal serum TSH and estimated free T4 and serum T3 values that are not increased. In both cases, the great majority of patients do nothave clinically significant thyroid disease. The responsibility of
providing pertinent clinical information to help guide the lab in selecting the most appropriate thyroid function test lies with
the requesting physician. However, if sufficient clinical details to allow the identification of patients with subnormal TSH and
unaltered T3 and T4 values, are not available, then laboratories should measure serum TSH and FT4 on all specimens. This is
a more prudent strategy than just measuring first-line serum
TSH, and then carrying out FT4 and FT3 estimations later when indicated.
Considerations which
Alter Thyroid Levels
• Binding protein abnormalities can increase totalT3 in the absence of hyperthyroidism, notably during estrogen treatment contraceptive pills, and pregnancy. If necessary, a T3-uptake test or thyroxine-binding globulin measurement can be used to calculate a free-T3 index, or a free-T3 test can be obtained to clarify an ambiguous increased total-T3 result.
• When hypothyroidism is suspected, a free-T4 estimate is appropriate because total-T3 and free-T3 tests have
inadequate sensitivity and specificity in this setting. • When hyperthyroidism is suspected, the combination
of a free-T4 estimate and a total- or free-T3 estimate provides the most complete assessment of the severity of
hyperthyroidism and identifies cases of “T3-toxicosis”, i.e. a selective increase of the serum T3 concentration.
• In some centres, free-T4 and -T3 tests are routinely used when the TSH is increased, but in others, serum T3 measurements are obtained only when the TSH is low and the free T4 is within the reference interval. It is preferable to monitor both serum free T4 and T3 in patients with low serum TSH (other than hypothyroid patients taking T4),even
after the thyroid diagnosis is known, to establish patterns
of increasing or decreasing values over time (Table 3) (Fig. 1a, b).1,3
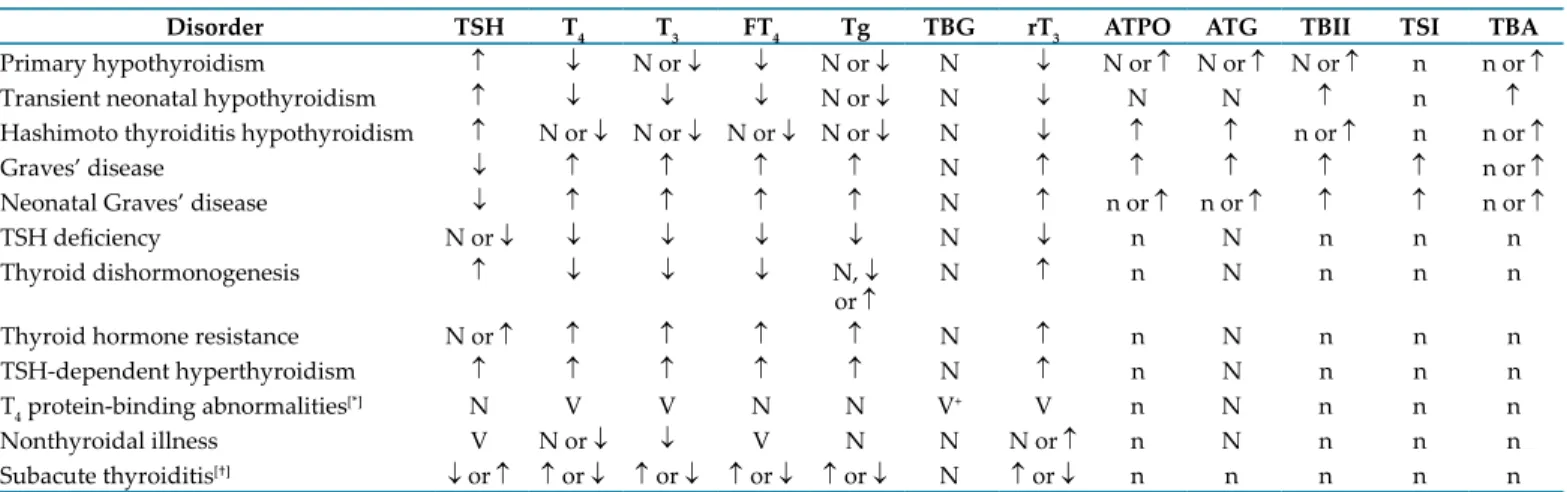
Table 3 : Characterization of thyroid disorders according to results of thyroid function tests
Disorder TSH T4 T3 FT4 Tg TBG rT3 ATPO ATG TBII TSI TBA
Primary hypothyroidism ↑ ↓ N or ↓ ↓ N or ↓ N ↓ N or ↑ N or ↑ N or ↑ n n or ↑
Transient neonatal hypothyroidism ↑ ↓ ↓ ↓ N or ↓ N ↓ N N ↑ n ↑
Hashimoto thyroiditis hypothyroidism ↑ N or ↓ N or ↓ N or ↓ N or ↓ N ↓ ↑ ↑ n or ↑ n n or ↑
Graves’ disease ↓ ↑ ↑ ↑ ↑ N ↑ ↑ ↑ ↑ ↑ n or ↑
Neonatal Graves’ disease ↓ ↑ ↑ ↑ ↑ N ↑ n or ↑ n or ↑ ↑ ↑ n or ↑
TSH deficiency N or ↓ ↓ ↓ ↓ ↓ N ↓ n N n n n
Thyroid dishormonogenesis ↑ ↓ ↓ ↓ N, ↓
or ↑ N ↑ n N n n n
Thyroid hormone resistance N or ↑ ↑ ↑ ↑ ↑ N ↑ n N n n n
TSH-dependent hyperthyroidism ↑ ↑ ↑ ↑ ↑ N ↑ n N n n n
T4 protein-binding abnormalities[*] N V V N N V+ V n N n n n
Nonthyroidal illness V N or ↓ ↓ V N N N or ↑ n N n n n
Subacute thyroiditis[†] ↓ or ↑ ↑ or ↓ ↑ or ↓ ↑ or ↓ ↑ or ↓ N ↑ or ↓ n n n n n TSH = thyroid-stimulating hormone; T4 = thyroxine; T3 = triiodothyronine; FT4 = free thyroxine; Tg = thyroglobulin; TBG = thyroxine-binding globulin; rT3 = reverse T3; ATPO = antithyroidperoxidase; ATG = antithyroglobulin; TBII = TSH-binding inhibiting immunoglobulin; TSI = thyroid-stimulating immunoglobulin; TBA = TSH receptor-blocking antibody; N = normal; n = negative; V = variable.
* The spectrum of binding protein abnormalities includes increased or decreased TBG binding, increased or decreased transthyretin binding, and ↑ albumin binding.
† Subacute thyroiditis involves a transient period of hyperthyroidism followed by a transient hypothyroid state. (Reprinted from Fisha DA (ed) : Disorders of Thyroid Function, Quest Diagnostic Manual. 3rd Editor, p 268.)
Thyroid Autoimmunity
Thyroid-specific Autoantibodies (TPOAb,
TGAb AnD TRAb)
Tests for antibodies against thyroid-specific antigens,
anti-thyroid peroxidase (TPO), thyroglobulin (Tg) and TSH receptors are used in the diagnosis of autoimmune thyroid disorders. Over
the last five decades, antibody measurement techniques have
evolved from semi-quantitative agglutination and complement
fixation tests and whole animal bioassays to specific ligand
assays using recombinant antigens and cell culture systems transfected with the human TSH receptor. Unfortunately, the diagnostic and prognostic value of these thyroid autoantibody
measurements is hampered by differences in the sensitivity and specificity of current methods. Although autoantibody tests have
inherent clinical utility in a number of clinical situations, these tests should be selectively employed.
Thyroid peroxidase autoantibodies (TPOAb)
Originally, thyroid peroxidase autoantibodies (TPOAb) were detected as thyroid microsomal antibodies by semi-quantitative
complement fixation and tanned erythrocyte hemagglutination
techniques and were labeled antimicrosomal antibodies (AMA). The principal antigen in the thyroid microsomes was recently discovered to be the thyroid peroxidase enzyme (TPO), a 100kD
glycosylated protein. Currently, automated tests are replacing the older manual agglutination tests. These new tests are more
specific TPOAb immunoassays or immunometric assay methods, and are based on purified or recombinant TPO.
Clinical Use of TPOAb Tests
An abnormal TPOAb is detected in 15 to 20 percent of “healthy” euthyroid subjects and even higher percentages of patients with various non-thyroid autoimmune disorders. Approximately 70-80 % of patients with Graves’ disease and virtually all patients with Hashimoto’s, atrophic thyroiditis or post-partum thyroiditis have TPOAb detected. In fact, TPOAb is implicated as a cytotoxic agent in the destructive thyroiditic process. TPO antibodies are involved in the tissue destructive processes associated with the hypothyroidism observed in Hashimoto’s thyroiditis (Fig. 2). In the future, TPOAb measurement may be used as a prognostic indicator for thyroid dysfunction. Although the appearance of TPOAb usually precedes the development of thyroid dysfunction, recent studies
suggest that a hypoechoic ultrasound pattern may precede a
biochemical TPOAb abnormality, as shown in Figure 2. The paradoxical absence of TPOAb in some patients with unequivocal
TSH abnormalities likely reflects the suboptimal sensitivity and/ or specificity of current TPOAb tests or non-autoimmune thyroid
failure (atrophic thyroiditis). Although changes in autoantibody
concentrations often reflect a change in disease activity, serial Primary Hypothyroidism • Subclinical Hypothyroidism • ES* • TT* • Inappropriate TSH secretion • ES • TT • ES • TT Normal • ES • TT • Central Hypothyroidism • ES • TT • Subclinical Hyperthyroidism • ES • TT Overt Hyperthyroidism High TSH Low
Low Free T4 High
* ES, euthyroid sick; TT, thyroid in transition
Fig. 1a : Thyroid Function Test Algorithm Fig. 1b : Algorithm for the Diagnosis of Thyroid Dysfunction
TSH
High Normal Low
Free T4 Free T4
Low Normal Normal High
Hypothyroidism Hyperthyroidism
thyroid autoantibody measurements are not recommended for monitoring treatment for AITD. The prevalence of TPOAb is higher in patients with non-thyroid autoimmune diseases such as type 1diabetes and pernicious anemia. Aging is also associated with higher prevalence of TPOAb that parallel the increased prevalence seen in both subclinical (mild) and clinical hypothyroidism. A euthyroid subject with detectable TPOAb is at increased risk of development of hypothyroidism. Detectable level of TPOAb typically precedes the development of an elevated TSH and is therefore a risk factor for hypothyroidism. Moreover, reproductive complications (such as miscarriage, infertility, IVF failure, fetal death, pre-eclampsia, preterm delivery and post-partum thyroiditis and depression) have been associated with the presence of TPOAb. The enhanced sensitivity
and specificity of the TPO immunoassay methods make them a more cost-effective option over the older semi-quantitative AMA
agglutination tests, since they obviate the need for additional TgAb measurements in the routine diagnosis of autoimmune thyroid disorders.7
Thyroglobulin autoantibodies (TgAb)
Antithyroglobulin autoantibodies (TgAb) were the first thyroid antibodies to be recognized to circulate in
patients with autoimmune thyroid disorders. The first TgAb
methods were based on tanned red cell hemagglutination. Subsequently, methodologies have evolved in parallel with TPOAb methodology from semi-quantitative techniques, to more sensitive ELISA and RIA methods and more recently chemiluminescent immunoassays. Unfortunately, the inter-method variability of current TgAb assays is even greater than that of the TPOAb tests discussed above.
Clinical Use of TgAb Tests
Auto antibodies against Tg are encountered in autoimmune thyroid conditions, usually in association with TPOAb. However, the recent NHANES III study found that 3 % of subjects with no risk factors for thyroid disease had detectable TgAb without TPOAb. In these subjects with only TgAb detected, no association with TSH abnormalities was found so that the
clinical significance of an isolated TgAb abnormality remains to
be established. This suggests that it is unnecessary to measure
both TPOAb and TgAb for a routine evaluation of thyroid autoimmunity. According to the current guidelines, all sera should be prescreened for TgAb by a sensitive immunoassay method prior to Tg testing. Therefore, TgAb is primarily used as an adjunct test for serum Tg estimation. TgAb is detected
in approximately 20% of patients with differentiated thyroid
carcinoma compared with 10% of normal subjects by the immunoassay methods. The threshold TgAb concentration above normal that precludes TgAb interference is either not known or does not appear to exist. False positives may occur due to assay artifacts or illegitimate transcription while false negatives results may be seen in patients with metastatic disease.
TSH receptor autoantibodies (TRAb)
TSH Receptor Antibodies (TRAb) were first recognized as
long-acting thyroid stimulator (LATS) using mouse bioassays. These autoantibodies are directed against epitopes on the ectodomain of the TSH receptor. Methods for measuring TRAb are even more varied than for TPOAb and TgAb. Two classes of TRAb can be associated with autoimmune thyroid disorders – (a) thyroid stimulating autoantibodies (TSAb) that cause Graves’ hyperthyroidism and (b) thyroid stimulation-blocking antibodies (TBAb) which block receptor binding of TSH. Each class of TRAb (TSAb and TBAb) may be detected alone or in combination in Graves’ disease and Hashimoto’s thyroiditis. The relative concentrations of the two classes of TRAb may modulate the severity of Graves’ hyperthyroidism and may change in response to therapy or pregnancy.
Clinical Use of TRAb Tests
TRAb tests are used in the differential diagnosis of hyperthyroidism, the prediction of fetal and neonatal thyroid dysfunction due to transplacental passage of maternal TRAb and prediction of the course of Graves’ disease treated with antithyroid drugs. Although TBII assays do not directly measure the stimulating antibodies, these tests have comparable diagnostic sensitivity to TSAb bioassays (70-95%) for diagnosing Graves’ hyperthyroidism or detecting a relapse or response to therapy. The second generation assays employing human recombinant TSH receptor are now becoming available and are reported to have superior diagnostic sensitivity for Graves’ disease. Current tests are manual and expensive and vary in
precision, sensitivity, specificity and reference ranges. However,
the TBII tests are important for evaluating pregnant patients with a history of autoimmune thyroid disease, in whom there is a risk of transplacental passage of TRAb to the infant . The
lack of specificity of the TBII methods is actually an advantage
in this clinical situation, since a TBII test will detect both the stimulating and blocking classes of TRAb that can produce transient hyper- or hypothyroidism, respectively, in the fetus and newborn. TRAb plays an uncertain role in thyroid-associated ophthalmopathy (TAO), which appears to be exacerbated by radioiodine therapy. Since TRAb and other thyroid antibodies
levels increase acutely significantly after radioiodine therapy,
a TRAb measurement prior to radioiodine therapy may be useful to predict risk of TAO. However, prospective studies are needed to establish the clinical utility of TRAb measurement in this context. Patients with very high circulating concentrations of hCG due to choriocarcinoma or hydatiform mole, as well as a small number of pregnant patients, may have misleading positive results using TSAb assays.
Thyroglobulin (Tg) methods
Serum Tg measurement is used as a tumor marker in the
Fig. 2 : Thyroid Autoantibody Prevalence and Associations with Hypothyroidism (Reprinted from Hollowell JG, Staehling NW, Hannon WH, Flanders WD, Gunter EW, Spencer CA, and Braverman
LE. Serum thyrotropin, thyroxine, and thyroid antibodies in the United States population (1988 to 1994): NHANES III. 2002;J Clin
Endocrinol Metab 2002,87:489-99)
Prevalence of Thyroid Antidodies in the General Population NHANES III (n =16,869) 15 10 5 0 14.7 5.7 3.1 6.9 34.7 6.1 0.6 Thayroid Ab Odds Ratio for Hypothyroidism
(Low TT4+ TSH > 4.5 mU/L)
TPOAb
+TgAb TPOAb+Alone TgAbAlone %
management of patients with differentiated thyroid carcinomas
(DTC). Current Tg methods are based either on IMA or RIA techniques. There is a trend for non-isotopic IMA methods to replace RIA methods because IMA methods are easier to automate, have shorter turn around times, wider working ranges and use reagents with a longer shelf life. 4
Thyroid Function Tests in Special
Patient Populations
Patients with atrial fibrillation, hyperlipidaemia, osteoporosis, infertility
Patients presenting with atrial fibrillation, hyperlipidemia,
subfertility and osteoporosis, should undergo serum TSH estimations as assessment of thyroid function because:
• Atrial fibrillation may be secondary to thyrotoxicosis in
about 5-10% of patients.
• Osteoporosis may be secondary to hyperthyroidism and
can be corrected by treating the underlying cause.
• Both hyper as well as hypothyroidism may be contributing
factors in menstrual cycle disorders, fetal loss and infertility. Women with type 1 diabetes
Type 1 diabetes in women raises their likelihood of developing post-partum thyroid dysfunction by three times. Women with type 1 diabetes should have their thyroid function (including TSH, FT4 and thyroid peroxidise antibody status) assessed at preconception, at the time of registration for pregnancy and at three months post-partum.
Women with a past history of post-partum thyroiditis In women with post-partum thyroiditis, there is an increased long-term risk of developing hypothyroidism and its recurrence in subsequent pregnancies. Therefore, all women with a history of post-partum thyroiditis should be recommended to have a yearly thyroid function test, and also prior to and at 6 to 8 weeks after their subsequent pregnancies.
Patients with diabetes
The frequency of patients with type 1 diabetes and asymptomatic thyroid dysfunction is high. These patients should have a yearly thyroid function test. In patients with type 2 diabetes, thyroid function should be assessed at diagnosis, however, annual thyroid function assessment may not be recommended.
Down syndrome and Turner’s syndrome
Patients of Down syndrome as well as Turner’s syndrome are recommended to undergo thyroid function assessment annually, keeping in mind the high incidence of hypothyroidism seen in these patients.
Patients receiving Amiodarone and Lithium
Therapy with amiodarone is associated with iodide-induced thyroid dysfunction (hypothyroidism or hyperthyroidism) because of the presence of 75 mg iodine per each 200 mg tablet. Patients on amiodarone treatment should have thyroid function assessment at the time of beginning of amiodarone therapy and thereafter every 6 months during treatment and till 12 months after cessation of therapy. Lithium therapy (for bipolar disorder) is associated with mild to overt hypothyroidism in up to 34% to 16% of patients respectively, which can occur abruptly even many years after cessation of therapy. Thyrotoxicosis can also occur due to long-term treatment with lithium but is relatively rare. Therefore, all patients on lithium therapy should have a
thyroid function assessment before commencement of treatment and thereafter every 6-12 months during lithium therapy. Post neck irradiation
Patients who undergo surgery or external radiation therapy of the neck, or both, for head and neck cancer (including lymphoma) have a high incidence (up to 50%) of hypothyroidism. The incidence is particularly high in patients who undergo
surgery and receive high doses of radiation because the effect
is dose-dependent. The onset of overt hypothyroidism due to surgery or irradiation is gradual and may precede subclinical hypothyroidism for many years. In such patients, thyroid function assessment should be carried out annually.
Following destructive treatment for thyrotoxicosis by either radioiodine or surgery
Patients treated with radioiodine or those who undergo thyroidectomy should be screened indefinitely for the development of hypothyroidism or recurrence of hyperthyroidism. Assessment of thyroid function in these patients should be done four to eight weeks after treatment, followed by quarter yearly assessments for the subsequent year and annually thereafter.
Treatment of thyrotoxicosis with anti-thyroid drugs
Antithyroid drugs used in the management of thyrotoxicosis, carbimazole and propylthiouracil, decrease thyroid hormone secretion. Thyroid function assessment should be carried out every 1-3 months to determine whether stable hormonal concentrations have been reached when antithyroid therapy is instituted and annually thereafter if long-term treatment is used. Patients on thyroxine therapy
In patients undergoing thyroxine therapy regardless of the cause, long-term follow-up with annual measurements of serum TSH are recommended. This helps to check compliance, verify the dosage and take account of variations in dosage requirements due to concomitant medications. In pregnant women, the dose may need to be increased by a minimum of 50 μg per day to maintain normal serum TSH levels. The TSH levels should be tested in each trimester.8
Interferences with
Thyroid Test Methodologies
There are four categories of interferences in competitive immunoassays (IMA) as well as non-competitive IMAs: 1. Cross reactivity interferences
2. Endogenous analyte antibodies 3. Heterophilic antibodies 4. Drug interactions
1. Cross reactivity interferences
Early TSH RIA methods had the limitation of cross-reactivity with glycoprotein hormones (such as LH, hCG). Currently, this problem has been almost completely overcome by using monoclonal antibodies for TSH IMA methods. Occasionally, however, unusual cross-reacting isoforms of TSH may be encountered while using the current assays.
2. Endogenous analyte antibodies
Robbins et al were the first to report an unusual thyroxine
binding globulin in the serum in 1956. Subsequently,
autoantibodies against T3, T4 and TSH have been identified
as well as non-thyroid disorders. A number of reports have shown interference due to T3, T4 and TSH autoantibodies leading to anomalous free and total thyroid hormone levels and TSH values. However, the currently used methods rarely have this interference problem. Characteristics of interference due to endogenous autoantibodies may lead to falsely low or falsely high values, depending upon the type of assay and its composition.
3. Heterophilic antibodies
Heterophilic antibodies (particularly HAMA) may affect
IMA methods more than competitive immunoassays by causing the formation of a bridge between the signal and capture antibodies. This creates a false signal resulting in a high value artifact. Moreover, the result may not be abnormal; it may be inappropriately normal. A potential for
influencing results of neonatal screening also exists because
antibodies are able to cross the placenta. Interference due to
heterophilic antibodies can be classified into two categories:
i. HAMA (or human anti-mouse antibodies) are relatively
weak, polyreactive, multispecific antibodies that are
frequently IgM. The presence of HAMA can alter the total as well as free T3, T4 and TSH results due to interference. Use of Fab fragments and heterospecies
assay configurations can be employed as approaches
to reduce this kind of interference.
ii. HAAA. Specific human anti-animal antibodies
(HAAA) are produced in response to well-defined specific antigens after exposure to therapeutic agents
containing animal antigens (such as murine antibody) or by coincidental immunization through workplace contact (such as that which occurs in animal handlers). Though assays for HAMA have been developed, there
are large inter-method differences and therefore the
reliability of these tests is questioned. 4. Drug interferences
In vitro and in vivo effects may occur due to drug
interferences. When the specimen contains a sufficient
concentration of an interfering therapeutic or diagnostic agent, it may lead to methodologic interference resulting
in in-vitro effects. An example is that of heparin which, in
the specimen can cause in-vitro stimulation of lipoprotein
lipase; free fatty acids are liberated that inhibit T4 binding
to serum proteins. On the other hand, when results are altered due to administration of an interfering therapeutic
agent, then it is termed in-vivo effect. An example is that of
furosemide which competitively inhibits thyroid hormone binding to the specimen, thereby causing an abnormal value (low) thyroid hormone result. Interference may also be
secondary to certain pathologic conditions. For instance, in uraemia, abnormal serum constituents such as indole acetic acid may accumulate and cause interference. In addition,
the presence of fluorophor-related therapeutic or diagnostic
agents in the specimen may alter the results of thyroid tests
that employ fluorescent signals.1
Conclusion
• Thyroid disorders have diverse clinical manifestations
therefore, on part of vigilant clinician every suspected case of thyroid disease needs to be evaluated with laboratory investigations.
• Thereby appropriate treatment for thyroid disorders can
be instituted or conservative monitoring carried out to anticipate potential future consequences.
• The enhanced sensitivity and specificity of TSH assays have
greatly improved the assessment of thyroid function tests. Since TSH levels change dynamically in response to the alterations of T3 and T4, the approach to evaluate whether
the patient has thyroid disorder is to test the TSH levels first. • When hypothyroidism is suspected, a free-T4 estimate
is appropriate because total-T3 and free-T3 tests have
inadequate sensitivity and specificity in this setting. • When hyperthyroidism is suspected, the combination
of a free-T4 estimate and a total- or free-T3estimate provides the most complete assessment of the severity of
hyperthyroidism and identifies cases of “T3-toxicosis”, i.e.
a selective increase of the serum T3 concentration.
References
1. Spencer C. Thyroid Function Tests: Assay of Thyroid Hormones and Related Substances, www.thyroidmanager.com. 2010. 2. Supit EJ, Peiris AN. Interpretation of Laboratory Thyroid Function
Tests: Selection and Interpretation. Southern Medical Journal. 2002;95:481-85.
3. Werner SC, Ingbar SH. Werner & Ingbar’s The Thyroid: a fundamental and clinical text, 9th edition. Lippincott Williams & Wilkins.
4. Mascarenhas JMA. RxPG AIPG 2004 Book, 2006.
5. Daniels GH, Amiodarone-Induced Thyrotoxicosis, The J Clinical
Endo & Metab 2000;86:3-8.
6. Walfish PG. Triiodothyronine and thyroxine interrelationships in health and disease. Can Med Assoc J 1976;115:338–42.
7. Düsünsel R, Poyrazoglu HM, Gündüz Z et al. Evidence of central hypothyroidism in children on continuous ambulatory peritoneal dialysis. Adv Perit Dial. 1999;15:262-8.